
Abstract
Objectives
To determine the risk factors for mortality in Korean patients with rheumatoid arthritis (RA)-associated interstitial lung disease (ILD) in comparison to patients with RA but without ILD (RA-nonILD).
Methods
Data were extracted from a single-centre prospective cohort of RA patients with a chest computed tomography scan at an academic referral hospital in Korea. Patients with RA-ILD enroled between May 2017 and August 2022 were selected, and those without ILD were selected as comparators. The mortality rate was calculated, and the causes of each death were investigated. We used Cox proportional hazard regression with Firth’s penalised likelihood method to identify the risk factors for mortality in patients with RA-ILD.
Results
A total of 615 RA patients were included: 200 with ILD and 415 without ILD. In the RA-ILD group, there were 15 deaths over 540.1 person-years (PYs), resulting in mortality rate of 2.78/100 PYs. No deaths were reported in the RA-nonILD group during the 1669.9 PYs. The primary causes of death were infection (nine cases) and lung cancer (five cases), with only one death attributed to ILD aggravation. High RA activity (adjusted HR 1.87, CI 1.16–3.10), baseline diffusing capacity for carbon monoxide (DLCO) < 60% (adjusted HR 4.88, 95% CI 1.11–45.94), and usual interstitial pneumonia (UIP) pattern (adjusted HR 5.13, 95% CI 1.00–57.36) were identified as risk factors for mortality in RA-ILD patients.
Conclusion
Patients with RA-ILD have an elevated risk of mortality compared with those without ILD. Infection-related deaths are the main causes of mortality in this population. High RA activity, low DLCO, and the UIP pattern are significantly associated with the mortality in patients with RA-ILD.
Similar content being viewed by others


Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory autoimmune disease that frequently accompanies extra-articular manifestations such as rheumatoid nodules; vasculitis; and pulmonary, cardiovascular, and haematological diseases [1, 2]. Interstitial lung disease (ILD) was first reported in 1984 [3] and is a serious complication in patients with RA that leads to increased mortality [4, 5]. Although RA-associated ILD (RA-ILD) was previously thought to be the result of prolonged RA, it is currently understood that ILD can develop throughout the course of the disease or even before RA diagnosis [5, 6]. There is a lack of evidence on the optimal treatment for patients with RA-ILD. Physicians must consider the effect of disease-modifying antirheumatic drugs (DMARDs) on ILD in patients with RA-ILD, which narrows the treatment options and makes it difficult to control RA activity [7].
Patients with RA have an elevated risk of mortality compared with the general population [8, 9]. A large population-based cohort study conducted in Korea demonstrated a total age- and sex-adjusted standardised mortality ratio of 1.65 (95% confidence interval [CI] 1.44–1.87) in patients with RA [9]. Notably, among patients with RA, those with ILD are particularly vulnerable to mortality, with ILD identified as the leading cause of death following cardiovascular disease [8]. A substantial disparity in the risk of mortality was observed between RA-ILD and RA-nonILD patients, with RA-ILD patients having a 2 to 10 times higher risk of death [4, 5]. Specifically, the hazard rate ratio peaked at 10.4 (95% CI 5.9–18.2) during the first month following RA-ILD diagnosis. Furthermore, the stratified analysis found the risk to be higher in patients diagnosed with RA prior to the development of ILD [5].
Numerous studies have focused on identifying predictors of mortality in RA-ILD patients to better understand the disease course and enhance clinical management [4, 10,11,12,13,14,15]. Demographic factors, such as older age, male sex, and smoking history, have been recognised as prognostic indicators associated with mortality in patients with RA-ILD [4, 10,11,12]. Additionally, pulmonary physiological measures, including low percentage of predicted diffusing capacity for carbon monoxide (DLCO) and low percentage of predicted forced vital capacity (FVC), have emerged as predictors of ILD progression [11,12,13,14,15]. Computed tomography (CT) findings have also been explored, with the usual interstitial pneumonia (UIP) pattern identified as a marker for poor prognosis compared to other types, such as the non-specific interstitial pneumonia (NSIP) pattern [10,11,12]. However, the impact of CT patterns on mortality remains controversial, as some studies have not found any significant difference [13, 15]. Additionally, the association between seropositivity and mortality in RA-ILD patients has yielded inconsistent results [10, 12].
