
Abstract
Background
The association between osteoarthritis (OA) and hypertension is a subject of ongoing debate in observational research, and the underlying causal relationship between them remains elusive.
Methods
This study retrospectively included 24,871 participants in the National Health and Nutrition Examination Survey (NHANES) from 2013 to 2020. Weighted logistic regression was performed to investigate the connection between OA and hypertension. Additionally, Mendelian randomization (MR) analysis was conducted to explore the potential causal relationship between OA and hypertension.
Results
In the NHANES data, after adjusting for multiple confounding factors, there was no significant relationship between OA and hypertension (OR 1.30, 95% CI, 0.97–1.73, P = 0.089). However, among males, OA appeared to be associated with a higher risk of hypertension (OR 2.25, 95% CI, 1.17–4.32, P = 0.019). Furthermore, MR results indicate no relationship between multiple OA phenotypes and hypertension: knee OA (IVW, OR 1.024, 95% CI: 0.931–1.126, P = 0.626), hip OA (IVW, OR 0.990, 95% CI: 0.941–1.042, P = 0.704), knee or hip OA (IVW, OR 1.005, 95% CI: 0.915–1.105, P = 0.911), and OA from UK Biobank (IVW, OR 0.796, 95% CI: 0.233–2.714, P = 0.715). Importantly, these findings remained consistent across different genders and in reverse MR.
Conclusions
Our study found that OA patients had a higher risk of hypertension only among males in the observational study. However, MR analysis did not uncover any causal relationship between OA and hypertension.
Similar content being viewed by others


Introduction
With the aging of the population, osteoarthritis (OA) has become a leading cause of disability and chronic pain in the elderly [1]. Its pathological characteristics include cartilage degeneration, bone remodeling, osteophyte formation, and synovial inflammation, which ultimately lead to pain, joint stiffness, swelling, and the eventual loss of normal joint function [2]. According to statistical data, approximately 80% of patients with knee or hip osteoarthritis experience varying degrees of activity limitations, and 25% unable to perform essential daily life activities [3].
Hypertension is a prominent global health concern, characterized by a continuous increase in its prevalence. In 2015, it was estimated that there were approximately 1.13 billion cases of hypertension worldwide. The prevalence of hypertension significantly rises with age, affecting over 60% of individuals aged over 60 years [4]. It has been extensively linked to cardiovascular diseases, including coronary artery disease (CAD), congestive heart failure (CHF), stroke, myocardial infarction (MF), atrial fibrillation (AF), and peripheral arterial disease (PAD), as well as kidney damage, Alzheimer’s disease, and other serious complications [5,6,7]. And efficient prevention and management of hypertension play a crucial role in reducing the global disease burden and promoting overall longevity [8]. Consequently, hypertension research has garnered substantial attention, with the aim of gaining a better understanding of its etiology, risk factors, and connections with other medical conditions. Ultimately, these efforts seek to develop more effective interventions and treatment strategies.
However, there is still controversy surrounding the potential link between OA and hypertension. Evidence suggests that approximately 55% of knee osteoarthritis patients aged 65 and older have hypertension, and Incident OA occurred more frequently with an increase in blood pressure level, even after adjusting for confounding factors such as body mass index (BMI) [9, 10].Nevertheless, some studies present differing viewpoints [11,12,13,14]. In order to gain a deeper understanding of the potential connection between OA and hypertension, this study aims to investigate the relationship between them using observational data. Furthermore, it seeks to assess the causal relationship between the two through bidirectional Mendelian randomization (MR) analysis.
Methods
Study design and study overview
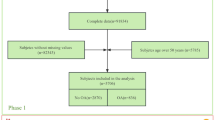
This study was conducted in two phases. Initially, we characterized observational associations between osteoarthritis and hypertension using data derived from the National Health and Nutrition Examination Survey (NHANES). Subsequently, to investigate the potential causal relationship between osteoarthritis and hypertension, bidirectional two-sample Mendelian randomization (MR) analysis was performed using summary statistics from the genome-wide association study (GWAS). The forward MR analyses considered osteoarthritis as the exposure and hypertension as the outcome, while the reverse MR analyses hypertension as the exposure and osteoarthritis as the outcome. The flowchart is shown in Fig. 1.

