
Abstract
Background
Nonalcoholic fatty liver disease (NAFLD) involves excessive liver fat accumulation and is closely linked to oxidative stress, which contributes to liver inflammation and damage. This study aimed to evaluate how interventions such as resistance training (RT) and vitamin E supplementation (VES) can modulate markers of NAFLD and key proteins regulating glucose and lipid metabolism, such as C1Q/TNF-related proteins (CTRPs).
Methods
Forty participants with NAFLD (mean age: 32.4 ± 8.2 years) were randomly assigned to one of four groups for 12 weeks: placebo (PLB), VES, PLB + RT, and VES + RT. VES was administered at 800 IU/day in a double-blind manner. The RT regimen included eight exercises at 60–80% of one-repetition maximum (1RM), with three sets of 8–12 repetitions, performed three times per week. Pre- and post-intervention assessments included body composition, aspartate aminotransferase (AST), alanine aminotransferase (ALT), lipid profile, glycemic control, CTRP-2, CTRP-9, and 1RM evaluations.
Results
Following the interventions, there was a significant improvement in body composition, lipid profile, glycemic control, and 1RM indices in the exercise groups compared to non-exercise groups (p < 0.05). AST and ALT levels decreased in all groups (p < 0.05) compared to the PLB group. There was also a significant difference between the VES + RT group and both the VES and PLB + RT groups (p < 0.05). CTRP-2 and CTRP-9 levels decreased in the exercise groups compared to non-exercise groups (p < 0.05), and their changes showed a marked correlation with body composition, lipid profile, and glycemic control indices (p < 0.05).
Conclusions
This study highlights the benefits of RT on various health parameters among NAFLD patients. While adding VES to RT resulted in greater decreases in aminotransferases, it did not provide further improvements in other variables. Additionally, enhancements in body composition, lipid profile, and glycemic control indices were possibly associated with decreased levels of CTRPs.
Trial registration
Registered retrospectively in the Iranian Registry of Clinical Trials (IRCT20220601055056N1) on December 21, 2023. Access at https://irct.behdasht.gov.ir/trial/69231.
Similar content being viewed by others

Background
Nonalcoholic fatty liver disease (NAFLD) is characterized by the accumulation of excess fat in hepatocytes (steatosis) in the absence of significant alcohol consumption or other chronic liver diseases [1]. Inflammation, hepatocyte damage, and apoptosis are hallmarks of NAFLD, potentially leading to severe complications such as cirrhosis and liver cancer [2]. Various factors contribute to the development and progression of NAFLD, including increased abdominal fat, insulin resistance (IR), hypertension, abnormal lipid levels, aging, and low physical activity [3]. The multihit hypothesis posits that IR is the primary driver of NAFLD, resulting in increased absorption and synthesis of free fatty acids (FFAs) and subsequent steatosis [4].
Additionally, markers such as lipid profile, aspartate aminotransferase (AST), and alanine aminotransferase (ALT) play crucial roles in assessing NAFLD severity and prognosis [5]. The atherogenic index of plasma (AIP), derived from the logarithmic ratio of triglycerides (TG) to high-density lipoprotein (HDL), has emerged as a potential diagnostic marker for NAFLD [6]. The AIP, body mass index (BMI), and ALT level constitute a simple screening and management model for NAFLD [7]. The global prevalence of NAFLD has increased in tandem with the increase in metabolic syndrome (MetS), obesity, and diabetes, affecting approximately one-quarter of the global population [8]. Current estimates suggest a prevalence ranging from 23 to 32%, with projections indicating global escalation [9].
C1Q/TNF-related proteins (CTRPs) constitute a family of 15 members with diverse roles in lipid and carbohydrate metabolism regulation [10]. CTRP-2, which shares 42% amino acid similarity with the globular C1q domain of adiponectin, is predominantly expressed in adipose tissue [11]. Studies in leptin-deficient ob/ob mice indicate that upregulated CTRP-2 expression mitigates severe IR and obesity development [12]. Compared with control mice, CTRP-2-overexpressing transgenic mice exhibit improved lipid tolerance and enhanced insulin sensitivity (IS) [13]. CTRP-9, with 54% similarity to the globular C1q domain of adiponectin, is abundantly expressed in adipose tissue [14]. Overexpression of CTRP-9 in ob/ob mice significantly reduces blood glucose and insulin levels [15]. Conversely, CTRP-9 deficiency in mice results in increased body weight (BW), food intake, and appetite stimulation, leading to liver steatosis and IR [16, 17]. Inducing CTRP-9 production may therefore be a promising approach for alleviating hepatic steatosis [14].
Lifestyle modification forms the cornerstone of NAFLD management, targeting BW control and metabolic disorders [2]. Both aerobic (AT) and resistance training (RT) have been shown to reduce hepatic steatosis in NAFLD patients [18]. RT, in particular, offers metabolic benefits with lower energy expenditure, making it feasible for individuals with lower cardiorespiratory fitness levels who may not tolerate AT [19, 20]. Zelber-Sagi et al. (2014) demonstrated significant reductions in steatosis and improvements in body composition following three months of RT in NAFLD patients [21]. Despite lifestyle modifications, medical treatment may be necessary for some patients, particularly those with advanced disease [2]. Increased oxidative stress (OS) and impaired antioxidant defense mechanisms are implicated in NAFLD progression, leading to antioxidant treatments such as vitamin E [2, 22]. Sanyal et al. (2010) reported significant improvements in steatosis, inflammation, and the resolution of NASH symptoms following 96 weeks of vitamin E supplementation (VES; 800 IU/day) in nondiabetic, noncirrhotic NAFLD patients [23].
The primary objective of this study was to therefore assess changes in aminotransferases, CTRP-2, CTRP-9, and IR following 12 weeks of RT combined with VES in males with NAFLD. Additionally, the study evaluated the effects of these interventions on body composition, metabolic components, and muscle strength.
