
Abstract
Background
We tested the hypothesis that patients who continued buprenorphine postoperatively experience postoperative respiratory depression less frequently than those who discontinued buprenorphine.
Methods
This is a retrospective cohort study of patients who were on buprenorphine preoperatively. The primary outcome was postoperative respiratory depression as defined by respiratory rate < 10/minute, oxygen saturation (SpO2) < 90%, or requirement of naloxone for 48 h postoperatively. The secondary outcome was the composite of postoperative respiratory complications. The associations between postoperative buprenorphine continuation and respiratory depression and respiratory complications were estimated using separate multivariable logistic regression models, including demographic, intraoperative characteristics, and preoperative buprenorphine dose as covariates.
Results
Postoperative buprenorphine continuation was not associated with postoperative respiratory depression (adjusted odds ratio (OR), 1.11, 95% confidence interval (CI), 0.61 to 1.99, P=0.72). In subanalysis stratified by the preoperative buprenorphine dose, buprenorphine continuation was not associated with postoperative respiratory depression either when preoperative buprenorphine dose was high (≥16 mg daily) or low (<16 mg daily). Postoperative buprenorphine continuation was associated with lower incidence of postoperative respiratory complications (adjusted OR, 0.43, 95% CI, 0.21 to 0.86, P=0.02).
Conclusions
Continuing buprenorphine was not associated with respiratory depression, but it was associated with a lower incidence of respiratory complications.
Similar content being viewed by others


Background
Buprenorphine is a partial mu-opioid agonist with a high-receptor binding affinity [1, 2] used for both chronic pain and medication-assisted treatment for opioid use disorder. Within the therapeutic dose range, buprenorphine occupies mu opioid receptors (16 mg blocks > 80% of available mu-receptors) [3] and prevents other full agonists from binding. Postoperative pain management of patients on buprenorphine has been thought to be difficult even with high doses of additional opioid analgesics [4, 5]. For this reason, perioperative discontinuation of buprenorphine has been historically recommended [6, 7].
However, several recent studies reported higher pain scores [8] and a trend towards larger opioid dose requirements in the immediate postoperative period in patients who discontinued, versus continued, buprenorphine perioperatively [9]. Therefore, it is possible that patients who continue to receive buprenorphine postoperatively may experience less pain and require smaller dose of opioids, which results in less respiratory depression.
We therefore tested the hypotheses that patients who continue buprenorphine during the immediate postoperative period experience postoperative respiratory depression and respiratory complications less frequently than those who discontinue.
Methods
After institutional review board approval and waiver of consent (University of Washington IRB ID: STUDY00012186, approval date: 1/11/2021), we obtained data for adults taking buprenorphine preoperatively who underwent in-patient non-cardiac surgery under general or regional anesthesia. We performed a retrospective cohort analysis restricting our study to patients requiring postoperative hospital admission for at least 48 h at the University of Washington Medical Center (UWMC) or Harborview Medical Center (HMC) in Seattle, Washington between 2013 and 2020. Patients were excluded from the study if during the first 48 h postoperatively they (1) received epidural analgesia containing opioids (epidural opioids were not documented in our electronic medical record), (2) received mechanical ventilation with sedation, or (3) had two or more surgeries. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Patients were identified as taking buprenorphine preoperatively if (1) there were outpatient orders for buprenorphine before the index surgery, (2) there were inpatient orders for buprenorphine that were flagged as home medications before the index surgery through post-operative hospital discharge, or (3) buprenorphine was listed as a medication in the admission note or the pre-anesthesia assessment note.
Surgery types were initially categorized using the Agency for Healthcare Research and Quality (AHRQ) Clinical Classification procedure category and were assigned based on relative value unit (RVU) surgical current procedural terminology (CPT) codes from professional fee billing [10]. This identified specific surgery types, which were subsequently categorized into 13 categories based on the operative body site.
