
Abstract
Background
In traditional laparoscopic hysterectomy, an assistant is typically assigned to hold a uterus manipulator to facilitate the surgical procedures. The responsibility of the assistant is to position the uterus according to the primary surgeon’s instructions. Throughout the surgery, which typically lasts more than 90 min, the assistant has to support the uterus manipulator with his/her hands, which easily causes fatigue to the assistant and eventually affects the manipulation performance and threatens the patient. Moreover, the manipulation done by the assistant may not always be satisfactory from the primary surgeon’s point of view. Thus, having a robot assistant which can release the human assistant’s hands from the manipulation task and allow the primary surgeon to directly position the patient’s uterus can be a solution.
Methods
A four degrees of freedom (DOF) robot assistant is designed for positioning the patient’s uterus during hysterectomy. The robot assistant is composed of three parts, a 3-DOF robotic positioning arm, a 1-DOF motorized uterus manipulator, and a supporting stand of the robot. To improve safety, the remote center of motion (RCM) mechanism is applied to the design of the robotic positioning arm. The positioning arm generates a partial spherical workspace and allows the manipulation of uterus to be done in a decoupled manner. To enhance the ability of the robot assistant to perform anteversion and retroversion motions, the motorized uterus manipulator is designed. The robot assistant is mounted to the operating table through the supporting stand.
Results
A prototype of the robot assistant is built, and experiments are conducted to verify the performance of the prototype. It is shown that the prototype is able to respond to the user’s instructions accordingly and manipulates the uterus of a manikin to a desired position. Performances of robot manipulation and human manipulation are also compared. It is shown that the robot assistant can retain the manikin’s uterus in a specified position in a more stable manner.
Conclusions
Our experimental study shows that the use of a robot is a feasible alternative to position the uterus. By using this type of system, costs can be reduced and safety can be improved.
Similar content being viewed by others