Despite advancements in the management of RA-ILD, there are still significant gaps in the current understanding of this condition and optimal strategies for its management [16,17,18]. In the present study, we aimed to investigate the causes of death and identify the risk factors associated with mortality in Korean patients with RA-ILD in comparison to patients with RA but without ILD (RA-nonILD) using data from a prospective cohort.
Methods
Study population
The Hanyang University Medical Centre Arthritis Network-ILD Screening and Management (HUMANISM) cohort is a multidisciplinary prospective cohort of patients with RA at an academic referral hospital in Korea, established in May 2017 (clinicaltrials.gov NCT03099525) [19]. The HUMANISM cohort included patients aged 19 years or older, who met the 1987 American College of Rheumatology (ACR) or the 2010 ACR/European Alliance of Associations for Rheumatology (EULAR) classification criteria for RA and signed an informed consent. Additionally, patients were required to undergo a chest CT scan within the two years prior to joining the study and provide written consent. The enroled patients were assigned to either the RA-ILD or the RA-nonILD group according to the results of chest CT scans evaluated by radiologists and rheumatologists. Consensus between the radiologists and rheumatologists was reached if a disagreement in the interpretation of the chest CT scans was noted. Patients diagnosed with other autoimmune diseases (such as inflammatory myositis, systemic sclerosis, systemic lupus erythematosus, and mixed connective tissue disease) were excluded. Patients with asbestosis or a history of lobectomy, pneumonectomy, or radiation therapy were also excluded. Patients enroled in the HUMANISM cohort between May 2017 and August 2022 were included.
Data collection
Demographic and clinical information of the patients was collected at enrolment. Demographic features including age, sex, body mass index, socioeconomic status, and smoking status were obtained by interviewing the patient. Clinical characteristics included comorbidities, medication use, RA disease activity, and patient-reported outcomes, such as the Health Assessment Questionnaire-Disability Index (HAQ-DI), EuroQol-5-Dimensions questionnaire (EQ-5D), and the patient’s global assessment values. Clinical information was obtained by interviewing the participants and reviewing their medical records. Comorbidities within 3 years of enrolment were investigated, and the Charlson Comorbidity Index (CCI) score was used to assess comorbidities [20]. Connective tissue diseases were excluded from the calculation of the CCI score in this study because all patients had RA. Laboratory results, including erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), rheumatoid factor (RF), and anti-citrullinated protein antibody (ACPA) levels, were also collected. Patients in the RA-ILD group underwent chest CT scan and pulmonary function tests (PFTs). The interpretation of chest CT scans performed by radiologists and the type of ILD were determined based on the official ATS/ERS/JRS/ALAT clinical practice guidelines [21].
Annual follow-ups were conducted to investigate each participant’s clinical information in both groups, and observations were terminated if the patient died, was lost to follow-up, or reached June 2023. As this was a completely observational study, no intervention other than treatment determined by the physician in a real-world clinical setting was applied.
Statistical analyses
We compared the baseline characteristics between the RA-ILD and RA-nonILD groups using the chi-square test or Fisher’s exact test for categorical variables and the Mann–Whitney U test for continuous variables. The clinical characteristics of patients with RA-ILD, including the results of PFTs and CT findings, were described. The mortality rate was calculated as cases per 100 person-years (PYs) and the causes of death were investigated. RA-ILD and RA-nonILD mortality were visualised using the Kaplan-Meier survival curve. Cox proportional hazard regression with Firth’s penalised likelihood method, which is robust for sparse data, was performed to compare mortality between the two groups after adjusting for covariates. To identify the risk factors for mortality in patients with RA-ILD, we used Cox proportional hazard regression with Firth’s penalised likelihood. The multivariable regression model included variables that were significant in the univariable regression analysis.
All analyses were performed using SAS® 9.4 software (SAS Institute, Cary, NC, USA) or R software version 3.4.2 (R Foundation for Statistical Computing, Vienna, Austria). Missing values were excluded from the analyses without imputation, and the results were considered statistically significant when the P-value was < 0.05.
