
Abstract
Background
Kinetic and kinematic gait analysis is increasingly practised as a part of lameness evaluation in dogs. The aim of this study was to examine the normal short- and long-term variation in forelimb gait in sound control dogs (CD) at a walk using seven selected variables of objective kinetic and kinematic gait analyses. Also, to compare the findings in CD to a group of forelimb lame dogs with elbow osteoarthritis (OAD). An additional aim was to test a kinetic based graphic method for lameness detection; symmetry squares (SS). A prospective longitudinal study was carried out on client owned CD and OAD. Clinical and orthopaedic evaluations were performed to ensure soundness and detect and grade lameness. Seven kinetic and kinematic variables and SS were tested for lameness evaluation. The CD were divided into two subgroups, CD1 and CD2, and examined twice: CD1 with two months interval and CD2 with 3–4 h interval. The OAD group was evaluated once and compared to the CD groups’ first examination.
Results
Thirteen CD and 19 OAD were included. For CD1 and CD2, there were no significant differences in any examined variable between examination occasions. Total peak force/impulse symmetry and fore-hind peak force/impulse symmetry differed significantly between OAD and CD. Symmetry squares had a 74% agreement to subjective orthopaedic evaluations.
Conclusions
In CD, no difference in the examined variables was seen between examination occasions. Four out of seven objective variables differed significantly between CD and OAD. The graphic SS method might have diagnostic potential for lameness detection, making it possible to detect a shift from lame to non-lame limbs. Potentially, this might be especially helpful in bilaterally lame dogs, which often represent a clinical challenge in lameness evaluation.
Similar content being viewed by others


Background
Consistent and reliable assessment of lameness in dogs remains a clinical challenge, especially in cases of subtle lameness [1, 2]. A considerable variability in gait can occur even in clinically sound dogs [3], which can be assumed to complicate lameness assessment in the presence of orthopaedic diseases. Knowledge of the normal variation span in frequently used gait parameters in non-lame dogs is crucial to define and identify significant changes. Understanding normal variation is necessary for clinical research as well as for appropriate assessment of each patient’s improvement or development of an orthopaedic ailment.
Visual assessment of gait is commonly performed in clinical practice to identify lameness. However, unless lameness is severe, visual assessment has been described to show substantial interobserver variation and poor agreement with objective kinetic analysis, as previously stated [1, 4].
Kinetic gait analysis is the study of forces generated during locomotion. Ground reaction forces (GRFs) can be measured using a force plate [1]. Peak vertical force (PF) and vertical impulse (I) are frequently used force plate variables and may be considered gold standard for the evaluation of weight bearing lameness in dogs [1, 4,5,6,7,8,9,10].
Kinematic analysis of gait is the study of motion and quantifies variables that describe the location and motions of body segments in space. Markers are placed on predetermined anatomic landmarks, with reflective markers being the most commonly used landmarks for three-dimensional (3D) kinematics. Cameras record the markers’ locations during locomotion on a treadmill or over ground. Specialized software [11] supplies 3D-coordinates of markers over time.
There are different inherent limitations with each of the methods mentioned above for lameness/gait asymmetry evaluation. Combined tests for evaluation of lameness are therefore reported and clinically used in human orthopaedics [12,13,14], which produces more accurate results than each method separately [11]. Recently, combined tests for stifle function in dogs, including subjective and objective variables, have been suggested [15, 16].
The first aim of this study was to examine the normal variation in several kinetic, kinematic and subjective gait variables in clinically sound control dogs (CD) at a walk; then compare these results to similar variables in forelimb lame dogs with elbow OA (OAD). Secondly, we aimed to investigate the normal variability in load distribution in CD over time, with measurements repeated the same or after two months. We also tested a kinetic-based graphic method, “Symmetry Squares” (SS), depicting the load of all four legs. An additional aim was to compare this graphic method to orthopaedic lameness evaluation in a pilot test of its diagnostic value and potential as a future clinically applicable tool to aid in detection of lameness.
