
Abstract
Background
Antiretroviral therapy (ART) has led to an increased lifespan for people living with HIV (PWH). This increased lifespan, coupled with the effects of HIV and adverse effects of ART have resulted in an increasing burden of cardiometabolic disease (CMD) among PWH. Physical activity (PA) has been proposed as an effective strategy to reduce the risk of developing cardiometabolic disease and other health complications in PWH. The aim of this paper is to review the characteristics and efficacy of PA interventions to improve cardiometabolic and psychosocial outcomes among PWH in sub-Saharan Africa.
Methods
The review will follow the preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P). Literature searches will be conducted in PubMed, Web of Science (WoS), African Index Medicus, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Embase. Peer-reviewed publications will be included if they include adults (age 18 or older), PWH in sub-Saharan Africa, and a PA intervention to improve cardiometabolic outcomes and/or psychosocial outcomes. We will include randomized controlled trials and quasi-experimental study designs. Two independent reviewers will screen all abstracts and full-text articles. The study methodological quality (or bias) will be appraised using the Revised tool to assess risk of bias in randomized trials and the Downs and Black checklist. Certainty of evidence will be evaluated using the Grading of Recommendations Assessment, Development and Evaluation guidelines. Meta-analyses will be conducted if our results are adequate for meta-analysis. Outcomes will be analyzed as continuous or dichotomous and meta-analyses will be conducted using random effects models with Stata computer software.
Discussion
This review will identify and synthesize the current evidence regarding the characteristics and efficacy of PA interventions to improve cardiometabolic and psychosocial outcomes among PWH in sub-Saharan Africa. We also plan to identify the strengths and weaknesses of evaluated interventions. Based on the evidence, recommendations will be made to promote the design and further evaluate the most promising strategies to maximize the efficacy of PA interventions in improving cardiometabolic and psychosocial outcomes in PWH in sub-Saharan Africa.
Systematic review registration
PROSPERO registration ID: CRD42021271937.
Similar content being viewed by others


Background
Even though sub-Saharan Africa only makes up about 11% of the world population, it remains the global epicenter of the HIV epidemic. Of the 37 million global HIV infections, it is estimated that 20.6 million and 4.7 million HIV infections were found in Eastern and Southern Africa and Western and Central Africa respectively [1]. But notably, health priorities for people living with (PWH) have meaningfully changed in the region. The advent and global distribution of antiretroviral therapy (ART) is has led to a normalization of the lifespan of people living with HIV (PWH) [2]. Thus, ART has changed HIV from a nearly routinely fatal condition, to a manageable chronic disease that extends life expectancy to near that of uninfected people when initiated early and maintained [3, 4].
The widespread use of ART and increasing life expectancy for PWH has concomitantly led to an increased burden of non-communicable diseases among this population [5]. Cardiovascular and metabolic diseases (CMDs) have been found to be the most prevalent and most morbid non-infectious among PWH [6]. It is thus not surprising that, even though there is a narrowing life expectancy gap between PWH and people without HIV, PWH live fewer comorbidity-free years than people without HIV, and this is not improving over time [4]. This finding is also supported by a study with more than 37,000 adult PWH who were matched with up to three HIV-negative control subjects, which compared the rates of co-morbid conditions and trends over time among PWH and HIV-negative people [7]. The study found that PWH had higher comorbidity rates than HIV-negative people and that the greater rate of comorbidities, which included CMDs, osteoporosis and fractures, hyperlipidemia and endocrine disease increased with time among PWH [7]. Among these comorbidities, hypertension has been found to be the leading risk factor for cardiovascular disease in PWH in sub-Saharan Africa [8]. A higher risk for diabetes mellitus has also been reported for PWH on ART compared to people without HIV [9, 10]. PWH are also becoming more obese with rates ranging from 5% in Nigeria [11] to 23% in South Africa [12]. Recently, The Randomized Trial to Prevent Vascular Events in HIV (REPRIEVE) reported poor cardiovascular health among PWH as measured by Life’s Simple 7 (LS7), which includes smoking, diet, physical activity (PA), body mass index (BMI), blood pressure, total cholesterol, and glucose [13]. Poor dietary and PA patterns were reported on LS7 among the participants [13]. Specifically, for PA, out of a total of 7382 participants, only 773(11%) had an ideal PA score on LS7 and 2949 (40%) had poor PA scores on LS7 [13].
In summary, this body of literature suggest that with use of lifelong ART, PWH approach a normal life expectancy, and that priorities for health among PWH are shifting from preventing opportunistic infections to maintaining a healthy life and preventing/managing CMDs. Thus, more attention to comorbidity prevention for PWH is warranted and the critical and independent role for lifestyle interventions together with conventional treatment to improve cardiometabolic health outcomes in PWH must be prioritized. This is particularly important since ART has been found to be associated with unwanted adverse effects [14], including inducing cardiometabolic toxicities [15], which may eventually lead to CMD. The Action in Diabetes and Vascular Disease-PreterAx and DiamicroN Controlled Evaluation (ADVANCE) and the New Antiretroviral and Monitoring Strategies in HIV-infected Adults in Low-Income Countries (NAMSAL) studies, two large clinical trials in sub-Saharan Africa, found that women on dolutegravir-based ART treatment have a significantly higher risk of becoming overweight or obese [16]. In response, interventions which reduce the risk of obesity and its CMD downstream effects are urgently needed in this population.