Overall Study Design Based on Observational Analysis and Mendelian Randomization. (A) The flowchart of the observational analysis. (B) The flowchart of the mendelian randomization analysis. OA, osteoarthritis; UKB, UK Biobank
Observational analyses
Data sources and study population
NHANES constitutes an ongoing series of cross-sectional surveys aimed at evaluating the health and nutritional status of the civilians in the United States. This initiative is overseen by the National Center for Health Statistics under the purview of the Centers for Disease Control and Prevention (CDC). Additionally, it has received the ethical approval of the Ethics Review Board at the National Center for Health Statistics [15]. All procedures were performed following the guidelines of the Declaration of Helsinki.
In order to investigate the potential connection between osteoarthritis and hypertension, we conducted a retrospective analysis using data gathered from participants (≥ 20 years of age) across four 2-year NHANES survey cycles (2013–2020). The proportion of missing values for all variables was less than 15%, and missing data were imputed using the package “missforest” in R.
Diagnosis of osteoarthritis and hypertension
Osteoarthritis was denoted as M19.9 based on the International Classification of Diseases 10th Revision (ICD-10). Hypertension was defined as the average of three systolic blood pressure measurements ≥ 140 mmHg, the average of three diastolic blood pressure measurements ≥ 90 mmHg, current usage of medications for blood pressure control, or previously told had high blood pressure [16].
Assessment of covariates
The following covariates were included in this study: age, gender, NHANES cycles, race, educational level, family income, heavy drinker, smoker, BMI, uric acid, high-density lipoprotein cholesterol (HDL-C), total cholesterol (TC), triglyceride (TG), blood urea nitrogen (BUN), aspartate transaminase (AST), alanine aminotransferase (ALT), glycohemoglobin, estimate glomerular filtration rate (eGFR), cancer, diabetes mellitus (DM), osteoporosis, stroke, arteriosclerotic cardiovascular disease (ASCVD), heart attack, CHF, walk or bicycle, work activity, recreational activity, antiplatelet agents, statins, antihypertensive agents. Family income was divided into three levels according to the family poverty income ratio: low income (≤ 1.3), medium income (> 1.3 to 3.5), and high income (> 3.5) [17]. The definition of smoker, heavy drinker, ASCVD, and DM as described in previous literature [18]. Data on diagnosed history of cancer, osteoporosis, stroke, heart attack, and CHF were self-reported. Physical activity including walk or bicycle, work activity, and recreational activity was obtained in questionnaire. Specifically, work activity and recreational activity were classified into four categories based on NHANES guidelines: none, moderate, both, and vigorous. The use of antiplatelet agents, statins, and antihypertensive agents was derived from medication history.
Statistical analysis
According to NHANES analytic guidelines, complex sampling design and sampling weights were considered in this study [19]. T tests and Chi-square tests were applied for analyzing the association of hypertension with continuous variables and categorical variables, respectively. The multivariable logistic regression was employed to compute odds ratios (ORs) and 95% confidence intervals (95% CIs) to ascertain the effects of osteoarthritis on hypertension. In the logistic regression model, Model 1 was adjusted for none. Model 2 was adjusted for age, gender, heavy drinker, smoker, and education level. Model 3 was further adjusted for BMI, HDL-C, TC, BUN, ALT, glycohemoglobin, eGFR, family income, cancer, ASCVD, DM, osteoporosis, stroke, heart attack, CHF, uric acid, antiplatelet agents, and statins. Model 4 was based on model 3 and walk or bicycle. Confounding factors that were significantly associated with hypertension (P < 0.05) or a change in effect estimate of more than 10% were included in Model 4 [20]. The variance inflation factor (VIF) for all variables in the models was below 10, mitigating the impact of multicollinearity on the results [21]. Subgroup analyses were performed to evaluate the association between osteoarthritis and hypertension across various subgroups. And likelihood ratio tests were employed to identify potential interactions. Subsequently, propensity score matching (PSM) was conducted, the matching variables encompassed age, gender, heavy drinker, smoker, Race, education level, BMI, NHANES cycles, and walk or bicycle with caliper values set at 0.02. Final, logistic regression analysis was performed on the data after PSM. Model 1was adjusted for none. Model 2 was adjusted for age, gender, BMI, HDL-C, TG, BUN, ALT, AST, glycohemoglobin, eGFR, family income, uric acid, ASCVD, DM, stroke, heart attack, CHF, antiplatelet agents, recreational activity and statins. All analyses were performed using R 4.1.2 (http://www.r-project.org). Two-sided levels of significance were calculated, and the significance level was set as 0.05.