Methods
Dogs
Inclusion criteria
All dogs eligible to participate in the study were non chondrodystrophic individuals weighing 20–40 kg with an estimated stride length that allowed measurement of one stance phase on the force plate. This inclusion criterion maximized the chances of hitting the force plate with one paw at a time with the least possible attempts. Dogs should have reached their estimated full height, and their general health was not to be affected by a condition potentially influencing the orthopaedic assessment. Dogs with elbow osteoarthritis (OAD group) and control dogs (CD group) without signs of lameness according to clinical and subjective orthopaedic evaluations, were included and divided in to two separate groups.
The OAD had to have uni- or bilateral forelimb lameness and elbow osteoarthritis confirmed by radiography or computed tomography evaluated by a board-certified radiologist (ECVDI). Any ongoing pain medication was recorded. The OAD were also part of a parallel study [17].
The study was performed at the University Animal Hospital, Uppsala, Sweden, and was ethically approved by the Uppsala animal ethics committee (C102/15). All dog owners provided signed informed consent prior to enrolment in the study.
Exclusion criteria
For CD, exclusion criteria were history of lameness, presentation with lameness at a walk or trot on visual gait assessment and signs of joint disease during orthopaedic examinations. Additionally, ongoing medication with non-steroidal anti-inflammatory drugs, corticosteroids or other drugs that could potentially mask pain responses was a criterion for exclusion.
The OAD were excluded if clinical signs of lameness, originating from other than the elbow joints on visual assessment of gait and orthopaedic examinations, were found; including pain on palpation, abnormal range of motion, thickened joint capsules, or other musculoskeletal abnormalities unrelated to the elbow joints.
Subgroups and number of examinations
The CD group was divided into two subgroups. Group CD1 was examined twice with a two month interval. Group CD2 was examined twice during the same day, with at least three hours of rest and a short leash walk between the examinations. Data from the OAD group were collected once for the current study.
Clinical evaluations
All dogs were independently examined by two experienced clinicians: one board certified surgeon (AB) and a veterinary certified physiotherapist (KP). At first, gait was visually assessed on a concrete walkway outside the University Animal Hospital, at both a walk and a trot. During gait assessment, dogs were handled by their owners or by one of the authors (MK). Lameness was subjectively rated by both examiners using a numerical rating score (NRS) of increasing lameness graded 0–5 [18, 19].
Gait assessment was followed by clinical and orthopaedic examinations (AB) and a physiotherapist evaluation including orthopaedic examination as well as muscle circumference measurements of the brachium, thigh and crus and measurement of elbow passive range of motion (PROM) by goniometry (KP) [20]. Goniometry and muscle measurements for each dog were compared between examinations using the same reference points [21]. Orthopaedic palpable pain and PROM was assessed and graded as none (0), mild (1), moderate (2) or severe (3).
After discussing all of the subjective individual variables (AB and KP), a consensus score was set for each dog; who accordingly was put into one of three categories: normal, mildly, or moderately to severely affected (Table 1). The consensus score was based on the following clinical variables: lameness, joint pain and PROM. The purpose of using a consensus score in the study was to amalgamate and reduce the number of variables, while simultaneously evaluating an average of the clinical data for any deviations.
Kinetic and kinematic evaluations
Data collection
Overground kinetic and kinematic measurements and registrations were performed twice for the CD1 and CD2 groups and once for the OAD-group. High-speed cameras and a submerged 40 × 60 cm piezoelectric force plate (Kistler model 9286 B) were used. For details about the setup, see Additional file 1. The following variables were examined: Total Peak Force (PF) Symmetry (Sym), Fore-Hind PF Sym, Fore PF Sym, Total Impulse(I) Sym, Fore-Hind I Sym, Fore I Sym and Kinematic Range of Motion (ROM) elbow. The dogs were led by their owners or one of the authors (AB) on a leash with no tension applied. Trials were considered valid for further analysis when the dog walked at an even pace, straight forward without turning its head and with one paw at a time striking the FP close to the centre of the plate. Two observers evaluated the trials in real time, and collected data were also visually double-checked. Trials were repeated until data from six valid trials were obtained for each limb.