Background
Excluding the pregnancy-related procedures, hysterectomy is the most commonly performed gynecological procedure [1]. Since the 1990s, there has been an increasing trend in the number of hysterectomy procedures performed in laparoscopic approach [2]. In the 2000s, with the introduction of the daVinci surgical system, surgeons started performing robot-assisted hysterectomy [1],[3],[4]. During a robot-assisted laparoscopic hysterectomy, the primary surgeon controls the robotic arms located at the patient’s bedside from the surgeon’s console, which is located away from the patient’s bed; the assistant surgeon at the patient’s bedside assists the primary surgeon in operating the uterus manipulator and using the accessory port of the daVinci system [3].
In [3], it is reported that the typical operative time for this kind of robot-assisted laparoscopic hysterectomy lasts no less than 190 min; in [1], it is reported that out of 16 cases, the median of the operative time is 242 min. However, for traditional laparoscopic hysterectomy conducted in the 2000s, it is reported that the median operative time is in general not more than 135 min [5]. By comparison, it is observed that the operative time required to perform traditional laparoscopic hysterectomy (i.e., performed by the primary surgeon directly at the patient’s bedside) is in general shorter than those performed robotically with the daVinci system.
In terms of effectiveness, it is worth keeping the primary surgeon at the operating table to perform surgery. Besides, during this kind of robot-assisted surgery, operating the uterus manipulator is still the responsibility of the assistant surgeon. No matter in traditional or robot-assisted laparoscopic hysterectomy, asking an assistant surgeon to operate the uterus manipulator causes the problem that the manipulated position may not satisfy the primary surgeon’s need. Furthermore, if no supporting device is used to assist the assistant surgeon in holding the uterus manipulator, the assistant surgeon would suffer from the problem of fatigue as he/she is required to hold the uterus manipulator throughout the surgery. Fatigue may decrease the performance of the assistant surgeon and may eventually threaten the patient. Thus, a robotic system which is capable of assisting in this tool manipulation while keeping the primary surgeon at the operating table side during hysterectomy is necessary; this is precisely our aim in this article.
Existing surgical robots
Robots have been introduced to the operating theater in recent decades; the daVinci surgical system is a well-known example. The daVinci system is a multipurpose surgical robotic system designed for laparoscopic surgeries. Four robotic arms are included in the system for manipulating a laparoscope and other surgical tools during surgery. Though tele-surgery is allowed with the daVinci system, the primary surgeon who operates the robot is away distant from the patient’s bedside [6] due to its large footprint. Furthermore, as the robotic arms are designed for laparoscopic surgeries, the robotic arms are generally setup to operate above the patient’s abdomen; thus, when performing laparoscopic hysterectomy, an assistant is still required to position the patient’s uterus from the end of the operating table.
In general, surgical robots for minimally invasive surgery are mainly designed for endoscope manipulation or surgical tool manipulation during laparoscopic surgery in which several small incisions are opened on the patient’s abdomen and the endoscope and the surgical tools are inserted into the patient’s body through these incisions. Examples of robotic endoscope manipulators include AESOP [7], LARS [8], EndoAssist [9], and FreeHand [10].
EndoControl, the manufacturer of ViKY [11], a robot designed for endoscope or surgical tools manipulation, developed a system named ViKY UP [12] which aims at hysterectomy procedures. ViKY UP is a motorized uterus positioner which helps to manipulate the uterus manipulator during surgery. Though ViKY UP serves the aim of taking up the task of the assistant who is responsible for manipulating the uterus manipulator, the mechanism of the robot generates a cone-shaped workspace [13]. With this configuration, joint motions are coupled when the surgeon would like to manipulate the patient’s uterus laterally or vertically.
Contributions
In this article, we present a robotic prototype for uterus positioning during laparoscopic hysterectomy. Different from the majority surgical robots, the remote center of motion of our prototype is designed to be placed at the cervix (i.e., inside the patient’s body), which is more preferable in hysterectomy. With the use of the robot, safety can be improved as the robot can hold the uterus manipulator more stable than a human in general. Furthermore, a valuable manpower can be released with the use of the robot; thus, surgical costs can be reduced.
Methods
Design requirements
The robotic system presented in this article is aimed at providing assistance in positioning the uterus manipulator during laparoscopic hysterectomy. To achieve this, the proposed robotic system should have the following abilities:
-
1.
The robot should be able to grasp and hold the uterus manipulator securely.
-
2.
The robot should have the ability to manipulate the uterus manipulator in a natural manner as an assistant surgeon does.
-
3.
The robot should be able to receive commands from the primary surgeon and response correspondingly.
In traditional laparoscopic hysterectomy, the assistant surgeon who is responsible for operating the uterus manipulator generally manipulates the patient’s uterus according to the primary surgeon’s order in three ways:
-
1.
Anteversion/retroversion of uterus,
-
2.
Laterally manipulation of uterus, and
-
3.
Tensioning of uterus.
Design of the robot
The robotic system presented in this article is comprised of three parts, a robotic positioning arm, a motorized uterus manipulator, and a supporting stand of the robot.
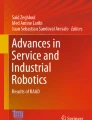
Schematic of the robotic uterus manipulator positioning arm is shown in Figure 1. In the schematic diagram, the motorized uterus manipulator is used as the surgical tool manipulated by the positioning arm. The positioning arm has three degrees of freedom, yaw, pitch, and insertion. As in medical robotics, safety is the most important issue, a remote center of motion (RCM) mechanism [14] is used in the robotic positioning arm to improve safety. With the RCM mechanism, a point which is to be placed at or close to the patient’s cervix will be mechanically forced to remain stationary no matter how the arm moves. To create the remote center of motion, the three actuated joints are designed to satisfy specific geometric arrangement. Here, denote the joint for yaw motion by joint 1, the joint for pitch motion by joint 2, and the joint for insertion by joint 3. The geometric arrangement of the joints is as follow:
Joint 1 is a revolute joint.

