
Abstract
Background
Dynamic contrast-enhanced MRI (DCE-MRI) is a revolution regarding screening and diagnosis of breast cancer. Yet, sometimes it is not the appropriate choice of imaging since the examination needs to be scheduled and may take place in another department. Contrast-enhanced mammography (CEM) is contrast-based digital mammogram, and consequently, it has emerged as a potential and promising replacer to DCE-MRI.
Main body of the abstract
There is a frequently asked question during the multidisciplinary breast cancer tumor boards is: which modality is more appropriate to be used in each clinical scenario? This article provided a detailed understanding of these two modalities in order to achieve a successful implementation of them into the clinical practice. Which modality to start with, in the context of the detection (screening) followed by characterization or diagnosis of the identified lesions? What is the appropriate application of both modalities in local staging and follow-up? All of these issues would be discussed in this article.
Short conclusion
MRI is a safe tool for breast imaging and has a superior diagnostic performance compared to CEM. However, CEM is getting close: this lies in its accessibility, short-time procedure, requirement of less training and feasibility to standardize.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
In the past few years, the volume of breast imaging modalities has grown exponentially and has undergone profound transformation, and thus, implementing a sound practice has become a real challenge [1]. At present, the challenge in breast imaging is not only about how to diagnose the causes behind breast symptoms, but it is also about how to apply the best practice to do so.
The success of breast imaging is the ability to choose the most appropriate imaging modality for the patient and this modality has to be convenient, fast and cost-effective at the same time.
The introduction of dynamic contrast-enhanced MRI (DCE-MRI) has long been considered a breakthrough in breast imaging. DCE-MRI had provided an enhanced morphology and functional information of the breast which yielded a sensitivity of 95–100% when compared to ultrasound and mammography as reported in large-scale multicenter trials [1,2,3]. Despite the reported high diagnostic performance, DCE-MRI has limitations [4, 5], while breast MRI is the most sensitive method for diagnosis of breast cancer; however, its use in the setting of the clinical practice is often hampered by the idea that the MRI examination has its own schedule, and probably takes place in another department. This may postpone the final diagnosis and the management of the patients, and accordingly, affect the prognosis.
Contrast-enhanced mammography is an advanced application of the digital mammogram that uses contrast material and so it has emerged as a strong competitor to DCE-MRI [6,7,8]. The attractiveness of CEM lies behind its availability, as the patient diagnostic work-up is accomplished on the same day by using the same machine. Another important advantage of CEM is the better patient tolerance and preference when compared to MRI according to surveys that compared both modalities [4, 5].
There is a growing body of evidence that enhances the contribution of CEM as an alternative to DCE-MRI in some situations of breast cancer and this has sparked a controversy among the radiologists and the clinicians. In spite of the abundance of literature discussing both modalities individually or in comparison, there is a lack of consensus about their appropriate use.
In this manuscript, a brief account of the technique of CEM and DCE-MRI will be discussed and then summarized in Table 1 with the stress on the main advantages and drawbacks of each one of them. The controversy in the use of these modalities with regard to the detection (screening), diagnosis (characterization), local staging and follow-up will be also deliberated in detail.
Technique of CEM and DCE-MRI: advantages and drawbacks
CEM and DCE-MRI each one of them is dedicated to improve lesion conspicuity and diagnostic performance. This takes place with the aid of intravenous injection of a contrast media to highlight areas of abnormal angiogenesis in the breast lesions.
In MRI, the patient lies prone and multi-planar imaging is performed before and after contrast injection (gadolinium gadopentate). Dynamic post-contrast sequences are taken after the injection of the contrast agent for duration up to 8 min. The subtraction images are obtained by subtracting the pre-contrast images from the post-contrast ones [9].
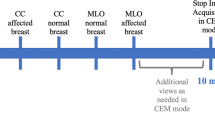
Contrast-enhanced mammography is performed in the erect position. The two conventional mammography views of each breast are taken after a 3-min wait following a single injection of the contrast agent (iohexol, 350 mg I/mL). No further dynamic sequences are obtained. There is a pair of low- and high-energy images which is obtained during a single compression in the standard cranio-caudal and medio-lateral oblique views. A re-combined image is obtained as a result of subtracting the post-contrast low- and high-energy images to produce an image with adequate background subtraction, and consequently, maximizes the conspicuity of the enhancing breast lesions.
Contrast-enhanced mammography is less time-consuming, with a relatively lower cost than DCE-MRI. Patel et al. [8] stated that CEM is a cost-effective modality that could be an alternate to MRI. They stated that CEM can reduce both the direct and the indirect cost of the examination. The review discussed the marked reduction in the equipment (reaching up to 53%) and the staffing (reaching 59%) costs for CEM as compared to breast MRI. They calculated the cost of screening according to the Medicare rates, and they had found that the cost of screening with MRI is fourfolds higher than the cost of screening with CEM. Also, that screening with MRI mandates an additional regular digital mammogram which is not the case with CEM. In CEM, the low energy images serve as a substitute to the regular mammogram.
The classic MRI acquisition takes approximately 30 min, whereas CEM requires about 7–10 min. The latter examination is better tolerated by patients being due to its short procedure time, and the less probability of claustrophobia from the device [4, 5, 8].
MRI also requires a longer interpretation time of the scanned images than CEM [8, 10].
All these factors have rendered CEM to be easily incorporated into the daily workflow [11].
To overcome the above-mentioned MRI limitations, the abbreviated MRI protocol was introduced by Kuhl et al. [11]. The rationale behind the abbreviated protocols is to decrease the cost of MR technique, the acquisition time of the images (3 min) and the interpretation time (3 s). This eventually enhances the feasibility of MRI and improves the patients’ and physicians’ acceptance to the idea of using MRI in the context of screening for breast cancer. According to Kuhl et al. [11], the diagnostic performance of the abbreviated protocol was equivalent to the full diagnostic protocol.