Mendelian randomization
Selection of genetic instruments for MR analyses
To ensure the accuracy and robustness of causal inference, the selection of genetic instruments should satisfy the three key assumptions of MR. First, Single Nucleotide Polymorphisms (SNPs) were chosen based on a genome-wide significance threshold and F-statistics > 10 [22]. Second, independent SNPs were kept based on linkage disequilibrium (LD) as measured by r2 < 0.001 and clumping distance = 10,000 kb. Final, SNPs associating with the outcome and confounding factors (p < 5 × 10− 8) were excluded, and palindromic SNPs with intermediate allele frequencies were deleted when harmonizing exposure and outcome data [23, 24].
Data sources and genetic instruments selection for osteoarthritis
The OA data were sourced from the UK Biobank (UKB) [25], which serves as a crucial biobank resource (http://www.nealelab.is/uk-biobank/) and from the GWAS data analyzed by Tachmazidou et al. [26]. In the dataset obtained from Tachmazidou, three distinct phenotypes were employed in our study: knee osteoarthritis, hip osteoarthritis, and knee or hip osteoarthritis, as detailed in Table S1. When osteoarthritis was considered as the exposure variable, the significance threshold was set at p < 5 × 10− 7. SNPs associated with hypertension or with confounding factors such as body weight, BMI, and obesity were systematically excluded through the use of PhenoScanner [27].
Data sources and genetic instruments selection for hypertension
The sources of GWAS data for hypertension encompassed the ninth release of the FinnGen Study [28]. In the FinnGen Study, the hypertension dataset consisted of 111,581 cases and 265,626 controls. When hypertension was considered as the exposure, we employed a more stringent significance threshold (p < 1 × 10− 8) due to the numerous SNPs associated with hypertension. Furthermore, SNPs associated with osteoarthritis or with confounding factors (bone density, body weight, BMI, obesity, and diabetes) were excluded using PhenoScanner.
Statistical analysis for MR
Heterogeneity for both inverse-variance weighted (IVW) and MR-Egger methods was evaluated through Cochran’s Q statistics. In light of observed potential heterogeneity, this investigation adopted the random-effects IVW model as the primary analytical approach to explore the causal association between osteoarthritis and hypertension [29]. And other MR methods, such as MR Egger, weighted median, simple mode, and weighted mode, were also employed as reference points. Furthermore, to bolster the assessment of the causal relationship and alleviate the potential influence of horizontal pleiotropy on the outcomes, MR-Egger methods were employed [30, 31]. Moreover, if MR-Egger methods detect horizontal pleiotropy in the genetic instruments, additional steps will be taken to address this issue. These include conducting an outlier test using MR-PRESSO, and subsequently, any outlying SNPs identified in the MR-PRESSO outlier test will be excluded [32]. This process aims to further mitigate the impact of pleiotropic SNPs. All MR analyses were performed using the package “TwosampleMR” [33](version 0.5.6) in R.
Result
Population characteristics of NHANES
This study comprised a total of 24,871 participants after excluding 1,418 individuals with missing sample weight data. The weighted mean age was 48.05 years (95% CI, 51.17–52.63 years), and females accounted for 51.90% (95% CI, 51.17-52.63%). The main characteristics are summarized in Table S2. Among all participants, 360 individuals were diagnosed with OA, representing 1.64% of the total participants, while 10,546 individuals had hypertension, constituting 37.78% of the participants. In comparison to those without OA, individuals with OA exhibited higher age, a greater proportion of females, and an increased BMI. Additionally, they demonstrated a heightened prevalence of conditions including cancer, ASCVD, DM, osteoporosis, stroke, CHF, and hypertension. Furthermore, they reported lower levels of physical activity, as indicated in Table 1.
Association between OA and hypertension in NHANES
The results from weighted logistic regression analysis indicated that, in the unadjusted model, individuals with osteoarthritis exhibited a higher hypertension risk compared to those without (OR 3.41, 95% CI, 2.64–4.40, P < 0.001). However, upon controlling for confounding factors in Model 3, this relationship ceased to be statistically significant (OR 1.30, 95% CI, 0.98–1.74, P = 0.080). Further adjustment for physical activity did not change the observed association between OA and hypertension (OR 1.30, 95% CI, 0.97–1.73, P = 0.089). The specific results are presented in Table 2.
In subgroup analyses, all subgroups adjusted for variables in Model 4 except for the stratification variable. The results of the subgroup analyses are depicted in Fig. 2. In the majority of subgroups, there was no significant association between OA and hypertension. It is noteworthy that among males, individuals with OA appeared to have a higher risk of hypertension (OR 2.25, 95% CI, 1.17–4.32, P = 0.019). However, interaction analysis indicated that there was no significant difference in the relationship between OA and hypertension across different genders.