Materials and methods
Study design and participants
This randomized, double-blind, placebo-controlled trial utilized a 2 × 4 factorial design and was conducted from October 2022 to March 2023. The study population consisted of participants diagnosed with NAFLD confirmed by ultrasonography [24]. The inclusion criteria were individuals aged 18–45 years with a BMI ranging from 25 to 40 kg/m2. Exclusion criteria encompassed diabetes, cirrhosis, hepatitis, hemochromatosis, Wilson’s disease, acquired immunodeficiency syndrome, prostate diseases, consumption of ≥ 30 g of alcohol/day for three consecutive months, use of drugs known to increase aminotransferases, regular sports activity in the three months prior to the study [25], and joint-muscular injuries or cardiorespiratory and renal conditions.
The sample size calculation was performed using Eq. 1 [26,27,28,29], with a significance level set at 0.05 and a statistical power of 80%. This calculation utilized the standard deviation (σ) of the primary research variable, as reported in previous studies, with CTRP-9 identified as the primary variable [30]. The target difference (D) was estimated based on the researcher’s predictions regarding the variable’s results.
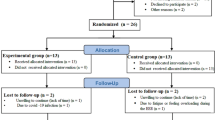
Each of the four groups required 10 individuals, totaling 40 participants. They were randomly assigned to one of the following groups: placebo (PLB), VES, PLB + RT, and VES + RT (Tables 1 and Fig. 1). Randomization was conducted using a simple method with numbered opaque sealed envelopes, as described by Doig and Simpson [31]. In summary, forty standard-size sheets of paper were divided into four categories, each containing ten papers labeled with the intervention types. The papers were folded, placed in sealed envelopes, shuffled for randomization, and assigned a number from 1 to 40. Participants were allocated to their intervention groups based on their recruitment sequence. Both participants and researchers were blinded to the type of supplements consumed after assignment to the interventions. Participants were instructed to maintain their regular dietary habits, and there were no significant differences in baseline characteristics among the four groups. All participants provided written informed consent after being briefed on the study’s methods and objectives. The study protocol was approved by the Research Ethics Committee of Razi University of Kermanshah (IR.RAZI.REC.1401.030) and registered with the Iranian Registry of Clinical Trials (IRCT20201129049525N1)”.This study was also adhered to CONSORT guidelines.

Flowchart of trial participants. One participant each from the PLB, VES, and VES + RT groups withdrew due to personal issues, irregular supplement consumption, and irregular participation in exercise sessions, respectively. PLB: Placebo; VES: Vitamin E Supplementation; RT: Resistance Training
Ultrasound evaluations
NAFLD diagnosis was confirmed via ultrasound at the Bustan Clinic in Kermanshah. Participants fasted for at least eight hours prior to assessment, and results were interpreted by a specialist using the MyLab Eight ultrasound system (Esaote, Italy). Diagnosis relied on liver parenchymal echogenicity and visualization of vessels and the diaphragm [32].
Body composition evaluations
Body composition Evaluations followed the American College of Sports Medicine (ACSM) [33] guidelines at the Sports Sciences Laboratory of Razi University while participants were fasting. Height was measured with a stadiometer (Seca, Germany). Weight and body fat percentage (BFP; via bioelectrical impedance) was recorded using the Zeus 9.9 body composition evaluation device (Jawon Medical, South Korea). Abdominal and hip circumferences were measured using a tape measure and the waist-to-hip ratio (WHR) was calculated accordingly.
Biochemical evaluations
Blood samples (5 ml) were obtained from the right brachial vein following a 12-hour fast and centrifuged at 1500 g for 15 min. Subsequently, serum levels of AST, ALT, TG, HDL, LDL, total cholesterol (TC), and glucose were determined via standardized enzymatic assays on an automated analyzer (Hitachi, Japan) with Pars Azmoun kits (Pars Azmoun, Iran). Serum insulin levels were assessed via ELISA according to manufacturers instructions (Monobind, USA), with a sensitivity of 0.75 µIU/ml and a measurement range of 0.75-25 µIU/ml. CTRP-2 and CTRP-9 serum levels were measured via ELISA according to manufacturers instructions (BT LAB, China), with sensitivities of 0.26 ng/ml and 1.15 ng/L, respectively, and measurement ranges of 0.56-36 ng/ml and 2-600 ng/L, respectively. Additionally, AIP, homeostasis model assessment of IR (HOMA-IR), and quantitative IS check index (QUICKI) were calculated using previously published protocols [34, 35].
Therapeutic interventions
Supplementation
Participants received supplements in a double-blind manner. The VES and VES + RT groups were administered a daily dose of 800 IU dl-alpha-tocopherol, divided into two 400 IU doses with lunch and dinner [36]. Conversely, the PLB and PLB + RT groups received two gelatin capsules containing edible paraffin, resembling the appearance of vitamin E capsules. Participants in both groups were instructed to maintain consistent physical activity levels throughout the study. Compliance with the vitamin E and placebo regimens was monitored every four weeks through participant-recorded sheets, with adherence to supplementation exceeding 90% of the total supplementation days. The supplementation period lasted for 12 weeks, and both participants and researchers were unblinded at the end of the interventions.
Exercise + supplementation
Participants in the PLB + RT and VES + RT groups underwent a 12-week structured RT program combined with vitamin E or placebo consumption. The RT sessions followed ACSM guidelines for healthy adults [37] and were held three nonconsecutive days per week at the Razi University weight room. Each session included a 15-minute warm-up with stationary cycling and dynamic movements, followed by a 40-45-minute primary exercise regimen. Exercises included machine chest press, wide-grip lat pull-down, machine shoulder press, biceps cable curl, cable triceps push-down, leg extension, leg press, and leg curls. Participants completed three sets of 8–12 repetitions for each exercise at 60–80% of their one-repetition maximum (1RM). After each session, a five-minute cool-down phase of static stretching exercises was performed (Table 2). Adherence to RT sessions exceeded 90% of the total sessions.
To determine the 1RM, participants completed an indirect 1RM test, which is considered safe for those less experienced in RT. This involved identifying a load within 3–5 sets that allowed them to complete six correct repetitions (i.e., 6RM) [38]. 1RM values were then calculated using the Berzyski formula [39]. After six weeks of training, the 1RM test was repeated to adjust training intensity for the exercise groups. Prior to starting the main exercises, participants underwent several thorough familiarization sessions with the training protocol.
