
Abstract
Background
A detailed understanding of the genetic basis of cancer is of great interest to public health monitoring programs. Although many studies have been conducted in Brazil, a global view on the molecular profile related to hereditary breast and ovarian cancer (HBOC) in this large and heterogeneous population is lacking.
Methods
A systematic review following the PRISMA guidelines was conducted in three electronic databases (PubMed, BIREME and SciELO). Brazilian studies covering molecular analysis of genes related to HBOC, published until December 2023, were considered.
Results
We identified 35 original studies that met all the inclusion criteria. A total of 137 distinct mutations were found in the BRCA1 gene, but four of them corresponded to 44.5% of all mutations found in this gene. The c.5266dupC BRCA1 mutation was responsible for 26.8% of all pathogenic mutations found in the BRCA1 gene in patients with clinical criteria for HBOC from the Brazilian population. Considering all studies that track this mutation in the BRCA1 gene, we found a frequency of 2% (120/6008) for this mutation in Brazilian patients. In the BRCA2 gene, the four most frequent mutations corresponded to 29.2% of pathogenic mutations. Even though it was tracked by few studies, the c.156_157insAlu mutation was responsible for 9.6% of all pathogenic mutations reported in the BRCA2 gene. Seventeen studies found pathogenic mutations in other non-BRCA genes, the c.1010G > A mutation in the TP53 gene being the most frequent one. Considering all studies that screened for this specific mutation in patients with the clinical criteria for HBOC, the frequency of c.1010G > A was estimated at 1.83% (61/3336).
Conclusions
Despite significant molecular heterogeneity among mutations in HBOC patients from Brazil, three mutations deserve to be highlighted, c.5266dupC, c.156_157insAlu and c.1010G > A in the BRCA1, BRCA2 and TP53 genes, respectively. With more than 200 records, these three mutations play a vital role in the pathology of breast and ovarian cancer in Brazil. The data collected shed light on the subject, but there is still not enough data from certain subpopulations.
Similar content being viewed by others

Introduction
Hereditary breast and ovarian cancer (HBOC) accounts for 5–10% of all breast cancer (BC) cases and is inherited in an autosomal dominant manner. The large number of cases of HBOC syndrome are caused by the presence of germline mutations in either the BRCA1 or the BRCA2 gene [1]. Women with pathogenic BRCA1/2 variants have up to an 87% risk of developing an associated cancer, while men have up to a 20% risk [2]. However, not all cases of HBOC can be assigned to BRCA1 and BRCA2, as more than 20 other genes have been associated with an increased risk of familial breast and/or ovarian cancer [3].
In Brazil, the estimated incidence of breast cancer was 73.610 new cases for 2023. Considering cases by region, the estimate for breast cancer in women was higher in the Southeast (84.46/100 thousand inhabitants), followed by the South (71.44/100 thousand inhabitants), Midwest (57.28/100 thousand inhabitants), Northeast (52.20/100 thousand inhabitants) and North (24.99/100 thousand inhabitants). Ovarian cancer is less frequent than breast cancer, with 7.310 new cases estimated for 2023. However, it is one of the most common cancers in Brazil. The regions of Brazil with the highest gross incidence rates per 100,000 inhabitants are the South, followed by the Southeast and Northeast, with lower rates in the North and Midwest regions [4].
The risk of developing breast and ovarian cancer may differ according to the mutations present in the individual’s genes, as well as their nationality and family history. Even though BRCA mutations occur in all ethnic groups, their prevalence varies among different countries and diverse groups within the same country [5]. Recognition of a genetic predisposition to cancer, the preventive measures available to healthy women with a BRCA mutation and the personalized cancer therapies available for BRCA-positive patients have reinforced the indication for BRCA testing worldwide. Currently, clinical and genetic analyses can guide the choice of treatment and the selection of the combination of antineoplastic agents to be used in a specific case [6].
Genetic testing remains expensive and inaccessible for most women in developing countries. A limited number of studies in the Brazilian population have focused on BRCA sequencing or screening for specific mutations in some HBOC-related genes. With the advent of next-generation sequencing (NGS) and the possibility of evaluating a panel of genes related to cancer simultaneously, the number of studies with this aim has increased in the Brazilian population [7]. However, there are still few studies, and most of them are restricted to a specific region of the country [6, 8]. Despite all this diversity, the only study reporting a more representative profile of HBOC mutations in Brazil was performed by laboratory reports showing pathogenic or likely pathogenic germline mutations from tests performed for BRCA1 and BRCA2 from several public and private health located in different Brazilian states [9].
The Brazilian population is one of the most heterogeneous in the world and originated from three major ethnic groups: Portuguese, Africans and Amerindians. Other minor groups also contributed to the genetic plurality of the country [10]. As the pattern of ethnic diversity in Brazil is complex, the objective of this review is to provide an update on the molecular basis of the HBOC syndrome in a very diverse population that differed in the occupation process during the time of colonization and to demonstrate the geographic variability of the genetic mutations described within the country.
Methods
This systematic review was reported according to the Preferred Reporting Items for Systematic reviews and Meta‐analysis (PRISMA) guidelines [11]. Study selection was conducted in three phases: identification, screening and eligibility. Two independent researchers performed the initial study identification by searching three databases, PubMed, SciELO and BIREME. The bibliographic search included all studies published until december 2023. The descriptors HBOC AND Brazil, Hereditary Breast and Ovarian Cancer AND Brazil and BRCA mutations AND Brazil were cross-checked with each database. The inclusion criteria were primary articles covering molecular analysis of genes related to HBOC in Brazil in unrelated patients with breast and/or ovarian cancer or HBOC patients. The exclusion criteria were primary articles not covering molecular analysis related to HBOC genes in Brazil, review articles, studies that did not report the variants found, those which used non-Brazilian populations, and those articles that studied only somatic mutations. A systematic review flowchart was developed following the PRISMA specifications.