The Relationship between OA and Hypertension in Different Subgroups of NHANES 2013–2020. Each stratification was adjusted for variables in Model 4 except the stratification factor itself
To further investigate the association between OA and hypertension, PSM was conducted, followed by univariate and multivariate logistic regression analyses on the matched data. The results showed that even after PSM, a total of 13,192 participants remained, including 6,596 with hypertension and 219 with OA (Table S3). Whether through univariate or multivariate logistic regression, the results consistently failed to reveal a significant association between OA and hypertension (Table S4).
Causal effects of OA on hypertension by MR
In our study, for each instrument, all F-statistics were > 10, indicating a reduced susceptibility to weak instrument bias and a higher confidence in the causal effect estimate. MR-Egger regression analysis did not reveal significant horizontal pleiotropy between OA and hypertension (P > 0.05). However, due to the presence of heterogeneity, using IVW as our primary assessment method is more appropriate. The horizontal pleiotropy and heterogeneity results for instrumental variables are shown in Tables S5 and S6. The results presented in Fig. 3 and Table S7 suggest the absence of a causal relationship between multiple OA datasets and hypertension: knee OA (IVW, OR 1.024, 95% CI: 0.931–1.126, P = 0.626), hip OA (IVW, OR 0.990, 95% CI: 0.941–1.042, P = 0.704), knee or hip OA (IVW, OR 1.005, 95% CI: 0.915–1.105, P = 0.911), and OA from UKB (IVW, OR 0.796, 95% CI: 0.233–2.714, P = 0.715). Moreover, alternative MR methods yielded similar findings, with none indicating any causal effects of OA on hypertension (both P > 0.05). Furthermore, in light of observations among male participants from NHANES suggesting that individuals with OA may exhibit an increased hypertension risk, we conducted an in-depth exploration of the causal effects of OA on hypertension within different gender subgroups using MR. The findings consistently indicated the absence of a causal relationship between the two in distinct gender groups: males (IVW, OR 1.874, 95% CI: 0.533–6.596, P = 0.328), and females (IVW, OR 0.789, 95% CI: 0.236–2.636, P = 0.701).

The Causal Relationship of OA on Hypertension. OR and 95% confidence interval were calculated using the inverse variance weighted method. OR, odds ratio; OA, osteoarthritis; UKB, UK Biobank
Causal effects of hypertension on OA by MR
To explore the potential reverse causal relationship between OA and hypertension, we conducted a reverse MR analysis, using hypertension as the exposure variable and OA as the outcome variable. Similarly, in the reverse MR analysis, no evidence of horizontal pleiotropy was detected. Moreover, we did not observe any causal association between hypertension and various OA outcomes: knee OA (IVW, OR 0.999, 95% CI: 0.949–1.052, P = 0.981), hip OA (IVW, OR 0.980, 95% CI: 0.917–1.047, P = 0.548), knee or hip OA (IVW, OR 0.989, 95% CI: 0.946–1.035, P = 0.639), and OA from the UK Biobank (IVW, OR 0.998, 95% CI: 0.995–1.001, P = 0.251). Detailed results can be found in Fig. 4 and Table S8.

The Causal Relationship of Hypertension on OA. OR and 95% confidence interval were calculated using the inverse variance weighted method. OR, odds ratio; OA, osteoarthritis; UKB, UK Biobank
Discussion
To the best of our knowledge, this study represents the first comprehensive investigation into the relationship between OA and hypertension risk, employing a combination of extensive observational study data and MR analysis based on large-scale genetic dataset. The outcomes of this research provide novel insights into the exploration of the connection between OA and hypertension. In the retrospective segment of the study, we included a substantial sample from the NHANES, comprising a total of 24,871 participants. Following meticulous weighting, this sample effectively represents the U.S. population. The findings initially suggest that, in unadjusted models, OA patients demonstrate a higher hypertension risk. However, upon further adjustment for confounding factors, this association loses its statistical significance. Even in subgroup analyses, with the exception of males, no substantial correlation between OA and hypertension was observed in other subgroups. These results are in alignment with prior literature [11,12,13,14].