Symmetry squares (SS)
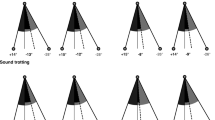
Based on the results from the CDs´ PF and I- measurements, a symmetry graph was constructed depicting the load distribution between all four legs for each dog (Fig. 1). Kinetic data from each dogs’ examination event were assigned a defined colour and projected together with a reference black square. Any deviation from the black square represents a shift of load. The results of the CD-group were compared to the results of the OAD- group in order to assess visual differences in gait patterns. For details, see Additional file 2. After a brief introduction to the method, three observers, blinded to all information regarding the dogs identities and lameness status, were asked to determine whether a dog was lame or not, based only on information from the 29 SS-graphs. All observers were experienced in performing orthopaedic examinations. In dogs assessed to be lame, the observers were to decide which leg(s) that was/were affected and if the dogs walked symmetrically or not. These results were thereafter compared to the orthopaedic consensus score. Two SS-graphs were constructed for each dog based on PF and I- measurements, respectively. The paired graphs were reviewed independently by the three observers. Anonymized and randomized SS graphs from the first examination for all CD and OAD- dogs were sorted into one of the following categories: normal, lame-bilateral, lame-left forelimb, lame-right forelimb, lame-bilateral left dominant, lame-bilateral right dominant. Thereafter, the panel members reviewed and discussed the cases they disagreed on to identify the reasons for disagreement and to evaluate if consensus could be reached. From these results, asymmetry deteced from the SS graph is presented (Table 1).

Symmetry squares (SS) from six different dogs illustrating load distribution between all four legs. The black square, with each corner representing a limb, illustrates the mean of control dogs. Each ¼ corner of the square represents a leg as seen from a dorsal view. Peak Vertical Force SS to the left and Vertical Impulse (I) SS to the right. a) CD4, very well fitting the reference square, the figure also includes an explanation of how the figures should be interpreted, with one limb in each corner of the square. b) CD13, deviations from reference square representing normal variation, c) OAD7, left forelimb lameness clearly seen as transferring of weight from the painful limb – the blue square shifts to the right. More negative values correspond to larger forces transferred to the hind limbs. d) OAD5, bilateral forelimb lameness, not possible to detect from the squares e) OAD4, bilateral forelimb lameness more severe on the left side, seen as transferring of weight to the hindlimbs and primarily to the right f) OAD17, symmetric bilateral forelimb lameness, seen as transferring of weight to the hindlimbs. CD = control dogs, OAD = dogs with elbow osteoarthritis, SS = symmetry squares
Data analysis
The details regarding data analysis and capturing of kinetic data via a Kistler force plate are found in Additional file 3. The motion capture software Qualisys Track Manager® (version 2.12) automatically calculated and reconstructed the three-dimensional coordinates of each reflective marker. Each marker was manually identified, labelled, and validated for correct tracking. For further analysis, marker data were exported to Matlab (R2013B) using custom made scripts.
The following temporospatial and kinetic variables were measured: stance time, peak vertical force (PF), vertical impulse (I) and elbow range of motion (ROM). Gait velocity was measured in m/s. Kinetic variables were normalized for body weight. Speed was normalized to mean speed at each session for each dog (Additional file 1, “Collection of objective data”). To further analyse the relative distribution of forces, the following symmetry variables were calculated for PF and I for each dog: total symmetry between all four legs, forelimb-hindlimb PF symmetry and left-right forelimb symmetry.
Statistical analysis
Statistical analyses were performed using a commercially available software program I. Data was analyzed using descriptive as well as inferential statistics. Continuous variables were presented as mean and standard deviation (SD). The chi-squared test was used to test for differences in proportions in sex between CD and OAD. Continuous data listed in Table 1 were analyzed between the groups (CD and OAD) using the non-parametric Wilcoxon rank sum test. A value of P < 0.05 was considered significant.
For the outcome of biomechanical and measured orthopaedic variables listed in Table 2, differences between time-points of examinations (two months apart for the CD1 group of dogs and three-four hours apart for the CD2 group of dogs, respectively) were investigated. A mixed linear model was used, including dog identity as a random variable, and time-point of examination. For the distributions of model residuals, normality was ensured by visual inspection.