PA has been shown to be an effective strategy to reduce the risk of developing CMD in PWH [17] and to effectively address the impairments caused by the virus itself and ART [18]. For example, resistance exercise is associated with significant decreases in total cholesterol, triglycerides, and low-density lipoprotein and increased high-density lipoprotein [19]. A resistance exercise intervention among PWH with metabolic syndrome led to significant decreases in fasting glucose, haemoglobin A1C (HbA1c) and body fat percentage compared to controls [20]. After the intervention, those in the exercise arm of the intervention no longer had metabolic syndrome [20]. A second study investigating blood pressure responses during and after one bout of resistance exercise in women with HIV found clinically relevant decreases (≥ 4 mm) in systolic blood pressure in women with a greater waist-to-hip circumference ratio (WHR) and decreases in diastolic pressure in those who had used ART for a shorter period [21]. PA has also been shown to increase cardiorespiratory fitness [22], while high intensity exercise has been shown to increase peak volume of oxygen consumption (VO2peak) [23] among PWH. Resistance exercise has also been found to lead to increased lean mass percentage in PWH [17, 18]. Similarly, systematic reviews have also shown that PA is beneficial for body composition [24, 25], psychological conditions [26, 27], fitness and functional capacity [28, 29] and health-related quality of life (HRQOL) [29, 30] among PWH.
Although the pathways by which PA effects CMD indicators is not fully elucidated, two potential mechanistic pathways [31] have been proposed. First, PA may increase the anti-inflammatory cytokine adiponectin and second, it may decrease pro-inflammatory adipokines [32, 33]. Thus, it has been shown that in PWH, supervised endurance training decreases C-reactive protein, interleukin 6, interleukin 18 and tumor necrosis factor-alpha [34] and that supervised moderate intensity exercise is associated with improvement in C-reactive protein, plasma soluble CD14, d-dimer, interleukin 6 and interleukin 18 levels [35]. Physically active PWH have significantly lower advanced glycation end products, lower triglycerides, waist circumference, [36] and less lipodystrophy than non-active PWH [30]. In summary, PA is associated with both improved health indicators and mechanistic inflammatory pathways that are associated with future risk of CMD and all-cause mortality.
The benefits of PA for PWH, highlight the need to facilitate the implementation of PA for PWH, especially in places where public health systems face considerable resource-constraints. Despite the widely recognized health benefits of regular PA for PWH, studies have consistently shown that most PWH engage in insufficient PA [29, 30, 37,38,39]. In sub-Saharan Africa specifically, a region where nearly two thirds of the world’s population of PWH reside [40], representing a third of the 2.6 million disability life-years caused by cardiovascular disease among PWH globally [41], a large proportion of PWH do not engage in PA as part of their rehabilitation [42]. Furthermore, attrition rates from PA programs in intervention studies are approximately 30% [24, 43, 44]. Inadequate engagement in PA is believed to be due to the over-congested public health systems where most of the focus is directed toward delivering pharmacologic interventions to patients, with restricted time to offer other public health services [45]. Other barriers to CMD screening and management include low knowledge and perceptions of CMDs among PWH [46], poor education of health care providers in CMD management [47,48,49], staffing shortages [50, 51], and poor transportation and urban planning with limited safe green spaces for PA activities [52].
Because CMD is a leading and growing cause of morbidity and mortality among PWH, and because PA is strongly associated with improved CMD health outcomes in other populations, a thorough understanding of approaches to promote PA among PWH in sub-Saharan Africa will be a crucial first step to develop, responding to an unmet health need for this population. To positively change health behavior and promote PA in this population, there is a crucial need for public health leaders and health professionals to understand the elements and impacts of successful PA interventions [53]. Identifying the most effective components of PA interventions as well as their effectiveness will be prerequisites for synthesizing, implementing, and replicating successful interventions [54]. Unfortunately, there is a lack of consolidated data on PA and its impacts on health among PWH in sub-Saharan Africa, notably, the features of PA interventions that are successful and have been implemented effectively to improve health among PWH in the era of ART.
Study aims
Our primary aim is to review the characteristics and efficacy of PA interventions to improve cardiometabolic outcomes, including body composition (e.g., waist circumference, body mass index, waist-to-hip ratio, total body weight), fitness and functional capacity, total cholesterol, lipids, triglycerides, glucose and blood pressure in PWH in sub-Saharan Africa. A secondary aim is to assess if these interventions also improve psychosocial outcomes, including HRQOL, anxiety, depression, self-efficacy, and social support.
