
Abstract
Background
Non-communicable diseases (NCDs) are a global epidemic challenging global public health authorities while imposing a heavy burden on healthcare systems and economies.
Aim
To explore and compare the prevalence of NCDs in South Asia, the Caribbean, and non-sub-Saharan Africa, aiming to identify both commonalities and differences contributing to the NCD epidemic in these areas while investigating potential recommendations addressing the NCD epidemic.
Method
A comprehensive search of relevant literature was carried out to identify and appraise published articles systematically using the Cochrane Library, Ovid, Google Scholar, PubMed, Science Direct, and Web of Science search engines between 2010 and 2023. A total of 50 articles fell within the inclusion criteria.
Results
Numerous geographical variables, such as lifestyle factors, socio-economic issues, social awareness, and the calibre of the local healthcare system, influence both the prevalence and treatment of NCDs. The NCDs contributors in the Caribbean include physical inactivity, poor fruit and vegetable intake, a sedentary lifestyle, and smoking, among others. While for South Asia, these were: insufficient societal awareness of NCDs, poverty, urbanization, industrialization, and inadequate regulation implementation in South Asia. Malnutrition, inactivity, alcohol misuse, lack of medical care, and low budgets are responsible for increasing NCD cases in Africa.
Conclusion
Premature mortality from NCDs can be avoided using efficient treatments that reduce risk factor exposure for individuals and populations. Proper planning, implementation, monitoring, training, and research on risk factors and challenges of NCDs would significantly combat the situation in these regions.
Similar content being viewed by others


Introduction
Background
Non-communicable diseases (NCDs), also referred to as chronic diseases, typically follow a life course progression and are brought on by a confluence of genetic, physiological, environmental, and behavioral variables [50]. The commonest dominating global NCDs are diabetes, cancer, chronic respiratory diseases (such as chronic obstructive pulmonary disease and asthma), and cardiovascular disorders (including heart attacks and stroke) [91]. NCDs are a global epidemic with progressive burdens across countries. They were primarily a matter of discussion in wealthy nations for many years, but today, they are the primary issue facing the countries of the developing world [44]. These patterns reflect our expanding society, hasty unplanned urbanization, and sedentary lifestyles [24]. Hospital-centered acute care is currently the main focus of healthcare for NCDs in many low- and middle-income countries [2]. The NCD epidemiologic transition is at varying stages in several nations. Many environmental, social, and structural changes occur when nations move from agrarian to industrial to postindustrial states. Some of these changes improve life expectancy, while others subject people to chronic risk exposures [76]. Nearly four out of five NCD-related fatalities take place in low- and middle-income nations, which are disproportionately affected by NCDs [90]. However, the problems mentioned above vary across different countries and regions. Thus, studying the main causes, prevalence, and impact of NCDs in vulnerable areas of the world is of public health importance.
South Asia, the Caribbean, and Africa represent diverse geographic regions, all of which are affected by NCDs superfluously. NCDs are becoming more prevalent throughout South Asia, causing serious health problems and economic losses while contributing to nearly two-thirds of all fatalities [33]. NCDs are also emerging as the primary cause of death in sub-Saharan Africa, where they accounted for 37% of fatalities in 2019 when compared to 24% in 2000 [92]. According to the 2022 World Health Organisation (WHO) Non-communicable Disease Progress Monitor, NCDs account for 50–88% of fatalities in seven African countries, most of which are small island states [92]. Similarly, research asserts that NCDs account for a significant portion of the disease burden in Latin America and the Caribbean (LAC), causing three out of every four deaths [12, 13, 15]. However, NCD mortality is rapidly increasing, and by 2030, those above four major NCDs will be responsible for about 81% of deaths in Latin America and the Caribbean [78].
Objective of the study
Numerous global studies address NCDs in the areas of South Asia, Africa, and the Caribbean. Some of these studies explain the links between lifestyle factors, like poor diet, tobacco use, and NCDs in these areas [59, 88]. Others evaluate the impact of the economy, poverty, industrialization, and the reduction of urban green space [4, 52, 84]. The importance of good quality health care in managing NCDs has also been discussed [56, 84].
A recurrent finding in a significant number of these papers is the association between poverty, economic development, and NCDs [7, 34, 58, 61, 62, 64, 77, 84]. However, existing studies provide fragmented evidence and indications of the impact of NCDs on the different low- and middle-income regions [23, 33, 40, 85]. Therefore, a more comprehensive overview is merited. Indeed, having a comprehensive understanding of the different contributing factors of NCDs and their impact on underprivileged regions is of importance and corresponds to the Sustainable Development Goal (SDG) 3 of “ensuring health, life, and well-being for all” [1], ECALC 2021). To our knowledge, no comparative review article explores the NCDs situation in South Asia, Africa, and the Caribbean countries. This systematic review aims to compare the prevalence, risk factors, and challenges associated with NCDs in South Asia, the Caribbean, and the African continent. The objective is to highlight the importance of acknowledging the burden of NCDs in low-middle-income countries, which is a requisite for a sustainable future.
Method
Literature selection
A literature search was conducted through different sources, including Cochrane Library, Ovid, Google Scholar, PubMed, ScienceDirect, and the Web of Science search engine. The search strategy was based on the following keywords; “Health Literacy” OR “Inadequate Health Literacy” OR “Adequate Health Literacy”) AND (“Non-communicable diseases” OR “NCDs” OR “NCDs Comparison” OR “Diabetes” OR “Cardiovascular disease” OR “CVD” OR “Chronic Kidney Disease” OR “CKD” OR “Hypertension” OR “Heart Disease” OR “High Blood Pressure” OR “Coronary Heart Disease” OR AND (“South Asia” OR “India” OR “Pakistan” OR “India” OR “Sri-Lanka” OR “Bangladesh” OR “Bhutan” OR “Maldives” OR “Afghanistan” AND “Caribbean” OR “Algeria” OR “Djibouti” OR “Egypt” OR “Libya” OR “Morocco” OR “Somalia” OR “Sudan” OR “Tunisia”. We have limited our search to literature published from 2010 till July 2023 to maintain significance.
