
Abstract
Background
Neoadjuvant chemotherapy (NAC) is currently one of the most commonly utilized treatment options for patients with breast cancer. Evaluating residual disease following NAC is vital in post-chemotherapy treatment planning. Underestimation or overestimation of the residual disease may result in incomplete surgical resection or unnecessary aggressive surgical treatment which can compromise patient survival or result in unwanted morbidity. Contrast-enhanced spectral mammography (CESM) is a new imaging modality that can provide both morphological and anatomical characterization of neoplastic breast lesions when MRI is unavailable or contraindicated. The aim of this prospective observational study was to evaluate the value of CESM in assessing the extent of residual disease following NAC and predicting complete response (CR) with histopathology as the gold standard.
Results
A total of 142 patients were included in our study with invasive duct carcinoma the most prevalent histopathological type seen in 81.7% of cases. The average tumor reduction in size was 40.8% by CESM and 35.8% by histopathology. Comparison between maximum tumor diameter after NAC by CESM and histopathology revealed a high degree of correlation (R = 0.918, p < 0.01). In 45.1% of cases, CESM underestimated the residual tumor size by an average of 1.1 cm. Comparison between CESM and histopathology in predicting CR yielded CESM sensitivity, specificity, positive predictive value (PPV), and negative predictive values (NPV) of 96.7%, 84.6%, 97.2%, and 100%, respectively.
Conclusions
CESM is a new effective imaging modality in assessing residual disease in breast cancer patients receiving NAC. Post-NAC CESM correlated well with residual tumor size by histopathology with a tendency for underestimation. Careful assessment of CESM images should be made to accurately measure the exact tumor size to avoid overestimation or underestimation potentially increasing the extent of the operation. Proper assessment of the true extent of residual disease can help the surgeon to select the optimal surgical technique ensuring radical treatment of the disease improving patient survival and reducing morbidity.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Neoadjuvant chemotherapy (NAC) is currently considered one of the most commonly prescribed therapeutic options for patients with locally advanced as well as operable breast cancer [1]. NAC enables surgical intervention by decreasing the tumor size of previously inoperable breast cancer lesions [2]. In patients with extensive yet operable breast neoplastic lesions who are candidates for modified radical mastectomy (MRM), NAC allows for conservative breast surgery (CBS) by reducing the tumor extent resulting in less postoperative morbidity as well as enhancing cosmetic and psychological yield [3,4,5]. Additionally, NAC offers an unrivaled opportunity for in vivo chemotherapeutic evaluation of cancer cell sensitivity and the development of novel biomarkers of treatment response which in turn can give an indication to patient prognosis [2, 6, 7]. NAC response differs among patients due to several factors including the stage of the disease, human epidermal growth factor 2 (HER2) status, receptor status as well as tumor heterogeneity resulting from varying molecular characteristics [8]. Consequently, 10–35 out of 100 breast cancer patients are resistant to chemotherapy and 5 out of 10 are completely nonresponsive to treatment with subsequent disease progression [9]. As a result, in the event of poor response or disease progression, NAC provides an opportunity to change the treatment plan or recommend some patients for surgical intervention [8].
Evaluation of residual disease following NAC is crucial for post-chemotherapy treatment planning. Underestimating residual disease following NAC may result in an inadequate surgical resection with a subsequent high rate of recurrence or the need for revision surgery. Overestimation, on the other hand, can result in unnecessary aggressive radical surgical treatment. Histopathological assessment remains the gold standard for assessing the response of NAC. However, histological assessment only occurs postoperatively which necessitates the need for a reliable preoperative imaging diagnostic tool [10].
Currently, mammography, ultrasound, contrast-enhanced magnetic resonance imaging (CE-MRI) as well as positron emission tomography (PET) are the most commonly utilized imaging tools to evaluate the response to NAC with CE-MRI considered the most accurate [11, 12]. Several studies have demonstrated that dynamic CE-MRI is the ideal imaging method to assess the response to NAC in patients with breast cancer with sensitivity, specificity, and accuracy up to 90%, 60–100%, and 91%, respectively. Cost, limited availability, long procedure duration, and the inability to examine claustrophobic patients and patients with cardiac pacemakers are all drawbacks to CE-MRI [13,14,15,16,17]. Additionally, some studies have shown that MRI may lead to under as well as overestimation of residual post-NAC disease in 18 out of 100 cases [18].
