
Abstract
Background
Renal salt wasting (RSW) is primarily seen with central nervous disorders and is characterized by hyponatremia, elevated urinary sodium excretion, increased urine output, and hypovolemia. Although there have been reports of RSW in children, it has not been reported in newborns.
Case presentation
A term (38 weeks 2 days) female weighing 2060 g, born via normal vaginal delivery, to a primi-gravida mother, was admitted to our neonatal intensive care unit. At birth, the baby was non-vigorous, had aspirated meconium, and required bag-and-mask ventilation following which the baby cried. The child was put on CPAP and inotropes for respiratory distress and shock, respectively, along with first-line antibiotics. Over the next few days, the child was weaned off CPAP, inotropes were stopped, and feeds were started. On postnatal day (PND) 8, the baby developed repeated episodes of seizures requiring two-antiepileptics followed by midazolam infusion, had shock requiring inotropes, and also had a tense anterior fontanelle with altered sensorium and tone changes, for which mannitol and 3% saline were given. Antibiotics were upgraded, and neuroimaging (MRI) revealed left basal-ganglia bleed with intraventricular extension and cerebral venous thrombosis. The baby showed gradual clinical improvement with the above measures and was restarted on feeds. However, from PND-19 onwards the baby had repeated episodes of hyponatremia requiring 3% saline infusions, progressive weight loss, and polyuria. Considering RSW, urine sodium was done which was high (110 mmol/L). For polyuria and weight loss, feed volume was increased, whereas, for hyponatremia, table salt was added to the expressed breast milk (1 gm × tds). Subsequently, all the serum sodium values remained within normal limits, and the baby started gaining weight and was discharged on similar advice (PND 38). On further follow-up, table salt was gradually decreased in the feeds and was stopped after 1 month of discharge with normal serum sodium values.
Conclusion
Management of recurrent hyponatremia in a neonate is challenging. Despite its rarity, RSW in newborns should be considered a differential.
Similar content being viewed by others


Background
Recurrent hyponatremia, defined as a series of episodes of low serum sodium concentration, is a challenging condition in neonates. Recurrent hyponatremia in neonates is a relatively infrequent occurrence; however, the exact incidence remains largely unknown [1]. Causes include the syndrome of inappropriate anti-diuretic hormone secretion (SIADH), renal salt wasting (RSW) syndrome, classical congenital adrenal hyperplasia, decreased effective plasma volume, primary polydipsia, etc. [2,3,4]. Renal salt wasting (RSW) is primarily seen with central nervous disorders, including brain tumors, head trauma, hydrocephalus, neurosurgery, and cerebrovascular accidents. Hyponatremia (S.Na + < 130 mmol/L) is accompanied by elevated urinary sodium excretion (> 40 mmol/L), increased urine output, hypovolemia, normal or high uric acid, suppressed vasopressin, and elevated brain natriuretic peptide concentrations. It is necessary to distinguish it from SIADH as both have opposite treatments; SIADH requires fluid restriction, whereas RSW needs saline infusion [5]. Although there have been reports of RSW in children, it has not been reported in newborns. Hereby, we report a case of renal salt wasting in a term, low birth weight neonate.
Case presentation
A term (38 weeks 2 days) female weighing 2060 g, born via spontaneous normal vaginal delivery, to a primigravida mother with gestational diabetes (on dietary modification), out of a non-consanguineous marriage, was admitted to our neonatal intensive care unit (NICU). At birth, the baby was non-vigorous (APGAR score 1 min-4/10; 5 min-7/10) and had aspirated meconium. Immediate bag and mask ventilation was started, following which the baby cried; however, she was in visible respiratory distress (Downe’s score was 5/10). She was put on bubble CPAP with appropriate settings. In view of the positive sepsis screen (Table 1) and shock (CRT > 3 s; MAP < 5th centile), empirical intravenous (IV) antibiotics (ampicillin, amikacin) and inotropes were started, respectively, along with other supportive treatments. Within 24 h, the clinical condition started improving, and there was no need for further escalation of therapy. By day 4, the baby was weaned off CPAP and was shifted on oxygen by nasal prongs; inotropes were tapered and stopped on the following day. The baby was gradually started on feeds and was tolerating well.