In the screening phase, all duplicate articles and those in which the title or subject of the abstract was outside the study objective, were excluded. In the eligibility phase, articles where all the full content was outside the main objective were excluded. To reduce bias in the data analysis, an email was sent to authors with similar works. The articles were analysed by two different evaluators, and those that met the inclusion criteria were selected for this review.
The Human Genome Variation Society (HGVS) nomenclature was followed despite some articles describing the mutations with different nomenclatures and the reference transcripts for each mutation can be accessed in ClinVar database.
Results
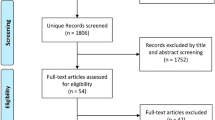
The database search generated a total of 296 records (Fig. 1). Of these, 158 were excluded after checking for duplication between databases. Our literature search returned 136 records from the three databases, and two articles were added from other sources (e.g., cross-references), resulting in 138 records. Eighty-one articles were excluded on the basis of their titles and abstracts. We evaluated the full text of 57 studies considered potentially eligible by the two authors and, after analysis, 22 manuscripts were removed because they did not meet the inclusion criteria. In the end, 35 studies were eligible for qualitative synthesis.

Flowchart representing the process of screening and selection of eligible studies, based on Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines [11]
According to the Brazilian regions studied, most of the articles described HBOC populations in the Southeast and South regions of the country, with few studies in the Northeast and Midwest (Fig. 2). Most of the patients came from the states of São Paulo, Rio de Janeiro and Rio Grande do Sul. However, it is not possible to obtain information about the place of birth for most of the patients included in the studies. Therefore, data on geographic location should be interpreted with caution.

Geographical distribution of the studies included in this review according to the regions of Brazil. Each black line indicates the number of studies with samples from the respective region of the country (they are not distributed on the map according to the state or municipality localization). Red lines indicate the number of studies with samples from South and Southeast regions. The blue lines indicate studies that used populations from more than two regions (South, Southeast and Northeast). *Only two study included samples from all regions of the country
When analyzing the distribution of articles per year, we found that the first Brazilian molecular evaluation study for HBOC was conducted in 2004. Ten articles were published in the next decade and Sanger sequencing was the most used technology. Several other techniques were employed, alone or in association with others, such as: Single-Stranded Conformation Polymorphism (SSCP), Denaturing Gradient Gel Electrophoresis (DGGE), Protein Truncation Test (PPT), Restriction Fragment Length Polymorphism (RFLP), Denaturing High Performance Liquid Chromatography (DHPLC), Allele-specific PCR (AS-PCR), multiplex PCR, High Resolution Melting (HRM), Real-time PCR (qPCR), Microarray and Multiplex Ligation-dependent Probe Amplification (MLPA). The first articles using NGS were from 2016 and in 2018 the first multigene analysis for non-BRCA genes was performed. From this date to now the NGS methodology has stood out as the method of choice. A timeline with all the articles identified, as well as the methods used, can be seen in (Fig. 3).

Timeline showing the distribution of Brazilian studies and all methods used to track mutations in HBOC populations
Among the 35 papers reviewed, 18 screened the complete BRCA genes, four using NGS technology only for BRCA genes, four using Sanger sequencing, four using both methodologies and the last six studies using NGS panels including BRCA genes. Only two studies performed NGS panel in which BRCA genes were not included and one was performed using next generation sequencing just for TP53 gene. There were three studies that tracked only the complete BRCA1 gene with or without analysis of point mutations in other genes, and nine studies used various techniques for tracking specific mutations or analyzing isolated exons. Only one study performed exome analysis and another one, only the MLPA technique. It is important to emphasize that among all the studies mentioned above, 15 of them also analyzed rearrangements in BRCA genes by MLPA.
Twenty-nine studies which examined BRCA mutations were verified, 22 of which reported finding mutations in both the BRCA1 and BRCA2 genes. Among 18 studies where whole BRCA genes were sequenced, the frequency of mutations in the BRCA1 gene was considerably higher than that in BRCA2 in 16 of them. Seventeen articles describing mutations in genes other than BRCA were found, and the majority of mutations were in the TP53, MUTYH, ATM, PALB2 and CHEK2 genes.
The description of the pathogenic mutation frequency found in each gene distributed by region of the country is shown in Table 1. Variants of unknown significance (VUS) were not included in this review.
A database was created with all pathogenic mutations identified in the reviewed articles (Additional file 1). Studies that reported the use of the same sample in two different studies were excluded. Considering all the works included in this review, a total of 137 distinct mutations were found in the BRCA1 gene (Additional file 1), but four of them (Table 2) correspond to 44.5% of all pathogenic mutations in this gene in the Brazilian population. In the BRCA2 gene, 127 different mutations were identified (Additional file 1) and the four most frequent mutations corresponded to 29.2% of pathogenic mutations in this gene (Table 2). The most common mutations in BRCA genes found in the Brazilian population so far are described in (Table 2).
Discussion
Brazil is one of the most populous countries in the world, and it has a great ethnic diversity that varies from state to state due to the colonization process that took place in the years 1500. According to the Brazilian Institute of Geography and Statistics (IBGE), in 2022 the Brazilian population reached 203 million inhabitants, making it the seventh most inhabited country in the world. Among the regions, the Southeast is the most populous, with about 85 million people. The Northeast has 54 million inhabitants and the South is home to approximately 30 million people. The North is the largest Brazilian region in terms of territorial extension (45% of the national territory), however, with about 17 million inhabitants. The Midwest region has a little more than 16 million inhabitants, making it the least populated region in the country. Regarding livelihood distribution, the Southeast and South regions have approximately twice the per capita household income of the North and Northeast regions [46, 47]; the latter also has fewer centers for molecular diagnosis and care for cancer patients [48].