Results
Baseline characteristics of the study population
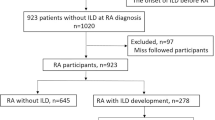
Among the 662 eligible patients with RA, patient who were not willing to or unable to participate the study were excluded (Fig. 1). The numbers of patients lost to follow-up in each group are presented in Supplementary Fig. 1 [see Additional File 1].

Flow-chart of patient selection. RA, rheumatoid arthritis; HUMANISM, Hanyang University Medical Centre Arthritis Network Interstitial Lung Disease Screening and Management; ILD, interstitial lung disease
A total of 615 patients were included in the analysis: 200 in the RA-ILD group and 415 in the RA-nonILD group. The median age of the study population was 61.2 years, and 21.3% were male patients (Table 1).
Patients in the RA-ILD group were older (66.8 years vs. 58.6 years, P < 0.001), and the proportion of male patients was higher in the RA-ILD group (34.0% vs. 15.2%, P < 0.001). There were significantly more ever-smokers in the RA-ILD group (35.5% vs. 18.6%, P < 0.001), and patients with RA-ILD had more comorbidities. Disease activity of RA estimated by the Disease Activity Score 28 (DAS28)-ESR was higher in the RA-ILD than the RA-nonILD group (3.4 vs. 3.2, P = 0.020).
For patients with RA-ILD who underwent PFTs at enrolment, the mean predicted percentage of FVC was 80.6%, and the mean predicted percentage of DLCO was 56.2% (Table 1). The median time between chest CT scans and enrolment was 91 days. Among the CT scans, the most prevalent ILD pattern observed was UIP (66.5%), consisting of definite UIP (42.1%) and probable UIP (24.4%). Patients with NSIP pattern accounted for 21.3%. Reticulation (97.5%) was the most common CT finding, followed by traction bronchiectasis (89.3%).
The medication use patterns of the two groups are presented in Table 2. Methotrexate and leflunomide were prescribed less frequently in the RA-ILD group. Tumour necrosis factor (TNF) inhibitors were used more commonly in the RA-nonILD group, whereas non-TNF inhibitors were used more in the RA-ILD group. Patients with RA-ILD were more frequently treated with higher doses of oral glucocorticoids.
Mortality and causes of death
Up until June 2023, 15 deaths occurred in the RA-ILD group during the 540.1 person-years (PYs) (median 2.6, interquartile range [IQR] 1.2–4.1 years), and the mortality rate was 2.78/100 PYs (95% CI 1.56–4.54). No deaths were observed in the RA-nonILD group during the 1669.9 PYs (median 4.2, IQR 3.6–4.9 years). The Kaplan-Meier survival curve between the RA-ILD and RA-nonILD groups is presented in Fig. 2. After adjusting for age, sex, smoking history, and baseline DAS28-ESR, the hazard ratio (HR) in the RA-ILD group was found to be significantly higher than that in the RA-nonILD group based on a Cox proportional hazard regression with Firth’s penalised likelihood method (Supplementary Table 1: adjusted HR 43.68, 95% CI 4.92–5791.23) [see Additional File 1].

Kaplan-Meier survival curves in RA patients with ILD versus nonILD. The shaded part represents the 95% confidence interval for the survival probability. Each vertical drop in the curve indicates one or more events (death). Right-censored cases are indicated by vertical marks on the curves at the censoring time. RA, rheumatoid arthritis; ILD, interstitial lung disease
The detailed characteristics of the deceased patients are presented in Supplementary Table 2 [see Additional File 1]. The most common cause of death was infection (nine cases), followed by lung cancer (five cases). Only one patient died due to ILD aggravation. All of the deceased patients had a predominant UIP pattern except one with an NSIP pattern.
Risk factors for mortality in RA patients with ILD
In the multivariable regression analysis for patients with RA-ILD, high RA activity assessed by DAS28-ESR (adjusted HR 1.87, 95% CI 1.16–3.10) and baseline DLCO < 60% of the predicted value (adjusted HR 4.88, 95% CI 1.11–45.94) were significant risk factors for mortality after adjusting for other confounding factors (Table 3). In addition, the UIP pattern (adjusted HR 5.13, 95% CI 1.00–57.36) was a marginally significant risk factor for mortality.