It is important to mention that in writing this review, we have not collected any primary data that involves human or animal subjects. Instead, we gathered secondary data from previously published articles. Therefore, ethical clearance was considered not applicable in this case.
The PICO framework was used to establish the inclusion criteria for this systematic review, as seen in Table 1. The research participants (P) included low-middle-income countries in the regions of South Asia, Africa, and the Caribbean. More specifically for South Asia, the South Asian Association for Regional Co-operations (SAARC) countries were included. These are Bangladesh, Bhutan, India, Nepal, Pakistan, Sri Lanka, Afghanistan, and the Maldives. African countries included in the systematic review were Algeria, Djibouti, Egypt, Libya, Morocco, Somalia, Sudan, and Tunisia [37]. We have considered these non-Sub-Saharan African countries as, according to the literature, NCDs are prevalent in these countries, as noted by Dalal et al. [20], and Formenti et al. [29]. Moreover, Sub-Saharan African countries were excluded because, even though they are classified as low-middle income countries, NCDs are not the primary cause of death or potential life years lost in these nations [63]. In the Caribbean, the areas having the highest death rates due to the four common NCDs were considered. These areas and their respective cumulative proportion of deaths attributed to these four NCDs are as follows: Bermuda (2005–2014) 62.97%, Grenada (2005–2014) 60.09%, Montserrat (2005–2014) 66.59%, and Trinidad and Tobago (2001–2010) 59.21% [80]. Studies discussed in this review include participants across different age groups and genders who have non-communicable diseases and are from these specified regions. For intervention (I), we focused on evaluating the effect of a balanced and healthy lifestyle, socio-economic factors, regional regulations, and quality of healthcare on NCDs. A descriptive comparison (C) was made between different regions of South Asia, Africa and the Caribbean. The outcome (O) of interest was the prevalence of NCDs, risk factors, and challenges among low and middle-income populations while assessing for measures to address them.
Studies of various designs were included in this review, including qualitative, quantitative, cross-sectional and comparative studies. Additionally, studies used were published in English within the last 20 years.
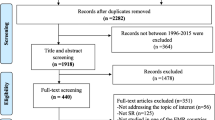
We adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, as seen in Fig. 1. A total of 50 literatures from South Asia, Africa, and the Caribbean Islands were analyzed in this review.

PRISMA flowchart
Assessment of risk of bias
The assessment of potential biases in studies chosen for this review was conducted using the updated Mixed Methods Appraisal Tool (MMAT), described by [42]. Each study was labeled as having a low, medium or high risk of bias within the relevant category. By using this tool, we were able to evaluate the design, methodology and validity of the included studies in order to enhance reliability of our conclusion as well as minimize bias.For the primary standardized appraisal, we have assessed all studies used in the review process using the same criteria. As the MMAT included criteria to evaluate qualitative, quantitative, and mixed methods, thus this comprehensive coverage of literature selections is rigorously evaluated, reducing the risk of bias from overlooking certain study designs. In addition, to enhance the reliability, more than one co-author independently reviewed and assessed each study. We have emphasized the relevance and rigor of studies to ensure that only methodologically sound and contextually appropriate studies are included in our review. This dual focus helped us minimize biases by including irrelevant or poorly conducted studies.
Results
Overview
In this comparative systematic review, 50 studies were included to explore the relationship between the prevalence, risk factors, challenges, and management of NCDs among the regions of South Asia, Africa, and the Caribbean. The prevalence and management of NCDs are determined by a variety of regional factors, including lifestyle factors, socio-economic factors, and the quality of the area’s healthcare system [17, 28].
Lifestyle factors and NCDs
A significant number of NCDs have been associated with unhealthy lifestyles. Therefore, transitioning to a healthier lifestyle is cost-effective to prevent these diseases [95]. Several studies have investigated the correlation between tobacco use and NCDs in South Asia. Tobacco is widely used in the region and was found to play a big role in NCD deaths, with the greatest number of NCD-related deaths among females noted in Maldives (79.4%) [88]. Similarly, Riaz et al. [81] conducted a cross-sectional study on NCD risk factors among Bangladesh’s adult population, which referred to tobacco usage as the chief risk factor for major NCDs in the area. This study also implied that those with sedentary lifestyles and poor eating habits are more predisposed to health issues like obesity and hypertension [81]. Overall, NCDs emerge as the leading cause of death and disability in the region of South Asia. Concerning this, dietary risks and tobacco usage were among the top three risk factors for premature death and disability, demonstrating the relationship between behavioral factors and NCDs [85].
The commonest lifestyle factors affecting NCDs in the Eastern Mediterranean Region (EMR) are unhealthy dietary habits, smoking, physical inactivity, and alcohol misuse. [5]. In countries like Libya, cardiovascular disorders, diabetes, hypertension, and cancer are on the rise, with physical inactivity being the key risk factor [9, 66]. Studies have shown that most people in EMR are unaware of having NCD risk factors. In fact, lifestyle changes over the years have increased NCD risk factors [9]. Evidence shows that effective interventions aimed at lowering the level of exposure of individuals and populations to risk factors such as smoking, malnutrition, inactivity, and alcohol misuse could have prevented 80% of premature deaths caused by NCDs in Morocco and neighboring countries [53, 68].
Similar studies were also conducted in the Caribbean. Prevalent NCD risk factors in the area were found to be physical inactivity, inadequate fruit and vegetable intake, a sedentary lifestyle, soft drink and fast-food consumption, and tobacco use [75]. This was especially representative of the student population. Most students were found to have three or more NCD risk factors. Psychological distress and advanced age increased the likelihood of having these risks, while good parental support and school attendance decreased it [75].
