
Abstract
Background
The COVID-19 pandemic and the consequences of safety measures, such as lockdowns, have impacted not only the physical health of individuals but also their lifestyle, psychosocial health, and mental health. In this analysis, we aimed to explore the effect of the COVID-19 pandemic on lifestyle, eating habits, and sleep quality in the Palestinian population. Furthermore, the current study aimed to determine the factors associated with poor sleep.
Methods
The study was carried out between November 2021 and February 2022 after a long lockdown. We adopted a cross-sectional design to achieve the objectives of this study. The questionnaire included information on sociodemographic characteristics and other characteristics. In addition, questions related to lifestyle changes and items related to changes in the consumption of certain types of food were included. Furthermore, in the present study, two scales were used to assess sleep quality: the Epworth Sleepiness Scale (ESS) and the Pittsburgh Sleep Quality Index (PSQI).
Results
A total of 978 participants were included in this study; 508 (51.9%) were women, and 465 (47.5%) were aged between 17 and 30 years. 41% of the participants added one meal or more, and almost 43% skipped one meal or more. A total of 39.2% believed that their habits worsened as a result of the COVID-19 pandemic. A significant portion of the population increased their vitamin intake by 62.5%. In general, nuts, fast food, fried food, coffee, snacks, cans, and homemade baked foods were consumed at higher rates overall. The median ESS score, which measures general levels of daytime drowsiness, was 20.00 (18.00–22.00). Residency (p = 0.008), living status (p < 0.001), salary (p < 0.001), education level (p = 0.002), job status (p = 0.015), and vitamin intake (p < 0.001) were significantly associated with the ESS score. The PSQI score, which evaluates adult sleep patterns and quality, has a median value of 5.00. (4.00–7.00). Living status (p < 0.001), salary (p = 0.006), job status (p = 0.002), smoking status (p = 0.030), chronic diseases (p = 0.002), and vitamin use (p < 0.001) were significantly associated with the PSQI score. Only taking multivitamins was a predictor of having a lower score on both the ESS (p = 0.001) and PSQI (p < 0.001).
Conclusions
Our findings clearly showed that the COVID-19 pandemic has substantially affected the Palestinian population in different aspects of life. We recommend that health authorities and healthcare providers continually share knowledge and awareness about good eating habits, sleep quality, and other aspects of lifestyles.
Similar content being viewed by others


Background
Severe acute respiratory syndrome known as coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome 2 (SARS-CoV-2), emerged in 2019 and was first identified in China [1]. On 20 September 2022, the COVID-19 crisis resulted in 614.803 million cases; among these, 6.532 million died [2]. The COVID-19 pandemic and the consequences of safety measures, such as lockdown, have impacted not only the physical health of individuals but also their lifestyle, psychosocial health, and mental health [3,4,5].
In fact, COVID-19 has affected many aspects of individuals’ lives, as most people work from home with little contact with their colleagues and friends. These may have negative impacts on physical activity and eating habits [6]. Unfortunately, unhealthy eating habits can affect human health by preventing COVID-19 infection, and having balanced and healthy nutritional status is vital for the immune system [7, 8]. Furthermore, obesity may be a consequence of unhealthy eating habits, and this population is at high risk for complications from COVID-19 [9].
On the other hand, sleep quality is strongly affected by this pandemic [10]. In a recent meta-analysis, sleep disturbances (42.49%) during lockdown were more common than those without lockdown, and adolescents, children, and infected individuals were the most common category [10]. Furthermore, a study recommends monitoring sleep quality during the COVID-19 crisis, especially in older individuals [11], as poor sleep may decrease the immune response to antigens [12]. In addition, the COVID-19 crisis can affect the population’s emotional status and may eventually disturb sleep quality [13].
Many publications were conducted to assess lifestyle changes that occurred during and after the lockdown, and they found notable changes in eating habits, body weight, sleeping patterns, and physical activity [7, 14,15,16,17,18,19,20,21,22,23]. However, each country has a unique modality for handling such a pandemic and, subsequently, a significant effect on the population. Therefore, our objective was to evaluate these changes in Palestine. As of September 20, 2022, there were 620,548 cumulative cases of COVID-19, with 5,403 deaths [24]. In this analysis, we aimed to explore the effect of the COVID-19 pandemic on lifestyle, eating habits, and sleep quality in the Palestinian population. Furthermore, the current study aimed to determine the factors associated with poor sleep. The findings of this study will provide important information for nutritionists, psychosocial specialists, and regulatory authorities to best handle such a pandemic, taking into account all aspects of human life.
