
Abstract
Background
This research aimed to investigate the prognostic factors of oral squamous cell carcinoma (OSCC), especially the role of age.
Methods
A total of 33,619 cases of OSCC were received from the Surveillance, Epidemiology, and End Results (SEER) database during 2005–2015. Kaplan–Meier curves of 5-year overall survival rates and 5-year cancer-specific survival rates were performed, and univariate and multivariate Cox regression analyses as well as competing risk model were used to help understand the relationship between various factors and mortality of OSCC.
Results
Compared to 18–39-year-old group, the older age was an important predictor of worse prognosis. The multivariate analysis of overall survival (OS) was 50–59 years (HR, 1.32; 95% CI 1.17–1.48; p ≤ .001), 60–69 years (HR, 1.66; 95% CI 1.42–1.87; p ≤ .001) and 70 + years (HR, 3.21; 95% CI 2.86–3.62; p ≤ .001), respectively, while the specific value of competing risk model was 60–69 years (HR, 1.21; 95% CI 1.07–1.38; p = .002) and 70 + years (HR, 1.85; 95% CI 1.63–2.10; p ≤ .001). In addition, female gender, unmarried, Blacks, tumor in floor of mouth, size and higher Tumor Node Metastasis (TNM) classification were also other predictors that signify significant clinically deterioration of OS/cancer-specific survival (CSS).
Conclusions
Our research revealed that age was an important factor in explaining the difference of survival in the whole process of OSCC. It is suggested that we should pay attention to the influence of age on diagnosis, treatment and prognosis in the clinical process.
Similar content being viewed by others

Introduction
Oral squamous cell carcinoma (OSCC) is the most common histological type of oral cancer, with high morbidity and mortality, accounting for about 90% of oral cancer [1]. Important causes of oral squamous cell carcinoma include smoking, drinking and betel nut chewing [2, 3]. It is worth mentioning that in recent years, human papillomavirus has also been found to be one of the important causes of OSCC [4, 5], which has attracted widespread attention. In the early stages, OSCC are commonly asymptomatic, it is often at advanced-stage at the time of diagnosis. Early detection of precancerous lesions in OSCC can greatly improve the survival rate of patients [6]. In addition, the low survival rate of OSCC is also related to the fact that older patients have more complication, which make them more likely to be infected with other diseases and prematurely die. In addition, there are more adverse drug reactions due to aging organ functions than younger patients. Hence, it has been suggested that different treatment strategies should be given to the young and the old [7]. In this paper, we made a survival analysis based on information of patients with oral squamous cell carcinoma in different ages.
The acquisition of the real data of large number of patients has been one of the main problems faced by researchers in the research process. We used The Surveillance, Epidemiology, and End Results (SEER) national cancer database, a cancer registry maintained by the American College of surgeons and the American Cancer Society. It records the incidence rate, mortality and morbidity of millions of malignant tumors in some states and counties in the United States. The tumor information in the database was unified and standardized by SEER*stat software, and is regularly updated and released. Researchers all over the world can easily get data through application, which provides a good data source for clinical researchers. In addition, SEER database has a large sample size cover about 34.6% of the U.S. population and strong statistical efficiency, which promoted the high clinical reference value of researches based on SEER database.
Methods
Data source
We collected the clinicopathological data of all 33,619 adult patients (≥ 18 years) with primary oral squamous cell carcinoma from the years of 2004 to 2015 from the SEER database. The histological type codes for squamous cell carcinoma are 8070, 8071, 8072, 8073, 8074, 8075, and 8076, according to the third edition of the International Classification of Diseases for Oncology (ICD-O-3). Specific information includes age, gender, race, tumor location, grade, marital status, surgery, radiation, chemotherapy, T-level, N-stage and M-stage.