Socio-economic factors and NCDs
The link between socio-economic factors like poverty, industrialization, urbanization, and country regulations has been studied thoroughly. Mirelman et al. [64] established the relationship between NCD occurrence and poverty in Bangladesh. Their results demonstrate that actions taken to reduce the burden of NCDs may help reduce household poverty, which will have benefits beyond better health. The rising burden of NCDs imposes significant costs on Afghanistan, having a negative impact on the country’s economy and reducing access to primary health care [69]. In contrast, in Sri Lanka, most medications are afforded by most people, regardless of their income. This affordability and accessibility of medications is thought to be due to the availability of numerous generic brands both in semi-government and private pharmacies [19]. In India, NCDs are rising due to industrialization, socio-economic development, and urbanisation, apart from changing age demographics and lifestyles [72].
Fewer studies have discussed socio-economic factors and NCDs in the African region. Extreme poverty and poor access to medical care have been linked with increasing health issues [29]. Similar to other developing nations, countries like Djibouti, Egypt, Libya, Morocco, Somalia, Sudan, and Tunisia have experienced a shift in the disease burden over the past three decades from communicable illnesses to NCDs [5]. What makes the situation worse is the significant disparities in access to NCD treatment among the various social groups. It was reported that access to NCD therapy is being disproportionately denied to the poor, young males and those living outside Urban Governorates [27].
The prevalence of NCDs in Latin America and the Caribbean is also greatly influenced by underlying socio-economic factors. Both rapid urbanization and globalization have been linked to poor lifestyle choices, such as the consumption of fast food and reduction in physical activity, which predispose individuals to NCDs. (Bonnila-Chacin, 2013). A region’s socio-economic factors also impact health status through their role in determining the availability of nutritious food and clean water [51]. Furthermore, once again, studies show that NCD management, including medications and health care systems, is less accessible to those who are socially and economically disadvantaged [52].
Policies, regulations, and NCDs
Biswas et al. [14] assessed the extent to which Bangladesh's NCD-related regulations adhered to WHO's 2013–2020 Action Plan for the Global Strategy for the Prevention and Control of NCDs. Findings reveal that while many NCD-related policies are in place, they lack proper planning, implementation, monitoring, training, and research [8]. In fact, countries like Bangladesh and Pakistan have struggled to combat the rising burden of NCDs effectively [57, 94]. Results indicate that the first step to combating NCDs is by creating NCD preventative programs and implementing current NCD regulations [65]. Similarly, studies in Afghanistan also show that good governance is fundamental to tackling NCDs, as this would result in better health promotion, community education, and the improvement of healthcare systems [70]. This applies to the rest of the South Asian region. In fact, in Bhutan, where Gross National Happiness (population well-being) is a priority for the government, applying strategic opportunities to address NCDs is necessary to improve well-being. This will require collaboration between healthcare, government, and other sectors [86].
Enhancing the level of public awareness of NCDs can give a better result to mitigate the situation. Daoud and Meddeb [21] believe that integrating active communication, participation, and support with the social community would help improve the current condition in Tunisia. However, public awareness on its own may not be sufficient. Taking the Sudanese nationals as an example, despite knowing the importance of a healthy lifestyle, most still do not adhere to one, and therefore, behavioral interventions are still required [36]. Like in South Asian countries, policy-making and implementation are also important in African nations. NCDs are affected by long-term disruptions in health services and policy-making processes in Libya [6, 82]. By providing survey-based proof of the burden of NCDs, WHO is raising awareness of the prevalence of NCDs and starting the conversation on the significance of low-cost public health care and community-based interventions for NCD management and prevention in Somalia (World Health Organisation, 2017). To prevent and control NCDs in Somalia, the following steps have been found significant: providing information on the WHO’s global strategic approach, discussing insights gained from other nations, monitoring and applying interventions targeting NCDs and associated risk factors, and encouraging the participation of Somali health authorities in both regional and international events [66].
Caribbean heads of state emphasized the 2030 Agenda for Sustainable Development's commitment to ensuring people can realize their potential in a healthy environment [1]. To do so, the region must adopt affordable policies to prevent NCD risk factors and promote access to high-quality healthcare in a situation where a sizable portion of the workforce is employed in the unorganized sector [10]. Although monitoring systems have been implemented [41], more specific objectives are still required, particularly for government entities that do not deal with health. Like African countries, inadequate funding has hindered several resource-dependent interventions in the Caribbean region [41]. The main difficulty in combating NCDs requires a coordinated, multifaceted, and persistent strategy with therapies, policy changes, and education [60]. Apart from this, the Caribbean culture, being shaped by different historical, economic, and political experiences, also plays a role in the region’s NCD-related policies [83]. However, information on the relationship between culture and NCD management is still scarce, and further research and evaluation are required, given the region’s cultural diversity and high NCD mortality [80].
Health care systems and NCDs
The importance of good quality healthcare systems for the prevention and management of NCDs in low- and middle-income countries has been assessed in different studies. In India, the fight against NCDs has been hindered by under-trained healthcare workers, primary care providers with insufficient knowledge or skills, and the obscure roles of different healthcare sectors in delivering medical services [89].
Rawal et al. [79] explored the possibility of enhancing the delivery of NCD services at the primary healthcare level. Their study assessed healthcare practitioners' perspectives on NCD prevention and management services offered through the NCD corners in Bangladesh. Patients who participated in these studies acknowledged the government's initiative to set up NCD corners to support the provision of NCD services. They believed that the NCD corners had significantly contributed to raising NCD awareness, providing NCD care, and offering referral services. However, participants also noted a number of issues with these NCD corners. These included a shortage of skilled personnel, subpar equipment and labs, poor logistics and medication supply, inadequate reporting and record-keeping, a lack of coordination, and an absence of good guidelines. Similar studies were also carried out in other areas, like Pakistan, Sri Lanka, and Bhutan. A common finding is the importance of NCD prevention public health models through good quality services and efficient healthcare workers [8, 18, 71, 87].