The North region of Brazil appeared in only two study in this review, and the above data may partly explain why the vast majority of studies found were from the Southeast and South regions. Although we did not find other studies with populations from the North region, a previous study described reports of BRCA1 and BRCA2 tests from several Brazilian states, and 20 reports from the North region were described. The authors compiled the testing reports of probands with pathogenic/likely pathogenic variants referred to public and private health care centers distributed across 11 Brazilian States. They found two variants unique to this region [9]. This study was not targeted at the identification stage with the descriptors used and it was not clear whether part of the data presented had already been reported by previous primary studies. For this reason, it was not included in this review. Another study carried out in the north of the country found that three variants of the BRCA2 gene, commonly linked to hereditary breast cancer, had a significantly higher allele frequency in Amazonian compared to other ethnic groups analyzed (Africans, Americans, Europeans and Asians) in control samples [49].
The first Brazilian study to include molecular evaluation of HBOC-related genes was published in 2004 by Lourenço et al. [34] and was based on screening only the BRCA1 gene, followed by Dufloth in 2005 [26], who sequenced some exons of the BRCA1 and BRCA2 genes. The following studies, in subsequent years, also screened for point mutations or sequencing of some exons in BRCA genes [33, 35, 40, 43]. Only in 2013 the complete sequencing of the BRCA genes was conducted in Brazil by Carraro et al. [27], and other genes began to be explored in a punctual way [13, 18, 21]. From 2014 onwards, more works were published each year, and other genes related to HBOC were analysed more frequently, mainly TP53 and CHEK2. Until 2014, Sanger sequencing was unanimous, although other screening techniques were also used in conjunction. The NGS platform was launched in 2005, and although the spectrum of articles found in this review ranges from 2004 to 2023, the first articles to use NGS for HBOC studies were published in 2016 [15, 19, 25]; however, none of them screened for other susceptibility genes. The first to study a panel including other genes were Timoteo et al. in 2018 [12], with 11 genes related to hereditary breast cancer, and the only one to carry out a multigene analysis in the Northeast region. Overall, most articles from 2020 to 2023 performed multigene screening in HBOC patients from Brazilian population. Only a single study used a more advanced technique, whole exome sequencing, to identify new genes related to breast and/or ovarian cancer [22].
There was high variability in the frequency of the mutations found among the 35 articles analyzed. The detection percentage of pathogenic mutations varied from 0.0% to 29.5% among the studies. These major differences may be due to the inclusion criteria used in each study, the genes evaluated, the wide variation in the techniques used and the prevalence of BRCA mutations among different ethnicities. Individuals who meet multiple criteria are more likely to carry a pathogenic variant in BRCA genes [14]. Works that performed the complete sequencing of BRCA genes found higher rates of mutations in the population [7, 18, 31], contrasting with those tracking for point mutations as expected [16, 30, 42]. Only one study performed whole-exome sequencing [22], and mutations were found in genes not reported in any other study.
The pathogenic mutation frequency was higher in the BRCA1 than in the BRCA2 gene in most of the studies that performed complete BRCA sequencing. In these works, the frequency of mutations found in both BRCA genes ranged from 0.5% to 17%. Only two studies, in Minas Gerais and São Paulo states reported a higher frequency of BRCA2 mutations compared to BRCA1 [29, 31]. Of the 35 studies analysed, 17 studies found pathogenic mutations in other genes, with a total of 28 mutated genes: ATM—ATR—BARD1—BIRP1—BLM—CDH1—CHEK2—CTNNA1—CTNNA2—DROSHA—FANCC—HERPUD1—LCP1—MLH1—MRE11A—MSH2—MSH6—MUTYH—NBN PALB2—PLK2—PTCH1—PMS2—RAD51C—RAD51D—RECQL4—RIPK1 and TP53.
In this review, 23 studies described variants of unknown significance (VUS) in their results. These variants create an obstacle to patient diagnosis, since they raise doubts about their real role in the pathology of breast cancer. Different criteria have been adopted to indicate the pathogenicity of VUS as bioinformatics, frequency in a control population and functional studies. However, classification is not always possible. Although 23 articles reported the presence of VUS, we believe that others also found it but did not report it, mainly the works that used the NGS methodology. Therefore, a more in-depth study within the database of each work is necessary to expand our knowledge of VUS in Brazil.
After analyzing the database with pathogenic mutations most frequently identified in BRCA genes and excluding studies with overlapping samples, we can verify that the c.5266dupC mutation in BRCA1 is the most commonly found in Brazil in patients with breast and/or ovarian cancer. The c.5266dupC mutation was first described as a founder effect in the Ashkenazi Jewish population [50, 51]. This mutation was found in 20 of 24 studies where it was investigated, and the highest frequencies found in Brazilian studies were 11.6% (11/95) followed by 8.5% (4/47) and 5.1% (7/137), all from the Southeast and South regions [7, 35, 41]. Although the mutation BRCA1 c.5266dupC has been reported in different regions of Brazil, it is more frequently found in populations with Central and Eastern Europe ancestors [49]. Considering all studies that track this mutation in the BRCA1 gene, we found a frequency of 2% (120/6008) for this mutation in Brazilian patients (Additional file 1). The results reported here are in accordance with Palmero et al. [9], where the c.5266dupC mutation was found as the most frequent mutation, representing to 20.2% of all variants found in the BRCA1 gene in Brazil. In this review, this mutation corresponded to 26.8% of all pathogenic mutations found in the BRCA1 gene.