Discussion
In this single-centre prospective cohort study, we identified the differing characteristics between RA-ILD and RA-nonILD patients. Deaths occurred only in the RA-ILD group over 2.6 years of observation, whereas none occurred in the RA-nonILD group over the 4.2-year observation period. The most common cause of death was infection, and the risk factors for mortality among RA-ILD patients were high RA activity, baseline DLCO < 60% of the predicted value, and the UIP pattern on chest CT scan.
The characteristics of patients with RA-ILD were markedly different from those of patients with RA without ILD. The proportion of male patients was higher in the RA-ILD group than in the RA-nonILD group. Patients with RA-ILD also had more comorbidities; however, a history of pulmonary tuberculosis was more common in the RA-nonILD group. In our study, the proportion of patients with a history of pulmonary tuberculosis was high. According to a previous study on the comorbidities in Korean patients with RA, 8.6% of patients with RA had pulmonary tuberculosis [22]. In addition, our previous study revealed that the latent tuberculosis infection positivity rate was 26.5% in patients with RA initiating targeted therapy at a tertiary referral hospital in Korea [23]. The information about the history of pulmonary tuberculosis was obtained by interviewing patients in addition to reviewing medical records; therefore, the prevalence of pulmonary tuberculosis could be overestimated. Nevertheless, none of the patients had active pulmonary tuberculosis at enrolment.
One intriguing finding of this study was that deaths occurred exclusively in the RA-ILD group, which made a direct comparison of the mortality rates between the two groups not possible. However, this observation suggests a potential association between ILD and an increased risk of mortality in patients with RA. It is important to acknowledge the differences in the baseline characteristics between the two groups, such as age, smoking status, comorbidities, and RA activity, as these factors may have influenced the outcomes. Although a comprehensive analysis adjusting for these variables would provide a more accurate understanding of the impact of ILD on mortality, we were unable to conduct further analysis due to the absence of deaths in the RA-nonILD group.
The primary cause of death in this study was infection, with pneumonia being the most prevalent cases of urosepsis and biliary sepsis. Patients with RA have an increased susceptibility to infections compared to the general population. This susceptibility can be attributed to immunological dysfunction, comorbidities, and the use of immunomodulatory drugs [24]. Considering that no deaths occurred in the RA-nonILD group, RA-ILD may be a potential risk factor for developing fatal pneumonia. It is worth noting that, of the 15 deceased patients, six had received targeted therapy, and five of them had their deaths attributed to infection. This observation raises the possibility of an increased risk of infection associated with the targeted therapy. However, it is important to note the high RA disease activity levels that necessitated the use of targeted therapy in these patients.
The second most common cause of death in patients with RA-ILD was cancer, with all five cases being lung cancer. Patients with RA have an approximately 1.5-fold higher risk of developing lung cancer than the general population [25, 26]. The hypothesis is that lung cancer and RA share a common risk factor: smoking [27]. In addition, ILD is considered as a possible risk factor for lung cancer, with a recent retrospective cohort study conducted in China reporting that approximately 3% of patients with ILD were diagnosed with lung cancer [27, 28]. In our study, all five patients who died of lung cancer were smokers.
Higher RA activity and the UIP pattern were significant risk factors for mortality in patients with RA-ILD. The UIP pattern has been recognised as a poor prognostic factor compared with other patterns, such as the NSIP pattern [11, 12, 15], and our study showed similar trends. However, it is important to investigate whether the UIP pattern association with poor outcomes is truly due to an ILD flare-up or other factors, such as infection or malignancy. Further detailed analyses are required to confirm this hypothesis.
One of the risk factors for mortality in the RA-ILD group was a baseline DLCO < 60% of the predicted value. The importance of pulmonary physiology in the prognosis of patients with RA-ILD has been previously reported. According to previous studies, low baseline DLCO was related to the risk of ILD progression and mortality [12, 13, 29]. Low baseline FVC is also known to be a risk factor for mortality in patients with RA-ILD [11, 12, 15, 29]; however, this was not true in our study. PFT results correlate more significantly with the extent of lung involvement than with the ILD pattern [30]. This indicates that the importance of PFT results and CT findings may differ when evaluating the prognosis of patients with RA-ILD as individuals or in a group.