Methods
Study design
The study was carried out between November 2021 and February 2022 after a long lockdown and aimed to explore eating habits and lifestyle changes during the COVID-19 pandemic, in addition to evaluating the current sleeping patterns of the Palestinian population. We adopted a cross-sectional design to achieve the objectives of this study. In September 2021, approximately 2,000 cases of COVID-19 were documented per day in Palestine.
Study population
The study was carried out in northern Palestine (Nablus, Jenin, Tubbas, Tulkarem, and Qalqilyia).
Sample size and sampling procedure
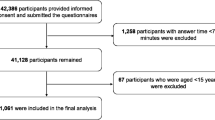
Three medical students collected data through face-to-face interviews using nonrandom selection and taking all safety measures against COVID-19. The sample size was 978 participants. It was collected in public places and sectors.
Inclusion and exclusion criteria
All Palestinians who were 18 years or older and agreed to participate after providing verbal informed consent were willing to participate. However, we excluded participants from other parts of Palestine and those who did not complete the questionnaire.
Data collection instrument
The questionnaire included information on sociodemographic characteristics and other characteristics. In addition, questions related to lifestyle changes and items related to changes in the consumption of certain types of food were included.
Furthermore, the current analysis used two scales to assess sleep quality. First, the Epworth Sleepiness Scale (ESS) assesses general daytime sleepiness levels. The respondent is asked to rate how likely they are to fall asleep while participating in eight typical everyday activities to establish their level of daytime sleepiness, where the possible ESS values, which are the average of the eight item scores (0–3), are 0–24. A person’s average sleep propensity, often known as “daytime sleepiness,” or “ASP,” increases with increasing ESS score. In addition, a score > 10 on the ESS indicates excessive daytime sleepiness (EDS). An ESS score of 16 or higher indicates a high level of EDS. Scores in this range typically indicate significant sleep disorders, such as narcolepsy. Additionally, the ESS is a reliable and valid score [25,26,27].
Second, Buysse and colleagues established the Pittsburgh Sleep Quality Index (PSQI) as a score to evaluate the quality and pattern of adult sleep. The following seven domains (components) were measured to distinguish between “poor” and “good” sleep quality: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disruptions, use of sleeping drugs, and daytime dysfunction during the previous month. The authors recommend that a score of 5 or higher be considered a significant sleep disturbance [28]. The scores range from 0 to 21. Furthermore, the Arabic version of the NRS-2002 is valid and reliable [29]. We used previously translated and validated Arabic versions of the PSQI [29], and ESS [30] with permission.
Ethical issues
The study was approved by the Institutional Review Board (IRB) of An-Najah National University (approval number: Med. July 2021/3). We discussed the study’s objectives and all other aspects with the participants, in addition to ensuring their confidentiality and privacy. After that, we obtained informed verbal consent to participate in the survey.
Statistical analysis
All the data were analyzed using the Statistical Package for Social Sciences version 21 (IBM-SPSS 21). Frequencies, percentages, means ± standard deviations, and medians (Q1-Q3) were used to present the data. In addition, two nonparametric tests (the Mann‒Whitney U test and Kruskal–Wallis test) were applied to explore differences in median sleep quality scores between groups. For variables with significant univariate p values, multiple linear regression analysis was performed to determine the predictors of poor sleep quality. A value of less than 0.05 was considered to indicate statistical significance.
Results
Characteristics of the sample
A total of 978 participants were included in this study. There were 508 (51.9%) women, 465 (47.5%) were aged between 17 and 30 years, most of the participants were single, 456 (46.6%), 10.2% reported having no jobs, 44.8% were uneducated, and 24.2% reported having chronic diseases. More details on the demographic characteristics are shown in Table 1.
Number of meals
Regarding the number of meals consumed during the COVID-19 crisis, 41% of the participants added one meal or more, almost 43% skipped one meal or more, and the remaining population (16.3%) reported no changes in the number of meals.
Lifestyle changes
Regarding lifestyle changes during the COVID-19 lockdown, most of the population (52%) declared not having changed their habits, while 39.2% and 8.8% believed that their habits had worsened or improved due to the COVID-19 pandemic, respectively.
The results indicate that during the COVID-19 lockdown, 831 people (85.0%) had no difficulty getting food, while only 15% had trouble. Regarding the consumption of vitamins and supplements, a significant portion of the population increased their vitamin intake by 62.5%, while the others (37.5%) did not take any vitamins during the crisis.