Hypothesis
-
1.
PA interventions are effective in improving cardiometabolic and psychosocial outcomes among PWH in sub-Saharan Africa.
-
2.
Successful PA interventions are characterized by socioecological factors and the employment of behavioral change techniques such as motivation, goal setting, self-efficacy, social support, and feedback that are tailored for PWH in resource-poor settings.
Methods
The review will follow the preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) guideline [55] of reporting systematic reviews. Additional file 1: Table S1 shows the populated PRISMA-P checklist for the review protocol. The protocol will be registered with PROSPERO and a detailed preregistered protocol will also be published.
Inclusion criteria
The following criteria must be satisfied to be eligible for review:
-
1.
Studies published between 2000 and the current date.
-
2.
Population: includes adults (18 + years) living with HIV in sub-Saharan Africa.
-
3.
Interventions: any PA-based intervention with a primary aim to improve cardiometabolic and psychosocial outcomes. This may or may not be explicitly stated in the study aim.
-
4.
Comparator or control: No specified comparator or control but may include any passive (e.g., usual care) or active (e.g., alternative behavioral approaches) control group.
-
5.
Outcomes: cardiometabolic, including but not limited to, body composition (including, waist circumference, body mass index (BMI), waist-to-hip-ratio, body weight), fitness and functional capacity, total cholesterol, triglycerides, lipids, glucose, blood pressure and psychosocial outcomes (including but not limited to, HRQOL, anxiety, depression, self-efficacy, and social support).
-
6.
Study design: we will include randomized controlled trials and quasi-experimental study designs.
Exclusion criteria
The following will be excluded from the review:
-
1.
Manuscripts that do not include original data about the effects of PA on cardiometabolic and psychosocial outcomes.
-
2.
Observational studies, case series, preprint, and theses will be excluded.
Information sources
We will conduct a search in five reference databases, as follows: PubMed, African Index Medicus, Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Embase. Articles published in any language will be included, being translated in Google translator when the language is not native to the authors. Reference lists of previous reviews and included papers will be searched to check for any further studies. The PubMed draft search strategy is presented in Additional file 2.
Selection of sources of evidence
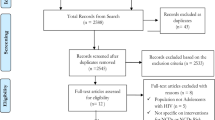
The review will be conducted in four phases: (i) searching for relevant articles using the search strategy, (ii) including or excluding articles based on their titles or abstracts, (iii) checking for article relevance in full-text articles, and (iv) looking for additional relevant articles by reviewing the reference lists of included articles and published relevant reviews.
Brief summary of data synthesis plan
Screening
The full search output will be imported into Covidence software (Veritas Health Innovation 2020) for screening. This software will also assist in managing the study records and data throughout the review. Two authors (S.Z.M and J.M-G) will screen the first 250 abstracts in duplicate, in sets of 50. When agreement between the 2 authors exceeds Cohen κ > 0.90 for 2 successive sets of 50 abstracts, a single reviewer (S.Z.M.) will screen the remaining abstracts.
Data extraction
Each selected study will be analyzed using a standardized consensual form adopted from Howlett et al. [53], to obtain the following data: characteristics of the sample, study design, study setting, intervention description, behavioral theories, PA measures used and results.
Specifically, we will extract the author’s name, year of publication, aim, inclusion and exclusion criteria for participants, characteristics of included participants (i.e., age, gender, stage of disease, comorbidity, and whether they were on ART).The following intervention details will also be recorded (name of the intervention (where applicable), exercise modality (i.e., aerobic, resistance or multimodal exercise), frequency and total duration of the intervention, setting, mode of delivery, theoretical framework informing the intervention, components of the intervention, and the summary of the findings), the outcomes of interest and their values at baseline and study completion, number of participants at baseline and study completion (including number of withdrawals), and the effectiveness and potential weaknesses of each intervention. In terms of PA outcome, the method of measuring PA, the number of participants randomly assigned and assessed, as well as the mean PA level at baseline and at post-intervention will be extracted. Missing data will be recorded as “missing in article”. Table 1 shows a summary of intervention content to be extracted.
Methodological quality of the included studies
An appropriate scale based on the study design of the article will be used to assess the methodological quality of the included studies. Specifically, the revised tool to assess risk of bias in randomized trials (RoB 2) [56] will be used to assess the methodological quality of the included randomized controlled trial studies. In terms of quasi-experimental study designs, methodological quality will be assessed using the relevant items from the Downs and Black [57] checklist. Using the 10-item criteria, studies will be given a positive (greater than 50% criteria met), neutral (50% criteria met), or negative (less than 50% criteria met) rating. Two persons (SZM and JM-G) will be assigned to independently review the quality of the studies. Where the reviewers do not agree, a third reviewer will be consulted (MS or MH) and the final decision regarding the rating of the study will be resolved by joint discussion and consensus among the reviewers as a group.