Funding pressures have been made worse by integration and coordination issues. Low funds are associated with less employee motivation and negatively affect primary healthcare [30]. This is the case in Tunisia, where, despite the importance of primary healthcare, the country is unprepared to manage NCDs [82]. The primary change that has filled the gap is private healthcare. However, in countries like Morocco, where health systems are well-funded and public services are free, there is still the question of quality [68]. Therefore, appropriate and good quality equipment is also necessary.
Studies carried out in the Caribbean also reveal significant faults in healthcare systems and how they contribute to NCDs. For instance, it was found that those who suffer from hypertension and diabetes and are managed at a primary care level do not reach optimal blood pressure or blood glucose levels. This results from healthcare workers not adhering to the recommended guidelines [80]. Contrastingly, other studies show that improvement in primary healthcare has enabled population aging, increasing NCD prevalence [80]. Multimorbidity is also an issue in this region, with the most commonly co-existing NCDs being diabetes and heart disease. A positive correlation was found between multimorbidity, out-of-pocket expenses, and challenges in affording healthcare. This leads to poorer health outcomes and a higher risk of NCDs [54].
Risk of bias
For this systematic review, we evaluated the included studies for potential bias, summarized in Table 2. While most of the studies exhibited a low risk of bias, a few showed medium to high-risk bias and fell under the following categories: information, confounding, and selection bias. For studies that were found to have a medium or high-risk information bias, this was mostly due to the author’s own perception and a lack of participant knowledge or information. Confounding bias occurred due to uncontrolled variables, like the combination of NCD risk factors that may be present simultaneously and, therefore, impact study results. Selection bias was mostly present in studies that included specific subgroups of participants that were not representative of the whole population or had a small sample size. Overall, this evaluation revealed a number of potential biases that could influence the analysis in this review.
Discussion
Interpretation of results
NCDs enhance the disease burden through both morbidity and mortality and are considered a global health epidemic. This systematic review aimed to assess and compare NCDs' prevalence, risk factors, challenges, and management in South Asia, Africa, and the Caribbean.
In this systematic review, an important similarity was noted in the contributing factors for the development of NCDs among the three regions examined. Poor lifestyle choices, including a sedentary lifestyle, poor diet, tobacco use, alcohol misuse and physical inactivity emerge as common NCD risk factors in these locations. These findings highlight the importance of targeted public health interventions and population education. By addressing these risk factors through promotion of healthy lifestyle choices, the prevalence of NCDs in these regions may be reduced significantly [4, 36, 80]. Overall, the burden of NCDs in South Asia is shaped by complex social determinants and mostly caused by the region's fast urbanization, shifting lifestyles, and aging population [48]. Diabetes, cardiovascular disease, and respiratory problems are a few of the main causes of morbidity and mortality in the area, and poor lifestyle habits and air pollution influence them [25]. Mental health is prioritized in Pakistan and Bangladesh, but lacks regulations for mental health education and integration with NCD services. Thus, experts suggest multi-component, whole-systems approaches to enhance self-management, focusing on patient empowerment, education, tailored behavioural interventions, and better healthcare support in the region. Similarly, in Africa, NCDs are becoming a significant public health concern, with cardiovascular disease, chronic respiratory diseases, diabetes, and cancer becoming prevalent [35]. Once again, lifestyle factors and a deficient healthcare system are contributing factors. Furthermore, co-existing diseases prevalent in this region, such as HIV and malaria, create even more healthcare challenges [73]. Likewise, cardiovascular diseases, diabetes, and cancer are among the most common health issues in the Latin American and Caribbean region, with poor lifestyle factors being the most prevalent risk factors (Macinko,2019). Addressing these lifestyle factors and promoting healthier habits by enhancing awareness, education, and implementing focused interventions is the first step in preventing and managing NCDs.
Multiple studies showed that unfavorable living environments, inadequate healthcare funding, and the absence of regulations and policy reinforcement contribute to NCDs in low- and middle-income countries [17, 28]. Additionally, poor health infrastructure, limited access to health services, and a lack of resources further contribute to the burden of NCDs [46]. NCDs impose significant burdens on the economies of low- and middle-income nations, mainly due to the high cost of medications and health services, which may often exceed financial means of both the individual and the healthcare system. Additionally, there is also loss of income during time off work of both the affected individuals and their caregivers [47]. It is, therefore, imperative to foster multisectoral collaborations, with the recommendation that primary care is directly funded to manage this epidemic while simultaneously strengthening and incorporating NCD-specific services into the pre-existing systems. It was highlighted that NCD service funding is an important subject, especially in low- and middle-income countries. Therefore, proper funding and accessibility of good quality healthcare services for the early recognition and treatment of NCDs is the way forward. However, over the past ten years, there has been a downward trend in international donor support for preventing NCDs [74] and a significant mismatch between available resources and requirements in these nations. Comparing NCDs' financial analysis and political economy, Jakovljevic et al. [45] advised that the WHO outreach initiatives in Asia, Africa, and the Caribbean are insufficient to eradicate NCDs. However, they may be strengthened by going beyond capacities and being willing to invest in more relevant resources.