However, numerous studies have also suggested that OA serves as a risk factor for hypertension. In a prospective cohort study, it was found that patients with knee osteoarthritis experienced a 13% increased risk of developing hypertension during an 8-year follow-up period. This association remained robust even after employing propensity score matching [34]. Furthermore, the findings of a meta-analysis underscore a significant connection between hypertension and knee joints, as opposed to non-weight-bearing joints [35]. These studies are theoretically grounded in the notion that OA patients often contend with chronic pain and restricted mobility, which can potentially lead to weight gain, reduced physical activity, and metabolic disruptions [36, 37], all of which are recognized risk factors for hypertension. Moreover, Research suggest that OA is typically characterized by a certain degree of chronic low-grade inflammation, with various soluble inflammatory mediators such as Interleukin-6 (IL-6), Tumour necrosis factor alpha (TNF-α), and C-reactive protein (CRP) elevated in osteoarthritic tissues [38]. Notably, inflammation plays a pivotal role in hypertension. It has been reported that IL-6 inhibition attenuates hypertension and blunts the infiltration or proliferation of macrophages and mononuclear cells into the kidneys, thereby reducing hypertension-related renal damage in Dahl salt-sensitive rats [39]. And inflammation is believed to be a contributing factor to the elevated risk of cardiovascular disease-related mortality in individuals with OA. Inflammatory processes may expedite the development of atherosclerosis, leading to hypertension by causing arterial stiffening and proliferation due to arterial wall degeneration [40]. However, it’s worth noting that current anti-inflammatory therapies have not proven to be highly effective, whether in treating osteoarthritis or hypertension [38, 41].
In our retrospective study, we observed a heightened risk of hypertension among males with osteoarthritis, while no such association was observed in females. Androgen signaling may play a crucial role in this gender disparity, as previous studies have shown that increased androgen receptor (AR) activity and testosterone levels may influence hypertension by altering the renin-angiotensin-aldosterone system [42]. And lower CAG repeat lengths in the AR coding region are associated with central obesity and hypertension in males rather than females [43]. Additionally, study have suggested an association between androgen receptor polymorphism and osteoarthritis [44], and recent Mendelian randomization studies have further indicated a causal relationship between androgen and the occurrence of osteoarthritis [45]. Therefore, androgen signaling may partially explain the association between osteoarthritis and hypertension. Nonetheless, observational studies cannot conclusively determine whether this association is merely correlational or causal.
Owing to potential confounding factors and bidirectionality inherent in observational data, this may account for the disparities between our study and others. In order to bolster the control over confounders and thereby bolster more robust causal inferences, we conducted MR analysis to explore the causal relationships between different subtypes of osteoarthritis and hypertension within distinct gender groups. However, we found no association between the genetic liability to osteoarthritis and hypertension. This consistency was observed across different genders and in reverse analyses.
There is currently limited fundamental research on the connection between OA and hypertension. It has been reported that knee OA patients with comorbid hypertension and diabetes exhibit significant bone loss in the subchondral plate, with the medial part of the tibial plateau demonstrating lower bone mineral density (BMD) and higher porosity [46]. Additionally, in OA rats with coexisting hypertension, there is a higher level of synovial inflammation, which may potentially facilitate the progression of OA [47]. Nevertheless, these findings are still insufficient to explain whether OA leads to the development of hypertension or if hypertension contributes to the onset of OA. Overall, based on our research findings, there may not be a causal relationship between OA and hypertension.
This study has several strengths. We employed a combined approach of observational research and MR analysis to investigate the relationship between OA and hypertension. This comprehensive research design allows for a more holistic understanding of the connection between OA and hypertension, supported by multiple lines of evidence. Nonetheless, the study does come with certain limitations. Firstly, despite using a large-scale NHANES sample, the prevalence of OA is relatively low, which might affect our ability to detect causal relationships. Secondly, even though we controlled for various confounding factors in the study, there may still be unaccounted confounders that could introduce potential interference when explaining the relationship between OA and hypertension. And in the retrospective study, we did not further analyze the association between different subtypes of OA and hypertension. Moreover, although there was no pleiotropy in the MR analyses, some exhibited heterogeneity, which could potentially impact our results.