Data processing
The detailed steps are explained in Fig. 1. “Age”, as the main predictor, was clustered into five groups: 18–39, 40–49, 50–59, 60–69, 70 + . The SEER “stage” was used for tumor staging according to the seventh edition of the American Joint Committee on Cancer (AJCC) manual. In this study, the primary and secondary endpoints were overall survival and cancer-specific survival, which were analyzed based on the time of diagnosis, “status” and “cause-specific death classification”. In addition, we used the ICD-O-3 code to classify the site of oral tumors: floor of mouth (C04.0–4.1, C04.8–4.9), tongue (C01.9–2.4, C02.8–2.9), other (C03.0–3.1, C03.9, C05.0–5.2, C05.8–6.2, C06.8–6.9, C07.9–8.1, C08.9–9.1, C09.8–9.9). Moreover, the treatment methods were divided into the following groups: surgery, radiation, chemotherapy + XRT, surgery + XRT, others, triple therapy, no/unknown. Other variables available for statistical analysis were also standardized in the light of the definition of the SEER database.

Flow chart of OSCC patient data processing
Statistical analysis
All analyses were conducted in R-studio (version 4.0.2, https://www.r-proje ct.org/). We used the Kaplan–Meier method and log-rank test to obtain the Kaplan–Meier curves of 5-year overall survival rates and 5-year cancer-specific survival rates for each age, as well as Kaplan–Meier curves by age for each stage. To understand the relationship between other acquired factors and mortality of OSCC, univariate and multivariate Cox regression analyses were performed. The variables with p < 0.05 in univariate analysis were further analyzed by multivariate analysis.
Results
Patient recruitment and characteristics
A total of 33,619 cases in the SEER database were included in this study. The baseline characteristics of patients with OSCC are presented in Table 1. There were five groups stratified by age at diagnosis (18–39 years, 40–49 years, 50–59 years, 60–69 years, 70 + years). The incidence of OSCC was highest among 50–59 years (10,903, 13.24%), whereas the youngest group (18–39 years) had the least sample size. In addition, the proportion of male is much higher than that of women, especially in the group younger than 70 years. The most common site of cancer in the 18–39-year group was the tongue, which was different from other groups. The median follow‐up time of the whole cases and each group was 34 months, interquartile range 15–73 months (total), 52 months, interquartile range 19–96 months (18–39 years), 50 months, interquartile range 20–93 months (40–49 years), 40 months, interquartile range 17–79 months (50–59 years), 34 months, interquartile range 15–68 months (60–69 years), 22 months, interquartile range 9–51 months (70 + years), respectively.
Survival analyses of OSCC according to age at diagnosis
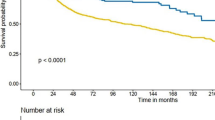
Figure 2A presents the 5‐year OS for OSCC decreased with age analyzed by Kaplan–Meier. With the extension of the follow-up time, the differences between the groups were larger. The oral squamous cell cancer-specific survival among 18–39-year, 40–49-year, 50–59-year, 60–69-year, 70 +-year group also gave a similar result (Fig. 2B), revealing that age had a major influence on survival time.

Kaplan–Meier survival curves and cumulative incidence function for 5-year OS/CSS. A Survival curve of patients with OSCC at different ages; B cumulative incidence function of patients with OSCC at different ages
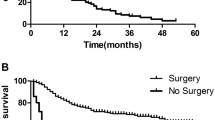
Kaplan–Meier survival curves as well as cumulative incidence function divided by age at each stage are produced (Figs. 3 and 4). The 5-year OS of stages I–II were similar to that of the general population, but for stages III and IV, only those aged over 60 had significant difference in survival rate, while the three groups of 18–39 years, 40–49 years and 50–59 years were similar, which indicated that age was an important factor in explaining the difference of survival, but not the only factor (Fig. 3). As for the result of CSS in different stages, the elderly group, especially 70 +-year and 60–69-year patients, still have a significant difference connection with cancer‐specific death (Fig. 4).