Certainty evidence
Certainty of evidence will be evaluated using the Grading of Recommendations Assessment, Development and Evaluation guidelines (GRADE) [58]. We will use the GRADE evaluation process to develop “Evidence Profiles” tables of the outcomes of interest in each included study based on full-text narrative abstraction and methodological quality scoring. The GRADE criteria will entail assessing the following five domains: risk of bias, inconsistency, imprecision, indirectedness, and publication bias. Certainty relating to the extent to which the body of evidence represents a true estimate of effect for each outcome will be deemed to be high, moderate, low, or very low in accordance with the GRADE criteria [58]. Table 2 shows the GRADE criteria. Studies start as high quality evidence but can be downgraded for serious flaws that violate the five domains of the GRADE criteria. For each GRADE table, we will provide an estimate of certainty or the strength of evidence (from high to very low) and a direction of effect (positive, no effect, or negative). However, we will only provide a GRADE for studies that score ≥ 50% on methodological quality rating. SZM and JM-G will be assigned to independently review the certainty of evidence. Where the reviewers do not agree, a third reviewer will be consulted (MS or MH) and the final decision regarding the rating of the study will be resolved by joint discussion and consensus among the reviewers as a group.
Synthesis and analysis of results
The emanating results found using the outlined methodology will provide a summary of the current research and an assessment of the quality of individual studies. Results will be reported in the form of a narrative synthesis summarizing data on the effectiveness and the characteristics/components of effective interventions to improve cardiometabolic and psychosocial outcomes among PWH in sub-Saharan Africa. The narrative will take the methodological quality of the studies and certainty of evidence into perspective. The review will also highlight the strengths and weaknesses of PA interventions amongst PWH in sub–Saharan Africa. Based on the evidence, recommendations will be made to improve and further strengthen the interventions.
Meta-analyses will be conducted if sufficient studies assess the same outcome (e.g., quality of life or change in weight), compare similar groups (e.g., standard of care versus a well-described PA intervention) and the articles provide the mean and standard deviation of the outcome variables immediately after the end of the intervention to evaluate the immediate between-group effects [59]. Meta-analyses will be conducted with Stata software version 17.0 (StataCorp LP, College Station, TX) computer software and the random-effects model for outcomes will be used. We will calculate the weighted mean difference (WMD) and 95% confidence intervals for the means for continuous outcomes whenever possible. On the other hand, for dichotomous outcomes, the odds ratio, absolute difference in odds, relative risk (RR), risk difference (RD), and the number needed to treat (NNT), and 95% confidence intervals will be calculated whenever possible. A p value of less than 0.05 will show statistical significance for overall effect of the intervention. For heterogeneity between studies (I2), a p value of less than 0.1 will be considered as statistically significant [60]. We will consider an I2 ≤ 40 as low heterogeneity, I2 > 40–75% as moderate and I2 > 75% as a high heterogeneity [61]. Subgroup analyses will be performed whenever possible to evaluate if PA interventions are associated with differences among the following pre-specified sub-groups: (1) female and male gender, (2) BMI > 30 (i.e., traditionally defined obesity) versus BMI < 30, (3) blood pressure: systolic > 120 mm Hg, diastolic > 80 mm Hg versus systolic < 120 mm Hg, diastolic < 80 mm Hg,(4) HbA1c < 5.7% versus > 5.7% and PA of < 150 min/wk versus > 150 min/week, (5) ART vs no ART at enrolment.
Discussion
This systematic review will identify and synthesize the current evidence regarding the effectiveness and characteristics of PA-based interventions to improve cardiometabolic and psychosocial outcomes among PWH in sub-Saharan Africa. We also hope to identify and highlight the strengths and weaknesses of these interventions. Additionally, based on the evidence, recommendations will be made on possible strategies to adopt when designing PA interventions for PWH in sub-Saharan Africa to improve and strengthen the selection of these interventions for recommendation, further study and/or implementation in public health programs.
It is important to assess the effectiveness and characteristics of PA interventions for PWH in sub-Saharan Africa because, regardless of the observed benefits, most PWH in sub-Saharan Africa are still not engaging in adequate PA as part of their health promotion activities [42] and withdrawal rates from PA programs in sub-Saharan Africa studies are up to 30% [23, 43, 44]. We focus on PWH in sub-Saharan Africa not only because of the high prevalence of HIV in the region, but also because PWH in sub-Saharan Africa face unique societal and health system challenges compared to other regions of the world and have particularly high rates of obesity with modern ART regimens [11, 12, 16, 62].
This review will aid researchers in designing effective and contextualized PA interventions for PWH in sub-Saharan Africa. We posit that an understanding of the effectiveness and characteristics of PA interventions for PWH in sub-Saharan Africa will assist in the design and implementation of context-sensitive interventions that are more suitable in the sub-Saharan African environment, and specifically for PWH. The recommendations emanating from this systematic review should serve well the needs of researchers, policy-makers, and other public health decision-makers in influencing the future agenda for efforts to explore and promote PA among PWH in sub-Saharan Africa.
Availability of data and materials
Not applicable.