One major disadvantage of CEM is that the estimated radiation dose to the patient may be up to 81% higher than that for the standard 2D digital mammography. This varies according to the breast tissue thickness and density; however, the dose still remains within the permissible range [12,13,14]. Moreover, the risk of a severe adverse reaction to the used contrast medium in CEM is much higher (0.2–0.4%) as compared to gadolinium (0.001–0.01%) [15, 16].
Table 1 shows the summary of the variations of the technique, advantages and drawbacks of the CEM and the classic as well as the abbreviated MR protocols.
*Screening/detection
According to the recommendations of the American College of Radiology (ACR), the screening of the breast cancer should be tailored according to the individual’s risk category. In general, the female population can be categorized into average, moderate and high risk [17].
Average-risk women have no specific risk of developing breast cancer (lifetime risk < 15%). Moderate-risk women are those with a lifetime risk of between 15 and 20%. They include women with biopsy results of an atypical epithelial proliferation, women with a personal history of breast cancer, and women with heterogeneously or extremely dense breasts. High-risk women are defined as those with a lifetime risk for the development of breast cancer of 20–25% higher than the general population, and they include females with a genetic predisposition or those who have received mantle radiation between the ages of 10 to 30 years of age [18,19,20].
The high sensitivity of MRI as compared to mammography comes on the expense of a relatively low specificity with a consequent increase in patient anxiety and an increase in the number of recall rates and unnecessary biopsies. The reason for its low specificity is because of the overlap of contrast uptake by both benign and malignant mass lesions, Fig. 1.

Young patient, high risk, 31 years old. a Ultrasound gray scale image that displayed an oval-shaped solid mass with suspicious infiltrative presentation and irregular borders and accordingly was given as BI-RADS 4 category. b Pre-contrast T2-weigthed MR image that displayed lower outer solid breast mass (circle). c Post-contrast subtraction image (taken at 2 min.40 s, post-injection of contrast, circle) that showed suspicious early and heterogeneous contrast uptake of the left breast mass (arrow). According to the morphology descriptors of the MR images, the mass was irregular and showed intense contrast uptake; these criteria rendered the mass to be suspicious of malignancy (BI-RADS 4) and biopsy was requested. d The time/signal intensity curve showed type I pattern presented with early peak of the contrast uptake with a corresponding high signal intensity percentage of 96%. Examination of the removed specimen after surgery revealed an intracanalicular fibroadenoma surrounded with fibrofatty tissue with no evidence of malignancy
On the other side, microcalcifications that constitute approximately 31% of identified lesions on screening mammogram and also low grade invasive cancers can be missed on MRI [21, 22]. In a study performed by Bennani-Baity et al. [22], 10% of the false negative MRI results were microcalcifications identified only on mammogram Fig. 2.

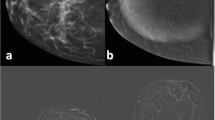
A 35-year-old female that had a palpable left breast lump. a Bilateral digital mammogram craino-caudal views that showed right breast upper outer and central regional asymmetrical density and associate upper outer segmental clustered pleomorphic microcalcifications malignant looking masses that extent beyond the confine of the asymmetrical density. b CEM of both breasts craino-caudal view that showed heterogeneous enhancement of the right breast asymmetrical density, while the area involved with the clustered microcalcifications showed no contrast uptake. The case was proved to be invasive ductal carcinoma and ductal carcinoma in situ. CEM images provided information about the actual extent of the disease in the form of a vascular enhancing invasive component and the distribution of the non-enhancing component of calcifications. This can significantly change the management from breast-conservative surgery to mastectomy
Up-to-date, there is no sufficient data to define the appropriate indications of CEM [23]. The use of CEM as a potential alternative to screening with breast MRI has been discussed in several studies as both modalities provide the same kind of information needed for breast imaging, Fig. 3a, b.

Two cases: the first case was a 35-year-old female presented with left breast palpable lump. Biopsy revealed bilateral invasive ductal carcinoma. a Digital mammogram of both breasts MLO views that showed dense breasts with left breast deep central spiculated mass (BI-RADS 5) (arrow) and right breast retroareolar probably benign (BI-RADS 3) linear asymmetry (circle). b CEM of both breasts MLO views showed left breast mass that was seen on the mammogram and additional newly detected multiple adherent masses (BI-RADS 5- multifocal carcinoma) (circle). The right breast also presented retroareolar ill-defined focal nodule of contrast uptake corresponding to the linear opacity that was seen on the mammogram (BI-RADS 4 proved to be a contra-lateral carcinoma) (circle). The carcinomas were more obvious at the CEM. The second case was a 48-year-old high-risk female that needed a screening mammogram. Biopsy revealed left breast invasive ductal carcinoma. c Left-sided digital mammogram CC and MLO views that showed dense breast with upper outer and lower inner two ill-defined suspicious focal masses (circles). d CEM of the left breast confirmed the malignant suspicion of the left lower mass as it presented rim contrast uptake, moreover another similar focus was also noted nearby (i.e. multifocal not a unifocal carcinoma) (circle). The upper outer mass previously noted on the mammogram showed no contrast uptake (proved to be benign cyst by complementary ultrasound). CEM not only detected the breast masses, but also estimated the accurate extension of the cancer in spite of the high density of the breast parenchyma
A recent study by Sung et al. [24] concluded that CEM has the potential to be used as an alternative screening modality for women of high risk of developing breast cancer especially when MRI is unavailable or contra-indicated [24] (Fig. 3c, d). In another study performed by Xing et al. [25] on 263 breast lesions in 235 patients, they reported that the accuracy and the specificity of CEM were higher than those of MRI (81% and 89.5% for CEM versus 80.2% and 71.7% for MRI), and that the false-positive rate was lower (10.5% for CEM versus 19.8% for MRI) than MRI. The reported relatively low specificity and positive predictive value of DCE –MRI when used in screening have limited its wide-world use as a screening modality. In a study performed by Kuhl et al. [26] to investigate the prognostic significance of tissue changes that cause false-positive imaging diagnoses in MRI, they stated that not all false positive lesions are the same. They found that a significant fraction of lesions reported as false-positive diagnoses were actually high-risk proliferative precancerous lesions. They thus proposed re-defining true positive lesions as those that impact further patient management and thus, proliferative lesions, especially those with atypia, can be considered true and not false positives, Fig. 4.