Kaplan–Meier survival curves grouped by age at each stage. A Survival curve of stage I OSCC patients at different ages; B survival curve of stage II OSCC patients at different ages; C survival curve of stage III OSCC patients at different ages; D survival curve of stage IV OSCC patients at different ages

Cumulative incidence function grouped by age at each stage. A Cumulative incidence function of stage I OSCC patients at different ages; B cumulative incidence function of stage II OSCC patients at different ages; C cumulative incidence function of stage III OSCC patients at different ages; D cumulative incidence function of stage IV OSCC patients at different ages
When we conducted univariate and multivariate analyses targeting overall survival (OS) and cancer‐specific survival (CSS), as expected, age, sex, marital status, race, tumor location and size, treatment, pathological grade and TNM staging were covariates in the adjusted model, which showed statistical significance (P < 0.05) (Tables 2, and 3). Older age (≥ 50 years) was an important predictor of worse prognosis at all stages compared with patients aged 18–39. The specific value was 50–59 years (HR, 1.32; 95% CI 1.17–1.48; p ≤ 0.001), 60–69 years (HR, 1.66; 95% CI 1.42–1.87; p ≤ 0.001) and 70 + years (HR, 3.21; 95% CI 2.86–3.62; p ≤ 0.001). While the competing risk model was 60–69 years (HR, 1.21; 95% CI 1.07–1.38; p = 0.002) and 70 + years (HR, 1.85; 95% CI 1.63–2.10; p ≤ 0.001). In addition, Tables 2 and 3 also reveal other predictors that signify significant clinically deterioration of OS/CSS in univariate and multivariate regression analyses included female gender, unmarried, Blacks, tumor in floor of mouth, size and higher TNM classification.
Discussion
Age has always been an important factor in the occurrence, development and prognosis of various tumor. Squamous cell carcinoma of the head and neck (HNSCC) is generally considered to be more frequent in the elderly, associated with tobacco and alcohol, and mainly occurs in men [8]. However, more and more young patients with HNSCC have been reported all over the world [9]. For the past few years, the incidence of OSCC has been on the rise, especially among young patients [10].The purpose of this SEER database analysis was to assess the clinical characteristics and risk factors of OSCC in different age groups. At the same time, understanding of other factors (gender, tumor size, histological grade, treatment, etc.) that affect the premature death of patients will help to formulate the corresponding treatment plan in advance and improve the survival rate. To our knowledge, this study is the first to observe the possible differences stratified by age in studies with a large sample size.
As we expected, whether it is OS or CSS, the research shows that the survival time of patients decreases orderly and stepwise with the increase of age group. This result is consistent with other large cohort studies that have been published. A study carried out in Brazil shown that age has a strong impact on mortality from oral and oropharyngeal cancer. The risk increases from 40 years for men to 55 years for women and the effect of the overall period was observed [11]. Laith et al. reported that their study indicated improved OS and disease-specific survival in young patients with oral tongue squamous cell carcinoma (OTSCC) [12]. However, another interesting finding of the regression analysis is that compared with the higher age group, people aged < 30 showed a higher probability of transition, which is not statistically significant [13]. Younger age at diagnosis even was found to be a risk factor for the development of pleural metastasis [14]. In general, the effect of age on the prognosis of OSCC is still controversial. Although a number of studies have made different results, they are unable to explain the etiology and pathological mechanism in detail. From our analysis of the results, young patients (18–39) had a higher rate of surgery (34.11%) and triple therapy (32.05%), indicating that they tend to accept more aggressive treatments.
It has reported that 5-year survival rates for patients with oral squamous cell carcinoma vary greatly by stage, from about 90% in the early stage to about 30% in the late stage [15]. Surgery is the main treatment for early (Stages I–II) oral squamous cell carcinoma. Advanced (Stages III–IV) disease indicates difficulty in obtaining a clear incision margin, which means a higher recurrence rate. Under the circumstance, adjuvant therapy is appropriate [16]. Our research found that age has different effects on prognosis at different stages. In the early stage, the patient's survival period decreased with increasing age. As the stage progresses, the impact of different age groups on the prognosis is less obvious, which is mainly reflected in the poor prognosis of the elderly. Therefore, clinical staging at diagnosis is important and can be used as a predictor of recurrence and death in patients with OSCC.