Abbreviations
- ART:
-
Antiretroviral therapy
- CMD:
-
Cardiometabolic disease
- HIV:
-
Human immunodeficiency virus
- HbA1c:
-
Hemoglobin A1C
- HRQOL:
-
Health-related quality of life
- LS7:
-
Life’s Simple 7
- PA:
-
Physical activity; PWH: People living with HIV
References
UNAIDS. UNAIDS DATA 2021. Available at https://www.unaids.org/sites/default/files/media_asset/JC3032_AIDS_Data_book_2021_En.pdf. Accessed 24 May 2022.
Collaboration ATC. Life expectancy of individuals on combination antiretroviral therapy in high-income countries: a collaborative analysis of 14 cohort studies. The Lancet. 2008;372(9635):293–9. https://doi.org/10.1016/S0140-6736(08)61113-7.
Surur AS, Teni FS, Wale W, Ayalew Y, Tesfaye B. Health related quality of life of HIV/AIDS patients on highly active anti-retroviral therapy at a university referral hospital in Ethiopia. BMC Health Serv Res. 2017;17:737. https://doi.org/10.1186/s12913-017-2714-1.
Marcus JL, Leyden WA, Alexeeff SE, Anderson AN, Hechter RC, Hu H, Lam JO, Towner WJ, Yuan Q, Horberg MA, Silverberg MJ. Comparison of overall and comorbidity-free life expectancy between insured adults with and without HIV infection, 2000–2016. JAMA Netw Open. 2020;3(6):e207954. https://doi.org/10.1001/jamanetworkopen.2020.7954.
Feinstein MJ, Bahiru E, Achenbach C, Longenecker CT, Hsue P, So-Armah K, Freiberg MS, Lloyd-Jones DM. Patterns of cardiovascular mortality for HIV-infected adults in the United States: 1999 to 2013. Am J Cardiol. 2016;117(2):214–20. https://doi.org/10.1016/j.amjcard.2015.10.030.
Nguyen KA, Peer N, Kengne AP. Associations of gamma-glutamyl transferase with cardio-metabolic diseases in people living with HIV infection in South Africa. PloS One. 2021;16(2):e0246131. https://doi.org/10.1371/journal.pone.0246131.
Hsue P, Shreay S, Song X, Meyer N. A longitudinal analysis of comorbidities among human immunodeficiency virus (HIV) patients and matched non-HIV controls in the United States. Open Forum Infect Dis. 2016;3(1):950. https://doi.org/10.1093/ofid/ofw194.90.
WHO. Cardiovascular diseases (CVDs) fact sheet Vol 20202017. https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (2017). Accessed 14 May 2021.
Omech B, Sempa J, Castelnuovo B, Opio K, Otim M, Mayanja-Kizza H, Colebunders R, Manabe YC. Prevalence of HIV-associated metabolic abnormalities among patients taking first-line antiretroviral therapy in Uganda.Int Sch Res Notices. 2012. https://doi.org/10.5402/2012/960178.
Maganga E, Smart LR, Kalluvya S, Kataraihya JB, Saleh AM, Obeid L, Downs JA, Fitzgerald DW, Peck RN. Glucose metabolism disorders, HIV and antiretroviral therapy among Tanzanian adults. PloS One. 2015;10(8):e0134410. https://doi.org/10.1371/journal.pone.0134410.
Ogunmola OJ, Oladosu OY, Olamoyegun AM. Association of hypertension and obesity with HIV and antiretroviral therapy in a rural tertiary health center in Nigeria: a cross-sectional cohort study. Vasc Health Risk Manag. 2014;10:129–37. https://doi.org/10.2147/VHRM.S58449.
Malaza A, Mossong J, Bärnighausen T, Newell ML. Hypertension and obesity in adults living in a high HIV prevalence rural area in South Africa. Plos One. 2012;7(10):e47761. https://doi.org/10.1371/journal.pone.0047761.
Douglas PS, Umbleja T, Bloomfield GS, Fichtenbaum CJ, Zanni MV, Overton ET, Fitch KV, Kileel EM, Aberg JA, Currier J, Sponseller CA. Cardiovascular Risk and Health Among People With HIV Eligible for Primary Prevention: Insights From the REPRIEVE Trial. Clin Infect Dis. 2021. https://doi.org/10.1093/cid/ciab552.
Fonsah JY, Njamnshi AK, Kouanfack C, Qiu F, Njamnshi DM, Tagny CT, Nchindap E, Kenmogne L, Mbanya D, Heaton R, Kanmogne GD. Adherence to antiretroviral therapy (ART) in Yaoundé-Cameroon: association with opportunistic infections, depression, ART regimen and side effects. PLoS One. 2017;12(1):e0170893. https://doi.org/10.1371/journal.pone.0170893.
Ozemek C, Erlandson KM, Jankowski CM. Physical activity and exercise to improve cardiovascular health for adults living with HIV. Prog Cardiovasc Dis. 2020;63(2):178–83. https://doi.org/10.1016/j.pcad.2020.01.005.