Considerations when prescribing DMARDs for patients with RA-ILD are more complex compared to those without ILD. Methotrexate is the first-line treatment recommended for patients with RA; however, its effects on ILD remain controversial [31, 32]. An inception cohort study of patients with early RA showed that methotrexate treatment reduced the risk and delayed the incidence of ILD [33]. In contrast, leflunomide is not recommended for patients with RA-ILD because of its association with an increased risk of the development and/or exacerbation of ILD [34]. However, a meta-analysis of RCTs found no evidence of increased respiratory adverse events in RA patients [35]. In our study, the proportion of patients with RA-ILD treated with methotrexate or leflunomide was significantly lower than that of RA-nonILD patients. Regarding targeted therapy, abatacept was most frequently used in the RA-ILD group and was associated with a slower deterioration of ILD and a lower risk of infection than TNF inhibitors [36, 37].
The 2023 ACR guidelines for the treatment of ILD in individuals with systemic autoimmune rheumatic disease were recently announced, and a summary was posted [38]. Mycophenolate, azathioprine, and rituximab are recommended as first-line therapies for patients with RA-ILD according to the guidelines. However, mycophenolate mofetil is not approved for patients with RA in Korea. In addition, the prescription rates for azathioprine and rituximab were low in our study. In Korea, rituximab is approved only for patients who have an inadequate response to other targeted therapies (TNF inhibitors, non-TNF inhibitors, or Janus kinase inhibitors). Our results are expected to serve as important evidence demonstrating the discrepancies between the new ACR guidelines and medication use in Korean patients with RA-ILD.
This study had several strengths. First, we used data from a well-established multidisciplinary prospective cohort. In particular, we improved the reliability of CT readings by reaching a consensus through discussions between rheumatologists and radiologists. Second, we identified the risk factors for mortality in patients with RA-ILD, which still have an unmet need for clinical studies in Korea.
This study had several limitations. First, this was a single-centre study, which could be questioned for generalisability. However, our hospital contains the largest rheumatology centre in the nation, drawing patients from across the country. In addition, more detailed information could be collected by interviewing patients directly or through medical records because the study was performed at a single institution. Second, all patients in the RA-nonILD group survived the observation period; therefore, it was not possible to compare the mortality risk between the two groups. Further studies with longer observation periods are necessary. Third, some ILD patients and the majority of nonILD patients did not undergo PFTs; therefore, we could not compare the PFT results between the two groups. However, there were only 12 patients without PFTs in the ILD group, and the number of RA-ILD patients with PFTs was considered sufficient for multivariable analysis.
In conclusion, patients with RA-ILD had an increased risk of mortality compared to RA-nonILD patients. The main causes of death were infections, especially pneumonia, and lung cancer. Risk factors for mortality in patients with RA-ILD are high RA disease activity, low baseline DLCO, and the UIP pattern. Further studies with longer observation periods are needed to clarify the increased incidence of mortality in RA-ILD patients compared to that in RA-nonILD patients.
Data availability
No datasets were generated or analysed during the current study.
References
Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet. 2016;388:2023–38.
Figus FA, Piga M, Azzolin I, et al. Rheumatoid arthritis: extra-articular manifestations and comorbidities. Autoimmun Rev. 2021;20:102776.
Ellman P, Ball RE. Rheumatoid disease with joint and pulmonary manifestations. Br Med J. 1948;2:816–20.
Bongartz T, Nannini C, Medina-Velasquez YF, et al. Incidence and mortality of interstitial lung disease in rheumatoid arthritis: a population-based study. Arthritis Rheum. 2010;62:1583–91.
Hyldgaard C, Hilberg O, Pedersen AB, et al. A population-based cohort study of rheumatoid arthritis-associated interstitial lung disease: comorbidity and mortality. Ann Rheum Dis. 2017;76:1700–06.
McDermott GC, Doyle TJ, Sparks JA. Interstitial lung disease throughout the rheumatoid arthritis disease course. Curr Opin Rheumatol. 2021;33:284–91.