Besides ensuring affordability of healthcare services, it is also imperative to ensure delivery of a good standard of care. Caribbean primary care centers’ readiness for NCD interventions, identifying insufficient resources and training but also staff support and stakeholder optimism. Nurses’ roles in managing chronic illnesses in Africa, highlighting their active involvement but also noting challenges like shortages and inadequate training is a barrier. Poorly trained health care professionals, a lack of standard operating procedures, inadequate equipment and poorly maintained facilities all contribute to ineffective medical care and therefore, delay diagnosis and hinder management of NCDs [80, 87, 89]. Contrastingly, some studies also showed that the improvement in the quality of healthcare is leading to population aging and increasing the prevalence of multimorbidity and NCDs. In view of this, health care systems need to adapt by working on preventative care and the management of comorbidities [80]. Integrated care models for HIV and NCD comorbidities in Sub-Saharan Africa, finding benefits like improved patient retention and NCD detection but also increased burdens on existing staff. Therefore, effective NCD control requires overcoming several challenges, including scarce resources, a lack of political commitment, inadequate healthcare systems, and social and cultural variables.
By recognizing the main factors leading to the rise of NCDs in low- and middle-income countries, one can improve management by targeting the root of the problem. One of the most effective approaches to targeting risk factors is by enhancing public awareness and education to avoid harmful risk factors. However, information on its own is not sufficient. People also require the implementation of effective regulations and policies to encourage them to live a healthy lifestyle and take care of their health. It is also important that individuals have access to affordable healthcare services that offer quality care. This might reduce health discrepancies and improve quality of life across different populations with different financial means.
Study limitations
While this systematic review discusses valuable insights on NCDs in South Asia, Africa, and Latin America, it is also important to address the encountered limitations. These were primarily due to the variations in the quality of the reviewed studies. Three main categories were identified in evaluating risk bias: information, confounding, and selection bias.
Conclusion
The NCD situation in South Asia, the Caribbean, and Africa showcased similarities and differences. However, all three regions are being significantly affected by NCDs. The increased frequency of NCDs in these areas results from lifestyle factors, socio-economic inequalities, a lack of NCD regulations, and issues with the healthcare system. Indeed, healthcare systems in these regions face challenges in effectively addressing these diseases despite ongoing efforts to develop specific strategies and improve the healthcare infrastructure. Policymakers and public health experts are recommended to create context-specific policies to successfully target NCDs by acknowledging the contributing risk factors. In the context of rising urbanization and changing lifestyles, it is recommended that longitudinal research in high-burden transition neighborhoods be conducted. Public health intervention initiatives designed specifically for these densely populated cities are also required [48]. International partnerships, knowledge exchange, and evidence-based medicine can help these regions effectively prevent, diagnose, and manage NCDs, thereby improving their populations' overall health and well-being. However, further research is still needed to explore the efficacy and scalability of interventions tailored to the specific needs of each region.
Availability of data and materials
All studies reviewed are either openly accessible online or upon request from their respective authors.
References
Abdulkadri A, Floyd S, Mkrtchyan I, Marajh G, Gonzales C, Cunningham-Myrie C. Addressing the adverse impacts of non-communicable diseases on the sustainable development of Caribbean countries 2021.
Abebe F, Schneider M, Asrat B, Ambaw F. Multimorbidity of chronic non-communicable diseases in low-and middle-income countries: a scoping review. J Comorbid. 2020;10:2235042X2096191.
Aboobakur M, Latheef A, Mohamed AJ, Moosa S, Pandey RM, Krishnan A, Prabhakaran D. Surveillance for non-communicable disease risk factors in Maldives: results from the first STEPS survey in Male. Int J Public Health. 2010;55:489–96.
Adhikari B, Pokharel S, Mishra SR. Shrinking urban Greenspace and the rise in non-communicable diseases in South Asia: an urgent need for an advocacy. Front Sustain Cities. 2019;1:5.
Al-Jawaldeh A, Abbass MM. Unhealthy dietary habits and obesity: the major risk factors beyond non-communicable diseases in the eastern mediterranean region. Front Nutr. 2022;9:817808.
Allen LN, Aghilla M, Kak M, Loffreda G, Wild CEK, Hatefi A, Herbst CH, El Saeh H. Conflict as a macrodeterminant of non-communicable diseases: the experience of Libya. BMJ Glob Health. 2022;7:e007549.
Allen LN, Fox N, Ambrose A. Quantifying research output on poverty and non-communicable disease behavioural risk factors in low-income and lower middle-income countries: a bibliometric analysis. BMJ Open. 2017;7:e014715.
Almas A, Awan S, Bloomfield G, Nisar MI, Siddiqi S, Ahmed A, Ali A, Shafqat SH, Bhutta ZA, Mark DB. Opportunities and challenges to non-communicable disease (NCD) research and training in Pakistan: a qualitative study from Pakistan. BMJ Open. 2022;12:e066460.
Altajori NN, Elshrek YM. risk factors for non-communicable diseases in Libya. Egypt J Hosp Med. 2017;66:202–14.
Anauati MV, Galiani S, Weinschelbaum F. The rise of non-communicable diseases in Latin America and the Caribbean: challenges for public health policies. Latin American Econ Rev. 2015;24:1–56.
Bhandari GP, Angdembe MR, Dhimal M, Neupane S, Bhusal C. State of non-communicable diseases in Nepal. BMC Public Health. 2014;14:1–9.
Bonilla-Chacín ME. Risk factors for NCDs in Latin America and the Caribbean. Promoting Healthy Living in Latin America and the Caribbean, 2013;39.
Bonilla-Chacín ME. Non-communicable Diseases in Latin America and the Caribbean. Promoting Healthy Living in Latin America and the Caribbean, 2013;27.
Biswas T, Pervin S, Tanim MIA, Niessen L, Islam A. Bangladesh policy on prevention and control of non-communicable diseases: a policy analysis. BMC Public Health. 2017;17:1–11.
Bonilla-Chacín ME. Non-communicable diseases in Latin America and the Caribbean. Promoting Healthy Living in Latin America and the Caribbean 2013;27.
Boutata FZ, Bencharif M, Abdessemed D. Validity of four nutritional screening tools against subjective global assessment for inpatients with non communicable diseases (Algeria, 2020). Nutr Clin Métabol. 2022;36:54–8.