Hill A., Venter W F, Delaporte E, Sokhela S, Kouanfack C, Moorhouse M, et al. Progressive rises in weight and clinical obesity for TAF/FTC/DTG and TDF/FTC/DTG versus TDF/FTC/EFV: ADVANCE and NAMSAL trials. Abstract MOAX0102LB. Oral abstracts of the 10th IAS Conference on HIV Science, 21–24 July 2019, Mexico City, Mexico. J Int AIDS Soc. 2019;22:92–92. https://doi.org/10.1002/jia2.2532
Dirajlal-Fargo S, Webel AR, Longenecker CT, Kinley B, Labbato D, Sattar A, McComsey GA. The effect of physical activity on cardiometabolic health and inflammation in treated HIV infection. Antivir. 2016;21(3):237–45. https://doi.org/10.3851/IMP2998.
Monroe AK, Brown TT, Cox C, Reynolds SM, Wiley DJ, Palella FJ, Kingsley LA, Plankey MW. Physical activity and its association with insulin resistance in multicenter AIDS cohort study men. AIDS Res Hum Retroviruses. 2015;31(12):1250–6. https://doi.org/10.1089/aid.2015.0027.
Brito-Neto JG, Andrade MF, Almeida VD, Paiva DC, Morais NM, Bezerra CM, Fernandes JV, Nascimento EG, Fonseca IA, Fernandes TA. Strength training improves body composition, muscle strength and increases CD4+ T lymphocyte levels in people living with HIV/AIDS. Infect Dis Rep. 2019;11(1):10–5. https://doi.org/10.4081/idr.2019.7925.
Zanetti HR, da Cruz LG, Lourenco CL, Neves FF, Silva-Vergara ML, Mendes EL. Does nonlinear resistance training reduce metabolic syndrome in people living with HIV? A randomized clinical trial. J Sports Med Phys Fit. 2016;57(5):678–84. https://doi.org/10.23736/s0022-4707.16.06294-0.
Domingues WJ, Nogueira VC, de Souza DC, Germano-Soares AH, Ritti-Dias R, Avelar A. Blood pressure responses after resistance exercise session in women living with human immunodeficiency virus/acquired immunodeficiency syndrome. J Exerc Rehabil. 2018;14(4):688. https://doi.org/10.12965/jer.1836212.106.
O’Brien KK, Tynan AM, Nixon SA, Glazier RH. Effectiveness of Progressive Resistive Exercise (PRE) in the context of HIV: systematic review and meta-analysis using the Cochrane Collaboration protocol. BMC Infect Dis. 2017;17(1):1–23. https://doi.org/10.1186/s12879-017-2342-8.
Mutimura E, Crowther NJ, Cade TW, Yarasheski KE, Stewart A. Exercise training reduces central adiposity and improves metabolic indices in HAART-treated HIV-positive subjects in Rwanda: a randomized controlled trial. AIDS Res Hum. 2008;24(1):15–23. https://doi.org/10.1089/aid.2007.0023.
O’Brien KK, Tynan AM, Nixon SA, Glazier RH. Effectiveness of aerobic exercise for adults living with HIV: systematic review and meta-analysis using the Cochrane Collaboration protocol. BMC Infect Dis. 2016;16(1):1–56. https://doi.org/10.1186/s12879-016-1478-2.
Pedro RE, Guariglia DA, Peres SB, Moraes SM. Effects of physical training for people with HIV-associated lipodystrophy syndrome: a systematic review. J Sports Med Phys Fit. 2017;57(5):685–94. https://doi.org/10.23736/s0022-4707.16.06234-4.
Heissel A, Zech P, Rapp MA, Schuch FB, Lawrence JB, Kangas M, Heinze S. Effects of exercise on depression and anxiety in persons living with HIV: a meta-analysis. J Psychosom Res. 2019;126:109823. https://doi.org/10.1016/j.jpsychores.2019.109823.
Nosrat S, Whitworth JW, Ciccolo JT. Exercise and mental health of people living with HIV: a systematic review. Chronic Illn. 2017;13(4):299–319. https://doi.org/10.1177/1742395317694224.
Ibeneme SC, Omeje C, Myezwa H, Ezeofor SN, Anieto EM, Irem F, Nnamani AO, Ezenwankwo FE, Ibeneme GC. Effects of physical exercises on inflammatory biomarkers and cardiopulmonary function in patients living with HIV: a systematic review with meta-analysis. BMC Infect Dis. 2019;19(1):359. https://doi.org/10.1186/s12879-019-3960-0.
Gomes-Neto MG, Conceição CS, Carvalho VO, Brites C. Effects of combined aerobic and resistance exercise on exercise capacity, muscle strength and quality of life in HIV-infected patients: a systematic review and meta-analysis. PloS One. 2015;10(9):e0138066. https://doi.org/10.1371/journal.pone.0138066.