Yamakawa H, Ogura T, Kameda H, et al. Decision-making strategy for the treatment of Rheumatoid Arthritis-Associated interstitial lung disease (RA-ILD). J Clin Med. 2021;10(17):3806.
Raimundo K, Solomon JJ, Olson AL, et al. Rheumatoid arthritis–interstitial lung disease in the United States: prevalence, incidence, and Healthcare costs and mortality. J Rheumatol. 2019;46:360–69.
Lee YK, Ahn GY, Lee J, et al. Excess mortality persists in patients with rheumatoid arthritis. Int J Rheum Dis. 2021;24:364–72.
Kelly CA, Saravanan V, Nisar M, et al. Rheumatoid arthritis-related interstitial lung disease: associations, prognostic factors and physiological and radiological characteristics–a large multicentre UK study. Rheumatology (Oxford). 2014;53:1676–82.
Mena-Vazquez N, Rojas-Gimenez M, Romero-Barco CM et al. Predictors of progression and mortality in patients with prevalent rheumatoid arthritis and interstitial lung disease: a prospective cohort study. J Clin Med 2021;10.
Qiu M, Jiang J, Nian X, et al. Factors associated with mortality in rheumatoid arthritis-associated interstitial lung disease: a systematic review and meta-analysis. Respir Res. 2021;22:264.
Zamora-Legoff JA, Krause ML, Crowson CS, et al. Patterns of interstitial lung disease and mortality in rheumatoid arthritis. Rheumatology (Oxford). 2017;56:344–50.
Hyldgaard C, Ellingsen T, Hilberg O, et al. Rheumatoid arthritis-Associated interstitial lung disease: clinical characteristics and predictors of Mortality. Respiration. 2019;98:455–60.
Solomon JJ, Chung JH, Cosgrove GP, et al. Predictors of mortality in rheumatoid arthritis-associated interstitial lung disease. Eur Respir J. 2016;47:588–96.
England BR, Hershberger D. Management issues in rheumatoid arthritis-associated interstitial lung disease. Curr Opin Rheumatol. 2020;32:255–63.
Matson SM, Baqir M, Moua T, et al. Treatment outcomes for Rheumatoid Arthritis-Associated interstitial lung disease: a Real-World, Multisite Study of the impact of immunosuppression on pulmonary function trajectory. Chest. 2023;163(4):861–69.
Flaherty KR, Wells AU, Cottin V, et al. Nintedanib in progressive interstitial lung diseases: data from the whole INBUILD trial. Eur Respir J. 2022;59(3):2004538.
Kim H, Cho SK, Song YJ, et al. Clinical characteristics of rheumatoid arthritis patients with interstitial lung disease: baseline data of a single-center prospective cohort. Arthritis Res Ther. 2023;25:43.
Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–83.
Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2018;198:e44–68.
Jeong H, Baek SY, Kim SW, et al. Comorbidities of rheumatoid arthritis: results from the Korean National Health and Nutrition Examination Survey. PLoS ONE. 2017;12:e0176260.
Song YJ, Cho SK, Kim H. Risk of Tuberculosis Development in patients with rheumatoid arthritis receiving targeted therapy: a prospective single Center Cohort Study. J Korean Med Sci. 2021;36(10):e70.
Listing J, Gerhold K, Zink A. The risk of infections associated with rheumatoid arthritis, with its comorbidity and treatment. Rheumatology (Oxford). 2013;52:53–61.
Simon TA, Thompson A, Gandhi KK, et al. Incidence of malignancy in adult patients with rheumatoid arthritis: a meta-analysis. Arthritis Res Ther. 2015;17:212.
Wu X, Peng H, Wen Y, et al. Rheumatoid arthritis and risk of lung cancer: Meta-analysis and mendelian randomization study. Semin Arthritis Rheum. 2021;51:565–75.
Fragoulis GE, Chatzidionysiou K. Lung cancer in rheumatoid arthritis. Is there a need for better risk assessment and screening? Clin Rheumatol. 2020;39:957–61.