A high-risk 35-year-old female with dense breasts. a Bilateral digital mammogram craino-caudal views that showed extremely dense breasts, BI-RADS zero. b Bilateral CEM, craino-caudal views that showed right breast lower outer faint asymmetrical regional non-mass contrast uptake of nodular pattern (arrow heads), BI-RADS 3 and left breast deep central faintly enhancing circumscribed focal tiny mass (long arrow), BI-RADS 2. c Early series of DCE-MRI and d Three-dimensional post-contrast maximum intensity projection images. According to MRI findings, there was right breast obvious non-mass clumped contrast uptake, suspicious of malignancy, BI-RADS 4c and left breast deep central benign looking tiny enhancing mass, BI-RADS 2. Based on MRI, biopsy was requested for the right breast non-mass enhancement, and the pathology result was benign proliferative disorder (fibrocystic changes and papillomatosis)
The use of CEM had been validated to recall screened cases in the RACER trial (Rapid access to contrast-enhanced spectral mammography in women recalled for the screening of the breast cancer) by Neeter et al. [27] that was published on 2019. The RACER trial is a prospective, multicenter, randomized controlled trial that aimed to assess whether we can replace the current standard of care (ultrasound and 3D digital breast tomosynthesis) of the re-called women that is suggested by CEM or not. They based their study on the results of the previously published literature which proved that CEM can reduce false-positive results while still maintaining high sensitivity [1, 6, 7, 12].
However, the role of CEM in screening is still debatable whether it should be used as a complementary tool in the diagnostic work-up of the re-called individuals or whether it can be used as a primary screening modality for individuals at high risk of developing breast cancer.
An important point to be considered is that the use of CEM in screening the high-risk individuals exposes them to multiple, repeated low-dose radiation which might lead to an increased risk of radiation-induced breast cancer [1, 28].
Screening with MRI alone without mammography in high-risk individuals is even recommended in some countries like Australia [29] and some European countries [30] to avoid radiation exposure of these individuals.
So, until further large-scale studies are performed and until there is a CEM-BIRADS lexicon that clearly specifies the CEM indications and clinical applications, the use of CEM should be limited to the situations where MR imaging is unavailable or unfeasible.
*Lesion characterization and diagnosis
According to the 2013 MRI BIRADS lexicon, both the morphology descriptors and the kinematics have to be characterized for any identified breast lesion on MRI [31]. According to the morphology descriptors, lesions are classified into non-enhancing and enhancing. Non-enhancing lesions are almost always benign with few exceptions; the commonest of which is the low-grade ductal carcinoma in situ [32]. Enhancing lesions comprise malignant lesions as well as some benign breast lesions [12]. Enhancing lesions are then further classified into foci (< 5 mm, non-space occupying), mass (space-occupying lesions), and non-mass (non-space occupying areas of enhancement). Foci are the most difficult to characterize. Masses are further characterized by describing their shape (oval, rounded and irregular), margin (circumscribed and non-circumscribed), and internal enhancement pattern (homogeneous, heterogeneous, rim, dark septations). Oval or rounded masses with circumscribed margins that show homogeneous or dark septations are considered benign lesions, while irregular masses with non-circumscribed margins that show heterogeneous or rim enhancement are considered malignant. Non-mass lesions are further characterized by describing their distribution (focal, linear, segmental, regional, multiple regions and diffuse) and internal enhancement pattern (homogenous, heterogeneous, clumped and clustered ring). Using the dynamic sequences, a time/signal intensity curve is plotted and lesion kinematics can be described. According to lesion kinematics, three patterns are described: type 1 continuously rising curve, type 2 borderline plateau curve and type 3 early washout curves [33,34,35].
At present, there is no standardized approach for the interpretation of the breast lesions on CEM [35]. Basically, the evaluation of CEM examination requires the combined review of both the low-energy and the post-contrast subtraction images [6].
The low-energy images are identical to the standard mammography images and are thus interpreted according to the 2013, mammography BIRADS lexicon [36].
According to the mammography BIRADS lexicon [36], to characterize masses, the shape, margin and density are to be described. Rounded or oval masses with circumscribed margins and low density are considered benign, while irregular masses with indistinct or speculated margins and high density are considered malignant. Characterization of the breast calcification includes the morphology (benign as vascular, dermal, milk of calcium, large linear, pop corn, dystrophic, punctate, ring and suture calcifications or suspicious/malignant as coarse heterogeneous, amorphous calcifications, fine pleomorphic and linear or branched linear calcifications) and the distribution (diffuse, regional, grouped, linear, or segmental).
The recombined images are evaluated to add-on the value of the low-energy images and correlate them with the characteristics of the contrast enhanced areas. Such action had the privilege of correlating focal distortion or the subtle enhancement that can be easily missed with areas of microcalcifications detected on the low-energy images [6].