Statistical methods
Descriptive data are presented as mean ± standard deviation. Normality was checked with the Shapiro-Wilk test. A one-way ANOVA with Tukey correction was used to analyze the pre- to post-test changes in study variables among the four groups. Repeated measures ANOVA assessed group × time interactions, with paired t-tests for within-group changes. Effect sizes were reported using partial eta-squared (ηp2). Pearson correlation assessed bivariate correlations between changes in aminotransferases and CTRPs with BMI, AIP, and HOMA-IR. All analyses were performed at a 0.05 significance level using SPSS 26 (IBM, USA).
Results
Body composition and muscle strength
For BW, a significant main effect of time (F1,33=8.01, p = 0.008, ηp2 = 0.195) and a significant time×group interaction (F3,33=12.954, p = 0.001, ηp2 = 0.541) were observed. Significant decreases in BW occurred in the PLB + RT (p = 0.001) and VES + RT (p = 0.011) groups. The changes in BW were significant in the PLB + RT (p < 0.001) and VES + RT (p = 0.002) groups compared to the PLB and VES groups, respectively. Regarding BMI, a significant main effect of time (F1,33=7.539, p = 0.01, ηp2 = 0.186) and a significant time×group interaction (F3,33=12.646, p = 0.001, ηp2 = 0.535) were found. Significant decreases in BMI were noted in the PLB + RT (p = 0.001) and VES + RT (p = 0.01) groups. The changes in BMI were significant in the PLB + RT (p < 0.001) and VES + RT (p = 0.002) groups compared to the PLB and VES groups, respectively. For WHR, a significant main effect of time (F1,33=13.971, p = 0.001, ηp2 = 0.297) and a significant time×group interaction (F3,33=10.285, p = 0.001, ηp2 = 0.483) were identified. Significant decreases in WHR were seen in the PLB + RT (p = 0.003) and VES + RT (p = 0.004) groups. The changes in WHR were significant in the PLB + RT (p = 0.007) and VES + RT (p = 0.001) groups compared to the PLB and VES groups, respectively. In the case of BFP, a significant main effect of time (F1,33=25.386, p = 0.001, ηp2 = 0.435) and a significant time×group interaction (F3,33=21.00, p = 0.001, ηp2 = 0.656) were observed. Significant decreases in BFP occurred in the PLB + RT (p = 0.001) and VES + RT (p < 0.001) groups. The changes in BFP were significant in the PLB + RT (p < 0.001) and VES + RT (p < 0.001) groups compared to the PLB and VES groups, respectively. For 1RM, a significant main effect of time (F1,33=8.449, p = 0.006, ηp2 = 0.204) and a significant time×group interaction (F3,33=30.037, p = 0.001, ηp2 = 0.732) were observed. Significant increases in 1RM were noted in the PLB + RT (p < 0.001) and VES + RT (p < 0.001) groups. Interestingly, a significant decrease in 1RM was observed in the VES group (p = 0.004). The changes in 1RM were significant in the PLB + RT (p < 0.001) and VES + RT (p < 0.001) groups compared to the PLB and VES groups, respectively (Table 3).
Lipid profile
For TG, a significant main effect of time (F1,33=35.548, p = 0.001, ηp2 = 0.519) and a significant time×group interaction (F3,33=18.432, p = 0.001, ηp2 = 0.626) were found. Significant decreases in TG occurred in the PLB + RT (p = 0.001) and VES + RT (p = 0.001) groups. The changes in TG were significant in the PLB + RT (p < 0.001) and VES + RT (p < 0.001) groups compared to the PLB and VES groups, respectively. Regarding LDL, a significant main effect of time (F1,33=37.268, p = 0.001, ηp2 = 0.53) and a significant time×group interaction (F3,33=22.208, p = 0.001, ηp2 = 0.669) were observed. Significant decreases in LDL were noted in the PLB + RT (p < 0.001) and VES + RT (p = 0.001) groups. The changes in LDL were significant in the PLB + RT (p < 0.001) and VES + RT (p < 0.001) groups compared to the PLB and VES groups, respectively. For HDL, no significant main effect of time (p > 0.05) or time × group interaction (p > 0.05) was observed. In the case of TC, a significant main effect of time (F1,33=85.807, p = 0.001, ηp2 = 0.722) and a significant time×group interaction (F3,33=46.174, p = 0.001, ηp2 = 0.808) were found. Significant decreases in TC occurred in the PLB + RT (p < 0.001) and VES + RT (p < 0.001) groups. The changes in TC were significant in the PLB + RT (p < 0.001) and VES + RT (p < 0.001) groups compared to the PLB and VES groups, respectively. For AIP, a significant main effect of time (F1,33=22.731, p = 0.001, ηp2 = 0.408) and a significant time×group interaction (F3,33=13.953, p = 0.001, ηp2 = 0.559) were observed. Significant decreases in AIP occurred in the PLB + RT (p = 0.003) and VES + RT (p = 0.001) groups. The changes in AIP were significant in the PLB + RT (p = 0.004) and VES + RT (p < 0.001) groups compared to the PLB and VES groups, respectively. (Table 3).
Glycemic control
For glucose, a significant main effect of time (F1,33=17.632, p = 0.001, ηp2 = 0.348) and a significant time×group interaction (F3,33=13.314, p = 0.001, ηp2 = 0.548) were found. Significant decreases in glucose occurred in the PLB + RT (p < 0.001) and VES + RT (p < 0.001) groups. The changes in glucose were significant in the PLB + RT (p = 0.004) and VES + RT (p < 0.001) groups compared to the PLB and VES groups, respectively. Regarding insulin, a significant main effect of time (F1,33=9.107, p = 0.005, ηp2 = 0.216) and a significant time group interaction (F3,33=6.042, p = 0.002, ηp2 = 0.355) were observed. Significant decreases in insulin were noted in the PLB + RT (p = 0.014) and VES + RT (p = 0.007) groups. The changes in insulin were significant in the PLB + RT (p = 0.02) and VES + RT (p = 0.03) groups compared to the PLB and VES groups, respectively. For HOMA-IR, a significant main effect of time (F1,33=16.037, p = 0.001, ηp2 = 0.327) and a significant time×group interaction (F3,33=11.490, p = 0.001, ηp2 = 0.511) were identified. Significant decreases in HOMA-IR occurred in the PLB + RT (p = 0.003) and VES + RT (p = 0.001) groups. The changes in HOMA-IR were significant in the PLB + RT (p = 0.001) and VES + RT (p = 0.001) groups compared to the PLB and VES groups, respectively. In the case of QUICKI, a significant main effect of time (F1,33=16.037, p = 0.001, ηp2 = 0.327) and a significant time×group interaction (F3,33=7.615, p = 0.001, ηp2 = 0.409) were observed. Significant increases in QUICKI were noted in the PLB + RT (p = 0.003) and VES + RT (p = 0.016) groups. The changes in QUICKI were significant in the VES + RT (p = 0.002) group compared to the VES groups (Table 4).