Changes in food consumption
Data during the COVID-19 crisis revealed variations in food consumption, as shown in Table 2. In general, nuts, fast food, fried food, coffee, snacks, cans, and homemade baked foods were consumed at higher rates overall. Regarding the intake of fried foods, most participants (56.2%) increased their consumption. The majority of the population consumed nuts, snacks, cans and coffee, accounting for 52.1%, 41.2%, 48.6%, and 42.6%, respectively, while 24.7%, 21.3%, 19.2%, and 22.9%, respectively, of the population reported no changes in their consumption. Furthermore, as shown, food consumption, such as corn flakes (33.1%), chicken (32.5%), salty food (31.1%), candy (32.1%), soft drinks (30.1%) and ice cream (34.5%), decreased during the pandemic.
Sample characteristics according to the ESS and PSQI scales
The median ESS score, which measures general levels of daytime drowsiness, was 20.00 (18.00–22.00), as indicated in Tables 1 and 3. In relation to patient characteristics, living situation exhibited a significant association, with a p value of < 0.001. Individuals who resided in village areas had a higher median than others. Additionally, a noteworthy proportion of the population with a salary of less than 2000 had a median of 22.00 (19.00–26.00), which was higher than that of individuals earning 2000 or more. Concerning city status and salary, both factors demonstrated significant p values of 0.008 and < 0.001, respectively. The majority of participants (n = 611) who consumed vitamins and supplements during the COVID-19 crisis had a significantly lower median score than did those who did not take multivitamins (p value < 0.001). Furthermore, the effect of education was statistically significant (p value = 0.002), with the medians for individuals without education, with only a high school diploma, with undergraduate students, and with graduates being 20.00 (19.00–22.00), 23.00 (19.00-27.75), 20.00 (18.00–23.00) and 21.00 (19.00–23.00), respectively. Concerning job status, the highest ESS score was found for unemployed persons, 22.00 (18.25-26.00), and the association was statistically significant (p value = 0.015).
The PSQI score, which evaluates adult sleep patterns and quality, has a median value of 5.00 (4.00–7.00). Salary and living conditions were statistically significant (p values of 0.006 and < 0.001, respectively). Notably, people who lived in rural areas had higher PSQI scores than individuals who lived in cities or camps. Furthermore, unemployment status was associated with a significantly greater PSQI score than was other job statuses (p value = 0.002). The analysis of other sociodemographic data revealed that individuals who did not take vitamins during the crisis had a median of 5.00 (4.00–7.00) and a mean rank of 532.29, which was greater than that of individuals who took multivitamins (463.80). This finding was statistically significant, as indicated by a p value < 0.001. Additionally, participants who had chronic diseases had significantly greater PSQI scores than individuals without chronic conditions (p value = 0.002). Furthermore, smoking status was significantly associated with the PSQI score (p value = 0.030), where smokers had a higher score than nonsmokers did.
Only taking multivitamins was a predictor of having a lower score on both the ESS (p = 0.001) and PSQI (p < 0.001) (Tables 4 and 5).
Discussion
Healthy behaviors and lifestyles must be encouraged among communities, especially during and after the COVID-19 pandemic. Evidence from China and from around the world shows that these populations are at increased risk of complications and are more susceptible to developing severe conditions [31,32,33,34,35]. Furthermore, the COVID-19 pandemic has negatively affected quality of life and mental health [36,37,38,39].
The results of our study revealed variations in food consumption during the COVID-19 crisis, during which the majority of participants (56.2%) increased their consumption of fried food. More people consumed nuts, snacks, cans, and coffee, whereas approximately one-fourth of the population reported no changes in their consumption. These results were expected due to the total lockdown at the beginning of the crisis. Our team anticipated a possible increase in the consumption of such snacks, which is similar to results reported in different regions of the world [37,38,39]. Furthermore, the consumption of food, such as corn flakes, chicken, salty food, candy, soft drinks, and ice cream, decreased during the pandemic. In parallel to this study, the National Institute of Public Health in Mexico evaluated dietary behaviors during the COVID-19 lockdown. There were higher percentages of cereal, legume, coffee, sweetet, sweetened beverage, and snack consumption among the participants [40].