Schematic diagram of the design
Joint 2 is a sliding joint which moves along a circular trajectory. The axis of rotation of joint 1 intersects with the center of the circular trajectory of joint 2. This intersection point gives the remote center of motion.
Joint 3 is a translational joint. The axis of translation of joint 3 intersects with the axis of rotation of joint 1 and the center of the circular trajectory of joint 2. The surgical tool considered as a straight rod lies on the axis of translation of joint 3 and intersects with the RCM.
The motorized uterus manipulator is a device which enhances the ability of the robot assistant in performing anteversion and retroversion motions. It is a device with a tilting tip which has a moving direction similar to joint 2. Here, we denote this joint by joint 4.
Based on the schematic, a prototype of the robot assistant is designed and developed. Figure 2 shows the computer-aided design (CAD) model of the design and the CAD model of the robot assistant when it is used in the operating theater.

CAD model of the robot assistant (left) and when it is use (right)
Actuation and mechanisms
To realize the motion of joint 2, pinion and rack mechanism is used. A block with a spur gear installed to the actuator is allowed to run along an arc-shaped guide rail with gear teeth on the rail as shown. A 20 W DC motor with gearbox is used as the actuator to ensure enough power can be delivered to drive the system. Using a motor with larger power than what it actually needs may also prevent the motor from damage due to overloading.
The structure of joint 2 is mounted on top of joint 1 directly, that is, joint 1 drives the entire structure including the arc-shaped guide rail of joint 2. Joint 1 is a revolute joint; the rotation motion from the actuator drives the structures mounted to it directly. A 20 W DC motor with gearbox is also used as the actuator for joint 1.
Joint 3 is mounted to the actuated block of joint 2. To realize the inserting motion, ball-screw mechanism is used. A 2 W DC motor with gearbox is used as the actuator as the ball-screw mechanism provides large reduction ratio, and the power required to drive the system is greatly reduced. An adaptor for grasping the surgical tool is attached to this joint. The adaptor is designed to hold uterus manipulators with a diameter of 8 or 12 mm.
Joint 4 is a joint of the motorized uterus manipulator which enables tilting motion. The motorized uterus manipulator is composed of two parts, a disposable unit and a reusable driving unit. The two units are connected together through a lock as shown in Figure 3. In this joint, a pair of bevel gears is used to convert the actuation direction of the tip to a configuration which can be driven by the actuator installed in the reusable driving unit. To drive the tip, a 6 W DC motor with gearbox is used as the actuator. All motors used for building this prototype are from Maxon.

Structure of the motorized uterus manipulator
Control system architecture
A schematic representation of the control system architecture is shown in Figure 4, which is composed of a user interface, a control system, and the robot actuators. The user interface consists of a standard joystick device, which allows the user to directly control the motion of the robot. The control system is the one in charge to regulate and drive the DC motors of the robot; it is composed of a Linux-based PC, an industrial motion controller, and the power amplifiers. We use a Galil DMC-4040 (DMC-4040, Galil Motion Control, Rocklin, CA, USA) industrial motion controller with an embedded four-axis 20 W current amplifier. The motion controller has implemented a speed tracking servo loop for each of the joints.

Control system architecture of the robot assistant
The prototype
A prototype of the robot assistant is developed according to the design shown in Figure 2; the metal parts were fabricated using standard aluminum alloy and stainless steel. The moving ranges of joint 1 to joint 4 are −65° to 65°, 30° to 138°, 0 to 50 mm, and 0° to 180°, respectively. Motions of individual joints of the robot assistant are shown in Figure 5. Figure 6 shows the manipulation experiments conducted with manikin.