Aminotransferases
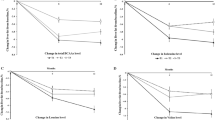
For AST, a significant main effect of time (F1,33=111.689, p = 0.001, ηp2 = 0.772) and a significant time×group interaction (F3,33=44.262, p = 0.001, ηp2 = 0.801) were found. Significant decreases in AST were observed in the VES (p < 0.001), PLB + RT (p = 0.001), and VES + RT (p < 0.001) groups. The changes in AST were significant in the VES group compared to the PLB group (p < 0.001), in the PLB + RT group compared to the PLB group (p < 0.001), and in the VES + RT group compared to both the VES (p < 0.001) and PLB + RT (p < 0.001) groups. Regarding ALT, a significant main effect of time (F1,33=136.973, p = 0.001, ηp2 = 0.806) and a significant time×group interaction (F3,33=24.59, p = 0.001, ηp2 = 0.691) were observed. Significant decreases in ALT occurred in the VES (p = 0.001), PLB + RT (p < 0.001), and VES + RT (p < 0.001) groups. The changes in ALT were significant in the VES group compared to the PLB group (p < 0.001), in the PLB + RT group compared to the PLB group (p < 0.001), and in the VES + RT group compared to the PLB + RT (p < 0.017) groups (Table 4; Fig. 2). There was also a significant correlation between changes in aminotransferases, BMI, AIP, and HOMA-IR (p < 0.05; Table 5).

Pre- to post-training changes in serum levels. Changes in serum levels from pre- to post-training for (A) Aspartate Aminotransferase, (B) Alanine Aminotransferase, (C) C1q/TNF-Related Protein-2, and (D) C1q/TNF-Related Protein-9 across the study groups are shown. Data are presented as means ± standard deviations. Significant differences compared to PLB: &p < 0.01; significant differences compared to VES: †p < 0.05, ‡p < 0.01; significant differences compared to PLB + RT: ◇p < 0.05, ±p < 0.01. PLB: Placebo; VES: Vitamin E Supplementation; RT: Resistance Training
C1Q/TNF-related proteins
For CTRP-2, despite no significant main effect of time (p > 0.05), a significant time×group interaction (F3,33=7.103, p = 0.001, ηp2 = 0.392) was found. Significant decreases in CTRP-2 occurred in the PLB + RT (p = 0.018) and VES + RT (p = 0.007) groups. The changes in CTRP2 were significant in the PLB + RT (p = 0.01) and VES + RT (p = 0.018) groups compared to the PLB and VES groups, respectively. Regarding CTRP-9, a significant main effect of time (F1,33=76.487, p = 0.001, ηp2 = 0.699) and a significant time×group interaction (F3,33=39.658, p = 0.001, ηp2 = 0.783) were observed. Significant decreases in CTRP-9 occurred in the PLB + RT (p < 0.001) and VES + RT (p < 0.001) groups. The changes in CTRP9 were significant in the PLB + RT (p < 0.001) and VES + RT (p < 0.001) groups compared to the PLB and VES groups, respectively (Table 4; Fig. 2). There was also a significant correlation between changes in CTRPs, BMI, AIP, and HOMA-IR (p < 0.05; Table 5).
Discussion
NAFLD is a prevalent liver disorder characterized by excessive fat accumulation in the liver, often associated with obesity and MetS. This study pioneers exploring the combined impacts of RT and VES in patients with NAFLD. The key findings indicate that RT significantly improves body composition, biochemical, and hormonal parameters in these patients. Although VES was effective in lowering aminotransferases, it did not offer additional benefits beyond RT.
Body composition and muscle strength
Exercise groups significantly improved body composition consistent with Zelber-Sagi et al. who reported reductions in BW, BMI, and BFP in patients with NAFLD after three months of RT [21]. RT programs can significantly reduce BFP in individuals who are overweight or obese, regardless of age or sex [40]. Potential mechanisms for RT’s effect on abdominal fat include increased resting metabolic rate, improved IS, and enhanced sympathetic activity [41]. This is crucial since liver fat infiltration closely correlates with abdominal fat [42]. Therefore, RT’s ability to boost energy expenditure during recovery and muscle regeneration [41] likely improved body composition in the RT groups. Additionally, our results indicate no further benefits of VES on body composition indices, consistent with a meta-analysis by Emami et al., which reported no significant effect of VES on weight, BMI, and waist circumference [43].
The RT protocol significantly increased the 1RM in the exercise groups consistent with previous findings [44]. Generally, adaptation to RT becomes evident after eight to 12 weeks, attributed to specific neuromuscular, connective tissue, and hypertrophy-related changes [45]. Importantly, VES provided no additional strength gain in the VES + RT group, and there was a significant decrease in 1RM in the VES group, possibly due to less motivation to reach their maximum strength. A meta-analysis by Clifford et al. evidenced that VES alone or combined with vitamin C neither enhances nor blunts exercise-induced training adaptations, including changes in aerobic capacity and muscle strength [46]. However, Betik et al. reported a significant 50% increase in exercise endurance in sedentary, diet-induced obese rats following supplementation with tocotrienols [47]. This discrepancy highlights the need for more research on the effects of different antioxidants on exercise performance. Future studies should consider whether supplementation is more beneficial in states of antioxidant deficiency or inadequate intake.