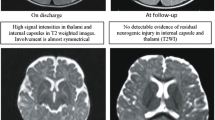
On the 8th post-natal day, the baby developed generalized tonic seizures followed by a dip in the alertness level. On evaluation, blood sugar (35 mg/dL) was low, whereas, ionized calcium (1.24 mmol/L), serum sodium (132 mmol/L), and potassium (4.2 mmol/L) were within the normal range. Immediate correction of hypoglycemia was done by giving a bolus of dextrose 10% along with an increase in the glucose infusion rate of the maintenance fluid. Despite these corrective measures, the baby had repeated episodes of seizures for which antiepileptics (phenobarbitone, followed by phenytoin) were started. On clinical examination, the baby was dull; anterior fontanelle was tense and bulging, with increased tone and repeated posturing episodes. Repeat blood sugar values were normal; however, seizures continued, requiring levetiracetam and midazolam infusions. Considering the possibility of meningitis, antibiotics were upgraded (meropenem) and a blood culture was sent. Baby again developed shock requiring inotropes (dopamine, adrenaline). On day 9 of life, a USG skull was planned however, it was inconclusive. Seizures were controlled on midazolam infusion (3 μg/kg/min). The baby required mannitol, acetazolamide, and 3% saline infusion for features of raised intracranial tension. In the following days, the child remained seizure-free with increased tone in all limbs, midazolam infusion was stopped on day 11. Additionally, there was a disproportionate increase in head circumference on serial monitoring (1 cm/day) with a tense anterior fontanelle and no improvement in sensorium. On day 12, a contrast-enhanced MRI brain was planned to look for the cause of seizures and altered mental status, which showed left basal ganglia bleed with intraventricular extension and watershed infarcts. MR venography revealed cerebral venous thrombosis (CSVT) involving the superior sagittal sinus, straight sinus, and transverse sinus (Fig. 1). Thrombotic workup revealed normal prothrombin and activated partial thrombin time, thrombocytopenia (107,000/mm3) and anemia (Hb 10 g/dL). Workup for inherited causes of hypercoagulable state was not possible due to financial constraints. Metabolic workup, including urine GCMS and blood TMS, was negative. Thyroid profile was normal (TSH 4.51, total T3 1.18 ng/mL, total T4 13.96 mcg/dL). Echocardiography was normal. Blood culture had grown Candida spp. for which fluconazole was added. Gradually, the child started showing some improvement in mental status and was started on orogastric feeds, followed by paladai feeds.

A T1W imaging showing left basal ganglia bleed. B MRI venography showing cerebral venous thrombosis involving superior sagittal, straight, and transverse sinus
On day 19, routine lab evaluation revealed serum sodium 129 mmol/L, which further dropped to 123 mmol/L the next day. Blood pH (7.4), serum potassium (4.3 mmol/L), and other electrolytes were within normal limits. The child also became hypotensive again, requiring fluid boluses and inotropes. Renal functions were also normal (BUN 7 mg/dL, serum creatinine 0.2 mg/dL). Considering the possibility of SIADH, a weight chart was reviewed, which, however, showed progressive weight loss over the last few days. Urine output monitoring revealed polyuria (urine output 6.5 ml/kg/h). The child also started vomiting; considering it symptomatic hyponatremia, a 3% saline bolus was given, followed by infusion at the rate of 0.1 ml/kg/h. Repeat serum sodium values after 24 h showed improvement (S Na 133 mmol/L). However, the next day serum sodium again dropped to 118 mmol/L (Fig. 2A), requiring an increase in the maintenance of 3% saline to 0.5 ml/kg/h. Over the next few days, there were repeated episodes of hyponatremia (Fig. 2A), persistent polyuria (Fig. 2B), and progressive loss of weight (Fig. 2C). In view of these findings, a possibility of renal salt wasting was considered and a urine spot sodium was sent which was 110 mmol/L (high). Serum and urine osmolality were 255 mOsm/kg (low) and 430 mOsm/kg (inappropriately high), respectively, consistent with RSW. Hypouricemia (S. urate 1.2 mg/dL) was also noted. For polyuria and weight loss, initially, extra fluids were given, followed by increased feed volume. For persistent hyponatremia, the baby was started on oral table salt 1 gm per feed three times a day (sodium 23 mmol/kg/day) on day 33 (via paladai). Thereafter, the sodium values remained within the normal range, weight gain started and the baby was shifted out of NICU. In the following days, the baby developed proper rooting, sucking, and swallowing coordination, and hence, direct breastfeeding was started. Subsequently, the baby was discharged in satisfactory clinical condition on day 38 (serum sodium 137 mmol/L, weight 2340 g) with advice to give a pinch (1 gm approx) of table salt 3 times a day mixed with expressed breast milk and review weekly.