Outcomes
The primary outcome was postoperative respiratory depression as defined by respiratory rate < 10/minute, oxygen saturation (SpO2) < 90%, or requirement of naloxone to reverse the effect of opioids for 48 h postoperatively. The secondary outcome was the composite of postoperative respiratory complications defined as any of the following diagnoses determined by International Classification of Diseases (ICD)-9 and ICD-10 codes during postoperative admission: pneumococcal pneumonia; other bacterial pneumonia; bronchopneumonia, organism unspecified; pneumonia, organism unspecified; pulmonary collapse; pulmonary insufficiency following trauma and surgery; acute respiratory failure; other pulmonary insufficiencies, not elsewhere classified; apnea; other respiratory anomalies; respiratory arrest; pneumonia due to Streptococcus pneumoniae; pneumonia due to Hemophilus influenzae; bacterial pneumonia, not elsewhere classified; pneumonia, unspecified organism; acute respiratory distress syndrome; acute respiratory failure; respiratory failure, unspecified, unspecified whether with hypoxia or hypercapnia; atelectasis; other pulmonary collapses; apnea, not elsewhere classified; and respiratory arrest (Supplemental Table 1).
Additionally, acute pain intensity, defined as the time-weighted average (TWA) pain score, and opioid dose requirements in morphine milligram equivalents (MME) for 48 h postoperatively, were reported. Postoperative pain was evaluated by nurses using an 11-point numeric rating scale (NRS) (0=no pain, 10=worst pain possible) every 4 h until 48 h postoperatively. TWA pain score is equal to the sum of the portion of each time interval in-between two adjacent pain score measurements multiplied by the average of the corresponding two pain scores, and that was then divided by the time interval between the first and the last pain score measurements. Opioid dose requirements in MME for 48 h postoperatively, not including the dose of buprenorphine given postoperatively, was calculated using the Multicenter Perioperative Outcomes Group conversion table [11].
Statistical analyses
Univariable tests of association between demographic, intraoperative and postoperative characteristics, and postoperative buprenorphine continuation were conducted using Pearson’s chi-squared test for categorical variables and t test or Wilcoxon Mann-Whitney U test for continuous variables, as appropriate. Distributions of continuous variables were assessed visually using histograms.
The associations between postoperative buprenorphine continuation and respiratory depression and respiratory complications were estimated using separate multivariable logistic regression models. We hypothesized that the associations would be different for patients who were receiving a high (≥16 mg daily) versus low (<16 mg daily) dose of buprenorphine. Therefore, in addition to primary analysis without stratification by preoperative buprenorphine dose, we developed models in which postoperative buprenorphine continuation, preoperative buprenorphine dose (high/low), and their interaction were included as covariates.
A purposeful variable selection strategy, as described by Bursac et al., was utilized for variable selection and model development [12]. Variable entry criteria into the multivariable logistic regression model was P < 0.2 for univariable association with postoperative buprenorphine continuation (Table 1), and variable retention criteria in the multivariable model were P < 0.1, or variables which changed any of coefficient estimates of the variables of primary interest by > 10%. Calibration and discrimination of the final logistic regression models were assessed using the Hosmer-Lemeshow goodness of fit test and the c-statistic, respectively [13].
For both respiratory depression and respiratory complications outcomes, adjusted odds ratio estimates for the association between buprenorphine continuation and the outcome, with 95% simultaneous confidence intervals, were extracted from the final model using the multcomp package (generalized linear hypotheses function) in R program [14].
R statistical software, version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria), was used for all statistical analyses. The nominal type I error rate for hypothesis testing procedures and confidence intervals was fixed at 5%.
We anticipated 25% incidence of postoperative respiratory depression in our population based on the preliminary data search performed during the planning stage of the study. This confirmed that our sample size would provide power of 80% to detect a 15% difference in the incidence of respiratory depression between patients who continued versus discontinued buprenorphine postoperatively based on a Z test for independent proportions.
