
Abstract
Background
Aneuploidy is one of the most important chromosomal aberrations, which involves an abnormal number of the chromosomes. Trisomy 21 (Down syndrome) and numerical aberrations of the sex chromosomes have a relatively high prevalence in the general population. However, the patients usually have one of the above genetic disorders and combined cases of two different trisomies are unusual.
Case presentation
We report a case of a patient with double aneuploidy—a combination of trisomy 21 and triple X syndrome. The proband had typical features of Down syndrome and did not manifest any symptoms of polysomy X. The patient had hypotonia, a cardiac defect, and an annular pancreas. A clinical diagnosis of Down syndrome was established, but the cytogenetic analysis found two free full trisomies—trisomy 21 (Down syndrome) and triple X.
Conclusion
Cases of double aneuploidy, combining trisomy 21 and trisomy of a sex chromosome, could be challenging because the patients manifest only symptoms, typical for Down syndrome. The discovery of a second complete free trisomy X in our case was an incidental finding. This illustrates the importance of the cytogenetic analysis, despite the evident phenotype of trisomy 21.
Similar content being viewed by others

Background
Double aneuploidy (DA) is a rare genetic phenomenon in humans, and the majority of cases are found in abortive material [1]. It usually involves an autosomal trisomy such as trisomy 21, 18, or 13 and aneuploidy of the sex chromosomes. The last one could be Klinefelter, Turner syndrome, polysomy X, or polysomy Y [2]. There are also reported mosaic cases of DA, which may include other autosomes such as chromosome 8 or 14 [3, 4]. The clinical presentation of every case would be different, depending on the cytogenetic finding.
In this study, we present a case of a full free double aneuploidy, combining both trisomy 21 and triple X syndrome, described for the first time in Bulgaria.
Case presentation
The patient was a preterm girl, born in 37 gestational weeks per vias naturales after a second uneventful pregnancy. The mother’s age was 25 years old. The pregnancy was not followed-up by an obstetrician.
The birth weight of the patient was 2470 g (17.3rd percentile), birth length 46 cm (10.3rd percentile), head circumference 30 cm (2.3rd percentile). Apgar score was 5 points in 1 min and 6 points in 5 min.
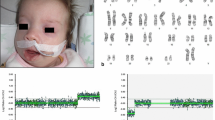
The baby girl presented with upslanting palpebral fissures, and the ears were low set and with abnormal outer morphology (Fig. 1). She also showed a tendency for tongue protrusion. The patient had hypotonia. The above described dysmorphic features were suspicious for the presence of Down syndrome.

Phenotype of the proband, presenting with hypotonia
А chest X-ray of the baby was done due to а systolic murmur. The X-ray showed a normal-sized cardiac silhouette and a dislocated to the right shadow of the right ventricle. A ventricular and an atrial septal defect were diagnosed after a transthoracic ultrasound of the chest. The patient had tachypnea, two-sided vesicular breathing with crepitations. The child needed a constant supply of oxygen.
Every time after the baby was fed, it vomited stomach content, and it could not gain weight. A barium X-ray examination of the abdomen was done, and it was diagnosed with a possible stenosis of the pylorus or the duodenum. On the 7th day after birth, the girl underwent a surgical correction for annular pancreas, which was constricting the duodenum. The other internal organs, bone, and soft tissues were normal.
A blood sample for cytogenetic analysis was collected to prove the clinical diagnosis of trisomy 21. The patient was discharged from the hospital and was clinically improved. The family was referred to genetic counseling.
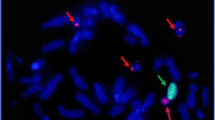
Cytogenetic analysis of peripheral lymphocytes was performed using Giemsa staining in the Laboratory of Medical Genetics, Varna. An informed consent was received from the family. A pathological karyotype 48,ХХХ,+21 was observed in all 100 analyzed metaphase spreads. There were two additional copies of the Х chromosome and chromosome 21 (Fig. 2). The proband was diagnosed with double aneuploidy and two free full trisomies—trisomy 21 (Down syndrome) and triple X syndrome. Cytogenetic analysis of the parents was not performed.