Results
Thirteen dogs in the CD group and 19 dogs in the OAD group were included in the study. Four dogs were excluded due to lameness and/or pain not related to the elbow joints. There were no significant differences in age, body weight or sex between groups. Breeds represented in the CD group were Belgian malinois (n = 1), German shepherd (n = 2) German wirehaired pointer (n = 1), Labrador retriever (n = 5), Mixed breed (n = 1), Rottweiler (n = 2), and Smooth collie (n = 1). Breeds represented in the OAD group were Belgian malinois (n = 1), Bernese mountain dog (n = 2), Bullmastiff (n = 1), German shepherd (n = 3), German spaniel (n = 1), Labrador retriever (n = 7), Leonberger (n = 1), Mixed breed (n = 2) and Rottweiler (n = 1).
The clinical orthopaedic, as well as kinetic and kinematic measurements and comparisons between groups are presented in Table 1.
There were no significant differences between first and second examination in any tested parameter; neither when examination was repeated after a few hours (CD2) nor after two months (CD1) (Table 2).
The variables Total PF Sym, Fore-Hind PF Sym, Total I Sym, Fore-Hind I Sym and measured ROM right elbow differed significantly between the CD and OAD groups. The asymmetry and diverging Total PF, as well as the overlap in Total PF between CD and OAD, is presented in Fig. 2. Blinded evaluation of SS initially resulted in 70.4% inter-observer agreement (Table 3). After consensus discussion, a 100% inter-observer agreement was reached. Figure 1 shows a selection of SS illustrating variation in load distribution in non-lame CD and lame OAD. When comparing the observer’s consensus SS evaluation to the orthopaedic consensus evaluation, agreement was found on 13/19 (68%) of the OAD and 7/8 of the CD (87.5%); in total 74% agreement. Non-agreement was found in 2/13 unilaterally lame dogs and 3/6 bilaterally lame dogs.

The median value of the Total PF Symmetry for each dog. Control dogs (CD) CD (blue) to the left and dogs with elbow osteoarthritis (OAD) (red) to the right. Overall, Total PF Symmetry was lower and showed a greater variation span for OAD compared to CD. However, there was a noticeable area of overlapping between groups. PF = peak force, CD = control dogs, OAD = dogs with elbow osteoarthritis
Discussion
The results from this study show that Total PF and Total I as well as Fore-Hind PF- and Fore-Hind I symmetry differed significantly between CD and OAD. In CD, these variables did not change between repeated examinations within a period of two months. Also, a kinetic-based graphic method (SS) was tested and found to have 74% agreement with subjective orthopaedic evaluation.
Total PF and Total I as well as Fore-Hind PF and Fore-Hind I- symmetry all differed significantly between OAD and CD in the current study. In accordance with these results, several earlier studies have identified PF and I as the parameters best correlating with limb function [9, 10, 22]. There are contradicting results in the literature regarding consistence over time of Total PF and Total I. Some observers report PF to be consistent over time at a trot using a force plate and a pressure mat [23, 24]. In contrast, inter-day and -week differences have been reported in PF of the forelimbs of healthy dogs at a trot, which potentially could be attributed to habituation [25]. In the present study, only non-significant variations between first and second evaluation of CD were found in all tested parameters and for both time intervals when examinations were performed under similar conditions. Notably, although lame dogs were more asymmetric and showed more diverging results, an overlap between CD and OAD was seen. Lame dogs can have a Total PF equal to normal dogs [10, 26]. This emphasizes the complexity in lameness assessment and may imply that objective methods should be seen as an important complement when evaluating lameness, rather than an absolute truth - as there are no specific thresholds to distinguish lame from sound. A multivariable approach to lameness has previously been suggested as there is no existing consensus for a single specific diagnostic test to evaluate limb function in dogs [1, 10, 26]. To the authors’ knowledge, there exists no evaluation method combining objective and subjective measurements for elbow assessment in dogs to this date. However, it is likely that a combination of multiple diagnostic methods might delineate the most accurate picture of the lame dog.