Based on the results of previous studies, the most common major sites involved in OSCC vary by geographic location. The buccal mucosa is more common in Asian populations, including South Asia, Sri Lanka, etc., where 40% of oral cancers are found in the buccal mucosa due to the common practice of men and women chewing betel nut/tobacco. In contrast, the tongue is the most common site of oral cancer in European and American populations, accounting for 40–50% of oral cancers [17, 18]. The main source of cases in our study is mostly white Americans and our results for the location of OSCC are also within this range. It is worth noting that the proportion of tongue cancer patients is the highest in the 18–39-year-old group (69.29%). This is consistent with a previous study based on a global database analysis [19]. However, the incidence factors of young people are still unclear, and may be related to changes in the etiology of oral cancer, such as human papilloma virus (HPV) infection. In addition, the Centers for Disease Control and Prevention (CDC) and the Food and Drug Administration (FDA) analyzed data from the 2011–2015 National Youth Tobacco Survey (NYTS) and determined that the use of e-cigarettes and hooks by middle school students has increased significantly, and the trend is much larger than that of adults [20]. However, it is still necessary to further investigate the influence of young people’s eating habits, lifestyle and other factors on their incidence and tumor location.
As a retrospective study, we acknowledge that there are certain limitations to the study. As for SEER database, a large population retrospective database, inevitably, it has some drawbacks. It does not provide the data of detailed immunohistochemical analysis, for example. It also lacks related chemotherapy or radiotherapy regimens. However, the strengths of our study include a large nationally representative sample, meticulous grouping of age, as well as a wealth of other relevant factors.
Conclusions
Our study revealed that age was an independent predictor of both OS and CSS in the oral squamous cell carcinoma patients, and more aggressive treatments (surgery, triple therapy) tend to be used in young patients, which can provide certain reference value for the current clinical diagnosis and treatment.
Availability of data and materials
The data sets generated and/or analyzed during the current study are freely available in the SEER repository, [https://seer.cancer.gov/seerstat/].
Abbreviations
- OSCC:
-
Oral squamous cell carcinoma
- OS:
-
Overall survival
- CSS:
-
Cancer-specific survival
- SEER:
-
The Surveillance, Epidemiology, and End Results
- TNM:
-
Tumor node metastasis
- CI:
-
Confidence interval
- HR:
-
Hazard ratios
- AJCC:
-
American Joint Committee on Cancer
- XRT:
-
X-ray diffraction topography
- HNSCC:
-
Squamous cell carcinoma of the head and neck
- HPV:
-
Human papilloma virus
- CDC:
-
Centers for Disease Control and Prevention
- FDA:
-
Food and Drug Administration
- NYTS:
-
National Youth Tobacco Survey
References
Dewan AK, Dabas SK, Pradhan T, Mehta S, Dewan A, Sinha R. Squamous cell carcinoma of the superior gingivobuccal sulcus: an 11-year institutional experience of 203 cases. Jpn J Clin Oncol. 2014;44(9):807–11.
Oji C, Chukwuneke F. Poor oral hygiene may be the sole cause of oral cancer. J Maxillofac Oral Surg. 2012;11(4):379–83.
Tsai S, Wong T, Ou C, Fang S, Chang J. The interplay between alcohol consumption, oral hygiene, ALDH2 and ADH1B in the risk of head and neck cancer. Int J Cancer. 2015;135(10):2424–36.
Rooper LM, Windon MJ, Hernandez T, Miles B, Ha PK, Ryan WR, et al. HPV-positive squamous cell carcinoma of the larynx, oral cavity, and hypopharynx: clinicopathologic characterization with recognition of a novel warty variant. Am J Surg Pathol. 2020;44(5):691–702.
Johnson DE, Burtness B, Leemans CR, Lui VWY, Bauman JE, Grandis JR. Head and neck squamous cell carcinoma. Nat Rev Dis Primers. 2020;6(1):92.
Silverman S, Kerr AR, Epstein JB. Oral and pharyngeal cancer control and early detection. J Cancer Educ. 2010;25(3):279–81.
Yamada S-I, Kurita H, Nakano R, Ohta R, Akita D, Hashidume M, et al. Treatment strategies for and outcomes of older patients with oral squamous cell carcinoma. Oral Surg Oral Med Oral Pathol Oral Radiol. 2020;129(4):322–9.