Gimsa-banded metaphase chromosomes of the patient: 48, XXX, +21. Circles indicate the additional copies of chromosome 21 and X chromosome
Discussion
The first published case of the same type of double aneuploidy—trisomy 21 together with triple X syndrome was in 1962 by Breg et al. [5]. We summarized 12 other reported cases through the years (Table 1). Even though the individual frequency of the described aneuploidy is not clear, it is estimated that the frequency of DA in general is around 0.05% in newborns [14]. Despite this, the incidence of these cases could be higher than expected, if it is multiplied by the individual frequency of each of these aneuploidies [12].
The clinical presentation of patients with DA could be different, depending on the cell line, which prevails, the degree of mosaicism, and the type of affected chromosomes. There could be a combination of symptoms, typical for both observed chromosomal aberrations [1, 16]. However, DA of trisomy 21 and a sex chromosome aneuploidy is an exception since there are usually phenotypic traits only of Down syndrome. This is because trisomies of the sex chromosomes generally do not manifest with facial dysmorphism or congenital anomalies [17].
This is also observed in our case due to the fact that triple X syndrome is not associated with any clinical severe features [18]. The main symptoms of our patient are due to the additional copy of chromosome 21. Nevertheless, in cases of triple X syndrome, there may be a developmental delay, learning disabilities, speech problems, behavioral, emotional disorders, and delayed motor skills. Also, there could be menstrual disturbances and early menopause [19]. This illustrates the importance of regular follow-up of our patient with DA not only for complications due to trisomy 21, but also because of the additional copy of the X chromosome.
In contrast to polysomy X, dysmorphic features of monosomy X could be present right after the birth of the baby—for example, lymphedema of hands and feet [20]. However, in cases of mosaicism for the Turner syndrome, the dysmorphic features of Down syndrome would be the main reason for genetic testing [21]. That is why cytogenetic analysis is always required to check for other chromosomal aberrations.
Double aneuploidies are the result of nondisjunction of the chromosomes during the meiotic or mitotic division, but the last one would lead to somatic mosaicism. In cases of meiotic nonreduction, the parental origin of the additional genetic material depends on the time of the nondisjunction [13, 14]. If it occurs during meiosis I, the newly formed gamete will have 24 chromosomes in total and there will be both a maternal and a paternal copy of the additional chromosome. If the homologous chromosomes do not separate during meiosis II, the gamete will have again 24 chromosomes, but the extra one will have the same parental origin—either maternal or paternal. Both of the described aneuploidies in cases of double aneuploidy could have the same or different parental background [13]. However, in around 85.00% of the cases the additional chromosome 21 is maternal. The parental contribution for the additional X chromosome is equal [22].
In most of the cases described in the literature, it was concluded that the DA, no matter if it is trisomy and/or monosomy of two different chromosomes, resulted from the nondisjunction of the chromosomes during the second mitotic division [13, 23, 24]. The failure of the sister chromatids to separate during the cell division (mitosis or meiosis) is relatively common, especially during ovogenesis, and it is not so typical for spermatogenesis. There are no certain risk factors or specific mutations, which are associated with a greater chance of nondisjunction. The most important risk factor is advanced maternal age over 35 years old [18]. However, in our case, the maternal age is not increased—it is 25 years.
Also, monosomies of the autosomes are not compatible with life. Only X monosomies could result in a live birth [1, 14]. Having an additional genetic material is better tolerated possibly due to dosage compensation mechanisms [25]. That is why most of the published cases of DAs, which did not end with the death of the embryo, had for example trisomies. The most common DAs involve chromosome 21, followed by chromosome 16, X, 22, 18, 13, and 15 in a descending order. The combination of Down and Klinefelter syndromes occurs with the highest prevalence in live births [26]. However, the main etiological factors, responsible for double aneuploidies, are unknown [12]. In order to examine the possible mechanism of nondisjunction, it is recommended to check the parental origin of each of the additional chromosomes [24]. This was not done in the case described because of the parents’ refusal, and we were unable to identify the mechanism of the DA. The mother of our patient denied any exposure to teratogenic agents during pregnancy, and there was no history of other cases of chromosomal aberrations in the family (for example, other children with Down syndrome) and the maternal age was not advanced. That is why it is difficult to presume what were the etiological factors for double aneuploidy in the case described.