Contrast-enhanced spectral mammography (CESM) is a new imaging technique that was developed in recent years which uses contrast agents to generate low energy and subtraction images using digital mammography providing morphological and anatomical features of neoplastic breast lesions [19, 20]. The contrast enhancement in the subtraction images reflects the vascularity of the breast lesions. CESM has been reported to have a diagnostic accuracy that is comparable to CE-MRI [21, 22]. Other advantages of CESM include shorter procedure time, lower cost, and the ability to visualize microcalcifications [23,24,25,26]. The use of CESM to assess the response of NAC is therefore justifiable considering its efficiency. The European Society of Breast Imaging (EUSOBI) recommendations published in 2017 stated that CESM can be considered as an alternative imaging technique to CE-MRI when MRI is contraindicated or not available [26]. The aim of this study was to evaluate the value of CESM in assessing the extent of residual disease following NAC in patients with breast cancer as well as predicting complete response (CR) with histopathology as the gold standard.
Methods
This prospective double-institution observational study included all consecutive female patients with pathologically proven breast cancer with a decision to start NAC after being reviewed by each institution’s Breast Unit multidisciplinary team. All patients were initially diagnosed with baseline mammography and breast ultrasound followed by a core needle biopsy under sonographic guidance from the radiologically suspicious masses for histopathological confirmation. Data were collected from January 2017 to February 2021. The study was approved by the institutions’ Ethics Committees. Written informed consent was obtained from all patients who agreed to take part in this study. Inclusion criteria included female patients’ ages more than 18 years, breast cancer diagnosis based on core needle biopsy, completion of institutional NAC treatment protocol followed by surgery and histopathology as well as completion of pre- and post-NAC CESM examinations. Exclusion criteria included contrast media reaction, renal impairment, pregnancy, incomplete NAC treatment or CESM examinations, and lack of informed consent.
CESM examination
All mammographic examinations were performed at the institutions’ Radiology Departments using the GE Healthcare machine (Chalfont St. Giles, UK) allowing dual-energy CESM acquisitions with some specific hardware and software enhancements for image processing and acquisition.
Unlike conventional mammography, the X-ray spectrum was tailored to produce energies just above the K-edge of iodine (33.2 keV) to increase the sensitivity to low concentrations of iodine to optimize the visualization of iodine. Typically, for a 50% glandular and 5-cm-thick breast, exposure times were around 1 s and 3 s for low and high-energy images, respectively.
An intravenous injection of 1.5 ml/kg body weight of a non-ionic contrast medium (Omnipaque) was done manually at one shot with a flow rate of 3 ml/s followed by a flush of saline. After 2 min of contrast medium injection, the patient was positioned, and the exposure was done in the four standard mammographic views: two mediolateral oblique (MLO) and two craniocaudal (CC) views. In each view, the breast was subjected to a combination of low and high-energy exposures, while the breast was still compressed to minimize motion blur keeping the image details seen with the standard mammography. The subtracted images were automatically generated after each low- and high-energy exposure for each view. The average examination time was 10 min. After the examination, the patients were monitored for around 30 min for any potential contrast medium adverse reactions.
Image interpretation
Two sets of CESM were evaluated: one before the start of the NAC treatment and the second after the last dose of chemotherapy with a maximum interval of 14 days from the elective surgery. In our institutions, CESM is displayed paired to allow for comparison. The MLO is assessed followed by CC views with the patient’s right breast on the left side of the screen and the left breast on the left side of the screen. In the CC views, the outer aspect of the breasts is displayed superiorly.
Interpretation of CESM studies was performed via one of the participating radiologists, and in cases of interobserver disagreement, the case was discussed, and a joint consensus was reached. CESM images were evaluated in accordance with the Breast Imaging Reporting and Data System (BI-RADS). The largest dimension of the lesion was recorded from the two consecutive CESMs taken before the start and at the end of NAC.
The Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 criteria were used in our study to evaluate the response to NAC where the response was classified as follows:
-
“Complete response (CR, disappearance of all lesion/s)
-
Partial response (PR, ≥ 30% reduction in longest diameter)
-
Stable disease (SD, < 30% reduction/ < 20% increase in longest diameter)
-
Progressive disease (PD, ≥ 20% increase in longest diameter)” [11, 27]
We compared the largest diameter of the residual lesion taken from the CESM, 2 weeks before surgery to that in the postoperative histopathological study. The efficacy of CESM in assessing residual disease after NAC was compared to the histological analysis, which was considered the gold standard.