Joint motions of the robot assistant

Manipulating the uterus of a manikin with the robot
Results and discussion
To verify the performance of the prototype, four experiments are conducted. Two experiments are conducted to verify the closed-loop response of the robot’s motion, and two are conducted to compare the manipulation performance of the robotic assistant with of a human assistant.
Velocity tracking experiment (auto-feed)
The objective of this experiment is to verify the performance of the robot in responding to an assigned velocity profile. In particular, we would like to verify the robot’s performance when moving with non-constant speeds. In this experiment, the four degrees of freedom of the robot are tested separately. To each joint, a time-varying velocity profile (a sinusoidal function of time) is assigned, which the robot must follow as accurately as possible. We denote the i th velocity input to the robot by
where v i represents the joint velocity and k i is a positive user-definable velocity gain.
The results of this velocity tracking experiment are shown in Figure 7. In the figure, the desired velocity profiles fed to the robot are represented by the black lines while the measured velocities of the joints are represented by the red lines. These experiments are obtained with the following velocity gains: k1=13, k2=27, k3=1.7, and k4=50. From these results, it is shown that the robot can closely track the time-varying velocity inputs.

Results of the velocity tracking experiment (auto-feed)
Velocity tracking experiment (manual input from joystick)
As the robot is designed to be controlled and operated by the primary surgeon, this experiment is conducted in a manual-control mode. The objective of this experiment is similar to the auto-feed one, i.e., to verify the performance of the robot in responding to the user’s input commands.
In this experiment, the robot is manually controlled by human through a joystick interface. For these experiments, we denote the i th velocity input to the robot by
where J i represents a discrete (i.e. −1,1,0) input provided by the joystick interface. The user is asked to control the robot by pressing the buttons on the control joystick which correspond to the robot joints and their moving directions.
Similar to the auto-feed experiment, the joints of the robot are tested separately in this experiment. Figures 8 and 9 show the results of this experiment; Figure 8 shows the steady state response of the system while Figure 9 shows the transient responses. In the figures, the black lines indicate the input velocity profiles converted from the input commands from the joystick while the red lines indicate the measured joint velocities. These experiments are obtained with the following velocity gains: k1=20, k2=50, k3=3.5, and k4=60. From the results, it is shown that the robot can accurately regulate a constant speed profile provided by the user.

Results of the velocity tracking experiment (manual control)

Transient responses of the joints in manual control mode
Manipulation experiment (one-dimensional distance)
In traditional laparoscopic hysterectomy, visual feedback is obtained from the laparoscopic camera inserted into the patient’s body through a small incision opened on the patient’s abdomen. In general, 2D visual feedback can be obtained and the surgery is performed with the use of this 2D visual information. This scenario is emulated in this experiment, and the experimental setup is shown in Figure 10. The objective of this experiment is to compare the manipulation performance of the robot with that of human.

Experimental setup of the manipulation experiments
In this experiment, a medical manikin is used as the simulated environment. To emulate the laparoscopic camera, a webcam is used to obtain the visual feedback from the manikin. With the webcam, images with resolution of 640 × 480 pixel are obtained. An artificial marker is attached to the uterus as a visual feedback tracking point. In this experiment, a standard non-motorized uterus manipulator (produced by Apple Med [15]) is used as the surgical tool to position the uterus of the manikin.
On the robot side, the uterus manipulator is grasped by the robotic positioning arm. Human participants are asked to move the marker to a desired image configuration with the assistance of the robot and retain that position. The robot is controlled by the participants using a joystick.
To compare the performance of the robot with the performance of a human, the same experiment is conducted without the assistance of the robot. The human participants are asked to hold the uterus manipulator by themselves and keep a specified image position without the use of any supporting device. All participants involved in this experiment are without medical background. Short training for both manipulating with and without the robot is given to the participants before the experiment started.
In this experiment, the desired image position is represented by a one-dimensional line as shown in Figure 11. The participants are asked to align the marker attached to the uterus of the manikin to any point of the line specified on the screen both with and without the use of the robot. We choose this task as it is a common procedure to move the uterus aside during laparoscopic hysterectomy.