Results
Demographic, intraoperative, and postoperative characteristics
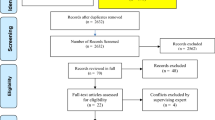
We retrieved the data of 330 unique patients who were on sublingual buprenorphine preoperatively. In six patients, preoperative daily buprenorphine dose was 0.5 mg despite having opioid use disorder. They were considered to be not on a stable dose of buprenorphine, rather in the process of uptitration of buprenorphine. Four patients had non-surgical diagnostic or therapeutic procedures under anesthesia. After removal of those patients, data of 320 patients were subjected to analysis (Fig. 1). Preoperative daily dose of buprenorphine was not significantly different between the patients who continued versus discontinued buprenorphine postoperatively (P=0.06), but a higher proportion of patients who continued buprenorphine postoperatively took the medication for opioid use disorder as opposed to chronic pain (P=0.01). Over the study period (2013 to 2020), the practice has shifted from discontinuing buprenorphine to continuing buprenorphine postoperatively (P=0.001). There was a significant difference in the makeup of surgery category based on body system between those who continued versus discontinued buprenorphine (P=0.02), and higher percentage of patients who continued buprenorphine was on antidepressants preoperatively (P=0.02) (Table 1).

Flow diagram
Postoperative opioid dose requirements and pain intensity
Opioid dose requirements in MME for 48 h postoperatively, excluding the dose of buprenorphine, was higher (P<0.001), and TWA pain score was higher, in patients who discontinued buprenorphine postoperatively than those who continued, in univariable analysis (P<0.001) (Table 2). The patients who continued received 28.0 [12.0 to 40.0] mg of buprenorphine for 48 h postoperatively.
Univariable association between postoperative buprenorphine continuation and respiratory depression and respiratory complications
The incidence of respiratory depression for 48 h postoperatively was not significantly different between those who continued versus discontinued buprenorphine, at 27.3% and 23.1%, respectively (P=0.40). Incidences of components of respiratory depression (i.e., respiratory rate < 10/minute and SpO2 < 90%) were not different between the two groups, and no patients required naloxone (Table 2). The detail of the components of the composite of respiratory complications is described in Supplemental Table 1. Respiratory complications were less frequent in those who continued buprenorphine than discontinued, with the incidences 10.7% and 19.1%, respectively (P=0.048). The three most common diagnosis of respiratory complications were atelectasis (ICD-10: J98.11), pneumonia, unspecified organism (ICD-10: J18), and acute respiratory failure (ICD-10: J96.0) (Table 2).
In the subgroup of preoperative low-dose buprenorphine (<16 mg daily), a continuation was not significantly associated with the incidence of respiratory depression (unadjusted odds ratio (OR), 0.71, 95% confidence interval (CI), 0.35 to 1.42). In the high-dose subgroup (≥16 mg daily), continuation was associated with a higher incidence of respiratory depression (unadjusted OR, 3.23, 95% CI, 1.36 to 7.69).
In the low-dose subgroup (<16 mg daily), continuation was associated with a lower incidence of respiratory complications (unadjusted OR, 0.32, 95% CI, 0.12 to 0.88). In the high-dose subgroup (≥16 mg daily), continuation was not associated with the incidence of respiratory complications (unadjusted OR, 0.84, 95% CI, 0.32 to 2.19).
Multivariable association between postoperative buprenorphine continuation and postoperative respiratory depression
The multivariable model showed good discrimination (a c-statistic equal to 0.71) and calibration (a Hosmer-Lemeshow Goodness-of-Fit test with P=0.78). Postoperative buprenorphine continuation was not associated with postoperative respiratory depression (adjusted OR, 1.11, 95% CI, 0.61 to 1.99, P=0.72).
