
Abstract
Background
The use of peripherally inserted central venous catheters (PICCs) has increased worldwide in the last decade. However, PICCs are associated to catheter-related thrombosis (CRT) and central line-associated bloodstream infections (CLABSIs). We describe the characteristics of patients requiring a PICC, estimate the incidence rate, and identify potential risk factors of PICC-related complications.
Methods
All adult patients requiring a PICC at our institution (Fundación Santa Fe de Bogotá, Bogota, Colombia) from September 2022 to May 2024 were included in the analysis. The database from active PICC monitoring collected demographic and PICC-related information. The incidence rate of CLABSI and CRT, and crude odds ratios (cORs) were estimated.
Results
Overall, 1936 individuals were included in the study. The median age was 67 years (IQR: 50–78 years), and 51.5% were females. The median duration of PICC lines was 10 days (IQR: 4–17). Seventy-nine patients had catheter-related complications, mostly in the Intensive Care Unit (ICU). The CLABSI and CRT institutional incidence rates per 1000 catheter-days were 2.03 (2.96 in the ICU) and 0.58 (0.61 in the ICU), respectively. Prolonged catheter use (≥ 6 days), PICC insertion in the intensive care unit, and postoperative care after cardiac surgery were identified as potential risk factors for CLABSI, while a catheter insertion into the brachial vein was associated with CRT.
Conclusion
Daily PICC assessment, particularly in patients with prolonged catheter use, PICC insertion into the brachial vein, or in postoperative care after cardiac surgery may significantly reduce CLABSI and CRT cases. Implementing Vascular Access Teams, venous catheter care bundles, and institutional insertion protocols optimize clinical outcomes.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Vascular access is key in the clinical management of nearly all patients attending healthcare facilities, particularly in inpatient and Intensive Care Unit (ICU) settings. Among the diversity of catheterization options, peripherally inserted central catheters (PICCs), a subset of central venous catheters (CVCs), are an appealing option for oncological patients, those with limited peripheral access, and ICU patients. Unlike other CVCs, PICCs are easier to insert and have fewer morbidity complications [1, 2]. Similarly, compared to peripheral venous catheters, PICCs can be used to administer irritant, hyperosmolar, and extreme pH drugs or solutions, and medications for several weeks or months. Despite their advantages, PICCs are not exempt from complications, with catheter-related thrombosis (CRT) and central line-associated bloodstream infections (CLABSIs) being the most common [3]. In this study, we would like to share our experience inserting PICC lines in our institution by describing the characteristics of adult patients requiring a PICC, estimating the incidence rate, and identifying potential risk factors for PICC-related complications in our institution from September 2022 to May 2024.
Methods
Data
All adult patients (≥ 18 years) requiring a PICC at our institution (Fundación Santa Fe de Bogotá, Bogota, Colombia) were included in the analysis. Data were obtained from an institutional database that monitors all PICCs inserted in both the inpatient and outpatient settings. This database collects demographic and PICC-related information, including catheter and vein diameter, site of catheter insertion, number of venipuncture attempts, catheter days, PICC-related complications, and indications for PICC removal. CLABSI were identified according to the Centers for Disease Control and Prevention definition [4]. CRT included both superficial and deep vein venous thrombosis cases. The data are gathered by the Institutional Vascular Access Team—an ICU initiative formulated as a standard of care—which has been extended to the whole institution. The team includes physicians and nurses trained in PICC insertion using ultrasound guidance.
PICC insertion
The PICC insertion technique is based on the recommendations of the Safe Insertion of PICCs (SIP) protocol [5], which includes the following steps:
-
1.
Patient Preparation: The procedure is explained to the patient and informed consent is obtained.
-
2.
Vein Selection: A suitable vein is selected for catheter insertion, usually in the arm. The basilic vein is preferred, but the brachial vein may be used if the basilic vein’s diameter is less than 3 mm.
-
3.
Ultrasound Scanning: Venous flow is confirmed through pulsed Doppler.
-
4.
Catheter Size: A 1 Fr catheter corresponds to a diameter of approximately 0.33 mm. Therefore, a 3 Fr catheter has a diameter of about 1 mm, a 4 Fr catheter about 1.33 mm, and so on. Ideally, the catheter to vein diameter ratio should be 1:3 (33%).
-
5.
Skin Disinfection: The skin at the insertion site is disinfected with a 2% chlorhexidine solution.
-
6.
Catheter Insertion: Guided by ultrasound to minimize the risk of complications.
-
7.
Measurement of Catheter Insertion Distance: From the puncture site to the mid-clavicular line, add 10 cm if on the right side, 13 cm if on the left.
-
8.
Advancement of the Catheter: The catheter is advanced to a central vein such as the superior vena cava.
-
9.
Confirmation of Catheter Position: The final catheter tip position is confirmed through two safety checks involving the subclavian and internal jugular veins.