Lipid Profile
The lipid profile improved significantly in the exercise groups, although HDL levels remained unchanged. Bacchi et al. also observed a significant decrease in TG levels after four months of RT in individuals with Type 2 Diabetes (T2D) and NAFLD [48]. Conversely, Venojärvi et al. did not find a significant change in AIP levels following 12 weeks of RT in males who were overweight and obese, despite a decreasing trend [49]. The majority of individuals with obesity exhibit a dyslipidemic profile, which is also commonly seen in patients with NAFLD [50]. Exercise interventions can improve lipid profile, primarily by affecting peripheral tissues such as the liver [51]. One possible mechanism for reducing plasma lipid levels in RT groups is the improved activity of lecithin cholesterol acyltransferase and lipoprotein lipase [51]. Notably, VES provided no additional benefit in lipid profile improvement, consistent with Hendarto et al.‘s findings, which reported no significant difference in the lipid profile of adolescents with obesity after two months of VES [52].
Glycemic Control
Glycemic control indices improved significantly in the exercise groups, consistent with Charatcharoenwitthaya et al., who observed enhanced IR/IS after 12 weeks of RT in patients with NAFLD [53]. However, Zelber-Sagi et al. did not find significant changes in glucose, insulin, and HOMA-IR levels after three months of RT in patients with NAFLD [21]. RT has been reported to improve hyperglycemia mainly in patients with disturbed glucose metabolism or diabetes [21, 54], though some studies have shown significant glycemic improvements in healthy individuals as well [55], confirming RT’s effectiveness across different populations. Our study’s results are significant because NAFLD is strongly associated with both hepatic and adipose tissue IR, as well as reduced whole-body IS [56]. RT can improve glucose and insulin homeostasis by increasing lean body mass and enhancing muscle metabolic properties, including higher density of glucose transporter type 4, glycogen synthase content/activity, and insulin-mediated glucose clearance [41]. Our findings also suggest that VES provided no additional benefit over placebo in glycemic control. A meta-analysis by Asbaghi et al. concluded that VES can be effective in improving glycemic control in people with diabetes [57]. Considering that our participants were not diabetic may explain these contrasting results.
Aminotransferases
Aminotransferases levels improved significantly in all groups except the PLB group. Similarly, Shamsoddini et al. observed significant reductions in AST and ALT among males with NAFLD after eight weeks of RT [58]. Changes in IS, circulatory lipids, and energy balance are possible mechanisms underlying the change in hepatic fat following exercise training [59]. In the current study, we found a significant correlation between changes in aminotransferases and BMI, AIP, and HOMA-IR. These changes likely contributed to enhanced liver oxidation and lowered aminotransferase levels. Our results are also consistent with Yakaryilmaz et al., who demonstrated significant AST and ALT decreases following 24 weeks of VES in patients with NASH [60]. MetS can increase the delivery of FFAs to the liver, resulting in high OS due to oxidative phosphorylation of FFAs. High OS creates an environment rich in reactive oxygen species that can cause hepatocyte injury [61]. Vitamin E, a major lipid-soluble antioxidant with anti-inflammatory activities, targets OS components and is a promising therapeutic approach for NAFLD [62]. In a long-term study, Sanyal et al. demonstrated histological improvements in patients with NASH after 96 weeks of VES, with decreases in liver steatosis and ALT [23], indicating a relationship between histological and aminotransferase improvements. We also observed significant AST/ALT improvements in our VES group, possibly due to liver histological improvements. Additionally, significant differences were observed between the VES + RT group and both the VES and PLB + RT groups, suggesting that adding vitamin E to RT provided additional benefits in lowering aminotransferases in patients with NAFLD over the 12-week study period.
C1Q/TNF-Related proteins
CTRP-2 and CTRP-9 levels decreased significantly in the exercise groups. While acute bouts of aerobic and high-intensity interval training have been linked to increased CTRP-9 levels [63, 64], the chronic effects of exercise on CTRP-2 and CTRP-9 are controversial. Jerobin et al. and Hasegawa et al. found no significant changes in these components after AT in individuals within normal weight ranges or classified as overweight [27, 65]. Conversely, Sadeghi et al. reported a significant increase in CTRP-9 following 12 weeks of AT and RT in males with T2D [66]. In obese mice, increased expression of CTRP-2 suggests a compensatory mechanism [12]. Additionally, overexpression of CTRP-9 in transgenic mice has been associated with improved glucose homeostasis and enhanced fat oxidation in skeletal muscle mitochondria, leading to reductions in BW, fasting insulin, and blood glucose levels [14]. Structurally and functionally similar to adiponectin, CTRP-2, and CTRP-9 exhibit identical expression patterns and responses to metabolic changes [11, 14]. Given the inverse relationship between adiponectin levels and obesity [67], the increased CTRP-2 and CTRP-9 levels in individuals with obesity may represent a compensatory response to decreased adiponectin levels. In this study, we found a significant correlation between changes in CTRPs and BMI, AIP, and HOMA-IR. Improvements in BMI, AIP, and HOMA-IR following RT likely contributed to a rebalancing of adipokines, potentially leading to decreased CTRP-2 and CTRP-9 levels. However, this hypothesis needs further research to validate it. Moreover, since VES had no significant effect on BMI, AIP, and HOMA-IR, it provided no additional benefit in lowering CTRPs levels either.
Study strengths and limitations
The study has notable strengths, including the combination of RT and VES and the assessment of CTRPs in NAFLD patients. However, there are several limitations to consider. The relatively small sample size may affect the study’s power and generalizability, so results should be interpreted with caution. Future research with larger cohorts could provide more robust insights. The diagnosis of NAFLD was based on ultrasound, which lacks the histological detail of liver examination. Additionally, we did not monitor participants’ dietary regimens during the study period, and the long-term effects of the interventions were not assessed. The study also did not measure other important factors, such as adiponectin, which could provide further insights into changes in CTRPs.
Conclusions
In conclusion, our study underscores the effectiveness of RT as a therapeutic option for NAFLD patients, demonstrating benefits in body composition, lipid profile, glycemic control, and aminotransferase levels. Although the addition of VES to RT resulted in further decreases in aminotransferases, it did not provide additional benefits for other study variables. Our results also highlight the link between improved body composition, lipid profile, and glycemic control with reductions in CTRP-2/CTRP-9 levels, suggesting a compensatory role for these proteins in metabolic diseases like NAFLD. However, further research is needed to validate these findings.
Data availability
All data generated or analyzed during this study are included in this published article.