The results of subanalysis stratified by preoperative buprenorphine dose are summarized in Table 3. The model term representing the hypothesized interaction between postoperative buprenorphine continuation and preoperative buprenorphine dose was not statistically significant (likelihood-ratio test: P=0.056) (Table 3), but the evidence was marginal (i.e., P value near 0.05). Further, in univariable analysis, buprenorphine continuation demonstrated non-statistical trend of protection against postoperative respiratory depression when preoperative dose was low (i.e., unadjusted OR, 0.71 for low dose), while buprenorphine continuation increased the risk of postoperative respiratory depression with statistical significance when preoperative dose was high (i.e., unadjusted OR, 3.23 for high dose). Therefore, postoperative buprenorphine continuation x preoperative buprenorphine dose interaction term was included in the multivariable model of the subanalysis. When preoperative buprenorphine dose was low (<16 mg daily), continuation was not associated with postoperative respiratory depression (adjusted OR, 0.71, 95% CI, 0.30 to 1.68, P=0.599). When preoperative buprenorphine dose was high (≥16 mg daily), continuation was not associated with postoperative respiratory depression (adjusted OR, 2.19, 95% CI, 0.76 to 6.27, P=0.182) (Table 4).
Multivariable association between postoperative buprenorphine continuation and respiratory complications
The results of the multivariable logistic regression model for postoperative respiratory complications are summarized in Table 5. This multivariable model showed good discrimination (a c-statistic of 0.69) and calibration (a Hosmer-Lemeshow Goodness-of-Fit test of P=0.99). The model term representing the hypothesized interaction between postoperative buprenorphine continuation and preoperative buprenorphine dose was not statistically significant (likelihood-ratio test: P=0.13), and the univariable association between buprenorphine continuation and postoperative respiratory complications was in the same direction when preoperative buprenorphine dose was low and high (i.e., unadjusted OR, 0.32 for low dose, and unadjusted OR, 0.84 for high dose). Therefore, postoperative buprenorphine continuation x preoperative buprenorphine dose interaction term was not included in the multivariable regression model for this outcome. Postoperative buprenorphine continuation was associated with lower incidence of respiratory complications (adjusted OR, 0.43, 95% CI, 0.21 to 0.86, P=0.02) (Table 5).
Discussion
Among inpatient surgical patients taking sublingual buprenorphine preoperatively, continuation during the first 48 h postoperatively was not associated with postoperative respiratory depression. However, postoperative buprenorphine continuation was associated with 57% decreased odds of respiratory complications than postoperative discontinuation. As postoperative respiratory complications have major impact on morbidity and also leads to increased length of hospital stay, continuation of buprenorphine might lead to significant cost saving.
When stratified by preoperative buprenorphine dose, postoperative buprenorphine continuation was associated with non-statistically significant trend of decreased respiratory depression when preoperative buprenorphine dose was low (< 16 mg daily) and with non-statistically significant trend of increased respiratory depression when preoperative buprenorphine dose was high (≥16 mg daily).
Opioid dose requirements (excluding buprenorphine dose given postoperatively) and time weighted average pain scores during postoperative 48 h were lower when buprenorphine was continued postoperatively. This may be partially explained by the analgesic effect of buprenorphine. As extensive dose-response relationship of the analgesic effect of buprenorphine over the entire clinical dose range has not been available, the dose at which buprenorphine reaches analgesic ceiling effect as a partial mu-agonist is not known. However, at least in the range of daily buprenorphine dose given postoperatively in our study (i.e., 14.0 [6.0–20.0] (median [Q1–Q3])), buprenorphine seemed to exert additive analgesic effect with other mu-agonists.
The most frequently reported components of composite of respiratory complications were atelectasis, pneumonia, and acute respiratory failure. Therefore, the lower incidence of respiratory complications when buprenorphine was continued versus discontinued are mainly attributed to the difference in the incidences of those components. Lower TWA pain score with continuation (5.3 ± 2.4, versus 6.2 ± 1.9 with discontinuation) could at least partially explain the association between continuation and the lower incidence of respiratory complications. Half of the patients included in the current study underwent surgeries involving musculoskeletal system, and associations between lower incidences of pneumonia and respiratory failure and lower amounts of opioid consumption have been reported after total knee arthroplasty [15]. Therefore, it seems that pain, and immobility caused by pain, increase the risk of postoperative respiratory complications in those undergoing musculoskeletal surgery.