Fu Q, Wang L, Li L, et al. Risk factors for progression and prognosis of rheumatoid arthritis-associated interstitial lung disease: single center study with a large sample of Chinese population. Clin Rheumatol. 2019;38:1109–16.
Zamora-Legoff JA, Krause ML, Crowson CS, et al. Progressive decline of lung function in Rheumatoid Arthritis-Associated interstitial lung disease. Arthritis Rheumatol. 2017;69:542–49.
Arcadu A, Byrne SC, Pirina P, et al. Correlation of pulmonary function and usual interstitial pneumonia computed tomography patterns in idiopathic pulmonary fibrosis. Respir Med. 2017;129:152–57.
Smolen JS, Landewe RBM, Bijlsma JWJ, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79:685–99.
Fraenkel L, Bathon JM, England BR, et al., et al. 2021 American College of Rheumatology Guideline for the treatment of rheumatoid arthritis. Arthritis Care Res (Hoboken). 2021;73:924–39.
Kiely P, Busby AD, Nikiphorou E, et al. Is incident rheumatoid arthritis interstitial lung disease associated with methotrexate treatment? Results from a multivariate analysis in the ERAS and ERAN inception cohorts. BMJ Open. 2019;9:e028466.
Sawada T, Inokuma S, Sato T, et al. Leflunomide-induced interstitial lung disease: prevalence and risk factors in Japanese patients with rheumatoid arthritis. Rheumatology (Oxford). 2009;48:1069–72.
Conway R, Low C, Coughlan RJ, et al. Leflunomide Use and Risk of Lung Disease in Rheumatoid Arthritis: a systematic literature review and metaanalysis of Randomized controlled trials. J Rheumatol. 2016;43:855–60.
Vicente-Rabaneda EF, Atienza-Mateo B, Blanco R, et al. Efficacy and safety of abatacept in interstitial lung disease of rheumatoid arthritis: a systematic literature review. Autoimmun Rev. 2021;20:102830.
Chen SK, Liao KP, Liu J, et al. Risk of hospitalized infection and initiation of Abatacept Versus Tumor necrosis factor inhibitors among patients with rheumatoid arthritis: a propensity score-matched cohort study. Arthritis Care Res (Hoboken). 2020;72:9–17.
American College of Rheumatology. Interstitial lung disease guideline. https://rheumatology.org/interstitial-lung-disease-guideline. Accessed 9 Apr 2024.
Acknowledgements
We would like to thank Editage (www.editage.co.kr) for English language editing.
Funding
The establishment of the HUMANISM cohort was supported by Bristol-Myers Squibb and JW Pharmaceuticals. This research was supported by a grant of the Korea Health Technology R&D Project through the Patient-Doctor Shared Decision Making Research centre (PDSDM), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HV23C1762).
Author information
Authors and Affiliations
Contributions
Y-JS, HK, S-KC, and Y-KS contributed to the study design. Y-JS, HK, S-KC, C-BC, T-HK, J-BJ, S-CB, D-HY, S-JH, S-JY, and Y-KS contributed to data acquisition. H-WK, CL, and EN conducted statistical analysis. Y-JS, S-KC, H-WK, CL, EN, and Y-KS interpreted the results. S-KC and Y-KS acquired funding for this study. YJS, HK, and YKS drafted the manuscript. All the authors contributed to the revision of the manuscript and approved the final version. Y-KS accepts full responsibility as the guarantor of this study.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study complied with the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of Hanyang University Hospital (IRB no. HYUH 2016-06-019). Written informed consent was obtained from all patients at the time of enrolment.
Consent for publication
Not applicable.
Competing interests
DHY has received research grants from Celltrion, served as a consultant for Celltrion and is a member of the Speakers’ Bureau of Celltrion and Celltrion Healthcare. YKS has received research grants from Bristol-Myers Squibb, Eisai, Pfizer, and JW Pharmaceuticals. The authors declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Song, YJ., Kim, H., Cho, SK. et al. Risk factors of mortality in patients with rheumatoid arthritis-associated interstitial lung disease: a single-centre prospective cohort study. Arthritis Res Ther 26, 137 (2024). https://doi.org/10.1186/s13075-024-03362-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13075-024-03362-1