Unlike this study, another study conducted in Mexico expected to have similar results with more consumption of snakes; however, the results showed a decrease in consuming sweets, sweetened beverages, snacks, and pastries among 40% of Mexican households compared to home maid food [41]. On the other hand, another study in France reported a reduction in fresh food consumption and increased consumption of sugar-containing foods [42].
In Spain, food consumption was also assessed during the pandemic, and participants reported higher rates of consumption of fruits, vegetables, and olives (Mediterranean diet), which contain vitamins and antioxidants that play a crucial role in supporting the immune system [43].
Regarding lifestyle changes, most of the population (52%) declared that they had not changed their habits, while 39.2% believed that their habits worsened with an increase in sedentary behavior due to the COVID-19 pandemic and the lockdown period. Our findings are similar to the results of studies from other countries around the world, including the United States, Mexico, Italy, Spain, Poland, Cheli, France and China, which all reported that lifestyle and physical activity were negatively affected by COVID-19 [7, 40, 43,44,45,46]. These lifestyle changes were expected and explained to be due to the lockdown period involving new excess home activities during confinement, such as homeschooling, working from home and less access to gyms and sports places.
Interest in vitamin consumption as a supplement was also noted in this study, which was anticipated to be due to individuals’ belief about vitamin use as a way to improve immunity. Our results are consistent with results observed worldwide that support the idea of using immune-related compounds and dietary supplements such as vitamins, minerals and amino acids to help in the prevention or treatment of COVID-19. Studies have shown that these practices may be due to advertisements about the benefit of the use of dietary supplements and the high interest of the community in understanding and reading about COVID-19 and its treatment in Europe and worldwide. Moreover, a study conducted in Poland using Google Forms agreed with our study results on the high consumption of dietary supplements among society during the COVID-19 pandemic [47,48,49]. We found that taking multivitamins is a predictor of sleep quality. This could be explained by the fact that certain vitamins, such as magnesium, vitamin D, and vitamin B12, may help improve sleep quality [50,51,52].
Sleep disturbances during the COVID-19 pandemic were also assessed in our study using the PSQI score, which evaluates adult sleep patterns and quality and has a median value of 5.00, indicating significant sleep disturbance. Similarly, a meta-analysis of 139 studies in different countries around the world evaluated sleep patterns, and the most commonly used scale for sleep quality was the PSQI. The general mean global PSQI score was 6.73, indicating poor sleep quality. The USA, Canada and Brazil had higher levels of insomnia and poorer sleep quality than Asia did, which was likely due to the higher mortality rate among COVID-19 patients and the more severe pandemic situation in these regions of the world, which eventually caused higher levels of stress and anxiety among individuals, leading to poor sleep quality [42, 43]. The characteristics of the subjects were evaluated and found to be correlated with sleep patterns. The majority of the population with chronic diseases had a median of 6.00. This was expected, as individuals with comorbidities are at high risk for severe COVID-19, and complications increase susceptibility to stress, insomnia and poor sleep patterns [42, 43].
Several studies have similarly assessed sleep quality during the COVID-19 pandemic and reported a correlation with psychological problems such as stress, anxiety, and depression, especially during the lockdown period. In addition, studies in the U.S. found significant sleep impairment and higher insomnia scores, which could be due to a more critical pandemic condition leading to a greater level of stress that can affect sleep quality [28, 53].
Furthermore, the results of our study showed that the median ESS score, which measures general levels of drowsiness at night, was 20.00, indicating excessive daytime sleepiness and was significantly associated with patient characteristics, such as living situation, city status, salary, degree of education, and employment status. Therefore, the sedentary lifestyle of the population experienced during the lockdown period could explain these results, especially for door workers and students, which was similarly mentioned in other studies around the world [42, 44, 45].
A related study in Italy reported that 8% of physicians who worked during the COVID-19 pandemic had an ESS of more than 10, suggesting excessive sleepiness during the day [54]. Furthermore, compared with those in the population in our study, only 6% of healthcare workers reported high ESS scores in another study, which is expected since healthcare workers had excessive work hours, loads, and tasks during the COVID-19 pandemic [55].
Additionally, the PSQI and ESS scores were significantly greater among respondents living in villages than among those living in cities and camps. The reason for this difference may be the shorter duration of sleep among the rural population than among the city and camp populations and the different lifestyles, as people in these villages used to have active lifestyles, which was strongly affected by the lockdown and COVID-19 pandemic. These findings are similar to the results reported by a study conducted in urban and rural areas situated in the Parganas district [56].