Histopathological examination
Following surgery, all surgical specimens were sent to the institutions’ laboratories for histopathological confirmation. Apart from the macroscopic measurement, the tumor’s longest diameter, which is required for identifying the T stage in the TNM classification, was confirmed histopathologically.
Statistical analysis
Data were statistically described in terms of mean ± standard deviation (± SD), range, or frequencies (number of cases), and percentages when appropriate. A comparison of tumor size between CESM and histopathology was done using Wilcoxon signed rank test for paired (matched) samples. For comparing the response between the different pathological types, chi-square ((χ2) test was performed. Correlation between various variables was done using Pearson moment correlation equation for linear relation of normally distributed variables and Spearman rank correlation equation for non-normal variables/nonlinear monotonic relation. Accuracy was represented using the terms sensitivity, specificity, + ve predictive value, and − ve predictive value. Two-sided p values less than 0.05 were considered statistically significant. The diagnostic performance index of CESM for CR was tested using the Clopper–Pearson test with 95% confidence intervals. All statistical calculations were done using the computer program IBM SPSS (Statistical Package for the Social Science; IBM Corp, Armonk, NY, USA) release 22 for Microsoft Windows.
Results
One hundred and fifty-six women were initially enrolled. Three patients were excluded due to major contrast media reactions. Six patients lost to follow-up, and five patients had incomplete CESM examinations. Following exclusion criteria, a total of 142 patients were enrolled in our prospective study. The age ranged from 29 to 77 years with a mean of 46.7 years.
All the patients in our series underwent surgery after the end of chemotherapy. Sixty-two patients (43.7%) underwent CBS, whereas 80 patients (56.3%) underwent MRM. Invasive duct carcinoma (IDC) was the most common histopathological type detected in our patient population seen in 116 cases (81.7%) followed by invasive lobular carcinoma (ILC) in 14 cases (9.9%), mixed IDC and ILC in six cases (4.2%), invasive medullary carcinoma (IMC) in four cases (2.8%) and two cases (1.4%) of invasive papillary carcinoma (IPC).
The enhancement pattern on CESM was assessed qualitatively before and after NAC. Strong heterogeneous enhancement was the most common pattern before chemotherapy seen in 82 cases (57.8%). After NAC, weak heterogeneous enhancement was the most common pattern seen in 114 cases (80.3%). There was no residual enhancement in 26 cases (18.3%) and intense heterogeneous enhancement in only two cases (1.4%). The average tumor size before and after NAC by CESM was 6.0 cm and 3.6 cm, respectively, whereas the average tumor size in the histological examination was 3.7 cm (Table 1). Based on CESM, the average tumor reduction in size was 40.8% compared to the original tumor mass size, whereas it was 35.8% according to histopathology.
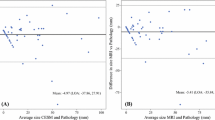
Comparison between maximum tumor diameter after NAC by CESM and histopathology revealed a high degree of correlation (R = 0.918, p < 0.01). CESM overestimated the actual pathology size of the residual tumor in 54 out of 142 cases (38.0%) by 0.1–3.0 cm (average 1.1 cm), underestimated the pathology size in 64 cases (45.1%) by 0.1–3.0 cm (average 1.0 cm), and gave the exact measurement in 24 cases (16.9%). Figure 1 shows the correlation between CESM size and histopathology size in our series.

Correlation between CESM size and histopathology size in our series
Morphological assessment of the tumors’ response to NAC using CESM is shown in Table 2 where CR was observed in 26 cases (18.3%).
Assessment of the tumors’ response to NAC by histopathology is shown in Table 3 where CR was observed in 22 cases (15.5%).
Histopathological assessment of IDC revealed CR in 16 out of 116 cases (13.8%), while CR was achieved in four out of 14 cases of ILC (28.6%) and two out of six cases of mixed IDC + ILC (33.3%). CR was not achieved in any of the six cases of IMC or IPC. Table 4 demonstrates NAC response by CESM and histopathology according to the histopathological type. Figures 2, 3, 4 demonstrate examples of cases encountered in our series.