Conclusions
In the MR analysis, no causal relationship was found between OA and hypertension, even though the observational study revealed a higher risk of hypertension in the male subgroup of OA patients. However, it’s important to note that the observational findings might be subject to bias due to uncontrolled confounders. Therefore, it is essential to conduct more well-designed prospective studies to minimize observational study biases and redundancy. Furthermore, utilizing larger GWAS datasets for MR analysis is recommended.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- AF:
-
Atrial fibrillation
- ASCVD:
-
Arteriosclerotic cardiovascular disease
- AST:
-
Aspartate transaminase
- ALT:
-
Alanine aminotransferase
- BUN:
-
Blood urea nitrogen
- BMI:
-
Body mass index
- BMD:
-
Bone mineral density
- CAD:
-
Coronary artery disease
- CHF:
-
Congestive heart failure
- CDC:
-
Centers for Disease Control and Prevention
- CRP:
-
C-reactive protein
- CI:
-
Confidence interval
- DM:
-
Diabetes mellitus
- eGFR:
-
Estimate glomerular filtration rate
- GWAS:
-
Genome-wide association study
- HDL-C:
-
High-density lipoprotein cholesterol
- IVW:
-
Inverse-variance weighted
- ICD-10:
-
International Classification of Diseases 10th Revision
- LD:
-
Linkage disequilibrium
- IL-6:
-
Interleukin-6
- MR:
-
Mendelian randomization
- MF:
-
Myocardial infarction
- NHANES:
-
National Health and Nutrition Examination Survey
- OA:
-
Osteoarthritis
- OR:
-
Odds ratio
- PAD:
-
Peripheral arterial disease
- SNPs:
-
Single Nucleotide Polymorphisms
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- TNF-α:
-
Tumour necrosis factor alpha
- UKB:
-
UK Biobank
References
Reyes C, Leyland KM, Peat G, Cooper C, Arden NK, Prieto-Alhambra D. Association between Overweight and Obesity and risk of clinically diagnosed knee, hip, and Hand Osteoarthritis: a Population-based Cohort Study. Arthritis Rheumatol (Hoboken NJ). 2016;68(8):1869–75.
Kolasinski SL, Neogi T, Hochberg MC, Oatis C, Guyatt G, Block J, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, hip, and Knee. Volume 72. Hoboken, NJ: Arthritis & rheumatology; 2020. pp. 220–33. 2.
Zeng C, Bennell K, Yang Z, Nguyen UDT, Lu N, Wei J, et al. Risk of venous thromboembolism in knee, hip and hand osteoarthritis: a general population-based cohort study. Ann Rheum Dis. 2020;79(12):1616–24.
Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021–104.
Carey RM, Wright JT Jr., Taler SJ, Whelton PK. Guideline-Driven Management of Hypertension: an evidence-based update. Circul Res. 2021;128(7):827–46.
Lip GYH, Coca A, Kahan T, Boriani G, Manolis AS, Olsen MH et al. Hypertension and cardiac arrhythmias: a consensus document from the European Heart Rhythm Association (EHRA) and ESC Council on Hypertension, endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS) and Sociedad Latinoamericana de Estimulación Cardíaca y Electrofisiología (SOLEACE). Europace: European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2017;19(6):891–911.
Abdulrahman H, van Dalen JW, den Brok M, Latimer CS, Larson EB, Richard E. Hypertension and Alzheimer’s disease pathology at autopsy: a systematic review. Alzheimer’s Dement J Alzheimer’s Assoc. 2022;18(11):2308–26.
Oparil S, Acelajado MC, Bakris GL, Berlowitz DR, Cífková R, Dominiczak AF, et al. Hypertens Nat Reviews Disease Primers. 2018;4:18014.
Lo GH, McAlindon TE, Katz JN, Driban JB, Price LL, Eaton CB, et al. Systolic and pulse pressure associate with incident knee osteoarthritis: data from the Osteoarthritis Initiative. Clin Rheumatol. 2017;36(9):2121–8.
Niu J, Clancy M, Aliabadi P, Vasan R, Felson DT. Metabolic syndrome, its components, and knee osteoarthritis: the Framingham Osteoarthritis Study. Arthritis Rheumatol (Hoboken NJ). 2017;69(6):1194–203.
Bagge E, Bjelle A, Edén S, Svanborg A. Factors associated with radiographic osteoarthritis: results from the population study 70-year-old people in Göteborg. J Rhuematol. 1991;18(8):1218–22.
Inoue R, Ishibashi Y, Tsuda E, Yamamoto Y, Matsuzaka M, Takahashi I, et al. Medical problems and risk factors of metabolic syndrome among radiographic knee osteoarthritis patients in the Japanese general population. J Orthop Science: Official J Japanese Orthop Association. 2011;16(6):704–9.
Lee BJ, Yang S, Kwon S, Choi KH, Kim W. Association between metabolic syndrome and knee osteoarthritis: a cross-sectional nationwide survey study. J Rehabil Med. 2019;51(6):464–70.