Higher scores and poor sleep quality were also correlated with employment status, and respondents who were unemployed had significantly higher scores than students and employed respondents. These findings agree with those of studies in the UK and Greece, which could be explained by the lower income of unemployed individuals, which eventually affects living standards and increases susceptibility to sleep disturbances due to stress and anxiety [57,58,59].
Strengths and limitations
The current study was carried out among a large number of participants, and to the best of our knowledge, this is the first study of this topic in Palestine. However, a ccross-sectional design, convenient sampling, and the exclusion of other parts of Palestine are the main limitations of our study, which affect the generalization of the current findings to the Palestinian population. In addition, the current study did not identify an association between lifestyle changes and BMI or sleep quality due to the absence of data on these variables before the onset of the COVID-19 crisis.
Conclusions and recommendations
Our findings showed that the COVID-19 pandemic has substantially impacted the Palestinian population in different aspects of life. Importantly, almost half of the population has increased their consumption of fast and fried foods, which requires healthcare professionals to focus on this issue. Additionally, unemployed people had poor sleep quality compared to other populations. It is crucial to encourage the population to improve their healthy lifestyle behaviors during the COVID-19 crisis to prevent any risk of chronic diseases or complications. Unfortunately, the lack of specialized programs that educate the general population to improve their lifestyle and health is one of the main challenges during and after the COVID-19 pandemic. Therefore, we recommend that health authorities and healthcare providers continuously share knowledge and awareness of good eating habits, sleep quality, and lifestyles.
Data availability
Due to privacy, the data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- COVID-19:
-
Coronavirus disease 2019
- ESS:
-
Epworth Sleepiness Scale
- PSQI:
-
Pittsburgh Sleep Quality Index
- EDS:
-
Excessive daytime sleepiness
- IRB:
-
Institutional Review Board
- SPSS:
-
Statistical Package for Social Sciences
References
Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020;395(10223):470–3.
Worldometer. COVID-19 Coronavirus Pandemic. 2022. https://www.worldometers.info/coronavirus/ (accessed September 20 2022).
Dubey S, Biswas P, Ghosh R, Chatterjee S, Dubey MJ, Chatterjee S, Lahiri D, Lavie CJ. Psychosocial impact of COVID-19. Diabetes Metab Syndr. 2020;14(5):779–88.
Atalan A. Is the lockdown important to prevent the COVID-19 pandemic? Effects on psychology, environment and economy-perspective. Ann Med Surg (Lond). 2020;56:38–42.
Wang C, Pan R, Wan X, Tan Y, Xu L, McIntyre RS, Choo FN, Tran B, Ho R, Sharma VK, et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav Immun. 2020;87:40–8.
Ammar A, Brach M, Trabelsi K, Chtourou H, Boukhris O, Masmoudi L, Bouaziz B, Bentlage E, How D, Ahmed M et al. Effects of COVID-19 Home Confinement on eating Behaviour and physical activity: results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12(6).
Di Renzo L, Gualtieri P, Pivari F, Soldati L, Attinà A, Cinelli G, Leggeri C, Caparello G, Barrea L, Scerbo F, et al. Eating habits and lifestyle changes during COVID-19 lockdown: an Italian survey. J Transl Med. 2020;18(1):229.
Zyoud SH, Al-Jabi SW, Koni A, Shakhshir M, Shahwan M, Jairoun AA. Mapping the landscape and structure of global research on nutrition and COVID-19: visualization analysis. J Health Popul Nutr. 2022;41(1):25.
Centers for Disease Control and Prevention, Obesity R, Ethnicity, and COVID-19. 2022. https://www.cdc.gov/obesity/data/obesity-and-covid-19.html#:~:text=Obesity%20Worsens%20Outcomes%20from%20COVID%2D19&text=People%20who%20are%20overweight%20may,linked%20to%20impaired%20immune%20function.&text=Obesity%20decreases%20lung%20capacity%20and%20reserve%20and%20can%20make%20ventilation%20more%20difficult. (accessed September 20 2022).
Jahrami HA, Alhaj OA, Humood AM, Alenezi AF, Fekih-Romdhane F, AlRasheed MM, Saif ZQ, Bragazzi NL, Pandi-Perumal SR, BaHammam AS, et al. Sleep disturbances during the COVID-19 pandemic: a systematic review, meta-analysis, and meta-regression. Sleep Med Rev. 2022;62:101591.