Abbreviations
- 1RM:
-
One-repetition maximum
- ACSM:
-
American College of Sports Medicine
- AIP:
-
Atherogenic index of plasma
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- AT:
-
Aerobic training
- BFP:
-
Body fat percentage
- BMI:
-
Body mass index
- BW:
-
Body weight
- CTRPs:
-
C1q/TNF-related proteins
- FFAs:
-
Free fatty acids
- HDL:
-
High-density lipoprotein
- HOMA-IR:
-
Homeostasis model assessment of insulin resistance
- IR:
-
Insulin resistance
- IS:
-
Insulin sensitivity
- MetS:
-
Metabolic syndrome
- NAFLD:
-
Nonalcoholic fatty liver disease
- OS:
-
Oxidative stress
- PLB:
-
Placebo
- QUICKI:
-
Quantitative insulin sensitivity check index
- RT:
-
Resistance training
- T2D:
-
Type 2 Diabetes
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
- VES:
-
Vitamin E supplementation
- WHR:
-
Waist-to-hip ratio
- ηp 2 :
-
Partial eta-squared
References
Guo X, Yin X, Liu Z, Wang J. Non-alcoholic fatty liver Disease (NAFLD) Pathogenesis and Natural products for Prevention and Treatment. Int J Mol Sci. 2022;23(24).
Raza S, Rajak S, Upadhyay A, Tewari A, Anthony Sinha R. Current treatment paradigms and emerging therapies for NAFLD/NASH. Front Biosci (Landmark Ed). 2021;26(2):206–37.
Farzanegi P, Dana A, Ebrahimpoor Z, Asadi M, Azarbayjani MA. Mechanisms of beneficial effects of exercise training on non-alcoholic fatty liver disease (NAFLD): roles of oxidative stress and inflammation. Eur J Sport Sci. 2019;19(7):994–1003.
Bessone F, Razori MV, Roma MG. Molecular pathways of nonalcoholic fatty liver disease development and progression. Cell Mol Life Sci. 2019;76(1):99–128.
Mansour-Ghanaei R, Mansour-Ghanaei F, Naghipour M, Joukar F. Biochemical markers and lipid profile in nonalcoholic fatty liver disease patients in the PERSIAN Guilan cohort study (PGCS), Iran. J Family Med Prim Care. 2019;8(3):923–8.
Ismaiel A, Ciobanu OS, Ismaiel M, Leucuta DC, Popa SL, David L et al. Atherogenic Index of Plasma in non-alcoholic fatty liver disease: systematic review and Meta-analysis. Biomedicines. 2022;10(9).
Liu J, Zhou L, An Y, Wang Y, Wang G. The atherogenic index of plasma: a novel factor more closely related to non-alcoholic fatty liver disease than other lipid parameters in adults. Front Nutr. 2022;9:954219.
Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15(1):11–20.
Paternostro R, Trauner M. Current treatment of non-alcoholic fatty liver disease. J Intern Med. 2022;292(2):190–204.
Ramanjaneya M, Jerobin J, Bettahi I, Siveen KS, Abou-Samra A-B. Emerging roles of C1Q tumor necrosis factor-related proteins in metabolic diseases. Translational Med Commun. 2021;6(1):5.
Ilbeigi D, Khoshfetrat M, Afrisham R, Rahimi B, Gorgani-Firuzjaee S. Serum C1q/TNF-Related Protein-2 (CTRP2) levels are Associated with Coronary Artery Disease. Arch Med Res. 2020;51(2):167–72.
Wong GW, Krawczyk SA, Kitidis-Mitrokostas C, Revett T, Gimeno R, Lodish HF. Molecular, biochemical and functional characterizations of C1q/TNF family members: adipose-tissue-selective expression patterns, regulation by PPAR-gamma agonist, cysteine-mediated oligomerizations, combinatorial associations and metabolic functions. Biochem J. 2008;416(2):161–77.
Peterson JM, Seldin MM, Tan SY, Wong GW. CTRP2 overexpression improves insulin and lipid tolerance in diet-induced obese mice. PLoS ONE. 2014;9(2):e88535.
Guan H, Wang Y, Li X, Xiang A, Guo F, Fan J, et al. C1q/Tumor necrosis factor-related protein 9: basics and therapeutic potentials. Front Physiol. 2022;13:816218.
Wong GW, Krawczyk SA, Kitidis-Mitrokostas C, Ge G, Spooner E, Hug C, et al. Identification and characterization of CTRP9, a novel secreted glycoprotein, from adipose tissue that reduces serum glucose in mice and forms heterotrimers with adiponectin. Faseb j. 2009;23(1):241–58.
Wei Z, Lei X, Petersen PS, Aja S, Wong GW. Targeted deletion of C1q/TNF-related protein 9 increases food intake, decreases insulin sensitivity, and promotes hepatic steatosis in mice. Am J Physiol Endocrinol Metab. 2014;306(7):E779–90.
Zuo A, Zhao X, Li T, Li J, Lei S, Chen J, et al. CTRP9 knockout exaggerates lipotoxicity in cardiac myocytes and high-fat diet-induced cardiac hypertrophy through inhibiting the LKB1/AMPK pathway. J Cell Mol Med. 2020;24(4):2635–47.
Hashida R, Kawaguchi T, Bekki M, Omoto M, Matsuse H, Nago T, et al. Aerobic vs. resistance exercise in non-alcoholic fatty liver disease: a systematic review. J Hepatol. 2017;66(1):142–52.
Chatzinikolaou A, Fatouros I, Petridou A, Jamurtas A, Avloniti A, Douroudos I, et al. Adipose tissue lipolysis is upregulated in lean and obese men during acute resistance exercise. Diabetes Care. 2008;31(7):1397–9.
Whitsett M, VanWagner LB. Physical activity as a treatment of non-alcoholic fatty liver disease: a systematic review. World J Hepatol. 2015;7(16):2041–52.
Zelber-Sagi S, Buch A, Yeshua H, Vaisman N, Webb M, Harari G, et al. Effect of resistance training on non-alcoholic fatty-liver disease a randomized-clinical trial. World J Gastroenterol. 2014;20(15):4382–92.