a Full-field digital mammography in MLO and CC views and b CESM in MLO and CC views in a 45-year-old woman with pathologically proven invasive duct carcinoma showing a heterogeneously enhancing malignant infiltration with speculated outline occupying the UOQ of the right breast and to a lesser extent to UIQ measuring 11.7 cm in longest diameter. c Follow-up full-field digital mammography in MLO and CC views and CESM in MLO and CC of the right breast after neoadjuvant chemotherapy. The tumor now measures about 8.2 cm in longest diameter indicating a PR with a 30% reduction in tumor size which was confirmed on histopathology examination following a right modified radical mastectomy

a Full-field digital mammography in MLO and CC views and b CESM in MLO and CC views in a 42-year-old woman with pathologically proven invasive duct carcinoma showing a right breast UOQ dense mass lesion with obscured outlines showing intense enhancement at the post-contrast study measuring 2.5 cm in longest diameter. c Follow-up full-field digital mammography in MLO and CC views and CESM in MLO and CC after neoadjuvant chemotherapy showing almost total resolution of the previously seen mass lesion with faint residual enhancing nodule measuring 1.5 cm indicating PR. The patient underwent wide local excision of the right breast lesion. Histopathology assessment revealed CR with no viable tumor cells, free resection margin, and free axillary lymph nodes 0/16

a Full-field digital mammography in MLO and CC views and b CESM in MLO and CC views in a 38-year-old woman with pathologically proven invasive duct carcinoma grade II showing a left breast dense mass lesion with obscured outlines at the retro-areolar region showing intense enhancement at the post-contrast study measuring about 4.1 cm in longest diameter. c Follow-up full-field digital mammography in MLO and CC views and CESM in MLO and CC after neoadjuvant chemotherapy showing total resolution of the previously seen mass lesion with no sizable residual enhancing nodule indicating CR. The patient underwent a left modified radical mastectomy. Histopathology assessment revealed CR with no viable tumor cells, free resection margin, and free axillary lymph nodes 0/16
Comparison between CESM and histopathology to predict CR in patients receiving NAC yielded a CESM sensitivity, specificity, positive predictive value (PPV), and negative predictive values (NPV) of 96.7% (95% CI 88.5–99.6%), 84.6% (95% CI 58.5–95.6%), 97.2% (95% CI 90.2–99.7%), and 100% (95% CI 71.5–100%), respectively.
Discussion
Evaluation of NAC response in breast cancer patients is crucial for treatment planning and future clinical outcomes. Patients who do not respond to NAC with disease progression during treatment generally have a poor prognosis. Conversely, patients with a complete pathological response (pCR) have favorable event-free survival (EFS) and overall survival (OS) rates [28, 29]. In this study, we demonstrated high sensitivity and specificity of CESM in predicting CR in breast cancer patients receiving neoadjuvant chemotherapy. We also reported a high degree of correlation between CESM and histopathology in assessing the extent of residual disease with a tendency of underestimation.
In the current study, we found high sensitivity, specificity, PPV, and NPV of CESM in predicting CR in patients receiving NAC similar to previously published results [2, 30,31,32]. All the forementioned studies, ours included, showed a high sensitivity and a lower specificity of CESM in the assessment of CR which reflects the inability of contrast-enhanced imaging techniques in distinguishing between residual neoplastic disease and associated inflammation and reactive changes. A similar problem has been reported in contrast-enhanced MRI which tends to overestimate as well as underestimate residual disease [18]. A meta-analysis study published by Tang and colleagues [33] concluded that CESM has a higher sensitivity and a similar specificity compared to contrast-enhanced MRI in the depiction of evaluation of residual disease in patients with breast cancer receiving neoadjuvant chemotherapy.
We found a high degree of correlation between maximum tumor diameter after NAC by CESM and histopathology similar to a previously published study [2]. A study by Lotti and colleagues [31] reported that CESM showed a better correlation with histopathology compared to MRI with Lin’s coefficient of 0.81 and 0.59 for CESM and contrast-enhanced MRI, respectively. Our findings were contrasted by the study published by Patel et al. [32], who reported a lower degree of correlation of CESM compared to contrast-enhanced MRI with Lin’s coefficient of 0.75 and 0.76 and R values of 0.77 and 0.80 for CESM and MRI, respectively. The contradictory results between different studies could be attributed to a small number of cases and call for a larger multicenter study with a larger group of patients.