Cha EJ, Jeon HJ. The effect of COVID-19 pandemic on sleep-related problems in adults and elderly citizens: an infodemiology study using relative search volume data. PLoS ONE. 2022;17(7):e0271059.
Besedovsky L, Lange T, Born J. Sleep and immune function. Pflugers Arch. 2012;463(1):121–37.
Partinen M, Holzinger B, Morin CM, Espie C, Chung F, Penzel T, Benedict C, Bolstad CJ, Cedernaes J, Chan RNY, et al. Sleep and daytime problems during the COVID-19 pandemic and effects of coronavirus infection, confinement and financial suffering: a multinational survey using a harmonised questionnaire. BMJ Open. 2021;11(12):e050672.
Catucci A, Scognamiglio U, Rossi L. Lifestyle changes related to eating habits, physical activity, and Weight Status during COVID-19 Quarantine in Italy and some European Countries. Front Nutr. 2021;8:718877.
Gür M. Post-pandemic lifestyle changes and their interaction with resident behavior in housing and neighborhoods: Bursa, Turkey. J Hous Built Environ. 2022;37(2):823–62.
Samanta S, Banerjee J, Rahaman SN, Ali KM, Ahmed R, Giri B, Pal A, Dash SK. Alteration of dietary habits and lifestyle pattern during COVID-19 pandemic associated lockdown: an online survey study. Clin Nutr ESPEN. 2022;48:234–46.
Fujii H, Nakamura N, Fukumoto S, Kimura T, Nakano A, Nadatani Y, Tauchi Y, Nishii Y, Takashima S, Kamada Y, et al. Lifestyle changes during the coronavirus disease 2019 pandemic impact metabolic dysfunction-associated fatty liver disease. Liver Int. 2022;42(5):995–1004.
Madan J, Blonquist T, Rao E, Marwaha A, Mehra J, Bharti R, Sharma N, Samaddar R, Pandey S, Mah E et al. Effect of COVID-19 Pandemic-Induced Dietary and Lifestyle Changes and Their Associations with Perceived Health Status and Self-Reported Body Weight Changes in India: A Cross-Sectional Survey. Nutrients 2021, 13(11).
Singh B, Jain S, Rastogi A. Effects of nationwide COVID-19 lockdown on lifestyle and diet: an Indian survey. J Family Med Prim Care. 2021;10(3):1246–50.
Cervera-Martínez J, Atienza-Carbonell B, Mota JC, Bobes-Bascarán T, Crespo-Facorro B, Esteban C, García-Portilla MP, Gomes-da-Costa S, González-Pinto A, Jaén-Moreno MJ, et al. Lifestyle changes and mental health during the COVID-19 pandemic: a repeated, cross-sectional web survey. J Affect Disord. 2021;295:173–82.
van der Werf ET, Busch M, Jong MC, Hoenders HJR. Lifestyle changes during the first wave of the COVID-19 pandemic: a cross-sectional survey in the Netherlands. BMC Public Health. 2021;21(1):1226.
Kifle ZD, Woldeyohanins AE, Asmare B, Atanaw B, Mesafint T, Adugna M. Assessment of lifestyle changes during coronavirus disease 2019 pandemic in Gondar town, Northwest Ethiopia. PLoS ONE. 2022;17(3):e0264617.
Li X, Li J, Qing P, Hu W. COVID-19 and the change in Lifestyle: Bodyweight, Time Allocation, and Food choices. Int J Environ Res Public Health 2021, 18(19).
Worldometer. Total coronavirus cases in the State of Palestine. 2022. https://www.worldometers.info/coronavirus/country/state-of-palestine/ (accessed September 20 2022).
Bonzelaar LB, Salapatas AM, Yang J, Friedman M. Validity of the epworth sleepiness scale as a screening tool for obstructive sleep apnea. Laryngoscope. 2017;127(2):525–31.
Izci B, Ardic S, Firat H, Sahin A, Altinors M, Karacan I. Reliability and validity studies of the Turkish version of the Epworth Sleepiness Scale. Sleep Breath. 2008;12(2):161–8.
Alami YZ, Ghanim BT, Zyoud SH. Epworth sleepiness scale in medical residents: quality of sleep and its relationship to quality of life. J Occup Med Toxicol. 2018;13:21.
Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213.
Suleiman KH, Yates BC, Berger AM, Pozehl B, Meza J. Translating the Pittsburgh Sleep Quality Index into Arabic. West J Nurs Res. 2010;32(2):250–68.