-
10.
Catheter Fixation: Using sutureless stabilization devices, the catheter is secured, and the exit site protected.
-
11.
Follow-up: Monitored daily by the vascular access group, noting any early signs of local infection or potential complications.
These steps may vary slightly depending on specific hospital practices and individual patient needs (see Fig 1).

Steps for the insertion of a peripherally inserted central venous catheter using the ultrasonographic technique
Statistical analysis
Categorical variables were reported as frequencies and proportions. The normality of continuous variables was assessed using the Shapiro-Wilk test. Normally distributed variables are presented as means and standard deviations, and non-normally distributed variables as medians and interquartile ranges. The incidence rate of catheter-related complications was estimated for each complication (CLABSI, CRT, malposition/migration, malfunction, and occlusion) using the total number of patient days (catheter days) as the denominator. Crude odds ratios (cORs) and their 95% confidence intervals (CI) were estimated after performing a univariate analysis using the chi-square test. Statistical analyses were performed using STATA 17.0 (College Station, Texas, USA).
Results
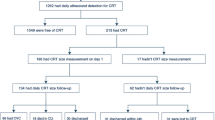
Between September 2022 and May 2024, 1936 PICCs were inserted in our institution. The patients’ median age was 67 years (IQR: 50–78 years), and the proportion of female patients (51.5%) was slightly higher than that of male patients. Almost 40% of patients were diagnosed with sepsis, followed by cerebrovascular disease (10.7%), and most PICC lines were inserted in the ICU (57.7%). The main indication for PICC insertion was the administration of vesicant/irritant drugs (66.7%). Seventy-nine patients had catheter-related complications, with CLABSI and CRT being the most common. Thirty-nine out of fifty-nine CLABSI cases and half of the CRT cases were reported in the ICU. The median duration of the PICC lines was 10 days (IQR: 4–17) (Table 1).
The CLABSI incidence rate per 1000 catheter-days was 2.03 at the institutional level and 2.96 in the ICU. The CRT incidence rates were lower compared to CLABSI, at 0.58 and 0.61 per 1000 catheter-days at the institutional and ICU levels, respectively.
Evidence from these data shows that patients with prolonged catheter use (≥ 19 days) are 34.2 times more likely (95% CI: 4.60-254.4; p-value = 0.001) to develop a CLABSI than patients with short-term catheter use (0–5 days). Likewise, patients with a catheter use between 6 and 10 days and those between 11 and 18 days are 12.4 (95% CI: 1.57–98.5; p-value = 0.02) and 26.7 (95% CI: 3.56–200.1; p-value = 0.001) more likely to develop a CLABSI than patients with short-term catheter use, respectively.
Additionally, patients in postoperative care after cardiac surgery are 6.61 times more likely (95% CI: 2.62–16.7; p-value = < 0.001) to develop a CLABSI than patients diagnosed with sepsis. PICC insertion in the ICU is more likely to develop a CLABSI compared to insertion in the general ward or the emergency room, while patients 80 years old and over are less likely to develop a CLABSI than patients between 18 and 39 years (Table 2).
On the contrary, no associations were identified between demographic, clinical, and PICC-related variables, and CRT. There is evidence (cOR: 3.42; 95% CI: 1.16–10.1; p-value = 0.03) suggesting that patients with PICCs inserted into the brachial vein are more likely to develop CRT than patients with PICCs inserted into the basilic vein (Table 1).
Discussion
Central venous access is crucial in various scenarios and for multiple purposes, such as hemodynamic monitoring, administering medications with acidic or alkaline solutions (e.g., antibiotics), providing vasopressor support, or using hyperosmolar solutions via parenteral routes that exceed 800 mOsm/L [6, 7]. , however, CVCs have been associated with potentially fatal complications such as pneumothorax, bloodstream infections, and thrombosis [8]. Over the last 10 years, the practice of inserting PICCs has evolved, some evidence is controversial regarding complications related to PICC catheters versus CVCs, even so, it has been demonstrated that following good practices for inserting peripherally inserted central venous catheters reduces complications related to thrombotic events or CLASBI compared to central venous catheters [9]. Reports indicate a reduction in complications associated with central catheter insertion after implementing vascular access teams [10, 11]. In a survey designed to assess perceptions and decision-making patterns regarding vascular access in ICUs of 13 centers, it was found that evidence-based practices are followed inconsistently and vary according to the device, training status, ICU situation, and hospital size. Additionally, 59% of the centers did not have written guidelines or protocols on the appropriate type of vascular access for ICU patients. Likewise, having local vascular access guidelines and protocols was associated with improved adherence to certain evidence-based practices [12]. It has also been suggested that the use of PICC over CVC reduces costs for specialized vascular access equipment [13], highlighting the importance of generating institutional groups specialized in the insertion, follow-up, and active monitoring of vascular access. This aligns with our findings, and to our knowledge, our cohort is the largest related to an ultrasound-guided vascular access team trained from the ICU to support the entire hospital.