A few small-scale publications have analyzed the correlation between the degree of enhancement on CEM and the tumor histological type [37, 38]. In a study by Kamal et al. [39], there were a confirmation on the feasibility to apply the MRI morphology descriptors for the characterization of breast lesions detected on CEM, Fig. 5 with the exception of the rim and the clustered ring patterns of contrast uptake; as these patterns were sometimes seen with breast abscesses, infected cysts and granulomatous mastitis and so eventually not specific for spotting the malignancy on CEM.

Bilateral breast lesions; right fibroadenoma and left locally advanced carcinoma. a Bilateral CEM medio-lateral views that showed right breast lower inner mass of oval shape, circumscribed borders and dark internal septations (arrow) and left breast regional asymmetrical non-mass enhancement of clumped enhancement pattern. b Color mapping post-contrast MR image that showed malignant-looking soft tissue infiltration of the left breast. c Post-contrast MR image that displayed right breast mass with characteristics of fibroadenoma. CEM and post-contrast MR images showed comparable morphology descriptors for both benign and malignant breast pathologies
MRI had an advantage over CEM by its ability to characterize the fluid content within rim enhancing lesions on the T2- and T2-fat suppressed weighted images and thus could be used more often to suggest benign pathology rather than to exclude carcinoma [39].
On the other side, sometimes the performance of the CEM could be limited due to some technical and positioning errors. Non-mass contrast uptake sometimes is not that obvious and unless the breast is not dense, it could be misinterpreted as background contrast uptake (Fig. 4).
Missed cancers are more frequently located at the deep pre-pectoral region, the infra-mammary fold, the upper inner quadrant or deep at the axillary tail [40,41,42]. Breast implants can also impede the visualization of breast lesions on CEM. The breasts have to be carefully compressed, and the implant is to be displaced posterior to be able to see lesions within the breast parenchyma without rupturing the implant [43, 44].
So, for evaluation of the breast implants and confirm or exclude coexisting breast lesion, diagnosis of the breast lesions that are presented with inflammatory features and those that are located in the mammography hidden areas, it is recommended to use MRI breast instead of CEM to avoid missed and/ or misinterpreted breast lesions.
*Cancer staging before surgery
Staging is a way of classifying breast cancer based on how large the cancer is and how far has it spread. In other words, it describes the extent of the disease. Preoperative staging is essential for treatment planning, and it helps in predicting the prognosis of the disease. The commonest used staging system is the tumor-node-metastasis (TNM) system proposed by the American Joint Committee for Cancer (AJCC). The latest update of the TNM staging system (8th edition) was declared in 2017 [45, 46]. In the new edition, the biomarkers are incorporated into the old anatomic TNM staging system if the immuno-histochemical examinations are available [47]. Such incorporation is needed to involve the impact of gene-expression profiling on the biology of the breast cancer [46].
Effective management depends on the accuracy of the pre-surgical assessment for the extent of the disease. The measurement of the tumor size and ascertaining multifocal or multicentric disease are essential items that have to be evaluated before deciding whether the patient will be prepared to mastectomy or breast conservation surgery.
It was proved that MRI is more accurate than conventional imaging examinations in the evaluation of the tumor extension and the detection of multifocal, multicentric and contralateral disease [47,48,49,50]. MRI is also highly sensitive in depicting chest wall infiltration which is identified on MRI as intrasubstance serratus anterior, intercostal muscles or rib infiltration.
However, from another point of view, some studies raised concerns about the low specificity of MRI and the consequent increase in the number of unnecessary extensive surgeries [34, 51].
Several studies have assessed the possibility of replacing MRI by CEM in the local staging of the cancer. These studies confirmed that both CEM and MRI were equivalently sensitive in detecting the index lesion size and in identifying additional lesions [52,53,54] (Fig. 3c, d). However, in a study performed by Helal et al. [55] that compared digital mammography, 3D digital breast tomosynthesis and CEM, the latter displayed the highest percentage regarding the underestimation of tumor sizes (10.2%) among these modalities. The underestimated lesions in their study were either spiculated masses or masses showing intra-ductal extension. Also, MRI is much superior to CEM in case of detection and characterization of the axillary lymph nodes, Fig. 6, and the assessment of the chest wall invasion; this is attributed to the physical limitation of mammography in imaging the axilla and chest wall [52,53,54, 56, 57].

Two different cases of primary breast carcinomas, (case 1 A and B, case 2 C and D). Digital mammograms and CEM medio-lateral views of breast carcinomas (a, c), the lymph nodes are noted at the mammograms (circles in (a) and arrow in (c)) but their differentiation are not clear on basis of the mammogram. On MR images (b, d), the malignant axillary node (arrow in B) could be easily discriminated from the benign one (arrow in d)
So, CEM is cherished for the evaluation of the extent of the breast cancer and multiplicity and so it can replace MRI in the routine local staging of the breast cancer. Yet, MRI is still the examination of choice in the assessment of the immediate post-operative residual disease. Also, the use of CEM in estimating the size of markedly spiculated mass lesions, chest wall and skin infiltration and in the assessment of axillary lymph node status is still questionable.
*Follow up of the treated breast
With the development of breast cancer treatment regimens, the number of breast cancer survivors has increased. The follow-up of patients with treated breast cancer has posed an increasing workload on the breast imaging centers, and thus it has become essential to follow cost-effective regimens [58]. In the post-breast cancer surveillance, the patient follows one of four scenarios: (1) Patient presented with a positive surgical margins after breast cancer excision (2) Asymptomatic patient that require follow-up after surgical and medical management (3) Symptomatic patient that showed up after surgical and medical management, and (4) Patients received neo-adjuvant therapy.
Immediate assessment of the treated breast after surgery for the presence of residual disease is often challenging because of the resultant inflammatory changes, operative bed seroma/hematoma, and scarring distortion, all of which may mimic residual malignancy [59, 60]. Although the role of CEM was assessed in some studies for the postoperative breast, its use in the immediate postoperative period has not yet been validated [61]. MRI has the ability to differentiate inflammatory collections and edema from residual malignancy [62].