Ahmed AE, Fatani A, Al-Harbi A, Al-Shimemeri A, Ali YZ, Baharoon S, Al-Jahdali H. Validation of the arabic version of the Epworth sleepiness scale. J Epidemiol Glob Health. 2014;4(4):297–302.
Zheng Z, Peng F, Xu B, Zhao J, Liu H, Peng J, Li Q, Jiang C, Zhou Y, Liu S, et al. Risk factors of critical & mortal COVID-19 cases: a systematic literature review and meta-analysis. J Infect. 2020;81(2):e16–25.
Tang N, Li D, Wang X, Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost. 2020;18(4):844–7.
Shi Y, Yu X, Zhao H, Wang H, Zhao R, Sheng J. Host susceptibility to severe COVID-19 and establishment of a host risk score: findings of 487 cases outside Wuhan. Crit Care. 2020;24(1):1–4.
Tian S, Hu N, Lou J, Chen K, Kang X, Xiang Z, Chen H, Wang D, Liu N, Liu D. Characteristics of COVID-19 infection in Beijing. J Infect. 2020;80(4):401–6.
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506.
Caroppo E, Mazza M, Janiri D, Moccia L, Janiri L, Sani G, Marano G, Avallone C, Claro AE, Sannella A. Will nothing be the same again? Changes in Lifestyle during COVID-19 pandemic and consequences on Mental Health. Int J Environ Res Public Health 2021, 18(16).
Mariani R, Renzi A, Di Monte C, Petrovska E, Di Trani M. The impact of the COVID-19 pandemic on primary emotional systems and emotional regulation. Int J Environ Res Public Health. 2021;18(11):5742.
Yıldız E. What can be said about lifestyle and psychosocial issues during the coronavirus disease pandemic? first impressions. Perspectives in psychiatric care 2020.
Caroppo E, Mazza M, Sannella A, Marano G, Avallone C, Claro AE, Janiri D, Moccia L, Janiri L, Sani G. Will nothing be the same again? Changes in lifestyle during COVID-19 pandemic and consequences on mental health. Int J Environ Res Public Health. 2021;18(16):8433.
Martínez-Vázquez SE, Ceballos-Rasgado M, Posada-Velázquez R, Hunot-Alexander C, Nava-González EJ, Ramírez-Silva I, Aguilar-López DK, Quiroz-Olguín G, López-Jara B et al. Delgado-de-la-Cruz C : Perceived Diet Quality, Eating Behaviour, and Lifestyle Changes in a Mexican Population with Internet Access during Confinement for the COVID-19 Pandemic: ESCAN-COVID19Mx Survey. Nutrients 2021, 13(12):4256.
Rodríguez-Ramírez S, Gaona-Pineda EB, Martínez-Tapia B, Romero-Martínez M, Mundo-Rosas V, Shamah-Levy T. [Not available]. Salud Publica Mex. 2021;63(6):763–72.
Deschasaux-Tanguy M, Druesne-Pecollo N, Esseddik Y, de Edelenyi FS, Allès B, Andreeva VA, Baudry J, Charreire H, Deschamps V, Egnell M, et al. Diet and physical activity during the coronavirus disease 2019 (COVID-19) lockdown (March-May 2020): results from the French NutriNet-Santé cohort study. Am J Clin Nutr. 2021;113(4):924–38.
Rodríguez-Pérez C, Molina-Montes E, Verardo V, Artacho R, García-Villanova B, Guerra-Hernández EJ. Ruíz-López MD: changes in Dietary Behaviours during the COVID-19 outbreak confinement in the Spanish COVIDiet Study. Nutrients. 2020;12(6):1730.
Navarro-Cruz AR, Kammar-García A, Mancilla-Galindo J, Quezada-Figueroa G, Segura-Badilla O, Tlalpa-Prisco M, Vera-López O, Aguilar-Alonso P, Lazcano-Hernández M. Association of Differences in Dietary Behaviours and Lifestyle with Self-Reported Weight Gain during the COVID-19 Lockdown in a University Community from Chile: A Cross-Sectional Study. Nutrients 2021, 13(9).
Sidor A, Rzymski P. Dietary choices and habits during COVID-19 Lockdown: experience from Poland. Nutrients 2020, 12(6).
Mallan KM, Fildes A, de la Piedad Garcia X, Drzezdzon J, Sampson M, Llewellyn C. Appetitive traits associated with higher and lower body mass index: evaluating the validity of the adult eating behaviour questionnaire in an Australian sample. Int J Behav Nutr Phys Act. 2017;14(1):130.