There are several limitations inherent to the current study. We used respiratory rate < 10/minute, SpO2 < 90%, and requirement of naloxone as the definition of respiratory depression (none of our patients received naloxone) in line with the cutoff values for respiratory rate and SpO2 described in the practice guidelines for the American Society of Anesthesiologists (ASA) as clinical signs of opioid-induced respiratory depression [16]. Respiratory rate and SpO2 were collected through routine checks every 4 h by ward nurses in the majority of our patients. In a study of continuous oxygen saturation monitoring for 48 h following non-cardiac surgery, 90% of serious hypoxemic events (SpO2 < 90% for ≥ 1 h) were missed by routine every 4 h vital sign checks [17]. Therefore, it is very likely that many hypoxemic events were undetected and the true incidence of hypoxemia was much higher in both patients who continued and discontinued buprenorphine postoperatively.
Another limitation is the use of ICD-9 and ICD-10 codes to capture postoperative respiratory complications. Although the incidence of postoperative complications based on ICD coding, and that based on prospective assessment of complications, have been reported to be similar, ICD coding captured events of minor clinical importance [18]. Therefore, the incidence rates of respiratory complications in the current study might be somewhat inflated.
Conclusions
Continuation of buprenorphine for the first 48 h postoperatively was not associated with postoperative respiratory depression. Postoperative buprenorphine continuation was associated with a lower incidence of postoperative respiratory complications than postoperative discontinuation.
Availability of data and materials
The data that support the finding of this study are available from the corresponding author, RK, upon reasonable request.
Abbreviations
- SpO2 :
-
Oxygen saturation
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- IRB:
-
Institutional review board
- ID:
-
Identification number
- UWMC:
-
University of Washington Medical Center
- HMC:
-
Harborview Medical Center
- STROBE:
-
Strengthening the Reporting of Observational Studies in Epidemiology
- AHRQ:
-
Agency for Healthcare Research and Quality
- RVU:
-
Relative value unit
- CPT:
-
Current procedural terminology
- ICD:
-
International Classification of Diseases
- TWA:
-
Time weighted average
- MME:
-
Morphine milligram equivalents
- NRS:
-
Numeric rating scale
- ASA:
-
American Society of Anesthesiologists
References
Potter JS, Dreifuss JA, Marino EN, Provost SE, Dodd DR, Rice LS, et al. The multi-site prescription opioid addiction treatment study: 18-month outcomes. J Subst Abuse Treat. 2015;48:62–9.
Weiss RD, Potter JS, Griffin ML, Provost SE, Fitzmaurice GM, McDermott KA, et al. Long-term outcomes from the National Drug Abuse Treatment Clinical Trials Network Prescription Opioid Addiction Treatment Study. Drug Alcohol Depend. 2015;150:112–9.
Greenwald MK, Comer SD, Fiellin DA. Buprenorphine maintenance and mu-opioid receptor availability in the treatment of opioid use disorder: implications for clinical use and policy. Drug Alcohol Depend. 2014;144:1–11.
Huang A, Katznelson R, de Perrot M, Clarke H. Perioperative management of a patient undergoing Clagett window closure stabilized on Suboxone(R) for chronic pain: a case report. Can J Anaesth. 2014;61:826–31.
Mccormick Z, Chu SK, Chang-Chien GC, Joseph P. Acute pain control challenges with buprenorphine/naloxone therapy in a patient with compartment syndrome secondary to McArdle’s disease: a case report and review. Pain Med. 2013;14:1187–91.
Anderson TA, Quaye ANA, Ward EN, Wilens TE, Hilliard PE, Brummett CM. To stop or not, that is the question. Anesthesiology. 2017;126:1180–6.
Childers JW, Arnold RM. Treatment of pain in patients taking buprenorphine for opioid addiction #221. J Palliat Med. 2012;15:613–4.