Our study shows a low incidence rate of PICC-related complications (CLABSI and CRT) and the risk factors related to these complications. Considering CRT, a meta-analysis aimed at identifying the incidence of thromboembolic events associated with the use of PICC in hospitalized patients, including those in the ICU, found an incidence of 3.7% of symptomatic deep vein thrombosis, with a higher incidence in critically ill patients (10.6%) [14]. CRT is associated with the catheter diameter ratio, the size of the catheter, and the location of the central line tip. A lower catheter-to-vein ratio and a smaller catheter diameter result in reduced impact on vein flow, decreasing the subsequent risk of thrombosis. In our practice, a catheter-to-vein ratio < 33% is encouraged (262 patients in our study surpassed that limit). In addition, implementing general ward and ICU protocols (Additional file 2: Fig. S2, Additional file 3: Fig. S3) to choose venous access devices might explain our findings. However, it should be noted that in our group, we do not actively search for asymptomatic thrombosis, which has been shown to have higher incidences in patients with PICCs, especially in superficial veins, particularly in the first 2 weeks after device insertion. It is also identified as a risk factor for CRT the low venous flow rates, which, as mentioned previously, is closely related to the catheter-vein ratio, and in most of our patients had a ratio of less than 1:3. We found no differences between left vs. right basilic vein puncture as a risk factor, which has been previously described as a risk factor for asymptomatic CRT (meta-analysis of asymptomatic DVT) [3]. Nevertheless, adherence to pharmacological antithrombotic prophylaxis could modify these results, the data of which are beyond the scope of this study. The adoption of evidence-based interventions, such as ultrasound-guided vein puncture [15], micro-introducers, novel materials, and sutureless securement devices [16] has also been shown to reduce PICC-related complications.
Regarding CLABSI previous evidence, a meta-analysis reported that patients with a PICC line have a lower CLABSI incidence (2.12 per 1000 catheter days) than those with CVCs (4.09 per 1000 catheter days), indicating a 48% lower risk of CLABSI in patients with PICCs [9]. We report similar incidence of CLABSI cases, most occurring in the ICU. Our findings might be attributed to daily follow-up strategies, which actively monitored all vascular accesses to identify early signs of local infection and constantly reassessed the catheter need.
The median number of catheter days was 10, which aligns with the Michigan Appropriateness Guide for Intravenous Catheters [17]. This guide recommends that PICC catheters should not be used in patients with a predicted duration of use below 6 days unless there are no other suitable vascular access options. Among the 605 patients with a PICC duration of less than 6 days, 72.9% were patients who were discharged, transferred to another institution, or died. The remaining patients required the PICC due to vesicant/irritant medications or parenteral nutritional administration or had limited vascular access.
The generalizability of these results is subject to certain limitations. For instance, the number of complications was low, which made unfeasible to perform a logistic regression model. Therefore, it is unknown if the identified risk factors are indeed risk factors or confounders, mediators, or effect modifiers. A longer study period or a multicentric study including a larger number of patients is required to perform multivariate analyses.
This study contributes to the safety profile evidence regarding the insertion and maintenance of PICCs. Following standard insertion guidelines, daily catheter routine care, and timely PICC removal should be implemented in institutions—particularly in ICUs—that regularly use PICCs to reduce the frequency of catheter changes and, most importantly, the number of catheter-related complications.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CI:
-
Confidence interval
- CLABSI:
-
Central line-associated bloodstream infections
- cOR:
-
Crude odds ratio
- CRT:
-
Catheter related thrombosis
- CVC:
-
Central venous catheter
- ICU:
-
Intensive care unit
- IQR:
-
Interquartile range
- PICC:
-
Peripherally inserted central catheter
- SIP:
-
Safe Insertion of PICCs
References
Pitiriga VC, Bakalis J, Campos E, Kanellopoulos P, Sagris K, Saroglou G et al (2024) Central venous catheters versus peripherally inserted Central catheters: a comparison of Indwelling Time resulting in colonization by Multidrug-Resistant Pathogens. Antibiotics 13(1):89
Grau D, Clarivet B, Lotthé A, Bommart S, Parer S (2017) Complications with peripherally inserted central catheters (PICCs) used in hospitalized patients and outpatients: a prospective cohort study. Antimicrob Resist Infect Control 6(1):18
Chen P, Zhu B, Wan G, Qin L (2021) The incidence of asymptomatic thrombosis related to peripherally inserted central catheter in adults: a systematic review and meta-analysis people’s. Nurs Open 8(5):2249–2261