Hamulka J, Jeruszka-Bielak M, Górnicka M, Drywień ME, Zielinska-Pukos MA. Dietary supplements during COVID-19 outbreak. Results of Google trends Analysis supported by PLifeCOVID-19 Online studies. Nutrients. 2020;13(1):54.
Kamiński M, Kręgielska-Narożna M, Bogdański P. Determination of the popularity of Dietary supplements using Google search rankings. Nutrients 2020, 12(4).
Mayasari NR, Ho DKN, Lundy DJ, Skalny AV, Tinkov AA, Teng IC, Wu MC, Faradina A, Mohammed AZM, Park JM et al. Impacts of the COVID-19 pandemic on Food Security and Diet-related lifestyle behaviors: an Analytical Study of Google trends-based query volumes. Nutrients 2020, 12(10).
Mirzaei-Azandaryani Z, Abdolalipour S, Mirghafourvand M. The effect of vitamin D on sleep quality: a systematic review and meta-analysis. Nutr Health. 2022;28(4):515–26.
García-García C, Baik I. Effects of poly-gamma-glutamic acid and vitamin B(6) supplements on sleep status: a randomized intervention study. Nutr Res Pract. 2021;15(3):309–18.
Arab A, Rafie N, Amani R, Shirani F. The role of Magnesium in Sleep Health: a systematic review of available literature. Biol Trace Elem Res. 2023;201(1):121–8.
Ballesio A, Zagaria A, Musetti A, Lenzo V, Palagini L, Quattropani MC, Vegni E, Bonazza F, Filosa M, Manari T et al. Longitudinal associations between stress and sleep disturbances during COVID-19. Stress Health 2022.
Parra Serrano HSMA, Diaz Cambriles J, Arias Arias T, Muñoz Méndez EM. Del Yerro Álvarez MJ, González Sánchez M: sleep characteristics in health workers exposed to the COVID-19 pandemic. Sleep Med. 2020;75:388–94.
Costa C, Teodoro M, Briguglio G, Vitale E, Giambò F, Indelicato G, Micali E, Italia S, Fenga C. Sleep Quality and Mood State in Resident Physicians during COVID-19 pandemic. Int J Environ Res Public Health 2021, 18(15).
Mondal H, Mondal S, Baidya C. Comparison of Perceived Sleep Quality among Urban and Rural Adult Population by Bengali Pittsburgh Sleep Quality Index. Adv Hum Biology. 2018;8(1):36–40.
Wright L, Steptoe A, Fancourt D. Are adversities and worries during the COVID-19 pandemic related to sleep quality? Longitudinal analyses of 46,000 UK adults. PLoS ONE. 2021;16(3):e0248919.
Wanberg C, Basbug G, Van Hooft EA, Samtani A. Navigating the black hole: explicating layers of job search context and adaptational responses. Pers Psychol. 2012;65(4):887–926.
Wanberg CR, Zhu J, Kanfer R, Zhang Z. After the pink slip: applying dynamic motivation frameworks to the job search experience. Acad Manag J. 2012;55(2):261–84.
Acknowledgements
We would like to thank Marah Hunjul, Haroun Neiroukh, and Yazan Giacaman for helping with the data collection.
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Contributions
AAK designed the study, performed the statistical analysis, wrote the manuscript, and supervised the team. IHH, SH, and HKJ collected the data and participated in the study design. MAN and ASA interpreted the results and participated in manuscript writing. SHZ conceptualized and designed the study and revised the manuscript critically for enhancement of intellectual content.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Institutional Review Board (IRB) of An-Najah National University (approval number: Med. July 2021/3). We discussed the objectives of the study and all other aspects with the participants, in addition to ensuring their confidentiality and privacy. After that, we obtained informed verbal consent to participate in the survey. The IRB of An-Najah National University approved only verbal consent. Because we did not collect any identification data during the interviews and our research did not pose a major risk to patients, the IRB of An-Najah National University waived the requirement for written informed consent. The researchers confirmed that all the methods followed the relevant regulations and guidelines.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Koni, A.A., Hasan, I., Nazzal, M.A. et al. Eating habits, sleep quality, and lifestyle changes during the COVID-19 crisis: a national survey from Palestine. transl med commun 9, 11 (2024). https://doi.org/10.1186/s41231-024-00171-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41231-024-00171-1