In the current study, study, CESM tended to underestimate the actual pathology size of the residual tumor in 45.1% of cases which was consistent with previous studies [2, 31]. Our findings were contrasted by previous investigators who reported a tendency of CESM to overestimate the tumor size by more than 1 cm in 31.8% of cases in their series [30]. Other investigators concluded that the overestimation can be attributed to the fact that NAC induces eradication of tumoral cancer cells before the actual reduction in tumor size can be appreciated on imaging in addition to fibrotic and edematous changes in the tumor bed [34, 35]. Because CESM is a diagnostic modality that involves tumor foci vascularization enhancement, the reduction of tumor vascularization around the tumor during NAC could explain the progressive reduction in the enhancement of the residual tumoral masses on follow-up studies, perhaps underestimating the true size and extent of residual lesions. A similar problem has been reported with contrast-enhanced MRI with a tendency to underestimate residual tumor size following NAC [31, 32]. Studies by Xing et al. [10] and Moustafa et al. [36] tried to overcome this problem through creation of a specialized mathematical model which involves measuring the target lesion’s largest diameter after contrast enhancement and summation of the number of pixels and their intensities within the region of interest before and after NAC. The use of such mathematical models in their studies has resulted in high sensitivity and specificity of CESM in evaluating NAC response [34, 35].
The limitation of our study is the relatively small sample size due to the limited number of patients recruited to NAC, particularly during the COVID pandemic. More multi-institution studies with larger sample sizes using different CESM vendors are needed in the future to confirm and further document our results.
Conclusions
The need for assessing post-NAC residual disease in breast cancer patients is crucial to help the surgeon select the most appropriate surgical technique to enhance the patient survival and quality of life as well as avoid unnecessary radical mastectomies with their associated morbidities. Although considered a relatively new diagnostic imaging tool, CESM has become an important diagnostic tool in the assessment of breast cancer patients. We demonstrated in our study that CESM is an effective imaging modality in the assessment of residual disease in breast cancer patients receiving NAC. Post-NAC CESM correlated well with residual tumor size by histopathology with a tendency for underestimation. Still, careful assessment of CESM images should be made to accurately measure the exact tumor size to avoid overestimation or underestimation potentially increasing the extent of the operation.
Availability of data and materials
The data sets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BI-RADS:
-
Breast Imaging Reporting and Data System
- CBS:
-
Conservative breast surgery
- CC:
-
Craniocaudal
- CE-MRI:
-
Contrast-enhanced magnetic resonance imaging
- CESM:
-
Contrast-enhanced spectral mammography
- CR:
-
Complete response
- EFS:
-
Event-free survival
- IDC:
-
Invasive ductal carcinoma
- ILC:
-
Invasive lobular carcinoma
- IMC:
-
Invasive medullary carcinoma
- IPC:
-
Invasive papillary carcinoma
- EUSOBI:
-
European society of breast imaging
- HER2:
-
Human epidermal growth factor 2
- MLO:
-
Mediolateral oblique
- MRM:
-
Modified radical mastectomy
- NAC:
-
Neoadjuvant chemotherapy
- NPV:
-
Negative predictive value
- OS:
-
Overall survival
- pCR:
-
Pathological complete response
- PET:
-
Positron emission tomography
- PPV:
-
Positive predictive value
- RECIST:
-
Response evaluation criteria in solid tumors
- SD:
-
Standard deviation
References
Gradishar WJ, Anderson BO, Balassanian R et al (2018) Breast cancer, version 4.2017, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 16:310–320
Steinhof-Radwańska K, Graźyńska A, Lorek A et al (2021) Contrast-enhanced spectral mammography assessment of patients treated with neoadjuvant chemotherapy for breast cancer. Curr Oncol 28:3448–3462
Gao W, Guo N, Dong T (2018) Diffusion-weighted imaging in monitoring the pathological response to neoadjuvant chemotherapy in patients with breast cancer: a meta-analysis. World J Surg Oncol 16:145. https://doi.org/10.1186/s12957-018-1438-y
Masuda N, Lee S-J, Ohtani S et al (2017) Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N Engl J Med 376:2147–2159