Xu A, Wang Y, Keshaw H, Xu LY, Lam KS, Cooper GJ. The fat-derived hormone adiponectin alleviates alcoholic and nonalcoholic fatty liver diseases in mice. J Clin Invest. 2003;112(1):91–100.
Sanyal AJ, Chalasani N, Kowdley KV, McCullough A, Diehl AM, Bass NM, et al. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. N Engl J Med. 2010;362(18):1675–85.
Petzold G. Role of Ultrasound methods for the Assessment of NAFLD. J Clin Med. 2022;11(15).
Cho MH. Preliminary reliability of the five item physical activity questionnaire. J Phys Ther Sci. 2016;28(12):3393–7.
Mohammadi S, Monazzami A, Alavimilani S. Effects of eight-week high-intensity interval training on some metabolic, hormonal and cardiovascular indices in women with PCOS: a randomized controlled trail. BMC Sports Sci Med Rehabil. 2023;15(1):47.
Monazzami A, Rajabi H, Ghrakhanlou R, Yari K, Rahimi, Z. Modulation of oxidative and glycolytic skeletal muscle fibers Na+/H+ exchanger1 (NHE1) and Na+/HCO3- co-transporter1 (NBC1) genes and proteins expression in type 2 diabetic rat (Streptozotocin + high fat diet) following long term endurance training. Cell Mol Biol (Noisy-le-Grand, France). 2017;63(5):11–8. https://doi.org/10.14715/cmb/2017.63.5.3.
Monazzami A, Momenpur R, Alipour E, Yari K, Payandeh, M. Effects of eight-week combined resistance and endurance training on salivary interleukin-12, tumor necrosis factor, cortisol, and testosterone levels in patients with breast cancer. Int J Cancer Manag. 2021;14(2):e109039. https://doi.org/10.5812/ijcm.109039.
Astinchap A, Monazzami A, Fereidoonfara K, Rahimi Z, Rahimi, M. Modulation of fibroblast growth factor-21 and βklotho proteins expression in type 2 diabetic women with non-alcoholic fatty liver disease following endurance and strength training. Hepat Mon. 2021;21(7):e116513. https://doi.org/10.5812/hepatmon.116513.
Jerobin J, Ramanjaneya M, Bettahi I, Parammal R, Siveen KS, Alkasem M, et al. Regulation of circulating CTRP-2/CTRP-9 and GDF-8/GDF-15 by intralipids and insulin in healthy control and polycystic ovary syndrome women following chronic exercise training. Lipids Health Dis. 2021;20(1):34.
Doig GS, Simpson F. Randomization and allocation concealment: a practical guide for researchers. J Crit Care. 2005;20(2):187–91. discussion 91 – 3.
Zhang YN, Fowler KJ, Hamilton G, Cui JY, Sy EZ, Balanay M, et al. Liver fat imaging-a clinical overview of ultrasound, CT, and MR imaging. Br J Radiol. 2018;91(1089):20170959.
Medicine ACoS. ACSM’s health-related physical fitness assessment manual. Lippincott Williams & Wilkins; 2013.
Mirzaalian Y, Nourian M, Gholamalizadeh M, Doaei S, Hatami M, Hassanzadeh A, et al. The association of quantitative insulin sensitivity indices (HOMA-IR and QUICKI) with anthropometric and cardiometabolic indicators in adolescents. Arch Med Sci Atheroscler Dis. 2019;4:e32–7.
Kim SH, Cho YK, Kim YJ, Jung CH, Lee WJ, Park JY, et al. Association of the atherogenic index of plasma with cardiovascular risk beyond the traditional risk factors: a nationwide population-based cohort study. Cardiovasc Diabetol. 2022;21(1):81.
Eslami L, Isazadehfar K, Karami M, Rahmani-Nia F, Nakhostinroohi B. The effect of 12 weeks regular physical activity and vitamin E in the treatment of non-alcoholic steatohepatitis: a pilot study. Govaresh. 2015;20:57–65.
American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2009;41(3):687–708.
Moro T, Marcolin G, Bianco A, Bolzetta F, Berton L, Sergi G et al. Effects of 6 weeks of traditional resistance training or high intensity interval resistance training on body composition, Aerobic Power and Strength in healthy young subjects: a randomized parallel trial. Int J Environ Res Public Health. 2020;17(11).
Wood T, Maddalozzo G, Harter R. Accuracy of seven equations for Predicting 1RM performance of apparently healthy, sedentary older adults. Meas Phys Educ Exerc Sci. 2002;6:67–94.
Lopez P, Taaffe DR, Galvão DA, Newton RU, Nonemacher ER, Wendt VM, et al. Resistance training effectiveness on body composition and body weight outcomes in individuals with overweight and obesity across the lifespan: a systematic review and meta-analysis. Obes Rev. 2022;23(5):e13428.
Westcott WL. Resistance Training is Medicine: effects of Strength Training on Health. Curr Sports Med Rep. 2012;11(4).
Jang S, Lee CH, Choi KM, Lee J, Choi JW, Kim KA, et al. Correlation of fatty liver and abdominal fat distribution using a simple fat computed tomography protocol. World J Gastroenterol. 2011;17(28):3335–41.
Emami MR, Jamshidi S, Zarezadeh M, Khorshidi M, Olang B, Sajadi Hezaveh Z, et al. Can vitamin E supplementation affect obesity indices? A systematic review and meta-analysis of twenty-four randomized controlled trials. Clin Nutr. 2021;40(5):3201–9.
Avila JJ, Gutierres JA, Sheehy ME, Lofgren IE, Delmonico MJ. Effect of moderate intensity resistance training during weight loss on body composition and physical performance in overweight older adults. Eur J Appl Physiol. 2010;109(3):517–25.
Hughes DC, Ellefsen S, Baar K. Adaptations to endurance and strength training. Cold Spring Harb Perspect Med. 2018;8(6).
Clifford T, Jeffries O, Stevenson EJ, Davies KAB. The effects of vitamin C and E on exercise-induced physiological adaptations: a systematic review and Meta-analysis of randomized controlled trials. Crit Rev Food Sci Nutr. 2020;60(21):3669–79.
Betik AC, Aguila J, McConell GK, McAinch AJ, Mathai ML. Tocotrienols and Whey Protein isolates substantially increase Exercise endurance capacity in Diet -Induced obese male sprague-dawley rats. PLoS ONE. 2016;11(4):e0152562.