The c.3331_3334delCAAG mutation was the second most frequent mutation found in the BRCA1 gene, with a total of 49 records distributed among twelve studies. Represented in different populations, it was first described in Canadian families [52]. To know the origin of this mutation, a study conducted in 2020 by Tuazon and collaborators [53] performed haplotype analysis with populations from Colombia, Spain, Portugal, Chile, Africa and Brazil and suggested that this mutation had a single origin in the Iberian Peninsula and was introduced in Colombia and South America at the time of Spanish colonization. This mutation was responsible for 10.2% of BRCA1 mutations found in Brazil in this review.
The c.211A > G mutation was the third most frequent in the BRCA1 gene been responsible for 3.8% of mutations in this gene. It is a mutation of Spanish origin and consists of a Galician founder mutation [54]. The c.1687C > T mutation was found in eight different studies with samples from all regions of Brazil, being the fourth most reported variant in HBOC patients in the Brazilian population. It was identified with an allele frequency of 0.000006576 in the general population and 0.00001471 in the European (non-Finnish) population, by the Genome Aggregation Database (gnD: https://gnomad.broadinstitute.org/).
The most frequent mutation found in the BRCA2 gene was c.156_157insAlu, although it was tracked by few studies. This mutation was classified as a founder due to the high frequency described in the Portuguese population [55]. The high occurrence of this mutation in Brazil possibly involves the arrival of Portuguese immigrants to Brazilian lands during centuries of colonization. The frequency of this mutation in HBOC patients from Brazilian studies varied from 0.007 to 2.06%. As many studies did not track this mutation, which requires a specific PCR reaction, and we have no information as to whether the studies that used MLPA included probes for this region, it was not possible to check their global frequency in HBOC patients from Brazil. This mutation was responsible for 9.6% of all pathogenic mutations reported in the BRCA2 gene, and we strongly suggest that it be screened in Brazilian patients. The c.2808_2811delACAA mutation in the BRCA2 gene was observed in nine Brazilian studies. It was the second most recurrent mutation in the BRCA2 gene reported in 25 patients from different regions of the country. This mutation was described in seven different countries in Western Europe and North America, and it was considered a Norwegian founder mutation [56, 57].
The c.6405_6409delCTTAA mutation was the third most frequent in the BRCA2 gene, reported in seven Brazilian studies. It was first described as 6630del5 in a study that tracked 25 families with breast and/or ovarian cancer cases in the UK and Ireland [58]. This mutation demonstrates an allele frequency in the global population of 0.000004156 in the gnomAD database.
The c.2 T > G mutation was the fourth most frequent mutation found in the BRCA2 gene, with a total of twelve records in this review. It has been reported in Portuguese families [59] and published in population databases with a total allele frequency of 0.000007957 and 0.00005784 in a mixed Latin American population by gnomAD.
The most frequently mutated gene after BRCA1/2 was TP53. The variant c.1010G > A (p.R337H) is a Brazilian founder mutation, identified in 0.3% of the general population in South Brazil [60]. Many other studies about this mutation have been conducted in the Brazilian population and were not included in this review because of the descriptors used here. This mutation is associated with a variety of cancers, most notably those of the Li-Fraumeni syndrome spectrum. However, several studies have associated the presence of this mutation with breast cancer and the HBOC syndrome [21, 61]. In a previous study with cancer patients and HBOC/HBCC patients from the South region, the mutation c.1010G > A was found with a frequency of 8.6% and 3.4%, respectively [62]. In this review, the frequency of this mutation ranged from 0.8% to 7.1% among HBOC patients. The highest frequency was identified in the study by Cury et al. [21] (2/28) and the lowest in Gomes et al. [36] (1/126). Of 16 studies that tracked the TP53 gene, 13 found pathogenic mutations, and 11 of them found the c.1010G > A variant. Considering all studies that screened for this specific mutation, the frequency of c.1010G > A in patients who met clinical criteria for HBOC from Brazil was estimated in 1.83% (61/3336) (Additional file 1). This lower frequency, compared to that found by Giacomazzi et al. [62] in HBOC patients, could reflect the greater variability of populations studied in this review, as here, in addition to the South region, many other studies from other regions of Brazil were also included.
Although a greater number of studies in this review have focused their attention on the CHEK2 and ATM gene, the second most mutated non-BRCA gene, curiously, was MUTYH. Ten different pathogenic variants were found in the MUTYH gene with a total of 34 mutated patients (Additional file 1), distributed in three studies [24, 38, 44]. In highlight, the c.1187G > A variant was reported in fifteen patients with HBOC in Brazil, including 13 patients from the cohort of Guindalini et al. [44], been this variant responsible for a significant proportion of pathogenic mutations in the MUTYH gene.
The third gene with the highest number of pathogenic variants reported in Brazil was ATM. Twenty-three pathogenic variants were reported in 32 HBOC patients (Additional file 1). Among nine studies using NGS technology, six found pathogenic mutations in the ATM gene, distributed in different regions of the country [12, 23, 36,37,38, 44]. Next comes the PALB2 gene with 14 patients identified as carriers of the pathogenic mutation (Additional file 1).