Boutayeb A. The double burden of communicable and non-communicable diseases in developing countries. Trans R Soc Trop Med Hyg. 2006;100:191–9. https://doi.org/10.1016/j.trstmh.2005.07.021.
Chandrasiri A, Dissanayake A, de Silva V. Health promotion in workplaces as a strategy for modification of risk factors for non communicable diseases (NCDs): a practical example from Sri Lanka. Work. 2016;55:281–4.
Dabare PRL, Wanigatunge CA, Beneragama BH. A national survey on availability, price and affordability of selected essential medicines for non communicable diseases in Sri Lanka. BMC Public Health. 2014;14:1–10.
Dalal S, Beunza JJ, Volmink J, Adebamowo C, Bajunirwe F, Njelekela M, Mozaffarian D, Fawzi W, Willett W, Adami HO, Holmes MD. Non-communicable diseases in sub-Saharan Africa: What we know now. Int J Epidemiol. 2011;40(4):885–901.
Daoud IM, Meddeb M. The role of social marketing in preventing the spread of non-communicable diseases: case of Tunisia. In: Research anthology on improving health literacy through patient communication and mass media. IGI Global, 2022;481–496.
D’Arca T, Agneta F, Branca F, Declich S, Scozzafava G, Simonetti A. Prevalence of Communicable and Non-communicable Disease in a Village of Jilib District, in the Framework of a Primary Health Care Programme. Presented at the Proceedings of the Third International Congress of Somali Studies, Il Pensiero Scientifico Editore 1988.
De Maio FG. Understanding chronic non-communicable diseases in Latin America: towards an equity-based research agenda. Glob Health. 2011;7:1–8.
Devi R, Kanitkar K, Narendhar R, Sehmi K, Subramaniam K. A narrative review of the patient journey through the lens of non-communicable diseases in low-and middle-income countries. Adv Ther. 2020;37:4808–30.
Dhawan D, Sharma S. Abdominal obesity: a stepping stone to non-communicable diseases in South Asia 2021.
Ella N, Shehab D, Ismail M. Prevalence of overweight and obesity, and status of chronic non-communicable diseases and some related risk factors among Egyptian adolescents. J Diabetes Endocrinol. 2011;2:41–52.
Elmoneer RA. Socio-Economic inequalities in accessing treatment of non-communicable diseases in Egypt using health issues survey 2015;2020.
Ezzati M, Pearson-Stuttard J, Bennett JE, Mathers CD. Acting on non-communicable diseases in low-and middle-income tropical countries. Nature. 2018;559:507–16.
Formenti B, Gregori N, Crosato V, Marchese V, Tomasoni LR, Castelli F. The impact of COVID-19 on communicable and non-communicable diseases in Africa: a narrative review. Infez Med. 2022;30:30.
Franco LM, Bennett S, Kanfer R. Health sector reform and public sector health worker motivation: a conceptual framework. Soc Sci Med. 2002;54:1255–66.
Friel S, Bowen K, Campbell-Lendrum D, Frumkin H, McMichael AJ, Rasanathan K. Climate change, non-communicable diseases, and development: the relationships and common policy opportunities. Annu Rev Public Health. 2011;32:133–47.
Gamage A, Jayawardana P. Knowledge of non-communicable diseases and practices related to healthy lifestyles among adolescents, in state schools of a selected educational division in Sri Lanka. BMC Public Health. 2018;18:1–9.
Ghaffar A, Reddy KS, Singhi M. Burden of non-communicable diseases in South Asia. BMJ. 2004;328:807–10.
Goldstein J, Jacoby E, del Aguila R, Lopez A. Poverty is a predictor of non-communicable disease among adults in Peruvian cities. Prev Med. 2005;41:800–6. https://doi.org/10.1016/j.ypmed.2005.06.001.
Gowshall M, Taylor-Robinson SD. The increasing prevalence of non-communicable diseases in low-middle income countries: the view from Malawi. Int J Gener Med. 2018;11:255–64.
Hag EM, Mustafa MH, Abdelmoneim Mukhtar B. Lifestyle patterns and the awareness of the risks of non-communicable diseases in Sudan: a community study. Sudan Med J. 2014;50:81–9.
Haldevang M de. Why do we still use the term “sub Saharan Africa” to describe things like Facebook’s Mark Zuckerberg visit to Nigeria [WWW Document] 2016. qz.com/africa. URL https://qz.com/africa/770350/why-do-we-still-say-subsaharan-africa (accessed 7.12.23).
Haregu TN, Setswe G, Elliott J, Oldenburg B. National responses to HIV/AIDS and non-communicable diseases in developing countries: analysis of strategic parallels and differences. J Public Health Res. 2014;3:jphr.2014.99.
Hassan-Kadle MA, Adani AA, Eker HH, Keles E, Muse Osman M, Mahdi Ahmed H, Görçin Karaketir Ş. Spectrum and prevalence of thyroid diseases at a tertiary referral hospital In Mogadishu, Somalia: a retrospective study of 976 cases. Int J Endocrinol. 2021;2021:1–7.
Hofman K. Non-communicable diseases in South Africa: a challenge to economic development: guest editorial. S Afr Med J. 2014;104:647.
Hospedales CJ, Samuels T, Cummings R, Gollop G, Greene E. Raising the priority of chronic non-communicable diseases in the Caribbean. Rev Panam Salud Publica. 2011;30:393–400.
Hong QN, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, Gagnon MP, Griffiths F, Nicolau B, O’Cathain A, Rousseau MC. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. 2018;34(4):285–91.
Islam SMS, Purnat TD, Phuong NTA, Mwingira U, Schacht K, Fröschl G. Non-Communicable Diseases (NCDs) in developing countries: a symposium report. Glob Health. 2014;10:1–8.