Bacchi E, Negri C, Targher G, Faccioli N, Lanza M, Zoppini G, et al. Both resistance training and aerobic training reduce hepatic fat content in type 2 diabetic subjects with nonalcoholic fatty liver disease (the RAED2 Randomized Trial). Hepatology. 2013;58(4):1287–95.
Venojärvi M, Korkmaz A, Wasenius N, Manderoos S, Heinonen OJ, Lindholm H, et al. 12 weeks’ aerobic and resistance training without dietary intervention did not influence oxidative stress but aerobic training decreased atherogenic index in middle-aged men with impaired glucose regulation. Food Chem Toxicol. 2013;61:127–35.
Ganjooei NA, Jamialahmadi T, Nematy M, Jangjoo A, Goshayeshi L, Khadem-Rezaiyan M et al. The role of lipid Profile as an independent predictor of non-alcoholic steatosis and steatohepatitis in morbidly obese patients. Front Cardiovasc Med. 2021;8.
Salehi Z, Salehi K, Moeini M, Kargarfard M, Sadeghi M. The Effect of Resistance Exercise on lipid Profile of Coronary Artery Disease patients: a Randomized Clinical Trial. Iran J Nurs Midwifery Res. 2017;22(2):112–6.
Hendarto A, Alhadar AK, Sjarif DR. The effect of vitamin E supplementation on lipid profiles and Adiponectin Levels in obese adolescents: a Randomized Controlled Trial. Acta Med Indones. 2019;51(2):110–6.
Charatcharoenwitthaya P, Kuljiratitikal K, Aksornchanya O, Chaiyasoot K, Bandidniyamanon W, Charatcharoenwitthaya N. Moderate-intensity aerobic vs Resistance Exercise and Dietary Modification in patients with nonalcoholic fatty liver disease: a Randomized Clinical Trial. Clin Transl Gastroenterol. 2021;12(3):e00316.
Baldi JC, Snowling N. Resistance training improves glycaemic control in obese type 2 diabetic men. Int J Sports Med. 2003;24(6):419–23.
Conceição MS, Bonganha V, Vechin FC, Berton RP, Lixandrão ME, Nogueira FR, et al. Sixteen weeks of resistance training can decrease the risk of metabolic syndrome in healthy postmenopausal women. Clin Interv Aging. 2013;8:1221–8.
Utzschneider KM, Kahn SE. The role of Insulin Resistance in nonalcoholic fatty liver disease. J Clin Endocrinol Metabolism. 2006;91(12):4753–61.
Asbaghi O, Nazarian B, Yousefi M, Anjom-Shoae J, Rasekhi H, Sadeghi O. Effect of vitamin E intake on glycemic control and insulin resistance in diabetic patients: an updated systematic review and meta-analysis of randomized controlled trials. Nutr J. 2023;22(1):10.
Shamsoddini A, Sobhani V, Ghamar Chehreh ME, Alavian SM, Zaree A. Effect of Aerobic and Resistance Exercise training on liver enzymes and hepatic Fat in Iranian men with nonalcoholic fatty liver disease. Hepat Mon. 2015;15(10):e31434.
Hallsworth K, Fattakhova G, Hollingsworth KG, Thoma C, Moore S, Taylor R, et al. Resistance exercise reduces liver fat and its mediators in non-alcoholic fatty liver disease independent of weight loss. Gut. 2011;60(9):1278–83.
Yakaryilmaz F, Guliter S, Savas B, Erdem O, Ersoy R, Erden E, et al. Effects of vitamin E treatment on peroxisome proliferator-activated receptor-alpha expression and insulin resistance in patients with non-alcoholic steatohepatitis: results of a pilot study. Intern Med J. 2007;37(4):229–35.
Perumpail BJ, Li AA, John N, Sallam S, Shah ND, Kwong W, et al. The role of vitamin E in the treatment of NAFLD. Diseases. 2018;6(4):86.
El Hadi H, Vettor R, Rossato M. Vitamin E as a treatment for nonalcoholic fatty liver disease: reality or myth? Antioxid (Basel). 2018;7(1).
Kon M, Tanimura Y. Responses of complement C1q/tumor necrosis factor-related proteins to acute aerobic exercise. Cytokine. 2023;161:156083.
Kon M, Ebi Y, Nakagaki K. Effects of a single bout of high-intensity interval exercise on C1q/TNF-related proteins. Appl Physiol Nutr Metab. 2019;44(1):47–51.
Hasegawa N, Fujie S, Horii N, Uchida M, Kurihara T, Sanada K, et al. Aerobic exercise training-induced changes in serum C1q/TNF-related protein levels are associated with reduced arterial stiffness in middle-aged and older adults. Am J Physiol Regul Integr Comp Physiol. 2018;314(1):R94–101.
Sadeghi R, keshavarz s, Kargarfard M, banaii j. The effects of Aerobic, Resistance, and combined Exercise on Adiponectin and CTRP-9 levels in patients with type 2 diabetes Mellitus. J Appl Health Stud Sport Physiol. 2022;9(2):173–87.
Nigro E, Scudiero O, Monaco ML, Palmieri A, Mazzarella G, Costagliola C, et al. New insight into adiponectin role in obesity and obesity-related diseases. Biomed Res Int. 2014;2014:658913.
Acknowledgements
The authors would like to sincerely thank all participants for their invaluable contributions to this study and extend gratitude to Mr. Bahram Bahrami for his assistance with laboratory tests.
Funding
This research did not receive any external funding.
Author information
Authors and Affiliations
Contributions
All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants provided written informed consent after being briefed on the research methods and objectives. The study was approved by the Research Ethics Committee of Razi University of Kermanshah (IR.RAZI.REC.1401.030) on July 24, 2022.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Varmazyar, I., Monazzami, A.A., Moradi, M. et al. Effects of 12-weeks resistance training and vitamin E supplementation on aminotransferases, CTRP-2, and CTRP-9 levels in males with nonalcoholic fatty liver disease: a double-blind, randomized trial. BMC Sports Sci Med Rehabil 16, 185 (2024). https://doi.org/10.1186/s13102-024-00972-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-024-00972-9