A Serum sodium. B Urine output. C Weight in relation to day of life
On follow-up visits, the serum sodium remained within the normal range and the child was gaining weight. In view of this, sodium supplementation was gradually tapered and stopped after one and a half months. Subsequent serum sodium values remained normal.
Discussion
Recurrent hyponatremia in newborns is a condition characterized by repeated episodes of low serum sodium levels. Although transient and self-limiting, hyponatremia is relatively common in neonates. Recurrent cases demand special attention due to the risk of serious complications, such as seizures, neurological impairments, and developmental delays. The etiology of recurrent hyponatremia in newborns is multifactorial and can be attributed to a variety of causes, including SIADH, cerebral/renal salt-wasting syndromes, and gastrointestinal fluid losses.
SIADH in children and neonates is generally associated with underlying conditions such as CNS disorders, malignancies, infections, or drug-induced causes. The primary mechanism involves inappropriate secretion or sustained elevation of ADH levels, leading to impaired free water excretion and subsequent hyponatremia. On the other hand, RSW is a relatively rare condition, characterized by renal salt wasting, leading to hyponatremia and hypovolemia [6, 7]. The main causes of RSW include intracranial disorders, trauma, and neurosurgical procedures. The mechanisms contributing to RSW involve disrupted regulation of the renin–angiotensin–aldosterone system, as well as the release of natriuretic peptides within the brain [8]. Diagnostic criteria include hyponatremia, hypovolemia, polyuria with elevated urine sodium levels, and decreased vasopressin levels. These tests aid in differentiating RSW from other hyponatremic conditions [5, 9, 10]. Additionally, cerebral imaging, such as cranial ultrasound or MRI, may be useful in detecting accompanying IVH [2].
The present case was diagnosed as RSW based on the clinical presentation of hypovolemia, together with laboratory findings of hyponatremia, polyuria, hypouricemia, and elevated urine sodium levels secondary to intraventricular bleed and CSVT [7, 11]. SIADH was ruled out because of the absence of euvolemia (progressive weight loss and polyuria).
The possibility of acetazolamide-induced hyponatremia was also kept which is a relatively rare adverse effect. However, it is primarily observed in adults and rarely reported in pediatric or neonatal populations [12]. Furthermore, our case was already on acetazolamide long before the development of these symptoms. Additionally, these normal levels remained even after discontinuation of oral sodium, despite the fact that acetazolamide was still being administered at that point, thus, favoring RSW.
Among the reported causes of RSW in children, intracranial surgery, meningoencephalitis (most frequently tuberculous) or head injury were the most common underlying intracranial disorders [11]. However, no clear-cut diagnostic criteria were used for most cases. To the best of our knowledge, this is the first case of RSW reported in a neonate. Alzarka et al. described persistent hyponatremia in a neonate having congenital SIADH associated with hypothalamic anomalies with chromosome 1q21.1 deletion syndrome [13]. The only report from India by Srinivasan et al. described severe hyponatremia in a neonate with SIADH while on therapy with theophylline and thiazide [14].
The long-term prognosis of neonatal RSW varies depending on the severity of the initial brain injury, timely intervention, and adherence to proper treatment [15]. Longitudinal studies assessing the neurodevelopmental outcomes of affected neonates are necessary to gain insights into the lasting effects of RSW on the developing brain [16, 17].
Conclusion
Recurrent hyponatremia in neonates presents a diagnostic challenge, necessitating a thorough evaluation of potential underlying causes. While SIADH, genetic disorders, and RSW can all contribute to hyponatremia in neonates, careful clinical assessment, appropriate diagnostic criteria, and the exclusion of other aetiologies are crucial in diagnosing and managing these cases. Further research is required to understand the exact incidence and optimal management strategies for recurrent hyponatremia in this population.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and are available from the corresponding author upon request.