Quaye A, Potter K, Roth S, Acampora G, Mao J, Zhang Y. Perioperative continuation of buprenorphine at low-moderate doses was associated with lower postoperative pain scores and decreased outpatient opioid dispensing compared with buprenorphine discontinuation. Pain Med. 2020;21:1955–60.
Martin YN, Deljou A, Weingarten TN, Schroeder DR, Sprung J. Perioperative opioid requirements of patients receiving sublingual buprenorphine-naloxone: a case series. BMC Anesthesiol. 2019;19:68.
Agency for Healthcare Research and Quality (AHRQ) Clinical Classification procedure category. Available from: https://www.hcup-us.ahrq.gov/toolssoftware/ccs_svcsproc/ccssvcproc.jsp. Accessed 27 Mar 2022.
Multicenter perioperative outcomes group oral morphine equivalent. Available from: https://phenotypes.mpog.org/Oral Morphine Equivalent. Accessed 27 Mar 2022.
Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. Source Code Biol Med. 2008;3:1–8 Biomed central.
Austin PC, Steyerberg EW. Interpreting the concordance statistic of a logistic regression model: relation to the variance and odds ratio of a continuous explanatory variable. BMC Med Res Methodol. 2012;12:1–8.
Hothorn T, Bretz F, Westfall P. Simultaneous inference in general parametric models. Biometrical J J Math Methods Biosci. 2008;50:346–63.
Ofa SA, Ross BJ, Flick TR, Patel AH, Sherman WF. Robotic total knee arthroplasty vs conventional total knee arthroplasty: a nationwide database study. Arthroplast Today. 2020;6:1001–8.
American Society of Anesthesiologists Task Force on Neuraxial Opioids. Practice guidelines for the prevention, detection, and management of respiratory depression associated with neuraxial opioid administration. Anesthesiology. 2009;110:218–30.
Sun Z, Sessler DI, Dalton JE, Devereaux PJ, Shahinyan A, Naylor AJ, et al. Postoperative hypoxemia is common and persistent: a prospective blinded observational study. Anesth Analg. 2015;121:709.
Campbell PG, Malone J, Yadla S, Chitale R, Nasser R, Maltenfort MG, et al. Comparison of ICD-9–based, retrospective, and prospective assessments of perioperative complications: assessment of accuracy in reporting. J Neurosurg Spine. 2011;14:16–22.
Acknowledgements
The authors would like to thank the Center for Perioperative & Pain initiatives in Quality Safety Outcome (PPiQSO) and the Department of Anesthesiology and Pain Medicine at the University of Washington, Seattle, for support of this project including provision of expertise to obtain the data extract analyzed in the present work.
Funding
This work was internally supported by the Department of Anesthesiology and Pain Medicine, University of Washington.
Author information
Authors and Affiliations
Contributions
Ryu Komatsu: This author helped design the analysis plan, extract study data, perform data analysis, draft the manuscript, and approved the final manuscript. Michael Singleton: This author helped to perform data analysis, draft the manuscript, and approve the final manuscript. Katherin Peperzak: This author helped to draft the manuscript and approved final manuscript. Jiang Wu: This author helped to draft the manuscript and approved final manuscript. Emily Dinges: This author helped to draft the manuscript and approved the final manuscript. Laurent Bollag: This author helped to draft the manuscript and approved the final manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the institutional review board with waiver of consent (University of Washington IRB ID: STUDY00012186, approval date: 1/11/2021). Patients’ written informed consent to participate in the study and publication of the study results were waived by the University of Washington IRB.
Consent for publication
Patients’ written informed consent to participate in the study and publication of the study results were waived by the University of Washington IRB.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1
. Description of individual components of postoperative respiratory complications.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Komatsu, R., Singleton, M.D., Peperzak, K.A. et al. Postoperative respiratory depression in patients on sublingual buprenorphine: a retrospective cohort study for comparison between postoperative continuation and discontinuation of buprenorphine. JA Clin Rep 8, 45 (2022). https://doi.org/10.1186/s40981-022-00535-2
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40981-022-00535-2