Sananta P, Zahrah VT, Widasmara D, Fuzianingsih EN. Association between diabetes mellitus, hypertension, and knee osteoarthritis in secondary referral hospitals in Indonesia with retrospective cross-sectional study. Annals of medicine and surgery (2012). 2022;80:104155.
Li W, Zheng Q, Xu M, Zeng C, Deng X. Association between circulating 25-hydroxyvitamin D metabolites and periodontitis: results from the NHANES 2009–2012 and mendelian randomization study. J Clin Periodontol. 2023;50(2):252–64.
Min JY, Min KB. Blood cadmium levels and Alzheimer’s disease mortality risk in older US adults. Environ Health: Global Access Sci Source. 2016;15(1):69.
Ruan Z, Lu T, Chen Y, Yuan M, Yu H, Liu R, et al. Association between Psoriasis and nonalcoholic fatty liver Disease among Outpatient US adults. JAMA Dermatology. 2022;158(7):745–53.
Tao L, Miao L, Guo YJ, Liu YL, Xiao LH, Yang ZJ. Associations of body roundness index with cardiovascular and all-cause mortality: NHANES 2001–2018. Journal of human hypertension. 2023.
Li B, Chen L, Hu X, Tan T, Yang J, Bao W, et al. Association of serum uric acid with all-cause and Cardiovascular Mortality in Diabetes. Diabetes Care. 2023;46(2):425–33.
Jaddoe VW, de Jonge LL, Hofman A, Franco OH, Steegers EA, Gaillard R. First trimester fetal growth restriction and cardiovascular risk factors in school age children: population based cohort study. BMJ (Clinical Res ed). 2014;348:g14.
Tang D, Bian J, He M, Yang N, Zhang D. Research on the current Situation and countermeasures of Inpatient cost and Medical Insurance Payment Method for Rehabilitation Services in City S. Front Public Health. 2022;10:880951.
Kuppa A, Tripathi H, Al-Darraji A, Tarhuni WM, Abdel-Latif A. C-Reactive protein levels and risk of Cardiovascular diseases: a two-sample bidirectional mendelian randomization study. Int J Mol Sci. 2023;24(11).
Yu Z, Coresh J, Qi G, Grams M, Boerwinkle E, Snieder H, et al. A bidirectional mendelian randomization study supports causal effects of kidney function on blood pressure. Kidney Int. 2020;98(3):708–16.
Bottigliengo D, Foco L, Seibler P, Klein C, König IR, Del Greco MF. A mendelian randomization study investigating the causal role of inflammation on Parkinson’s disease. Brain. 2022;145(10):3444–53.
Bycroft C, Freeman C, Petkova D, Band G, Elliott LT, Sharp K, et al. The UK Biobank resource with deep phenotyping and genomic data. Nature. 2018;562(7726):203–9.
Tachmazidou I, Hatzikotoulas K, Southam L, Esparza-Gordillo J, Haberland V, Zheng J, et al. Identification of new therapeutic targets for osteoarthritis through genome-wide analyses of UK Biobank data. Nat Genet. 2019;51(2):230–6.
Staley JR, Blackshaw J, Kamat MA, Ellis S, Surendran P, Sun BB, et al. PhenoScanner: a database of human genotype-phenotype associations. Bioinf (Oxford England). 2016;32(20):3207–9.
Kurki MI, Karjalainen J, Palta P, Sipilä TP, Kristiansson K, Donner KM, et al. FinnGen provides genetic insights from a well-phenotyped isolated population. Nature. 2023;613(7944):508–18.
Zhang Y, Fan J, Chen L, Xiong Y, Wu T, Shen S, et al. Causal Association of Coffee Consumption and total, knee, hip and self-reported osteoarthritis: a mendelian randomization study. Front Endocrinol. 2021;12:768529.
Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–25.
Huang D, Lin S, He J, Wang Q, Zhan Y. Association between COVID-19 and telomere length: a bidirectional mendelian randomization study. J Med Virol. 2022;94(11):5345–53.
Long Y, Tang L, Zhou Y, Zhao S, Zhu H. Causal relationship between gut microbiota and cancers: a two-sample mendelian randomisation study. BMC Med. 2023;21(1):66.
Hemani G, Zheng J, Elsworth B, Wade KH, Haberland V, Baird D et al. The MR-Base platform supports systematic causal inference across the human phenome. eLife. 2018;7.
Veronese N, Stubbs B, Solmi M, Smith TO, Noale M, Schofield P, et al. Knee osteoarthritis and risk of hypertension: a longitudinal cohort study. Rejuven Res. 2018;21(1):15–21.