Jailobaeva K, Falconer J, Loffreda G, Arakelyan S, Witter S, Ager A. An analysis of policy and funding priorities of global actors regarding non-communicable disease in low-and middle-income countries. Glob Health. 2021;17:1–15.
Jakovljevic M, Jakab M, Gerdtham U, McDaid D, Ogura S, Varavikova E, Merrick J, Adany R, Okunade A, Getzen TE. Comparative financing analysis and political economy of non-communicable diseases. J Med Econ. 2019;22:722–7.
Kabir A, Karim MN, Billah B. Health system challenges and opportunities in organizing non-communicable diseases services delivery at primary healthcare level in Bangladesh: a qualitative study. Front Public Health. 2022;10:1015245.
Kankeu HT, Saksena P, Xu K, Evans DB. The financial burden from non-communicable diseases in low- and middle-income countries: a literature review. Health Res Policy Syst. 2013;11:31. https://doi.org/10.1186/1478-4505-11-31.
Khan FS, Lotia-Farrukh I, Khan AJ, Siddiqui ST, Sajun SZ, Malik AA, Burfat A, Arshad MH, Codlin AJ, Reininger BM. The burden of non-communicable disease in transition communities in an Asian megacity: baseline findings from a cohort study in Karachi, Pakistan. PLoS ONE. 2013;8:e56008.
Khatiwada B, Rajbhandari B, Mistry SK, Parsekar S, Yadav UN. Prevalence of and factors associated with health literacy among people with Non-communicable diseases (NCDs) in South Asian countries: a systematic review. Clin Epidemiol Global Health. 2022;18:101174. https://doi.org/10.1016/j.cegh.2022.101174.
Kuh D, Shlomo YB. A life course approach to chronic disease epidemiology. Oxford University Press; 2004.
Ligeon CM, Jolly CM, Jolly PE. Socio-economic and environmental factors influencing health status of Caribbean and Central American countries. Trop Agric. 2012;89(4):258–67.
Legetic B, Medici A, Hernández-Avila M, Alleyne GA, Hennis A. Economic dimensions of non-communicable disease in Latin America and the Caribbean. Disease control priorities. Companion volume 2016.
Maamri A, Ben El Mostafa S. The environmental health role in reducing non communicable diseases through a healthy lifestyle. Disease prevention and health promotion in developing countries 2020;39–59.
Macinko J, Andrade FC, Nunes BP, Guanais FC. Primary care and multimorbidity in six Latin American and Caribbean countries. Rev Panam Salud Publica. 2019;43:e8.
Magny-Normilus C, Hassan S, Sanders J, Longhurst C, Lee CS, Jurgens CY. Implications for self-management among African Caribbean adults with non-communicable diseases and mental health disorders: a systematic review. Biomedicines. 2022;10:2735.
Maher D, Sekajugo J, Harries A, Grosskurth H. Research needs for an improved primary care response to chronic non-communicable diseases in Africa. Tropical Med Int Health. 2010;15:176–81.
Mahmood SAI, Ali S, Islam R. Shifting from infectious diseases to non-communicable diseases: a double burden of diseases in Bangladesh. J Public Health Epidemiol. 2013;5:424–34.
Manderson L, Jewett S. Risk, lifestyle and non-communicable diseases of poverty. Glob Health. 2023;19:1–9.
Matos RA, Adams M, Sabaté J. The consumption of ultra-processed foods and non-communicable diseases in Latin America. Front Nutr. 2021;8:622714.
Matthews C. Non-communicable diseases in the Caribbean: the new challenge for productivity and growth 2013.
Mendenhall E, Kohrt BA, Norris SA, Ndetei D, Prabhakaran D. Non-communicable disease syndemics: poverty, depression, and diabetes among low-income populations. The Lancet. 2017;389:951–63.
Menon J, Vijayakumar N, Joseph JK, David PC, Menon MN, Mukundan S, Dorphy PD, Banerjee A. Below the poverty line and non-communicable diseases in Kerala: The Epidemiology of Non-communicable Diseases in Rural Areas (ENDIRA) study. Int J Cardiol. 2015;187:519–24. https://doi.org/10.1016/j.ijcard.2015.04.009.
Mensah GA. Tackling non-communicable diseases in Africa: caveat lector. Health Educ Behav. 2016;43:7S-13S.
Mirelman AJ, Rose S, Khan JA, Ahmed S, Peters DH, Niessen LW, Trujillo AJ. The relationship between non-communicable disease occurrence and poverty—evidence from demographic surveillance in Matlab, Bangladesh. Health Policy Plan. 2016;31:785–92. https://doi.org/10.1093/heapol/czv134.
Mishra SR, Neupane D, Bhandari PM, Khanal V, Kallestrup P. Burgeoning burden of non-communicable diseases in Nepal: a scoping review. Glob Health. 2015;11:1–10.
Misra A, Khurana L. Obesity-related non-communicable diseases: South Asians vs White Caucasians. Int J Obes. 2011;35:167–87.
Moussouni A, Sidi-Yakhlef A, Hamdaoui H. Socio-Demographic Determinants and Prevalence of Comorbid Hypertension and Diabetes in Algeria: Evidence from Non Communicable Disease Risk Factor Steps Survey (2016–2017). Rev: Universitara Sociologie; 2022. p. 85.
Nemchenko A, Ziad S, Kurylenko YY. Study of approaches to control of non-communicable diseases in Morocco 2022.
Neyazi N, Mosadeghrad AM, AbouZeid A. Non-communicable diseases in Afghanistan: a silent tsunami. Lancet. 2023;401:2035–6.
Neyazi N, Mosadeghrad AM, Afshari M, Isfahani P, Safi N. Strategies to tackle non-communicable diseases in Afghanistan: a scoping review. Front Public Health. 2023;11:982416.
Nishtar S. Prevention of non-communicable diseases in Pakistan: an integrated partnership-based model. Health research policy and systems. 2004;2:1–5.