Vancampfort D, Mugisha J, Richards J, De Hert M, Probst M, Stubbs B. Physical activity correlates in people living with HIV/AIDS: a systematic review of 45 studies. Disabil Rehabil. 2018;40(14):1618–29. https://doi.org/10.1080/09638288.2017.1306587.
Gleeson M, Bishop NC, Stensel DJ, Lindley MR, Mastana SS, Nimmo MA. The anti-inflammatory effects of exercise: mechanisms and implications for the prevention and treatment of disease. Nat Rev Immunol. 2011;11(9):607–15. https://doi.org/10.1038/nri3041.
Lim S, Choi SH, Jeong IK, Kim JH, Moon MK, Park KS, Lee HK, Kim YB, Jang HC. Insulin-sensitizing effects of exercise on adiponectin and retinol-binding protein-4 concentrations in young and middle-aged women. J Clin Endocrinol Metab. 2008;93(6):2263–8. https://doi.org/10.1210/jc.2007-2028.
Mujumdar PP, Duerksen-Hughes PJ, Firek AF, Hessinger DA. Long-term, progressive, aerobic training increases adiponectin in middle-aged, overweight, untrained males and females. Scand J Clin Lab Invest. 2011;71(2):101–7. https://doi.org/10.3109/00365513.2011.554995.
Lindegaard B, Hansen T, Hvid T, Van Hall G, Plomgaard P, Ditlevsen S, Gerstoft J, Pedersen BK. The effect of strength and endurance training on insulin sensitivity and fat distribution in human immunodeficiency virus-infected patients with lipodystrophy. J Clin Endocrinol Metab. 2008;93(10):3860–9. https://doi.org/10.1210/jc.2007-2733.
Bonato M, Galli L, Passeri L, Longo V, Pavei G, Bossolasco S, Bertocchi C, Cernuschi M, Balconi G, Merati G, Lazzarin A. A pilot study of brisk walking in sedentary combination antiretroviral treatment (cART)-treated patients: benefit on soluble and cell inflammatory markers. BMC Infect Dis. 2017;17(1):61. https://doi.org/10.1186/s12879-016-2095-9.
Rodrigues KL, Borges JP, Lopes GD, Pereira EN, Mediano MF, Farinatti P, Tibiriça E, Daliry A. Influence of physical exercise on advanced glycation end products levels in patients living with the human immunodeficiency virus. Front Physiol. 2018;9:1641. https://doi.org/10.3389/fphys.2018.01641.
Vancampfort D, Stubbs B, Mugisha J. Physical activity and HIV in sub-Saharan Africa: a systematic review of correlates and levels. Afr Health Sci. 2018;18(2):394–406. https://doi.org/10.4314/ahs.v18i2.25.
Martin K, Naclerio F, Karsten B, Vera JH. Physical activity and quality of life in people living with HIV. AIDS Care. 2019;31(5):589–98. https://doi.org/10.1080/09540121.2019.1576848.
Frantz JM, Murenzi A. The physical activity levels among people living with human immunodeficiency virus/acquired immunodeficiency syndrome receiving high active antiretroviral therapy in Rwanda. SAHARA J. 2013;10(3–4):113–8. https://doi.org/10.1080/17290376.2014.886081.
UNAIDS. Global HIV & AIDS statistics — Fact sheet. 2021. Available at https://www.unaids.org/en/resources/fact-sheet. Accessed 02 Sept 2021.
Shah AS, Stelzle D, Lee KK, Beck EJ, Alam S, Clifford S, Longenecker CT, Strachan F, Bagchi S, Whiteley W, Rajagopalan S. Global burden of atherosclerotic cardiovascular disease in people living with HIV: systematic review and meta-analysis. Circ J. 2018;138(11):1100–12. https://doi.org/10.1161/CIRCULATIONAHA.117.033369.
Schuelter-Trevisol F, H Wolff F, R Alencastro P, Grigoletti S, L Ikeda M, BM Brandao A, T Barcellos N, C Fuchs S. Physical activity: do patients infected with HIV practice? How much? A systematic review. Curr HIV Res. 2012;10(6):487–97. https://doi.org/10.2174/157016212802429794
Ezema CI, Onwunali AA, Lamina S, Ezugwu UA, Amaeze AA, Nwankwo MJ. Effect of aerobic exercise training on cardiovascular parameters and CD4 cell count of people living with human immunodeficiency virus/acquired immune deficiency syndrome: a randomized controlled trial. Niger J Clin Pract. 2014;17(5):543–8. https://doi.org/10.4103/1119-3077.141414.
Mangona L, Daca T, Tchonga F, Bule O, Bhatt N, Jani I, Damasceno A, Prista A. Suppl 1: M5: effect of different types of exercise in HIV+ Mozambican women using antiretroviral therapy. Open AIDS J. 2015;9:89. https://doi.org/10.2174/1874613601509010089.
Mugisha J, Ssebunnya J, Kigozi FN. Towards understanding governance issues in integration of mental health into primary health care in Uganda. Int J Ment Health. 2016;10(1):1–4. https://doi.org/10.1186/s13033-016-0057-7.