Symmetry squares were based on PF- and I values and aimed to present “a clinically applicable and intuitive to understand diagnostic tool” that could potentially facilitate gait assessment in dogs in terms of weight distribution. A 74% agreement of SS was acquired with the orthopaedic consensus evaluation, which suggests the method might be a helpful addition in the clinical setting, possibly more so for long-term follow up of a single patient. Further prospective studies are warranted to evaluate the use of SS when assessing lameness in a single patient over time. For 19/27 dogs, all three observers separately, preceded by just a brief familiarization with the method, assessed SS identically. It is important that presentation of data is made intuitively easy to understand, which was the reason for why we at first hand wanted to test the ability of clinicians to interpret data based on a very brief introduction instead of a detailed walk through. The cases for which interobserver agreement was low when evaluating SS were either cases with bilateral forelimb lameness or control dogs with small deviations from normal gait symmetry, according to the other variables tested. With increasing experience of SS as a lameness evaluation tool, the sensitivity and specificity of the method may potentially improve. Symmetry squares seem to be simple to understand for clinicians working with orthopaedics and might be an additional evaluation method for detecting lameness. Total PF and Total I are also possible to obtain from a pressure mat, which potentially can make SS easier and cheaper to apply clinically compared to the force plate [23, 27,28,29]. Previously, studies have been done on vertical force distribution in forelimb lame vs healthy dogs [30]. It is likely that these kinds of visual techniques will be used more in the future to help understand how the load is distributed in lame dogs.
In the OAD group, a reduced kinematic ROM due to pain from OA elbows could have been expected, which we did not find. Our results are similar to other studies [31], who also compared normal and OA diseased elbows. As seen in Table 1, there was a greater variability in measured ROM in the OAD-group compared to the uniform CD-group, while there was no significant difference between the groups regarding kinematic ROM. Kinematic ROM at a walk is not directly comparable with measured ROM performed in lateral recumbency with the joint in maximal flexion/extension. In 1995, a study [32] tested repeatability of kinematic measures with three-week intervals in normal Greyhounds, indicating negligible variance.
Objective gait analysis was performed at a walk as some patients were not able to trot long enough for valid hits on the force plate. As [33] argues, excluding these individuals would pose a risk for selection bias towards less lame dogs. Differences between e.g. a control versus a treatment group might then appear smaller. Therefore, results from normal variation measurements at a walk could possibly be more clinically applicable.
There are several limitations to this study. There was a relatively small number of included dogs. Skin motion artifacts are a well-known concern in kinematic gait analysis [34, 35]. We tried to minimize artifacts by standardizing standing positions during marker placement [36], clipping fur and having the same person apply all markers. We used a single FP, which restricted the calculations to non-consecutive steps. The importance of this limitation is debatable [25, 37].
Orthopaedic evaluations are subjective with a risk of bias. By integrating a range of variables and meticulously calculating a consensus score, we attempted to reduce the method’s shortcomings. Factors such as bilateral lameness and individual dog reactions may still influence the outcome. Bilateral lameness is common in dogs and is considered more difficult to evaluate subjectively as well as objectively. There is a risk that bilateral lameness - especially if symmetrical, is identified as normal variation. Including bilaterally lame dogs can be regarded as a significant limitation to the study. However, a significantly bigger peak force shift from fore- to hind limbs was seen in OAD compared to in CD. SS makes this weight shift from lame forelimbs to hind limbs visible, which facilitates detection of forelimb lameness. Accordingly, SS is a potentially helpful tool for visualizing this load shift.
The variation potentially attributed to the dog handler in kinetic studies varies between 0 and 7% for the GRFs evaluated [38] and is considered to be of little concern. Therefore, this is regarded as an insignificant source of error in the present study.
Velocity was not strictly regulated. Researchers have previously concluded that a wider velocity range can be used with little or no effect on GRFs in sound dogs, at least at the trot, suggesting negligible interference from this factor [39].
Conclusions
Total PF and Total I, Fore-Hind PF and Fore-Hind I symmetry all differed significantly between OAD and CD. No difference was seen between examinations repeated the same day or after two months in the CD groups. Importantly, for all tested parameters there was an overlap between CD and OAD dogs. Symmetry squares appears to have potential as a complementary objective tool for lameness evaluation, making it possible to detect a shift from lame to non-lame limbs. Potentially, this might be especially helpful in bilaterally lame dogs, which often represent a clinical challenge in lameness evaluation. However, the method needs further evaluation in future studies.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
References
Quinn MM, Keuler NS, Lu Y, Faria MLE, Muir P, Markel MD. Evaluation of agreement between numerical rating scales, visual analogue scoring scales, and force plate gait analysis in dogs. Vet Surg. 2007;36:360–7. https://doi.org/10.1111/j.1532-950X.2007.00276.x.