Both the ATM, PALB2 and CHEK2 genes are breast cancer susceptibility genes of moderate penetrance. The CHEK2 gene was tracked by NGS panel studies, and the most reported 1100delC mutation was also tracked punctually by five different studies [63]. However, of the 14 studies that included the CHEK2 gene for screening in this review, only three were identified the c.1100delC variant [16, 18, 44]. This mutation has been described in less heterogeneous populations, as in studies conducted in the Netherlands that described the increased risk of breast cancer observed in patients with CHEK2 1100delC and another study that reported 4% of their tested patients carrying this pathogenic variant [64, 65]. Studies show that carriers with a family history of breast cancer are at 2–3 times greater risk when breast cancer is associated with the CHEK2 c.1100delC mutation [66]. In Brazil, studies tracking mutations in moderate- or low-penetrance genes for breast cancer are still rare, but this number should increase in the next year with the advent of NGS technology.
Limitations
Data analysis was challenging, and the review had some limitations, one of which was the scarcity of data from two regions of Brazil (the Midwest and the North). Although these are the least populous regions, their inclusion would give an interesting global view of the mutation profile. It was not possible to obtain information about the place of birth of the patients included in the studies. Therefore, data on geographic location should be interpreted with caution. In addition, some studies may not have been very representative of the region studied due to the sample size or study objective. Some works focused on tracking specific mutations or specific regions of the selected gene. The works are heterogeneous in their aim, which leads to an asymmetrical presentation of the results, leaving out some important data, such as VUS. The classification and final interpretation of the detected variants is also a limitation of this study, considering that many variants of uncertain meaning described mainly in older studies may currently lead to another classification based on the recommendations of the American College of Genetics and Medical Genomics (ACMG). It is important to highlight that this review did not aim to reclassify the variants in each study.
Conclusion
The identification of germline mutations is a crucial factor in the continuation and updating of clinical management protocols. Despite significant molecular heterogeneity among mutations in HBOC patients from Brazil, three mutations deserve to be highlighted: c.5266dupC, c.156_157insAlu and c.1010G > A in the BRCA1, BRCA2 and TP53 genes, respectively. With more than 200 records, these mutations play a key role in the pathology of breast cancer in Brazil. In addition, it was seen that MUTYH, ATM, PALB2 and CHEK2 genes also contributed significantly to the increased risk in HBOC patients. However, the accumulated knowledge about mutation profiles in HBOC susceptibility genes do not cover all Brazilian subpopulations, especially those from the Amazon in the north of the country. The multigene panels contributed to a greater identification of pathogenic mutations in non-BRCA1/2 genes, but the number of studies is not yet sufficient to show the full spectrum of mutations in the country.
Data Availability
All data from this research are already available in the suplemmentary material.
Abbreviations
- ACMG:
-
American College of Genetics and Medical Genomics
- AS-PCR:
-
Allele-specific PCR
- BC:
-
Breast cancer
- DGGE:
-
Denaturing gradient gel electrophoresis
- DHPLC:
-
Denaturing high performance liquid chromatography
- gnomAD:
-
Genome Aggregation Database
- HBCC:
-
Breast and colorectal cancer syndrome
- HBOC:
-
Hereditary breast and ovarian cancer syndrome
- HRM:
-
High resolution melting
- IBGE:
-
Brazilian Institute of Geography and Statistics
- LFL:
-
Li-Fraumeni Syndrome
- MLPA:
-
Multiplex ligation-dependent probe amplification
- NGS:
-
Next-generation sequencing
- PPT:
-
Protein Truncation Test
- qPCR:
-
Real-time PCR
- RFLP:
-
Restriction fragment length polymorphism
- SSCP:
-
Single-Stranded conformation polymorphism
- VUS:
-
Variants of unknown significance
- WES:
-
Whole exome sequencing
References
Yoshida R. Hereditary breast and ovarian cancer (HBOC): review of its molecular characteristics, screening, treatment, and prognosis. Breast Cancer. 2021;28(6):1167–80.
Petrucelli N, Daly MB, Pal T. BRCA1- and BRCA2-Associated Hereditary Breast and Ovarian Cancer. In: Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Gripp KW, editors. GeneReviews. Seattle: University of Washington; 1998.
Nielsen FC, van Overeem HT, Sørensen CS. Hereditary breast and ovarian cancer: new genes in confined pathways. Nat Rev Cancer. 2016;16(9):599–612.
Instituto Nacional de Câncer José Alencar Gomes da Silva. Estimativa 2023 incidência do Câncer no Brasil. Rio de Janeiro: INCA; 2022. p. 2022.
Weitzel JN, Clague J, Martir-Negron A, Ogaz R, Herzog J, Ricker C, et al. Prevalence and type of BRCA mutations in Hispanics undergoing genetic cancer risk assessment in the southwestern United States: a report from the clinical cancer genetics community research network. J Clin Oncol. 2013;31(2):210–6.
Palmero EI, Ashton-Prolla P, Rocha JC, Vargas FR, Kalakun L, Blom MB, et al. Clinical characterization and risk profile of individuals seeking genetic counseling for hereditary breast cancer in Brazil. J Genet Couns. 2007;16(3):363–71.
Carvalho SCS, Cury NM, Brotto DB, Araujo LF, Rosa RCA, Texeira LA, et al. Germline variants in DNA repair genes associated with hereditary breast and ovarian cancer syndrome: analysis of a 21 gene panel in the Brazilian population. BMC Med Genomics. 2020;13:21.
Acosta AX, Abé-Sandes K, Giugliani R, Bittles AH. Delivering genetic education and genetic counseling for rare diseases in rural Brazil. J Genet Couns. 2013;22(6):830–4.
Palmero EI, Carraro DM, Alemar B, Moreira MAM, Ribeiro-Dos-Santos Â, Abe-Sandes K, et al. The germline mutational landscape of BRCA1 and BRCA2 in Brazil. Sci Rep. 2018;8:9188.