Nongkynrih B, Patro B, Pandav CS. Current status of communicable and non-communicable diseases in India. Japi. 2004;52:118–23.
Noor SK, Elmadhoun WM, Bushara SO, Ahmed MH. The Changing Pattern of Hospital Admission to Medical Wards: burden of non-communicable diseases at a hospital in a developing country. Sultan Qaboos Univ Med J. 2015;15:e517.
Nugent R, Feigl A. Where have all the donors gone? Scarce donor funding for non-communicable diseases. Center for global development working paper, 2010;228.
Pengpid S, Peltzer K. Multiple behavioural risk factors of non-communicable diseases among adolescents in four Caribbean countries: prevalence and correlates. Int J Adolesc Med Health. 2021;33:305–12.
Popkin BM. Global nutrition dynamics: the world is shifting rapidly toward a diet linked with non-communicable diseases–. Am J Clin Nutr. 2006;84:289–98.
Pou SA, Tumas N, Soria DS, Ortiz P, del Pilar Díaz M. Large-scale societal factors and non-communicable diseases: Urbanization, poverty and mortality spatial patterns in Argentina. Appl Geogr. 2017;86:32–40.
PRB. Non-communicable Diseases in Latin America and the Caribbean: Youth Are Key to Prevention [WWW Document]. PRB. 2013. URL https://www.prb.org/resources/noncommunicable-diseases-in-latin-america-and-the-caribbean-youth-are-key-to-prevention/ (accessed 7.2.23).
Rawal LB, Kanda K, Biswas T, Tanim MI, Poudel P, Renzaho AM, Abdullah AS, Islam SMS, Ahmed SM. Non-communicable disease (NCD) corners in public sector health facilities in Bangladesh: a qualitative study assessing challenges and opportunities for improving NCD services at the primary healthcare level. BMJ Open. 2019;9:e029562.
Razzaghi H, Martin DN, Quesnel-Crooks S, Hong Y, Gregg E, Andall-Brereton G, Gawryszweski V, Saraiya M. 10-year trends in non-communicable disease mortality in the Caribbean region. Rev Panam Salud Publica. 2019;4:1–11.
Riaz BK, Islam MZ, Islam AS, Zaman M, Hossain MA, Rahman MM, Khanam F, Amin KB, Noor IN. Risk factors for non-communicable diseases in Bangladesh: findings of the population-based cross-sectional national survey 2018. BMJ Open. 2020;10:e041334.
Romdhane HB, Tlili F, Skhiri A, Zaman S, Phillimore P. Health system challenges of NCDs in Tunisia. Int J Public Health. 2015;60:39–46.
Samuels TA, Guell C, Legetic B, Unwin N. Policy initiatives, culture and the prevention and control of chronic non-communicable diseases (NCDs) in the Caribbean. Ethn Health. 2012;17:631–49.
Schneider M, Bradshaw D, Steyn K, Norman R, Laubscher R. Poverty and non-communicable diseases in South Africa. Scand J Public Health. 2009;37:176–86.
Siegel KR, Patel SA, Ali MK. Non-communicable diseases in South Asia: contemporary perspectives. Br Med Bull. 2014;111:31–44.
Sithey G, Li M, Thow AM. Strengthening non-communicable disease policy with lessons from Bhutan: linking gross national happiness and health policy action. J Public Health Policy. 2018;39:327–42.
Tamang M, Dahal BP, Dorji T, Tamang ST, Lucero-Prisno DE. Situation of physical activity in the prevention of non-communicable diseases in Bhutan: challenges and the way forward. BMJ Open Sport Exerc Med. 2022;8:e001448.
Thakur J, Garg R, Narain J, Menabde N. Tobacco use: a major risk factor for non communicable diseases in South-East Asia region. Indian J Public Health. 2011;55:155–60.
Upadhyay RP. An overview of the burden of non-communicable diseases in India. Iran J Public Health. 2012;41:1.
Wagner K-H, Brath H. A global view on the development of non communicable diseases. Prev Med. 2012;54:S38–41. https://doi.org/10.1016/j.ypmed.2011.11.012.
WHO. Non communicable diseases [WWW Document]. URL https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed 7.2.23) 2022a.
WHO. Deaths from non-communicable diseases on the rise in Africa [WWW Document]. WHO | Regional Office for Africa. URL https://www.afro.who.int/news/deaths-noncommunicable-diseases-rise-africa (accessed 7.2.23) 2022b.
World Health Organization. WHO country co-operation strategy at a glance: Djibouti. World Health Organization 2014.
Zafar M, Malik MA. Emerging challenges and health system capacity: the case of non-communicable diseases in Pakistan; a review. J Infect Dis Ther. 2014;2:2332.
Zhang YB, Pan XF, Chen J, Cao A, Xia L, Zhang Y, Wang J, Li H, Liu G, Pan A. Combined lifestyle factors, all-cause mortality and cardiovascular disease: a systematic review and meta-analysis of prospective cohort studies. J Epidemiol Community Health. 2021;75(1):92–9.
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Contributions
Conceptualization: MAB Literature search and study selection: MAB Data collection and interpretation: MAB, NG, SC Quality assessment: MAB, NG, SC Drafting of the Manuscript: MAB, NG Critical Review of the Manuscript: MAB, NG, SC Supervision: SC All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This paper was not considered to require ethical approval as it does not include human or animal trial activities and it used published secondary data.
Competing interests
All co-authors declare no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Bhuiyan, M.A., Galdes, N., Cuschieri, S. et al. A comparative systematic review of risk factors, prevalence, and challenges contributing to non-communicable diseases in South Asia, Africa, and Caribbeans. J Health Popul Nutr 43, 140 (2024). https://doi.org/10.1186/s41043-024-00607-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41043-024-00607-2