Voss K, Imhof J, Kaestner S, Montavon PM. Force plate gait analysis at the walk and trot in dogs with low-grade hindlimb lameness. Vet Comp Orthop Traumatol. 2007;20:299–304. https://doi.org/10.1160/vcot-07-01-0008.
Fahie MA, Cortez JC, Ledesma M, Su Y. Pressure mat analysis of walk and trot gait characteristics in 66 normal small, medium, large, and giant breed dogs. Front Vet Sci. 2018;5:256. https://doi.org/10.3389/fvets.2018.00256.
Waxman AS, Robinson DA, Evans RB, Hulse DA, Innes JF, Conzemius MG. Relationship between objective and subjective assessment of limb function in normal dogs with an experimentally induced lameness. Vet Surg. 2008;37:241–6. https://doi.org/10.1111/j.1532-950X.2008.00372.x.
Amimoto H, Koreeda T, Ochi Y, Kimura R, Akiyoshi H, Nishida H, et al. Force plate gait analysis and clinical results after tibial plateau levelling osteotomy for cranial cruciate ligament rupture in small breed dogs. Vet Comp Orthop Traumatol. 2020;33:183–8. https://doi.org/10.1055/s-0039-1700990.
Budsberg SC. Long-term temporal evaluation of ground reaction forces during development of experimentally induced osteoarthritis in dogs. Am J Vet Res. 2001;62:1207–11. https://doi.org/10.2460/ajvr.2001.62.1207.
Budsberg SC, Verstraete MC, Soutas-Little RW. Force plate analysis of the walking gait in healthy dogs. Am J Vet Res. 1987;48:915–8.
Conzemius MG, Evans RB, Besancon MF, Gordon WJ, Horstman CL, Hoefle WD, et al. Effect of surgical technique on limb function after surgery for rupture of the cranial cruciate ligament in dogs. J Am Vet Med Assoc. 2005;226:232–6. https://doi.org/10.2460/javma.2005.226.232.
DeCamp CE. Kinetic and kinematic gait analysis and the assessment of lameness in the dog. Vet Clin North Am Small Anim Pract. 1997;27:825–40. https://doi.org/10.1016/s0195-5616(97)50082-9.
Evans R, Horstman C, Conzemius M. Accuracy and optimization of force platform gait analysis in labradors with cranial cruciate disease evaluated at a walking gait. Vet Surg. 2005;34:445–9. https://doi.org/10.1111/j.1532-950X.2005.00067.x.
Clements DN, Owen MR, Carmichael S, Reid SW. Kinematic analysis of the gait of 10 labrador retrievers during treadmill locomotion. Vet Rec. 2005;156:478–81. https://doi.org/10.1136/vr.156.15.478.
Frohm A, Heijne A, Kowalski J, Svensson P, Myklebust G. A nine-test screening battery for athletes: a reliability study. Scand J Med Sci Sports. 2012;22:306–15. https://doi.org/10.1111/j.1600-0838.2010.01267.x.
Lin YC, Davey RC, Cochrane T. Tests for physical function of the elderly with knee and hip osteoarthritis. Scand J Med Sci Sports. 2001;11:280–6. https://doi.org/10.1034/j.1600-0838.2001.110505.x.
Rejeski WJ, Ettinger WH Jr., Schumaker S, James P, Burns R, Elam JT. Assessing performance-related disability in patients with knee osteoarthritis. Osteoarthritis Cartilage. 1995;3:157–67. https://doi.org/10.1016/s1063-4584(05)80050-0.
Hyytiainen HK, Molsa SH, Junnila JJT, Laitinen-Vapaavuori OM, Hielm-Bjorkman AK. Developing a testing battery for measuring dogs’ stifle functionality: the Finnish Canine Stifle Index (FCSI). Vet Rec. 2018;183:324. https://doi.org/10.1136/vr.104588.