Santos NP, Ribeiro-Rodrigues EM, Ribeiro-Dos-Santos AK, Pereira R, Gusmão L, Amorim A, et al. Assessing individual interethnic admixture and population substructure using a 48-insertion-deletion (INSEL) ancestry-informative marker (AIM) panel. Hum Mutat. 2010;31(2):184–90.
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160.
Timoteo ARS, Gonçalves AÉMM, Sales LAP, Albuquerque BM, Souza JES, Moura PCP, et al. A portrait of germline mutation in Brazilian at-risk for hereditary breast cancer. Breast Cancer Res Treat. 2018;172(3):637–46.
Felix GE, Abe-Sandes C, Machado-Lopes TM, Bomfim TF, Guindalini RS, Santos VC, et al. Germline mutations in BRCA1, BRCA2, CHEK2 and TP53 in patients at high-risk for HBOC: characterizing a Northeast Brazilian Population. Hum Genome Var. 2014;1:14012.
Alemar B, Gregório C, Herzog J, Matzenbacher Bittar C, Brinckmann ONC, Artigalas O, et al. BRCA1 and BRCA2 mutational profile and prevalence in hereditary breast and ovarian cancer (HBOC) probands from Southern Brazil: are international testing criteria appropriate for this specific population? PLoS ONE. 2017;12(11): e0187630.
Alemar B, Herzog J, Brinckmann ONC, Artigalás O, Schwartz IVD, Matzenbacher Bittar C, et al. Prevalence of Hispanic BRCA1 and BRCA2 mutations among hereditary breast and ovarian cancer patients from Brazil reveals differences among Latin American populations. Cancer Genet. 2016;209(9):417–22.
Palmero EI, Alemar B, Schüler-Faccini L, Hainaut P, Moreira-Filho CA, Ewald IP, et al. Screening for germline BRCA1, BRCA2, TP53 and CHEK2 mutations in families at-risk for hereditary breast cancer identified in a population-based study from Southern Brazil. Genet Mol Biol. 2016;39(2):210–22.
Buzolin AL, Moreira CM, Sacramento PR, Oku AY, Fornari ARS, Antonio DSM, et al. Development and validation of a variant detection workflow for BRCA1 and BRCA2 genes and its clinical application based on the Ion Torrent technology. Hum Genomics. 2017;11:14.
Silva FC, Lisboa BC, Figueiredo MC, Torrezan GT, Santos EM, Krepischi AC, et al. Hereditary breast and ovarian cancer: assessment of point mutations and copy number variations in Brazilian patients. BMC Med Genet. 2014;15:55.
Fernandes GC, Michelli RA, Galvão HC, Paula AE, Pereira R, Andrade CE, et al. Prevalence of BRCA1/BRCA2 mutations in a Brazilian population sample at-risk for hereditary breast cancer and characterization of its genetic ancestry. Oncotarget. 2016;7(49):80465–81.
Brianese RC, Nakamura KDM, Almeida FGDSR, Ramalho RF, Barros BDF, Ferreira ENE, et al. BRCA1 deficiency is a recurrent event in early-onset triple-negative breast cancer: a comprehensive analysis of germline mutations and somatic promoter methylation. Breast Cancer Res Treat. 2018;167(3):803–14.
Cury NM, Ferraz VE, Silva WA Jr. TP53 p.R337H prevalence in a series of Brazilian hereditary breast cancer families. Hered Cancer Clin Pract. 2014;12:8.
Felicio PS, Grasel RS, Campacci N, Paula AE, Galvão HCR, Torrezan GT, et al. Whole-exome sequencing of non-BRCA1/BRCA2 mutation carrier cases at high-risk for hereditary breast/ovarian cancer. Hum Mutat. 2021;42(3):290–9.
Bandeira G, Rocha K, Lazar M, Ezquina S, Yamamoto G, Varela M, et al. Germline variants of Brazilian women with breast cancer and detection of a novel pathogenic ATM deletion in early-onset breast cancer. Breast Cancer. 2020;28(2):346–54.
Grasel RS, Felicio PS, Paula AE, Campacci N, Garcia FAO, Andrade ES, et al. Using co-segregation and loss of heterozygosity analysis to define the pathogenicity of unclassified variants in hereditary breast cancer patients. Front Oncol. 2020;10:571330.
Maistro S, Teixeira N, Encinas G, Katayama ML, Niewiadonski VD, Cabral LG, et al. Germline mutations in BRCA1 and BRCA2 in epithelial ovarian cancer patients in Brazil. BMC Cancer. 2016;16:934.
Dufloth RM, Carvalho S, Heinrich JK, Shinzato JY, Santos CC, Zeferino LC, et al. Analysis of BRCA1 and BRCA2 mutations in Brazilian breast cancer patients with positive family history. Sao Paulo Med J. 2005;123(4):192–7.
Carraro DM, Folgueira MAK, Lisboa BCG, Olivieri EHR, Krepischi ACV, Carvalho AF, et al. Comprehensive analysis of BRCA1, BRCA2 and TP53 germline mutation and tumor characterization: a portrait of early-onset breast cancer in Brazil. PLoS ONE. 2013;8(3): e57581.
Nagy TR, Maistro S, Encinas G, Katayama MLH, Pereira GFL, Gaburo-Júnior N, et al. Germline and somatic mutations in postmenopausal breast cancer patients. Clinics. 2021;16(76): e2837.
Encinas G, Sabelnykova VY, de Lyra EC, Hirata Katayama ML, Maistro S, de Vasconcellos Valle PWM, et al. Somatic mutations in early onset luminal breast cancer. Oncotarget. 2018;9(32):22460–79.