The desired position in the 1D (left) and 2D (right) image space
Pixel error between the marker and the line is measured. As the image position of the desired destination is known and the image position of the marker attached to the manikin can be obtained by feature tracking, the pixel error can be calculated by
where e is the pixel error, p d is the pixel position of the desired destination, and p m is the pixel position of the marker. In this one-dimensional experiment, p d and p m can be understood as the x-coordinates of the desired destination and the marker on the image plane, respectively.
In both assisted and unassisted experiments, ten trials are conducted. The results are shown in Figure 12.

One-dimensional pixel error when manipulated with the robot (left) and without using the robot (right)
In Figure 12, the plot on the left shows the measured pixel error obtained the during manipulation with the assistance of the robot; the plot on the right shows the measured pixel error obtained without the use of the robot assistant. From these results, it is shown that with the use of the robot, the participants are able to manipulate the uterus to a specified image position in a more stable way compared to the traditional hand manipulation.
Manipulation experiment (two-dimensional point control)
To further verify the performance of the robot, the manipulation experiment is extended to the two-dimensional image space. In this experiment, the desired position is specified by an image point instead of a line, as shown in Figure 11. The pixel errors in both x and y directions on the image plane are measured to evaluate the performances.
Figures 13 and 14 compare the positioning performance of the robot with that of solely human manipulation. These results show that while both human and robot are able to manipulate the uterus to a desired position, the robot can retain the desired configuration in a more stable manner, as expected.