Although there is no data to indicate that any imaging other than annual mammography and complementary breast ultrasound points to a survival benefit in asymptomatic survivors, yet, the situation is different for symptomatic survivors or in those cases with positive clinical findings. In these cases, appropriate imaging should be immediately performed [63]. The aim of imaging in these patients is to detect ipsilateral recurrence or a new primary breast cancer in the treated or the contralateral breast so that conservative surgery or mastectomy ± reconstruction could be an option of management. In most of the cases, mammography and targeted ultrasound are enough to reach an accurate diagnosis. However, in patients with inconclusive findings and those with fixed implants, MRI is the modality of choice (Fig. 7). If no corresponding contrast enhancement is found on MRI, malignancy can be excluded with sufficient certainty, and the patient can be safely placed on a short-term follow-up study.

Known case of left breast cancer post-mastectomy. a CEM of the right breast MLO and CC views that showed faint and vague contrast uptake at the lower portion of the breast (circle) that was not obvious at the CC view. b Further scanning by post-contrast MR imaging displayed evident focal area of non-mass enhancement easily depicted at the sagittal and axial reformatted 3D maximum intensity projection images (arrows). MRI was the modality that confirmed the possibility of contralateral carcinoma
Few studies have been performed to test the validity to use CEM instead of MRI in the assessment of the symptomatic cases of breast cancer after surgery [61, 64] (Fig. 8a, b). Helal et al. [61] concluded that CEM is a credible technique that could be used in conjunction with the traditional mammogram to screen for cancer in the breast cancer patients which have been treated with surgery. However, sometimes the performance of the CEM is limited due to the inability to assess the mastectomy bed and the axillary node recurrence.

Two different cases: a case of right breast cancer post-conservative surgery and operative bed positive surgical margins. a Digital mammogram of both breasts MLO and CC views that demonstrated dense breasts and BI-RADS zero category of the mammogram. b CEM of the same views that showed operative bed numerous enhancing foci centered on the scar of the operative bed (circle) suggestive of recurrent carcinoma. The second case is a 53-year-old with pathologically proved triple negative invasive ductal carcinoma grade II. c Axial post-contrast MR imaging before chemotherapy that showed left breast enhancing mass (circle- proved carcinoma) and ipsilateral pathologically enlarged likely infiltrated axillary node (arrow). d Post-completion of the neo-adjuvant chemotherapy post-contrast MR image where there is almost complete resolution of the left breast carcinoma (arrow) and marked regression of the size of the ipsilateral lymph nodes (circle)
Neo-adjuvant chemotherapy (NAC) can induce tumor size reduction, improve the choice of the operation, and thus increase the probability of breast-conserving surgery [65]. During NAC, it is important to assess early tumor response so that treatment regimens can be appropriately tailored to obtain maximum tumor response. Imaging of the tumor response after completion of the course of the neo-adjuvant therapy can also provide valuable information about the extent of the residual tumor and enable better surgical plans to achieve a tumor-free margin. The absence of residual tumor cells in the primary tumor bed after NAC is strongly correlated with improved disease-free and consequently the overall patient survival [66, 67].
Dynamic contrast MRI has long been considered the best imaging modality for both monitoring tumor response to NAC and for the assessment of residual disease extent without competition (Fig. 8c, d). MRI expressed some disadvantages in the NAC context. MRI is highly sensitive to motion artifacts, and the examination is sometimes degraded by the metallic clips that are applied for the chemotherapy-responding tumors and eventually inadequate assessment of the residual tumor size may occur [65]. Moreover, the true extent of carcinomas presented with microcalcifications is not accurately defined using MRI (Fig. 2).
Iotti et al. [68] compared CEM and DCE-MRI in the evaluation of tumor response to NAC in a prospective study conducted on 54 women with breast cancer. Patients had undergone both CEM and MRI before, during and after NAC. They found that the size of the residual cancer measured by CEM and MRI were highly correlated, and they concluded that CEM was as reliable as MRI in assessing the response to NAC and identifying residual disease, and may be an alternative competent to MRI in case the latter modality was contraindicated or its availability was limited. In another study conducted by Barra et al. [69], they concluded that CEM was a feasible method to evaluate residual tumor size after NAC.
However, both modalities are not indicated for the routine annual follow-up of the asymptomatic breast cancer survivors.
Conclusions
CEM and MRI have many privileges but also there are flaws. CEM has shown comparable specificity to MRI so long the lesion is within the main confine of the breast. For the assessment of the extensive inflammatory/malignant breast lesions, deeply seated lesions and those located in the mammography hidden areas; MRI still takes the upper hand.
CEM is useful in the preoperative staging of breast cancer, post-treatment surveillance and the follow-up of patients who are receiving NAC.
The incorporation of CEM in screening high-risk individuals is still debatable.
There is no doubt about the quality of the MRI as a tool for breast imaging; it has a better safety profile (the contrast has less side effects and no risk of radiation induced cancer) and has a superior diagnostic performance compared to CEM. However, CEM is getting close; this lies in its accessibility, short-time procedure, requirement of less training and feasibility to standardize.
Availability of data and materials
The corresponding author is responsible on sending the used data and materials upon request.