Schayek H, De Marco L, Starinsky-Elbaz S, Rossette M, Laitman Y, Bastos-Rodrigues L, et al. The rate of recurrent BRCA1, BRCA2, and TP53 mutations in the general population, and unselected ovarian cancer cases, in Belo Horizonte Brazil. Cancer Genet. 2015;209(1–2):50–2.
Cipriano NM Jr, Brito AM, Oliveira ES, Faria FC, Lemos S, Rodrigues AN, et al. Mutation screening of TP53, CHEK2 and BRCA genes in patients at high risk for hereditary breast and ovarian cancer (HBOC) in Brazil. Breast Cancer. 2018;26(3):397–405.
Oliveira ES, Soares BL, Lemos S, Rosa RC, Rodrigues AN, Barbosa LA, et al. Screening of the BRCA1 gene in Brazilian patients with breast and/or ovarian cancer via high-resolution melting reaction analysis. Fam Cancer. 2015;15(2):173–81.
Moreira MA, Bobrovnitchaia IG, Lima MA, Santos AC, Ramos JP, Souza KR, et al. Portuguese c.156_157insAlu BRCA2 founder mutation: gastrointestinal and tongue neoplasias may be part of the phenotype. Fam Cancer. 2012;11(4):657–60.
Lourenço JJ, Vargas FR, Bines J, Santos EM, Lasmar CAP, Costa CH, et al. BRCA1 mutations in Brazilian patients. Genet Mol Biol. 2004;27(4):500–4.
Gomes MC, Costa MM, Borojevic R, Monteiro AN, Vieira R, Koifman S, et al. Prevalence of BRCA1 and BRCA2 mutations in breast cancer patients from Brazil. Breast Cancer Res Treat. 2007;103(3):349–53.
Gomes R, Soares BL, Felicio PS, Michelli R, Netto CBO, Alemar B, et al. Haplotypic characterization of BRCA1 c.5266dupC, the prevailing mutation in Brazilian hereditary breast/ovarian cancer. Genet Mol Biol. 2020;43(2): e20190072.
Matta BP, Gomes R, Mattos D, Olicio R, Nascimento CM, Ferreira GM, et al. Familial history and prevalence of BRCA1, BRCA2 and TP53 pathogenic variants in HBOC Brazilian patients from a public healthcare service. Sci Rep. 2022;12:18629.
Sandoval RL, Leite ACR, Barbalho DM, Assad DX, Barroso R, Polidorio N, et al. Germline molecular data in hereditary breast cancer in Brazil: lessons from a large single-center analysis. PLoS ONE. 2021;16(2): e0247363.
Silva PFF, Goveia RM, Teixeira TB, Gamba BF, Lima AP, Rogatto SR, et al. TP53 pathogenic variants in early-onset breast cancer patients fulfilling hereditary breast and ovary cancer and Li-Fraumeni-like syndromes. Biomolecules. 2022;12(5):640.
Ewald IP, Cossio SL, Palmero EI, Pinheiro M, Nascimento IL, Machado TM, et al. BRCA1 and BRCA2 rearrangements in Brazilian individuals with hereditary breast and ovarian cancer syndrome. Genet Mol Biol. 2016;39(2):223–31.
Ewald IP, Izetti P, Vargas FR, Moreira MA, Moreira AS, Moreira-Filho CA, et al. Prevalence of the BRCA1 founder mutation c.5266dupin Brazilian individuals at-risk for the hereditary breast and ovarian cancer syndrome. Hered Cancer Clin Pract. 2011;9:12.
Felicio PS, Alemar B, Coelho AS, Berardinelli GN, Melendez ME, Lengert AVH, et al. Screening and characterization of BRCA2 c.156_157insAlu in Brazil: results from 1380 individuals from the South and Southeast. Cancer Genet. 2018;228–9:93–7.
Esteves VF, Thuler LCS, Amêndola LC, Koifman RJ, Koifman S, Frankel PP, et al. Prevalence of BRCA1 and BRCA2 gene mutations in families with medium and high risk of breast and ovarian cancer in Brazil. Braz J Med Biol Res. 2009;42(5):453–7.
Guindalini RSC, Viana DV, Kitajima JPFW, Rocha VM, López RVM, Zheng Y, et al. Detection of germline variants in Brazilian breast cancer patients using multigene panel testing. Sci Rep. 2022;12:4190.
Mazzonetto P, Milanezi F, D’Andrea M, Martins S, Monfredini PM, Dos Santos SJ, et al. BRCA1 and BRCA2 germline mutation analysis from a cohort of 1267 patients at high risk for breast cancer in Brazil. Breast Cancer Res Treat. 2023;199(1):127–36.
Instituto Brasileiro de Geografia e Estatística. Síntese de indicadores sociais: uma análise das condições de vida da população brasileira 2020. Rio de Janeiro: IBGE; 2020.
Instituto Brasileiro de Geografia e Estatística. Censo Brasileiro de 2022. Rio de Janeiro: IBGE; 2022.
Instituto Nacional de Câncer José Alencar Gomes da Silva. A situação do câncer de mama no Brasil: síntese de dados dos sistemas de informação. Rio de Janeiro: INCA; 2019.
Dobbin EAF, Medeiros JAG, Costa MSCR, Rodrigues JCG, Guerreiro JF, Kroll JE, et al. Identification of variants (rs11571707, rs144848, and rs11571769) in the BRCA2 gene associated with hereditary breast cancer in indigenous populations of the Brazilian Amazon. Genes. 2021;12(2):142.