Pinna S, Lanzi F, Grassato L. Bologna healing stifle injury index: a comparison of three surgical techniques for the treatment of cranial cruciate ligament rupture in dogs. Front Vet Sci. 2020;7:567473. https://doi.org/10.3389/fvets.2020.567473.
Bergström A, Kjörk Granström M, Roepstorff L, Alipour MJ, Pettersson K, Ljungvall I. Long-term effect of intraarticular adipose-derived stromal vascular fraction and platelet-rich plasma in dogs with elbow joint disease. Submitted manuscript.
Impellizeri JA, Tetrick MA, Muir P. Effect of weight reduction on clinical signs of lameness in dogs with hip osteoarthritis. J Am Vet Med Assoc. 2000;216:1089–91. https://doi.org/10.2460/javma.2000.216.1089.
Scott H, Witte P. Investigation of lameness in dogs. Pract. 2011;33:20–7. https://doi.org/10.1136/inp.c7447.
Jaegger G, Marcellin-Little DJ, Levine D. Reliability of goniometry in labrador retrievers. Am J Vet Res. 2002;63:979–86. https://doi.org/10.2460/ajvr.2002.63.979.
Lorinson K, Lorinson D, Millis D. Examination of the physiotherapy patient. In: Bockstahler B, editor. Essential fact of physical medicine, rehabilitation and sports medicine in companion animals. Babenhausen: VBS GmbH; 2019. pp. 83–106.
Fanchon L, Grandjean D. Accuracy of asymmetry indices of ground reaction forces for diagnosis of Hind limb lameness in dogs. Am J Vet Res. 2007;68:1089–94. https://doi.org/10.2460/ajvr.68.10.1089.
Lascelles BD, Roe SC, Smith E, Reynolds L, Markham J, Marcellin-Little D, et al. Evaluation of a pressure walkway system for measurement of vertical limb forces in clinically normal dogs. Am J Vet Res. 2006;67:277–82. https://doi.org/10.2460/ajvr.67.2.277.
Nordquist B, Fischer J, Kim SY, Stover SM, Garcia-Nolen T, Hayashi K, et al. Effects of trial repetition, limb side, intraday and inter-week variation on vertical and craniocaudal ground reaction forces in clinically normal labrador retrievers. Vet Comp Orthop Traumatol. 2011;24:435–44. https://doi.org/10.3415/VCOT-11-01-0015.
Stejskal M, Torres BT, Sandberg GS, Sapora JA, Dover RK, Budsberg SC. Variability of vertical ground reaction forces collected with one and two force plates in healthy dogs. Vet Comp Orthop Traumatol. 2015;28:318–22. https://doi.org/10.3415/VCOT-15-02-0037.
Voss K, Damur DM, Guerrero T, Haessig M, Montavon PM. Force plate gait analysis to assess limb function after tibial tuberosity advancement in dogs with cranial cruciate ligament disease. Vet Comp Orthop Traumatol. 2008;21:243–9.
Evans R, Gordon W, Conzemius M. Effect of velocity on ground reaction forces in dogs with lameness attributable to tearing of the cranial cruciate ligament. Am J Vet Res. 2003;64:1479–81. https://doi.org/10.2460/ajvr.2003.64.1479.
Horstman CL, Conzemius MG, Evans R, Gordon WJ. Assessing the efficacy of perioperative oral carprofen after cranial cruciate surgery using noninvasive, objective pressure platform gait analysis. Vet Surg. 2004;33:286–92. https://doi.org/10.1111/j.1532-950x.2004.04042.x.
Light VA, Steiss JE, Montgomery RD, Rumph PF, Wright JC. Temporal-spatial gait analysis by use of a portable walkway system in healthy labrador retrievers at a walk. Am J Vet Res. 2010;71:997–1002. https://doi.org/10.2460/ajvr.71.9.997.
Braun L, Tichy A, Peham C, Bockstahler B. Comparison of vertical force redistribution in the pads of dogs with elbow osteoarthritis and healthy dogs. Vet J. 2019;250:79–85. https://doi.org/10.1016/j.tvjl.2019.06.004.