No matter the etiology of the DA, the change in the number of the chromosomes could be detected by using non-invasive prenatal testing [27]. However, the finding must be confirmed by chorionic villus sampling or amniocentesis because there might be another cause for the DA, for example, placental mosaicism or an underlying maternal disease [28]. The genetic counseling in these cases could be very challenging because of the possible discordance of the result and the actual karyotype of the patient.
Conclusions
The presented case of double aneuploidy could be a challenging diagnosis because the patient manifested only symptoms, typical for Down syndrome. The discovery of a second complete free trisomy X was an incidental finding. That is why it is recommended to order a cytogenetic analysis in every case of Down syndrome, despite the evident phenotype of trisomy 21. This type of genetic testing would not only confirm the diagnosis, but it would also exclude additional chromosomal aberration, like double aneuploidies.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Abbreviations
- DA:
-
Double aneuploidy
References
Balwan WK, Kumar P, Raina T, Gupta S (2008) Double trisomy with 48, XXX+ 21 karyotype in a Down’s syndrome child from Jammu and Kashmir. India. J Genet 87(3):257–259
Watabe T, Koga H (2019) Survival in double aneuploidy involving trisomy 18 and sex chromosome trisomy: a case report of a 27-month-old child and a review of the literature. Congenit Anom. 59(2):43–46
Massara LS, Delea M, Espeche L, Bruque CD, Oliveri J, Brun P et al (2019) Double autosomal/gonosomal mosaic trisomy 47, XXX/47, XX,+ 14 in a newborn with multiple congenital anomalies. Cytogenet Genome Res. 159(3):137–142
Jurcă MC, Bembea M, Iuhas OA, Kozma K, Petcheşi CD, JURCĂ AD et al (2018) Double autosomal trisomy with mosaicism 47, XY (+ 8)/47, XY (+ 21). Morphological and genetic changes of a rare case. Rom J Morphol Embryol. 59(3):985–988
Breg W, Miller O, Cornwell J, editors. Association of triple-X syndrome and mongolism in 2 families. Am J Dis Child; 1962: American Medical Association
Day R, Wright S, Koons A, Quigley M (1963) XXX 21-trisomy and retinoblastoma. Lancet. 282(7299):154–155
Chen AT, Sergovich FR, McKim JS, Barr ML, Gruber D (1970) Chromosome studies in full-term, low-birth-weight, mentally retarded patients. J Pediatr. 76(3):393–398
Papp Z, Osztovics M, Schuler D, Mehes K, Czeizel E, Horvath L et al (1977) Down’s syndrome: chromosome analysis of 362 cases in Hungary. Hum Hered. 27(5):305–309
Park VM, Bravo RR, Shulman L (1995) Double non-disjunction in maternal meiosis II giving rise to a fetus with 48, XXX,+ 21. J Med Genet. 32(8):650–653
Kovaleva NV, Mutton DE (2005) Epidemiology of double aneuploidies involving chromosome 21 and the sex chromosomes. Am J Med Genet. 134(1):24–32
Guzel AI, Demirhan O, Pazarbasi A, Ozgunen FT, Kocaturk-Sel S, Tastemir D (2009) Detection of parental origin and cell stage errors of a double nondisjunction in a fetus by QF-PCR. Genet Test Mol Bioma. 13(1):73–77
Sheth H, Munoz A, Sergi C, Pani J, Blouin J, Sheth J, et al. Triple-X syndrome in a trisomic Down syndrome child: both aneuploidies originated from the mother. Int J Hum Genet. 2011;11(1):51-53.