Abbreviations
- DEC-MRI:
-
Dynamic contrast-enhanced MR imaging
- CEM:
-
Contrast-enhanced mammogram
- ACR:
-
American College of Radiology
- RACER:
-
Rapid access to contrast-enhanced spectral mammography in women recalled for the screening of the breast cancer
- BI-RADS:
-
Breast imaging reading and data system
- TNM:
-
Tumor-node-metastasis
- AJCC:
-
American Joint Committee for Cancer
- NAC:
-
Neo-adjuvant chemotherapy
References
Cozzi A, Schiaffino S, Sardanelli F (2019) The emerging role of contrast-enhanced mammography. Quant Imaging Med Surg 9(12):2012–2018
Knopp MV, Weiss E, Sinn HP, Mattern J, Junkermann H, Radeleff J et al (1999) Pathophysiologic basis of contrast enhancement in breast tumors. J Magn Reson Imaging 10:260–266
Mann RM, Kuhl CK, Moy L (2019) Contrast-enhanced MRI for breast cancer screening. J Magn Reson Imaging 50:377–390
Hobbs MM, Taylor DB, Buzynski SM, Peake RE (2015) Contrast-enhanced spectral mammography and contrast enhanced MRI: patient preferences and tolerance. J Med Imaging Radiat Oncol 59(3):300–305
Phillips J, Miller MM, Mehta TS, Fein-Zachary V, Nathanson A, Hori W et al (2017) Contrast-enhanced spectral mammography (CESM) versus MRI in the high-risk screening setting: patient preferences and attitudes. Clin Imaging 42:193–197
Perry H, Phillips J, Dialani V, Slanetz PJ, Fein-Zachary VJ, Karimova EJ et al (2019) Contrast-enhanced mammography: a systematic guide to interpretation and reporting. Am J Roentgenol 212(1):222–231
Phillips J, Steinkeler J, Talati K, Brook A, Dialani A, Fishman M et al (2018) Work flow considerations for incorporation of contrast-enhanced spectral mammography into a breast imaging practice. J Am Coll Radiol 15(6):881–885
Patel BK, Gray RJ, Pockaj BA (2017) Potential cost savings of contrast-enhanced digital mammography. Am J Roentgenol 208:W231–W237
Kuczyńska E, Heinze-Paluchowska S, Hendrick E, Dyczek S, Rys J, Herman K et al (2015) Comparison between breast MRI and contrast-enhanced spectral mammography. Med Sci Monit 21:1358–1367
Lia L, Rotha R, Germaineb P, Renc S, Leea M, Huntere K et al (2017) Contrast-enhanced spectral mammography (CESM) versus breast magnetic resonance imaging (MRI): a retrospective comparison in 66 breast lesions. Diagn Interv Imaging 98:113–123
Kuhl CK, Schrading S, Strobel K, Schild HH, Hilgers RD, Bieling HB (2014) Abbreviated breast magnetic resonance imaging (MRI): first postcontrast subtracted images and maximum-intensity projection: a novel approach to breast cancer screening with MRI. J Clin Oncol 32:2304–2310
Tsigginou A, Gkali C, Chalazonitis A, Fedia E, Vlachos DE, Zagouri F et al (2016) Adding the power of iodinated contrast media to the credibility of mammography in breast cancer diagnosis. Br J Radiol 89:20160397
James JR, Pavlicek W, Hanson JA, Boltz TF, Patel BK (2017) Breast radiation dose with CESM compared with 2D FFDM and 3D tomosynthesis mammography. Am J Roentgenol 208:362–372
American College of Radiology Committee on Drugs and Contrast Media. ACR manual on contrast media: version 10.2. American College of Radiology website (2016). https://www.acr.org/~/media/37D84428BF1D4E1B9A3A2918DA9E27A3.pdf.
McDonald RJ, McDonald JS, Kallmes DF, Jentoft ME, Murray DL, Thielen KR et al (2015) Intracranial gadolinium deposition after contrast-enhanced MR imaging. Radiology 275:772–782
Lewin AA, Lourenco AP, Nance KJ, Niell BL, Slanetz PJ, Stuckey AR et al (2017) ACR appropriateness criteria breast cancer screening. J Am Coll Radiol 14(11S):S383–S390
Newell MS, Giess CS, Argus AD, Free P, Friedewald SM, Green ED et al (2018) ACR practice parameter for the performance of contrast enhanced magnetic resonance imaging (MRI) of the breast. American College of Radiology, Reston, VA
Tilanus Linthorst MM, Bartels CC, Obdeijn AI, Oudkerk M (2000) Earlier detection of breast cancer by surveillance of women at familial risk. Eur J Cancer 36:514–519
Kuhl CK, Schmutzler RK, Leutner CC, Kempe A, Wardelmann E, Hocke A et al (2000) Breast MR imaging screening in 192 women proved or suspected to be carriers of a breast cancer susceptibility gene: preliminary results. Radiology 215(1):267–327
Harvey SC, Di Carlo PA, Lee B, Obadina E, Sippo D, Mullen L (2016) An abbreviated protocol for high-risk screening breast MRI saves time and resources. J Am Coll Radiol 13:374–380
Bluekens AM, Holland R, Karssemeijer N, Broeders MJ, den Heeten GJ (2012) Comparison of digital screening mammography and screen-film mammography in the early detection of clinically relevant cancers: a multicenter study. Radiology 265(3):707–714
Bennani-Baiti B, Baltzer PA (2017) MR Imaging for diagnosis of malignancy in mammographic microcalcifications: a systematic review and meta-analysis. Radiology 283(3):692–701
Sorin V, Yagil Y, Yosepovich A, Shaimon GM, Neiman OH et al (2018) Contrast-enhanced spectral mammography in women with intermediate breast cancer risk and dense breasts. AJR Am J Roentgenol 211(5):W267–W274
Sung JS, Lebron L, Pike MC, Ayhan M, Moskowitz CS, Morris EA, Jochelson MS (2019) Performance of dual-energy contrast-enhanced digital mammography for screening women at increased risk of breast cancer. Radiology 293(1):81–88
Xing D, Lv Y, Sun B, Xie H, Dong J, Hao C et al (2019) Diagnostic value of contrast-enhanced spectral mammography in comparison to magnetic resonance imaging in breast lesions. J Comput Assist Tomogr 43(2):245–251
Kuhl CK, Keulers A, Strobel K, Schneider H, Gasia N, Schrading S et al (2018) Not all false positive diagnoses are equal: on the prognostic implications of false-positive diagnoses made in breast MRI versus in mammography/digital tomosynthesis screening. Breast Cancer Res 20(1):13
Neeter L, Houben IPL, Nelemans PJ, Van Nijnatten T, Pijnappel RM, Frotscher C et al (2019) Rapid access to contrast-enhanced spectral mammography in women recalled from breast cancer screening: the RACER trial study design. Trials 20(1):759
Colin C, Foray N, Di Leo G, Sardanelli F (2017) Radiation induced breast cancer risk in BRCA mutation carriers from low-dose radiological exposures: a systematic review. Radioprotection 52:231–240
MRI for high risk women | Cancer Australia. https://canceraustralia.gov.au/clinical-best-practice/breast-cancer/screening-and-early-detection/mri-high-risk-women. Accessed 11 Nov 2019.