Abbreviations
- ADH:
-
Anti-diuretic hormone
- BUN:
-
Blood urea nitrogen
- CPAP:
-
Continuous positive airway pressure
- CRT:
-
Capillary refill time
- CSVT:
-
Cerebral sinus venous thrombosis
- IV:
-
Intravenous
- IVH :
-
Intraventricular hemorrhage
- MRI :
-
Magnetic resonance imaging
- NICU:
-
Neonatal intensive care unit
- PND :
-
Post-natal day
- RSW :
-
Renal salt wasting
- SIADH:
-
Syndrome of inappropriate anti-diuretic hormone secretion
References
Späth C, Sjöström ES, Ahlsson F, Ågren J, Domellöf M (2017) Sodium supply influences plasma sodium concentration and the risks of hyper- and hyponatremia in extremely preterm infants. Pediatr Res 81:455–460
Berger TM, Kistler W, Berendes E et al (2002) Hyponatremia in a pediatric stroke patient: syndrome of inappropriate antidiuretic hormone secretion or cerebral salt wasting? Crit Care Med 30:792
Gutierrez OM, Lin HY (2007) Refractory hyponatremia. Kidney Int 71:79
Singh S, Bohn D, Carlotti AP et al (2002) Cerebral salt wasting: truths, fallacies, theories, and challenges. Crit Care Med 30:2575
Sherlock M, O’Sullivan E, Agha A et al (2006) The incidence and pathophysiology of hyponatraemia after subarachnoid haemorrhage. Clin Endocrinol (Oxf) 64:250
Maesaka JK, Imbriano LJ (2023) Cerebral salt wasting is a real cause of hyponatremia: PRO. Kidney360 4:e437
Sterns RH, Rondon-Berrios H (2023) Cerebral salt wasting is a real cause of hyponatremia: CON. Kidney360 4:e441
Albanese A, Hindmarsh P, Stanhope R (2001) Management of hyponatraemia in patients with acute cerebral insults. Arch Dis Child 85:246
Hasan D, Wijdicks EF, Vermeulen M (1990) Hyponatremia is associated with cerebral ischemia in patients with aneurysmal subarachnoid hemorrhage. Ann Neurol 27:106
Wartenberg KE, Schmidt JM, Claassen J et al (2006) Impact of medical complications on outcome after subarachnoid hemorrhage. Crit Care Med 34:617
Bettinelli A, Longoni L, Tammaro F et al (2012) Renal salt-wasting syndrome in children with intracranial disorders. Pediatr Nephrol 27:733
Kassamali R, Sica DA (2012) Acetazolamide: a forgotten diuretic agent. Cardiol Rev 19:276–278
Alzarka B, Usala R, Whitehead MT, Ahn S-Y (2018) Hyponatremia: an unusual presentation in a neonate with chromosome 1q21.1 deletion syndrome. Front Pediatr 6:1–6
Srinivasan K, Patole SK, Whitehall JS (2001) Severe hyponatremia in a neonate- an unusual association. Indian Pediatr 38:1410–1412
Qureshi AI, Suri MF, Sung GY et al (2002) Prognostic significance of hypernatremia and hyponatremia among patients with aneurysmal subarachnoid hemorrhage. Neurosurgery 50:749
Palmer BF, Clegg DJ (2023) Cerebral salt wasting is a real cause of hyponatremia: commentary. Kidney360 4:e445
Ganong CA, Kappy MS (1993) Cerebral salt wasting in children. The need for recognition and treatment. Am J Dis Child 147:167
Acknowledgements
Nil.
Funding
No funds, grants, or other support was received.
Author information
Authors and Affiliations
Contributions
IM, RM, AK, UF, and SMA performed the data collection. Interpretation of patient data and analysis were performed by IM, RM, and AK. The first draft of the manuscript was written by IM. RM, AK, UF, and SMA commented on previous versions of the manuscript. IM, RM, AK, UF, and SMA read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval is not applicable. Written informed consent was taken from parents for participating in the study.
Consent for publication
Parents/legal guardians signed written informed consent regarding publishing their data.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Maryam, I., Mazahir, R., Khanam, A. et al. Recurrent hyponatremia in neonate: a case of renal salt wasting syndrome. Egypt Pediatric Association Gaz 72, 32 (2024). https://doi.org/10.1186/s43054-024-00275-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43054-024-00275-1