Uwineza A, Hitayezu J, Murorunkweli S, Ndinkabandi J, Mutesa L (2012) An unusual case of double aneuploidy of down syndrome associated with triple x syndrome: 48, XXX,+ 21. Rwanda Med J. 69(4):27–29
Vergara-Mendez LD, Talero-Gutiérrez C, Velez-Van-Meerbeke A (2018) Double trisomy (XXX+ 21 karyotype) in a six-year-old girl with down phenotype. J Genet. 97(1):337–340
Tair HA, Gizi SNH. Rare case of the clinical combination of two nosological forms of chromosomal pathology. Вестник науки и образования. 2019(5 (59)).
Zaki M, Kamel A, El-Ruby M (2005) Double aneuploidy in three Egyptian patients: Down-Turner and Down-Klinefelter syndromes. Genet Counsel. 16(4):393–402
Otter M, Schrander-Stumpel CT, Curfs LM (2010) Triple X syndrome: a review of the literature. Eur J Hum Genet. 18(3):265–271
Sherman S, Freeman S, Allen E, Lamb N (2005) Risk factors for nondisjunction of trisomy 21. Cytogenet Genome Res. 111(3-4):273–280
Tartaglia NR, Howell S, Sutherland A, Wilson R, Wilson L. Una revisión de la Trisomía X (47, XXX). Orphanet J Rare Dis [Internet]. 2010;5(8).
Manassero-Morales G, Alvarez-Manassero D, Merino-Luna A (2016) Down-Turner syndrome: a case with double monoclonal chromosomal abnormality. Case Rep Pediatr. 2016
Gumus E (2019) Two rare variants of Down Syndrome: Down-Turner syndrome and Down syndrome with translocation (13; 14): a case report. Iran J Public Health. 48(11):2079–2082
Shu X, Zou C, Shen Z (2013) Double aneuploidy 48, XXY,+ 21 associated with a congenital heart defect in a neonate. Balkan J Med Genet. 16(2):85–89
Devlin L, Morrison P (2004) Mosaic Down’s syndrome prevalence in a complete population study. Arch Dis Child. 89(12):1177–1178
Eid SS, Shawabkeh MM, Hawamdeh AA, Kamal NR (2009) Double trisomy 48, XXY,+ 21 in a child with phenotypic features of Down Syndrome. Lab Med. 40(4):215–218
Kojima S, Cimini D (2019) Aneuploidy and gene expression: is there dosage compensation? Epigenomics. 11(16):1827–1837
Ford C, Jones K, Miller O, Mittwoch U, Penrose L, Ridler M et al (1959) The chromosomes in a patient showing both mongolism and the Klinefelter syndrome. Lancet. 273(7075):709–710
Echague CG, Petersen SM (2016) Double aneuploidy detected by cell-free DNA testing and confirmed by fetal tissue analysis. Obstet Gynecol. 127(6):1064–1066
Snyder HL, Curnow KJ, Bhatt S, Bianchi DW (2016) Follow-up of multiple aneuploidies and single monosomies detected by noninvasive prenatal testing: implications for management and counseling. Prenat Diagn. 36(3):203–209
Acknowledgements
Not applicable.
Funding
The presented research did not receive any funding.
Author information
Authors and Affiliations
Contributions
M.T. conducted the analysis and drafted the work. M.L. revised the manuscript and consulted the patients. S.T. is the neonatologist, who took care of the patient. M. H. helped with the laboratory work and the genetic counseling. E.K. provided key information and helped revise the manuscript. L.A. supervised the work process and revised the manuscript. All authors commented on previous versions of the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
An informed consent to participate in the study was obtained from the parents of the patient and a statement for this is included in the manuscript.
Consent for publication
Written informed consent was obtained from the parents of the patient for publication of this case report and accompanying images.
Competing interests
None.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tsvetkova, M., Levkova, M., Tsvetkova, S. et al. Double aneuploidy 48,ХХХ,+21 of a Bulgarian newborn with Down phenotype: a case report. Egypt J Med Hum Genet 21, 25 (2020). https://doi.org/10.1186/s43042-020-00068-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43042-020-00068-2