Associazione Italiana di Oncologia Medica. Breast neoplasms guidelines. https://www.aiom.it/wp-content/uploads/2018/11/2018_LG_AIOM_Breast_ENversion.pdf. Accessed 11 Nov 2019.
Morris EA, Comstock CE, Lee CH, et al. ACR BI-RADS® magnetic resonance imaging. In: ACR BI-RADS® atlas, breast imaging reporting and data system. Reston, VA: American College of Radiology; 2013.
Millet I, Pages E, Hoa D, Merigeaud S, Doyon FC, Prat X et al (2012) Pearls and pitfalls in breast MRI. Br J Radiol 85(1011):197–207
Mann RM, Cho N, Moy L (2019) Breast MRI: state of the art. Radiology 292(3):520–536
Vinnicombe S (2016) How I report breast magnetic resonance imaging studies for breast cancer staging and screening. Cancer Imaging 16:17
Kamal RM, Helal MH, Wessam R, Mansour SM, Godda I, Alieldin N (2015) Contrast- enhanced spectral mammography: impact of qualitative morphology descriptors on the diagnosis of breast lesions. Eur J Radiol 84:1049–1055
Sickles, EA, D’Orsi CJ, Bassett LW, et al. ACR BI-RADS® mammography. In: ACR BI-RADS® atlas, breast imaging reporting and data system. American College of Radiology, Reston, VA; 2013.
Łuczyńska E, Niemiec J, Hendrick E, Heinze S, Jaszczyński J, Jakubowicz J et al (2016) Degree of enhancement on contrast enhanced spectral mammography (CESM) and lesion type on mammography (MG): comparison based on histological results. Med Sci Monit 22:3886–3893
Lewin JM, Isaacs PK, Vance V, Larke FJ (2003) Dual-energy contrast-enhanced digital subtraction mammography: feasibility. Radiology 229(1):261–268
Kamal RM, Helal MH, Mansour SM, Haggag MA, Nada OM, Farahat IG et al (2016) Can we apply the MRI BI-RADS lexicon morphology descriptors on contrast-enhanced spectral mammography? Br J Radiol 89:20160157
Bae MS, Moon WK, Chang JM, Koo HR, Kim WH, Cho K et al (2014) Breast cancer detected with screening US: reasons for nondetection at mammography. Radiology 270(2):369–377
Yeom YK, Chae EY, Kim HH, Cha JH, Shin HJ, Choi WJ (2019) Screening mammography for second breast cancers in women with history of early-stage breast cancer: factors and causes associated with non-detection. BMC Med Imaging 19(2):1–9
Popli MB, Teotia R, Narang M, Krishna H (2014) Breast positioning during mammography: mistakes to be avoided. Breast Cancer (Auckl) 8:119–124
Sergi J, Elsa P, Oscar H, Naiara M, Josep P, Salvador P (2011) Imaging of breast implants—a pictorial review. Insights Imaging 2:653–670. https://doi.org/10.1007/s13244-011-0122-3
Lourenco AP, Moy L, Baron P, Didwania AD, diFlorio RM, Heller SL et al (2018) ACR appropriateness criteria breast implant evaluation. J Am Coll Radiol 15:S13–S25
Gabriel NH, James LC, Carl JD, Stephen BE, Elizabeth AM, Hope SR et al (2017) Breast. In: Mahul BA (ed) American Joint Committee on Cancer (AJCC). AJCC cancer staging manual, 8th edn. Springer, New York, NY, pp 589–628
Koh J, Kim MJ (2019) Introduction of a new staging system of breast cancer for radiologists: an emphasis on the prognostic stage. Korean J Radiol 20(1):69–82
Boetes C, Mus RD, Holland R, Barentsz JO, Strijk SP, Wobbes T et al (1995) Breast tumors: comparative accuracy of MR imaging relative to mammography and US for demonstrating extent. Radiology 197:743–747
DeMartini W, Lehman C (2008) A review of current evidence-based clinical applications for breast magnetic resonance imaging. Top Magn Reson Imaging 19:143–150
Sardanelli F, Giuseppetti GM, Panizza P, Bazzocchi M, Fausto A, Simonetti G et al (2004) Sensitivity of MRI versus mammography for detecting foci of multifocal, multicentric breast cancer in fatty and dense breasts using the whole-breast pathologic examination as a gold standard. Am J Roentgenol 183:1149–1157
Bitencourt AG, Pereira NP, França LK, Sliva CB, Paludo J, Paiva HLS et al (2015) Role of MRI in the staging of breast cancer patients: does histological type and molecular subtype matter? Br J Radiol 88(1055):20150458
Killelea BK, Gross CP (2014) Is the use of preoperative breast MRI resulting in more invasive breast cancer surgery? Womens Health (Lond Engl) 10:1–3
Fallenberg EM, Dromain C, Diekmann F, Engelken F, Krohn M, Singh JM et al (2014) Contrast-enhanced spectral mammography versus MRI: initial results in the detection of breast cancer and assessment of tumor size. Eur Radiol 24:256–264
Lobbes MB, Lalji UC, Nelemans PJ, Houben I, Smidt ML, Heuts E et al (2015) The quality of tumor size assessment by contrast-enhanced spectral mammography and the benefit of additional breast MRI. J Cancer 6:144–150
Youn I, Choi S, Choi YJ, Moon JH, Park HJ, Ham S et al (2019) Contrast enhanced digital mammography versus magnetic resonance imaging for accurate measurement of the size of breast cancer. Br J Radiol 92:20180929