Hashibe M, Brennan P, Chuang SC, Boccia S, Castellsague X, Chen C, et al. Interaction between tobacco and alcohol use and the risk of head and neck cancer: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. Cancer Epidemiol Biomarkers Prev. 2009;18(2):541–50.
Majchrzak E, Szybiak B, Wegner A, Pienkowski P, Pazdrowski J, Luczewski L, et al. Oral cavity and oropharyngeal squamous cell carcinoma in young adults: a review of the literature. Radiol Oncol. 2014;48(1):1–10.
Hussein AA, Helder MN, de Visscher JG, Leemans CR, Braakhuis BJ, de Vet HCW, et al. Global incidence of oral and oropharynx cancer in patients younger than 45 years versus older patients: a systematic review. Eur J Cancer. 2017;82:115–27.
Perea LME, Antunes JLF, Peres MA. Oral and oropharyngeal cancer mortality in Brazil, 1983–2017: age-period-cohort analysis. Oral Dis. 2022;28(1):97–107. https://doi.org/10.1111/odi.13732
Mukdad L, Heineman TE, Alonso J, Badran KW, Kuan EC, St John MA. Oral tongue squamous cell carcinoma survival as stratified by age and sex: a surveillance, epidemiology, and end results analysis. Laryngoscope. 2019;129(9):2076–81.
Siriwardena BSMS, Rasnayaka RMSGK, Masood Y, Masood M, Kumarasiri PVR, Tilakaratne WM. Predictive model of oral cancer metastasis for different cancer sites and age groups. J Investig Clin Dent. 2016;7(2):127–31.
Shao Y-Y, Hong R-L. Pleural metastases as a unique entity with dismal outcome of head and neck squamous cell carcinoma. Oral Oncol. 2010;46(9):694–7.
Omar E. Current concepts and future of noninvasive procedures for diagnosing oral squamous cell carcinoma—a systematic review. Head Face Med. 2015;11:6.
Fridman E, Na’ara S, Agarwal J, Amit M, Bachar G, Villaret AB, et al. The role of adjuvant treatment in early-stage oral cavity squamous cell carcinoma: an international collaborative study. Cancer. 2018;124(14):2948–55.
Shibahara T. Oral cancer-diagnosis and therapy. Clin Calcium. 2017;27(10):1427–33.
Siriwardena BSMS, Tilakaratne A, Amaratunga EAPD, Tilakaratne WM. Demographic, aetiological and survival differences of oral squamous cell carcinoma in the young and the old in Sri Lanka. Oral Oncol. 2006;42(8):831–6.
Ghantous Y, Abu EI. Global incidence and risk factors of oral cancer. Harefuah. 2017;156(10):645–9.
Singh T, Arrazola RA, Corey CG, Husten CG, Neff LJ, Homa DM, et al. Tobacco use among middle and high school students—United States, 2011–2015. MMWR Morb Mortal Wkly Rep. 2016;65(14):361–7.
Acknowledgements
Not applicable.
Funding
This study was supported by The Research Project of Zhejiang Chinese Medical University (2021RCZXZK10).
Author information
Authors and Affiliations
Contributions
JJY and KBG: contributed to the conception and design of the work, drafted and critically revised the manuscript, made the equal contribution to this paper; ALZ, YZ and WDL: contributed to the acquisition, analysis of data and drafted the work; PPW and JRY: contributed to the conception of the work, the analysis of data and critically revised the manuscript; All authors read and approved the final manuscript. The authors would like to thank Dr. Leitao Sun, Dr. Shanming Ruan and Shuning Ding for their technical assistance.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
1. SEER database, a cancer registry maintained by the American College of surgeons and the American Cancer Society, is the authoritative cancer statistical database in the United States, which has its own ethical approval; 2. because it is a public anonymous database, our hospital ethics has no related approval. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, J., Guo, K., Zhang, A. et al. Survival analysis of age-related oral squamous cell carcinoma: a population study based on SEER. Eur J Med Res 28, 413 (2023). https://doi.org/10.1186/s40001-023-01345-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-023-01345-7