Lo K, Au M, Ni J, Wen C. Association between hypertension and osteoarthritis: a systematic review and meta-analysis of observational studies. J Orthop Translation. 2022;32:12–20.
Kendzerska T, Jüni P, King LK, Croxford R, Stanaitis I, Hawker GA. The longitudinal relationship between hand, hip and knee osteoarthritis and cardiovascular events: a population-based cohort study. Osteoarthr Cartil. 2017;25(11):1771–80.
Skou ST, Grønne DT, Roos EM. Prevalence, severity, and correlates of Pain flares in response to a repeated sit-to-stand activity: a cross-sectional study of 14 902 patients with knee and hip osteoarthritis in primary care. J Orthop Sports Phys Ther. 2020;50(6):309–18.
Robinson WH, Lepus CM, Wang Q, Raghu H, Mao R, Lindstrom TM, et al. Low-grade inflammation as a key mediator of the pathogenesis of osteoarthritis. Nat Rev Rheumatol. 2016;12(10):580–92.
Hashmat S, Rudemiller N, Lund H, Abais-Battad JM, Van Why S, Mattson DL. Interleukin-6 inhibition attenuates hypertension and associated renal damage in Dahl salt-sensitive rats. Am J Physiol Ren Physiol. 2016;311(3):F555–61.
Sabio JM. Systemic inflammation and endothelial Dysfunction-a possible link between osteoarthritis and hypertension: comment on the article by Niu et al. Arthritis Rheumatol (Hoboken NJ). 2017;69(12):2403.
Murray EC, Nosalski R, MacRitchie N, Tomaszewski M, Maffia P, Harrison DG, et al. Therapeutic targeting of inflammation in hypertension: from novel mechanisms to translational perspective. Cardiovascular Res. 2021;117(13):2589–609.
Hall E, Vrolijk MF. Androgen receptor and Cardiovascular Disease: a potential risk for the abuse of supplements containing selective androgen receptor modulators. Nutrients. 2023;15(15).
Yang D, Tian J, Zhang X, Yu J, Li S, Wang Z, et al. The polymorphic CAG repeat in exon 1 of androgen receptor is associated with level of HDL cholesterol and hypertension in Chinese middle-aged and elderly men. Clin Endocrinol. 2017;87(1):29–34.
Fytili P, Giannatou E, Papanikolaou V, Stripeli F, Karachalios T, Malizos K, et al. Association of repeat polymorphisms in the estrogen receptors alpha, beta, and androgen receptor genes with knee osteoarthritis. Clin Genet. 2005;68(3):268–77.
Yan YS, Qu Z, Yu DQ, Wang W, Yan S, Huang HF. Sex steroids and osteoarthritis: a mendelian randomization study. Front Endocrinol. 2021;12:683226.
Wen CY, Chen Y, Tang HL, Yan CH, Lu WW, Chiu KY. Bone loss at subchondral plate in knee osteoarthritis patients with hypertension and type 2 diabetes mellitus. Osteoarthr Cartil. 2013;21(11):1716–23.
Yeater TD, Griffith JL, Cruz CJ, Patterson FM, Aldrich JL, Allen KD. Hypertension contributes to exacerbated osteoarthritis pathophysiology in rats in a sex-dependent manner. Arthritis Res Therapy. 2023;25(1):7.
Acknowledgements
We extend our gratitude to UK Biobank, NHANES, the FinnGen database, and Tachmazidou et al. for publicly sharing the data that we utilized in our analysis. And thanks to Zhang Jing (Second Department of Infectious Disease, Shanghai Fifth People’s Hospital, Fudan University) for his work on the NHANES database.
Funding
This research was funded by the National Natural Science Foundation of China (82060072).
Author information
Authors and Affiliations
Contributions
Zhi-Jie Yang and Yuan Liu participated in the design, Liu Miao, Yan-Li Liu, Bin Qi and Wan-Xin Shi performed the data extracted and analyzed, Zhi-Jie Yang drafted the manuscript, Liu Miao and Xin Yuan revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study is based on publicly available summary statistics, therefore no ethical approval is required.
Consent for publication
All authors approved the final manuscript and the submission to this journal.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, ZJ., Liu, Y., Liu, YL. et al. Osteoarthritis and hypertension: observational and Mendelian randomization analyses. Arthritis Res Ther 26, 88 (2024). https://doi.org/10.1186/s13075-024-03321-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13075-024-03321-w