Helal MH, Mansour SM, Zaglol M, Salaleldin LA, Nada OM, Haggag MA (2017) Staging of breast cancer and the advanced applications of digital mammogram: what the physician needs to know? Br J Radiol 90(1071):20160717
Ali-Mucheru M, Pockaj B, Patel B, Pizzitola V, Wasif N, Stucky C et al (2016) Contrast-enhanced digital mammography in the surgical management of breast cancer. Ann Surg Oncol 23:649–655
Lee-Felker SA, Tekchandani L, Thomas M, Gupta E, Andrews-Tang D, Roth A et al (2017) Newly diagnosed breast cancer: comparison of contrast-enhanced spectral mammography and breast MR imaging in the evaluation of extent of disease. Radiology 285(2):389–400
Swinnen J, Keupers M, Soens J, Lavens M, Postema S, Van Ongeval C (2018) Breast imaging surveillance after curative treatment for primary non-metastasised breast cancer in non-high-risk women: a systematic review. Insights Imaging 9(6):961–970
Chae EY, Cha JH, Kim HH, Shin HJ, Kim H, Lee J et al (2013) Evaluation of residual disease using breast MRI after excisional biopsy for breast cancer. Am J Roentgenol 200(5):1167–1173
Park G, Bae K, Hwang I, SungKim J, JungKwon W, Bang M (2019) Prediction of residual malignancy after excisional biopsy for breast cancer with suspicious microcalcifications: comparison of mammography and magnetic resonance imaging. Clin Breast Cancer 19(6):e753–e758
Helal MH, Mansour SM, Ahmed HA, Abdel Ghany AF, Kamel OF, Elkholy NG (2019) The role of contrast-enhanced spectral mammography in the evaluation of the postoperative breast cancer. Clin Radiol 74(10):771–781
Mansour SM, Abolfotooh A (2012) Does MRI help in the assessment of inflammatory breast disorders? Egypt J Radiol Nucl Med 43(3):487–497
Bick U, Helbich TH. Follow-up of patients with breast cancer: imaging of local recurrence and distant metastases. In: Hodler J, Kubik-Huch R, von Schulthess G (eds) Diseases of the chest, breast, heart and vessels. IDKD Springer Series. Cham: Springer; 2019–2022.
ElFiky SM, Elsaid NA, Azeb EA, Elmor ME, Abdel Aleem NA, Hassan THG (2018) Comparison between the role of contrast enhanced mammography and dynamic contrast enhanced MRI in assessment of breast cancer recurrence. Egypt J Hosp Med 73(1):5875–5885
Lobbes M (2012) Treatment response evaluation by MRI in breast cancer patients receiving neoadjuvant chemotherapy: there is more than just pathologic complete response prediction. Breast Cancer Res Treat 136(1):313–314
Zhu Q, DeFusco P, Ricci A, Cronin E, Kane M et al (2013) Breast cancer: assessing response to neoadjuvant chemotherapy by using US-guided near-infrared tomography. Radiology 266(2):433–442
Rastogi P, Anderson SJ, Bear HD, Geyer CE, Kahlenberg MS, Robidoux A et al (2008) Preoperative chemotherapy: updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27. J Clin Oncol 26(5):778–785
Iotti V, Ravaioli S, Vacondio R, Coriani C, Caffarri S, Sghedoni R et al (2017) Contrast-enhanced spectral mammography in neoadjuvant chemotherapy monitoring: a comparison with breast magnetic resonance imaging. Breast Cancer Res 19(1):106
Barra FR, de Souza FF, Camelo REFA, Ribeiro ACO, Farage L (2017) Accuracy of contrast-enhanced spectral mammography for estimating residual tumor size after neoadjuvant chemotherapy in patients with breast cancer: a feasibility study. Radiol Bras 50(4):224–230
Acknowledgements
Not applicable.
Funding
No source of funding.
Author information
Authors and Affiliations
Contributions
Guarantor of integrity of the entire study was done by KR. Study concepts and design were carried out by KR and MS. Literature research was done by MS, FA, EA and GM. None of them carried out clinical studies. Experimental studies / data analysis was carried out by MS, HM, FA and GM. None of them carried out statistical analysis. Manuscript preparation was done by KR, HM, EA and GM. Manuscript editing was done by KR, MS and HM. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethical committee of the Radiology Departments of an academic highly specialized multidisciplinary Hospital, and an informed written consent was taken from the patients that were included in the study. The committee’s reference number is not applicable.
Consent for publication
All patients included in this research were legible; all of them were above 16 years of age. They gave written informed consent to publish the data contained within this study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kamal, R., Mansour, S., Farouk, A. et al. Contrast-enhanced mammography in comparison with dynamic contrast-enhanced MRI: which modality is appropriate for whom?. Egypt J Radiol Nucl Med 52, 216 (2021). https://doi.org/10.1186/s43055-021-00586-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-021-00586-y