Abeliovich D, Kaduri L, Lerer I, Weinberg N, Amir G, Sagi M, et al. The founder mutations 185delAG and 5382insC in BRCA1 and 6174delT in BRCA2 appear in 60% of ovarian cancer and 30% of early-onset breast cancer patients among Ashkenazi women. Am J Hum Genet. 1997;60(3):505–14.
Janavičius R. Founder BRCA1/2 mutations in the Europe: implications for hereditary breast-ovarian cancer prevention and control. EPMA J. 2010;1(3):397–412.
Durocher F, Tonin P, Shattuck-Eidens D, Skolnick M, Narod SA, Simard J. Mutation analysis of the BRCA1 gene in 23 families with cases of cancer of the breast, ovary, and multiple other sites. J Med Genet. 1996;33(10):814–9.
Tuazon AMA, Lott P, Bohórquez M, Benavides J, Ramirez C, Criollo A, et al. Haplotype analysis of the internationally distributed BRCA1 c.3331_3334delCAAG founder mutation reveals a common ancestral origin in Iberia. Breast Cancer Res. 2020;22:108.
Vega A, Campos B, Bressac-De-Paillerets B, Bond PM, Janin N, Douglas FS, et al. The R71G BRCA1 is a founder Spanish mutation and leads to aberrant splicing of the transcript. Hum Mutat. 2001;17(6):520–6.
Machado PM, Brandão RD, Cavaco BM, Eugénio J, Bento S, Nave M, et al. Screening for a BRCA2 rearrangement in high-risk breast/ovarian cancer families: evidence for a founder effect and analysis of the associated phenotypes. J Clin Oncol. 2007;25(15):2027–34.
Neuhausen SL, Godwin AK, Gershoni-Baruch R, Schubert E, Garber J, Stoppa-Lyonnet D, et al. Haplotype and phenotype analysis of nine recurrent BRCA2 mutations in 111 families: results of an international study. Am J Hum Genet. 1998;62(6):1381–8.
Heramb C, Wangensteen T, Grindedal EM, Ariansen SL, Lothe S, Heimdal KR, et al. BRCA1 and BRCA2 mutation spectrum—an update on mutation distribution in a large cancer genetics clinic in Norway. Hered Cancer Clin Pract. 2018;16:3.
Gayther SA, Mangion J, Russell P, Seal S, Barfoot R, Ponder BA, et al. Variation of risks of breast and ovarian cancer associated with different germline mutations of the BRCA2 gene. Nat Genet. 1997;15(1):103–5.
Santos C, Peixoto A, Rocha P, Pinto P, Bizarro S, Pinheiro M, et al. Pathogenicity evaluation of BRCA1 and BRCA2 unclassified variants identified in Portuguese breast/ovarian cancer families. J Mol Diagn. 2014;16(3):324–34.
Palmero EI, Schüler-Faccini L, Caleffi M, Achatz MI, Olivier M, Martel-Planche G, et al. Detection of R337H, a germline TP53 mutation predisposing to multiple cancers, in asymptomatic women participating in a breast cancer screening program in Southern Brazil. Cancer Lett. 2008;261(1):21–5.
Assumpção JG, Seidinger AL, Mastellaro MJ, Ribeiro RC, Zambetti GP, Ganti R, et al. Association of the germline TP53 R337H mutation with breast cancer in southern Brazil. BMC Cancer. 2008;8:357.
Giacomazzi J, Graudenz MS, Osorio CA, Koehler-Santos P, Palmero EI, Zagonel-Oliveira M, et al. Prevalence of the TP53 p.R337H mutation in breast cancer patients in Brazil. PLoS ONE. 2014;9(6): e99893.
CHEK2 Breast Cancer Case-Control Consortium. CHEK2*1100delC and susceptibility to breast cancer: a collaborative analysis involving 10,860 breast cancer cases and 9,065 controls from 10 studies. Am J Hum Genet. 2004;74(6):1175–82.
Adank MA, Verhoef S, Oldenburg RA, Schmidt MK, Hooning MJ, Martens JW, et al. Excess breast cancer risk in first degree relatives of CHEK2∗1100delC positive familial breast cancer cases. Eur J Cancer. 2013;49(8):1993–9.
Velthuizen ME, van der Luijt RB, de Vries BJ, Koudijs MJ, Bleiker EMA, Ausems MGEM. Recontacting non-BRCA1/2 breast cancer patients for germline CHEK2 c.1100del pathogenic variant testing: uptake and patient experiences. Hered Cancer Clin Pract. 2021;19:9.
Wendt C, Muranen TA, Mielikäinen L, Thutkawkorapin J, Blomqvist C, Jiao X, et al. A search for modifying genetic factors in CHEK2:c.1100delC breast cancer patients. Sci Rep. 2021;11:14763.
Acknowledgements
Not applicable.
Funding
This work was supported by the Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG; Grant Number, RED-00314-16 and RED-00089-23), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) and Universidade Federal de São João del Rei (UFSJ).
Author information
Authors and Affiliations
Contributions
All authors contributed equally to this work offering (1) substantial contributions to conception and design, data collection, or analysis and interpretation of data; (2) article writing or relevant critical review of the intellectual content, and (3) final approval of the version to be published.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
As this manuscript is a literature review, informed consent is not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Shows all pathogenic mutations identified in the reviewed articles and the estimated frequencies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
de Freitas Ribeiro, A.A., Junior, N.M.C. & dos Santos, L.L. Systematic review of the molecular basis of hereditary breast and ovarian cancer syndrome in Brazil: the current scenario. Eur J Med Res 29, 187 (2024). https://doi.org/10.1186/s40001-024-01767-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-024-01767-x