Pixel error comparison in the x -axis

Pixel error comparison in the y -axis
Conclusions
In this article, a four degrees of freedom robot assistant for uterus positioning during laparoscopic hysterectomy is designed and developed. This system is composed of a 3-degrees of freedom (DOF) uterus manipulator positioning arm, a 1-DOF motorized uterus manipulator, and a supporting stand which mounts the robot to the operating table. The 3-DOF uterus manipulator positioning arm adopts the RCM mechanism, which is designed to improve safety. Instead of placing the RCM out of the patient’s body as most surgical robots do, the RCM of the presented positioning arm is designed to be placed inside the patient’s body. Note that when applying to hysterectomy procedures, the RCM must be placed at or close to the cervix. The positioning arm has a spherical workspace, and the three actuated joints are designed to satisfy specific geometric arrangement so that the manipulation of the uterus can be achieved in a decoupled manner. A 1-DOF motorized uterus manipulator with a tilting tip is also designed and developed to enhance the ability of the robot assistant to perform anteversion and retroversion motions.
Experiments are conducted to verify the performance of the robot assistant, and the experimental results are presented. It is shown that the developed robot assistant can respond to the user’s commands and assist the user in uterus manipulation. Furthermore, when compare with solely human manipulation, the robot assistant shows the advantage of being able to retain a desired position in a more stable manner, which is precisely the goal of this prototype. Our robotic system can release a human assistant from the task of uterus positioning. This helps saving the valuable human resources in the operating theater. Besides, more reliable and stable positioning of uterus can also be achieved.
However, there are several disadvantages in our system, for example, space under the operating table is required when installing the robot assistant to the operating table. When encountering with operating tables with this space unavailable, the RCM of the robotic positioning arm will be unable to align with the patient’s cervix, which is undesirable. Also, due to the mechanical structure, the motion of joint 2 is comparatively not smoothly enough (see Figures 7 and 8) and the vibration frequency of the robot is high than that of human (see Figures 12, 13, and 14).
In the future, we would like to eliminate the necessity of under-bed space for installation so that the installation of robot can be more feasible when encountering with different operating tables. Also, we would like to improve the structure of the robotic system to increase its rigidity and reduce the system’s vibration. Improvements on the controller are also expected for the same purpose. One step further, image-based automatic control can also be implemented to provide more autonomy to the system.
Last but not the least, in our experiments, a manikin is used. Though medical manikin is the closest simulated environment when comparing to human, differences exist. Indeed, differences also exist among different patients. These differences may eventually affect the workspace and payload required for the robot. Thus, to obtain more realistic and reliable data for designing future robots, ex vivo experiments with cadavers and clinical trials are expected.
References
Reynolds RK, Advincula AP: Robot-assisted laparoscopic hysterectomy: technique and initial experience. Am J Surg 2006, 191: 555–560. 10.1016/j.amjsurg.2006.01.011
Farquhar CM, Steiner CA: Hysterectomy rates in the United States 1990–1997. Obstet Gynecol 2002, 99: 229–234. 10.1016/S0029-7844(01)01723-9
Beste TM, Nelson KH, Daucher JA: Total laparoscopic hysterectomy utilizing a robotic surgical system. J Soc Laparoendosc Surg 2005, 9: 13–15.
Diaz-Arrastia C, Jurnalov C, Gomez G, Townsend CJr: Laparoscopic hysterectomy using a computer-enhanced surgical robot. Surg Endoscopy 2002, 16: 1271–1273. 10.1007/s00464-002-8523-5
Hysterectomy: procedures, complications, and alternatives. Nova Science Publishers, Inc., New York,; 2011.
Guthart GS, Salisbury, J Jr (2000) The intuitive telesurgery system: overview and application In: Robotics and automation, 2000. Proceedings. ICRA ‘00. IEEE international conference on, vol. 1, 618–621.
Sackier JM, Wang Y: Robotically assisted laparoscopic surgery. Surg Endoscopy 1994, 8: 63–66. 10.1007/BF02909496
Taylor RH, Funda J, Eldridge B, Gomory S, Gruben K, LaRose D, Talamini M, Kavoussi L, Anderson J: A telerobotic assistant for laparoscopic surgery. IEEE Eng Med Biol Mag 1995, 14: 279–288. 10.1109/51.391776
Aiono S, Gilbert JM, Soin B, Finlay PA, Gordan A: Controlled trial of the introduction of a robotic camera assistant (endoassist) for laparoscopic cholecystectomy. Surg Endoscopy 2002, 16: 1267–1270. 10.1007/s00464-001-9174-7
Sharma D, Brown C, Kouriefs C, Sood H, Grange P, Patel H: Initial experience with the freehand robotic camera holder in laparoscopic urology. J Endourol 2009, 23(1):A249.
Berkelman P, Ma J: A compact modular teleoperated robotic system for laparoscopic surgery. Int J Robot Res 2009, 28: 1198–1215. 10.1177/0278364909104276
Swan K, Kim J, Advincula AP: Advanced uterine manipulation technologies. Surg Tech Int 2010, 20: 215–220.
Long JA, Cinquin P, Troccaz J, Voros S, Berkelman P, Descotes JL, Letoublon C, Rambeaud JJ: Development of miniaturized light endoscope-holder robot for laparoscopic surgery. J Endourol 2007, 21: 911–914. 10.1089/end.2006.0328
Kuo C-H, Dai J: Robotics for minimally invasive surgery: a historical review from the perspective of kinematics. In International symposium on history of machines and mechanisms. Edited by: Yan H-S, Ceccarelli M. Springer, Netherlands; 2009:337–354. 10.1007/978-1-4020-9485-9_24
Ng C, Chern B: Total laparoscopic hysterectomy: a 5-year experience. Arch Gynecol Obstet 2007, 276: 613–618. 10.1007/s00404-007-0385-6
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
HMY designed the robot, conducted the experiments, and drafted the manuscript. PL built the robot and participated in the advisory of the design of the robot. DN-A constructed the control system and conducted the experiments. Y-hL conceived the study and supervised and coordinated the project. All authors read and approved the final manuscript.
Hiu Man Yip, Peng Li, David Navarro-Alarcon and Yun-hui Liu contributed equally to this work.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cite this article
Yip, H.M., Li, P., Navarro-Alarcon, D. et al. Towards developing a robot assistant for uterus positioning during hysterectomy: system design and experiments. Robot. Biomim. 1, 9 (2014). https://doi.org/10.1186/s40638-014-0009-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40638-014-0009-0