Wright MO, Decker SG, Allen-Bridson K, Hebden JN, Leaptrot D (2018) Healthcare-associated infections studies project: an American Journal of Infection Control and National Healthcare Safety Network data quality collaboration: location mapping. Am J Infect Control 46(5):577–578
Brescia F, Pittiruti M, Spencer TR, Dawson RB (2022) The SIP protocol update: eight strategies, incorporating Rapid Peripheral Vein Assessment (RaPeVA), to minimize complications associated with peripherally inserted central catheter insertion. J Vasc Access. ;112972982210998
Timsit JF, Tabah A, Mimoz O (2022) Update on prevention of intra-vascular accesses complications. Intensive Care Med 48(10):1422–1425
Stolz A, Efendy R, Apte Y, Craswell A, Lin F, Ramanan M (2022) Safety and efficacy of peripheral versus centrally administered vasopressor infusion: a single-centre retrospective observational study. Aust Crit Care 35(5):506–511
Parienti JJ, Mongardon N, Mégarbane B, Mira JP, Kalfon P, Gros A et al (2015) Intravascular complications of central venous catheterization by insertion site. N Engl J Med 373(13):1220–1229
Schears GJ, Ferko N, Syed I, Arpino JM, Alsbrooks K (2021) Peripherally inserted central catheters inserted with current best practices have low deep vein thrombosis and central line–associated bloodstream infection risk compared with centrally inserted central catheters: a contemporary meta-analysis. J Vasc Access 22(1):9–25
García-Zambrano L, Morales-Gómez D, Dennis-Halley MJ, Román-Ortega CF, Cabrera-Rivera PA, Parra M (2023) Making a difference? A retrospective review of peripherally inserted central catheters: a single-center experience in Colombia. SAGE Open Med 11:20503121231201349
Yu B, Hong J (2022) Safety and Efficacy of peripherally inserted Central Catheter Placement by Surgical Intensivist–Led Vascular Access Team. Vasc Spec Int 38:41
Govindan S, Jobe A, O’Malley ME, Flanders SA, Chopra V (2021) To PICC or not to PICC? A cross-sectional survey of vascular access practices in the ICU. J Crit Care 63:98–103
Comas M, Domingo L, Jansana A, Lafuente E, Civit A, García-Pérez L et al (2022) Cost-effectiveness analysis of peripherally inserted Central catheters Versus Central venous catheters for in-Hospital Parenteral Nutrition. J Patient Saf 18(7):e1109–e1115
Puri A, Dai H, Giri M, Wu C, Huang H, Zhao Q (2022) The incidence and risk of venous thromboembolism associated with peripherally inserted central venous catheters in hospitalized patients: a systematic review and meta-analysis. Front Cardiovasc Med 9:917572
Parkinson R, Gandhi M, Harper J, Archibald C (1998) Establishing an ultrasound guided peripherally inserted central catheter (PICC) insertion service. Clin Radiol 53(1):33–36
Karpanen TJ, Casey AL, Whitehouse T, Timsit JF, Mimoz O, Palomar M et al (2019) A clinical evaluation of two central venous catheter stabilization systems. Ann Intensive Care 9(1):49
Chopra V, Flanders SA, Saint S, Woller SC, O’Grady NP, Safdar N et al (2015) The Michigan Appropriateness Guide for Intravenous catheters (MAGIC): results from a Multispecialty Panel using the RAND/UCLA Appropriateness Method. Ann Intern Med 163(6Supplement):S1–40
Ministerio de Salud. Resolución 8430 de 1993 [Internet]. Bogotá: Ministerio de Salud; Oct 4 (1993) p 1–19. https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/RESOLUCION-8430-DE-1993.PDF
Acknowledgements
We would like to thank to the Institutional Vascular Access Team at Fundación Santa Fe de Bogotá for providing the PICC database require to conduct this study. We are also grateful to the clinicians in our intensive care unit for their contributions, suggestions, and encouragement.
Funding
This research received no specific grant or funding from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception and design of the study. The Institutional Vascular Access Team collected the data. AFYV and AFMS prepared the database. AFYV and AFMS performed the statistical analysis. All authors interpreted the data and results AFYV, JLMA, and AFMS wrote the final manuscript. All authors contributed to the critical revision of the manuscript. All the authors reviewed this final manuscript version and agreed on its publication. All the authors have agreed both to be personally accountable for the results and conclusions of this study.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee at the Fundación Santa Fe de Bogotá (CCEI-16180-2024) and conducted according to the declaration of Helsinki. According to the Colombian legislation, this study is considered as a ‘research without risk’ since we did not perform any experimental intervention in the patients and the data was collected retrospectively [18].
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Oviedo-Torres, M.A., Yepes-Velasco, A.F., Moreno-Araque, J.L. et al. Experience of a vascular ultrasound-guided program: from the ICU to the hospital. Ultrasound J 16, 43 (2024). https://doi.org/10.1186/s13089-024-00393-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13089-024-00393-2