Galindo-Zamora V, Dziallas P, Wolf DC, Kramer S, Abdelhadi J, Lucas K, et al. Evaluation of thoracic limb loads, elbow movement, and morphology in dogs before and after arthroscopic management of unilateral medial coronoid process disease. Vet Surg. 2014;43:819–28. https://doi.org/10.1111/j.1532-950X.2014.12250.x.
Kano WT, Rahal SC, Agostinho FS, Mesquita LR, Santos RR, Monteiro FOB, et al. Kinetic and temporospatial gait parameters in a heterogeneous group of dogs. BMC Vet Res. 2016;12:2. https://doi.org/10.1186/s12917-015-0631-2.
Wearing SC, Reed LF, Urry SR. Agreement between temporal and spatial gait parameters from an instrumented walkway and treadmill system at matched walking speed. Gait Posture. 2013;38:380–4. https://doi.org/10.1016/j.gaitpost.2012.12.017.
Kim SY, Kim JY, Hayashi K, Kapatkin AS. Skin movement during the kinematic analysis of the canine pelvic limb. Vet Comp Orthop Traumatol. 2011;24:326–32. https://doi.org/10.3415/VCOT-10-08-0123.
Schwencke M, Smolders LA, Bergknut N, Gustås P, Meij BP, Hazewinkel HA. Soft tissue artifact in canine kinematic gait analysis. Vet Surg. 2012;41:829–37. https://doi.org/10.1111/j.1532-950X.2012.01021.x.
Kim SY, Torres BT, Sandberg GS, Budsberg SC. Effect of limb position at the time of skin marker application on sagittal plane kinematics of the dog. Vet Comp Orthop Traumatol. 2017;30:438–43. https://doi.org/10.3415/VCOT-16-12-0172.
Volstad NJ, Sandberg G, Robb S, Budsberg SC. The evaluation of limb symmetry indices using ground reaction forces collected with one or two force plates in healthy dogs. Vet Comp Orthop Traumatol. 2017;30:54–8. https://doi.org/10.3415/VCOT-16-04-0054.
Jevens DJ, Hauptman JG, DeCamp CE, Budsberg SC, Soutas-Little RW. Contributions to variance in force-plate analysis of gait in dogs. Am J Vet Res. 1993;54:612–5.
Hans EC, Zwarthoed B, Seliski J, Nemke B, Muir P. Variance associated with subject velocity and trial repetition during force platform gait analysis in a heterogeneous population of clinically normal dogs. Vet J. 2014;202:498–502. https://doi.org/10.1016/j.tvjl.2014.09.022.
Acknowledgements
The authors would like to acknowledge the invaluable assistance of Christoffer Roepstorff with the practical assistance during data collection for the objective gait analysis. The authors also wish to acknowledge all dogs and owners participating in the study.
Funding
This study was funded by Agria Pet Insurance Research Foundation. The founding covered all costs related to the study such as reflective markers etc., but the founder had no influence on the manuscript.
Open access funding provided by Swedish University of Agricultural Sciences.
Author information
Authors and Affiliations
Contributions
All authors: MK, LR, KP, IL, MD, CP, AB, contributed to the study design (all parts or various parts). AB, MK and KP collected the data. IL performed the statistical analysis and LR performed the data processing and analysis of the objective measurements. MK, MD and CP performed the observational trial of the symmetry squares. MK wrote the manuscript with substantial input from all co-authors. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
The study was ethically approved by the Uppsala animal ethics committee (C102/15). All dog owners provided signed informed consent prior to enrolment in the study.
Consent for publication
As stated in the “Methods” section, all dog owners provided signed informed consent prior to enrolment in the study.
Prior publication
Data have not been published previously.
Competing interests
The authors declare that they have no competing interests.
Endnotes
Footnote I: JMP 16 Pro, Cary, NC USA.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Granström, M.K., Roepstorff, L., Pettersson, K. et al. Evaluation of forelimb gait variation overground at a walk in sound and lame dogs using a combination of diagnostic techniques. Acta Vet Scand 66, 25 (2024). https://doi.org/10.1186/s13028-024-00746-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13028-024-00746-w