Dube L, Rendall-Mkosi K, Van den Broucke S, Bergh AM, Mafutha NG. Self-management support needs of patients with chronic diseases in a South African township: a qualitative study. J Community Health Nurs. 2017;34(1):21–31. https://doi.org/10.1080/07370016.2017.1260983.
National Academies of Sciences Engineering and Medicine. Crossing the global quality chasm: improving health care worldwide. Washington, DC: The National Academies Press; 2018. https://doi.org/10.17226/25152.
Maimela E, Van Geertruyden JP, Alberts M, Modjadji SE, Meulemans H, Fraeyman J, Bastiaens H. The perceptions and perspectives of patients and health care providers on chronic diseases management in rural South Africa: a qualitative study. BMC Health Serv Res. 2015;15(1):1–2. https://doi.org/10.1186/s12913-015-0812-5.
Rabkin M, Palma A, McNairy ML, Gachuhi AB, Simelane S, Nuwagaba-Biribonwoha H, Bongomin P, Okello VJ, Bitchong RA, El-Sadr WM. Integrating cardiovascular disease risk factor screening into HIV services in Swaziland: lessons from an implementation science study. AIDS (London, England). 2018;32(Suppl 1):S43. https://doi.org/10.1097/QAD.0000000000001889.
Brown JB, Nichols GA, Perry A. The burden of treatment failure in type 2 diabetes. Diabetes Care. 2004;27(7):1535–40. https://doi.org/10.2337/diacare.27.7.1535.
Schmittdiel JA, Uratsu CS, Karter AJ, Heisler M, Subramanian U, Mangione CM, Selby JV. Why don’t diabetes patients achieve recommended risk factor targets? Poor adherence versus lack of treatment intensification. J Gen Intern Med. 2008;23(5):588–94. https://doi.org/10.1007/s11606-008-0554-8.
Ellulu M, Abed Y, Rahmat A, Ranneh Y, Ali F. Epidemiology of obesity in developing countries: challenges and prevention. Global Epidemic Obes. 2014;2(1):2. https://doi.org/10.7243/2052-5966-2-2.
Howlett N, Trivedi D, Troop NA, Chater AM. Are physical activity interventions for healthy inactive adults effective in promoting behavior change and maintenance, and which behavior change techniques are effective? A systematic review and meta-analysis. Transl Behav Med. 2019;9(1):147–57. https://doi.org/10.1093/tbm/iby010.
Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, Eccles MP, Cane J, Wood CE. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46(1):81–95. https://doi.org/10.1007/s12160-013-9486-6.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-34. https://doi.org/10.1016/j.jclinepi.2009.06.006.
Sterne JA, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge SM, Emberson JR. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:4898. https://doi.org/10.1136/bmj.l4898.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiology Community Health. 1998;52(6):377–84. https://doi.org/10.1136/jech.52.6.377.
Balshem H, Helfand M, Schünemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401–6. https://doi.org/10.1016/j.jclinepi.2010.07.015.
Kwan RY, Salihu D, Lee PH, Tse M, Cheung DS, Roopsawang I, Choi KS. The effect of e-health interventions promoting physical activity in older people: a systematic review and meta-analysis. Eur Rev Aging Phys Act. 2020;17:7. https://doi.org/10.1186/s11556-020-00239-5.
Lau J, Ioannidis JP, Schmid CH. Quantitative synthesis in systematic reviews. Ann Intern Med. 1997;127:820–6. https://doi.org/10.7326/0003-4819-127-9-199711010-00008.
Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 7. rating the quality of evidence–inconsistency. J Clin Epidemiol. 2011;64:1294–302. https://doi.org/10.1016/j.jclinepi.2011.03.017.
Kintu A, Liu E, Hertzmark E, Spiegelman D, Zack RM, Muya A, et al. Incidence and risk factors for overweight and obesity after initiation of antiretroviral therapy in Dar es Salaam, Tanzania. J Int Assoc Provid AIDS Care. 2018. https://doi.org/10.1177/2325958218759759.
Acknowledgements
Not applicable.
Funding
This research was funded in whole, or in part, by Wellcome [Grant number Wellcome Strategic Core award: 201433/Z/16/A]. For the purposes of open access, the author has applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission.
Author information
Authors and Affiliations
Contributions
S.Z.M was the project facilitator and main author. J.G.M, M.H, J.C, and M.S all contributed toward the background, research design, and discussion. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA-P 2015 Checklist.
Additional file 2.
Search strategy for PubMed.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mabweazara, S., Manne-Goehler, J., Hamer, M. et al. Characteristics and efficacy of physical activity interventions to improve cardiometabolic and psychosocial outcomes in people living with HIV in sub-Saharan Africa: a protocol for a systematic review. Syst Rev 12, 24 (2023). https://doi.org/10.1186/s13643-023-02186-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-023-02186-5