Curigliano G, Burstein HJ, Winer EP et al (2019) De-escalating and escalating treatments for early-stage breast cancer: the st. gallen international expert consensus conference on the primary therapy of early breast cancer 2017. Ann Cncol 30:118. https://doi.org/10.1093/annonc/mdy537
Morigi C (2019) Highlights of the 16th st gallen international breast cancer conference, vienna, austria, 20–23 March 2019: personalised treatments for patients with early breast cancer. Ecancermedicalscience 13:924. https://doi.org/10.3332/ecancer.2019.924
Bevers TB, Helvie M, Bonaccio E et al (2018) Breast cancer screening and diagnosis, version 3.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 16:1362–1389
Werutsky G, Untch M, Hanusch C et al (2020) Locoregional recurrence risk after neoadjuvant chemotherapy: a pooled analysis of nine prospective neoadjuvant breast cancer trials. Eur J Cancer 130:92–101
Colleoni M, Goldhirsch A (2014) Neoadjuvant chemotherapy for breast cancer: any progress? Lancet Oncol 15:131–132
Xing D, Mao N, Dong J, Ma H, Chen Q, Lv Y (2021) Quantitative analysis of contrast enhanced spectral mammography grey value for early prediction of pathological response of breast cancer to neoadjuvant chemotherapy. Sci Rep 11:5892. https://doi.org/10.1038/s41598-021-85353-9
Mao X, Wang H (2020) Evaluation of the efficacy of neoadjuvant chemotherapy for breast cancer. Drug Des Devel Ther 14:2423–2433
Moo T-A, Sanford R, Dang C, Morrow M (2018) Overview of breast cancer therapy. PET Clin 13:339–354
Choi WJ, Kim HH, Cha JH, Shin HJ, Chae EY (2019) Comparison of pathologic response evaluation systems after neoadjuvant chemotherapy in breast cancers: correlation with computer-aided diagnosis of MRI features. Am J Roentgenol 213:944–952
Taydaş O, Durhan G, Akpınar MG, Demirkazık FB (2019) Comparison of MRI and US in tumor size evaluation of breast cancer patients receiving neoadjuvant chemotherapy. Eur J Breast Health 15:119–124
Negrão EMS, Souza JA, Marques EF, Bitencourt AGV (2019) Breast cancer phenotype influences MRI response evaluation after neoadjuvant chemotherapy. Eur J Radiol 120:108701. https://doi.org/10.1016/j.ejrad.2019.108701
Goorts B, Dreuning KMA, Houwers JB et al (2018) MRI-based response patterns during neoadjuvant chemotherapy can predict pathological (complete) response in patients with breast cancer. Breast Cancer Res 20:34. https://doi.org/10.1186/s13058-018-0950-x
Yoshikawa K, Ishida M, Tsuta K et al (2020) Direct comparison of magnetic resonance imaging and pathological shrinkage patterns of triple-negative breast cancer after neoadjuvant chemotherapy. World J Surg Oncol 18:177. https://doi.org/10.1186/s12957-020-01959-9
Vriens BEPJ, de Vries B, Lobbes MBI et al (2016) Ultrasound is at least as good as magnetic resonance imaging in predicting tumour size post-neoadjuvant chemotherapy in breast cancer. Eur J Cancer 52:67–76
Lalji UC, Jeukens CRLPN, Houben I et al (2015) Evaluation of low-energy contrast-enhanced spectral mammography images by comparing them to full-field digital mammography using EUREF image quality criteria. Eur Radiol 25:2813–2820
Jochelson MS, Lobbes MBI (2021) Contrast-enhanced mammography: state of the art. Radiology 299:36–48
Li L, Roth R, Germaine P et al (2017) Contrast-enhanced spectral mammography (CESM) versus breast magnetic resonance imaging (MRI): a retrospective comparison in 66 breast lesions. Diagn Interv Imaging 98:113–123
Lewin J (2018) Comparison of contrast-enhanced mammography and contrast-enhanced breast MR imaging. Magn Reson Imaging Clin N Am 26:259–263
Xing D, Lv Y, Sun B et al (2019) Diagnostic value of contrast-enhanced spectral mammography in comparison to magnetic resonance imaging in breast lesions. J Comput Assist Tomogr 43:245–251
Fallenberg EM, Schmitzberger FF, Amer H et al (2017) Contrast-enhanced spectral mammography vs. mammography and MRI–clinical performance in a multi-reader evaluation. Eur Radiol 27:2752–2764
Hobbs MM, Taylor DB, Buzynski S, Peake RE (2015) Contrast-enhanced spectral mammography (CESM) and contrast enhanced MRI (CEMRI): patient preferences and tolerance. J Med Imaging Radiat Oncol 59:300–305
Sardanelli F, Fallenberg EM, Clauser P et al (2017) Mammography: an update of the EUSOBI recommendations on information for women. Insights Imaging 8:11–18
Litière S, Collette S, de Vries EGE, Seymour L, Bogaerts J (2017) RECIST—learning from the past to build the future. Nat Rev Clin Oncol 14:187–192
Cortazar P, Zhang L, Untch M et al (2014) Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 384:164–172
Ahmed SH (2019) Safety of neoadjuvant chemotherapy for the treatment of breast cancer. Expert Opin Drug Saf 18:817–827
Barra FR, Sobrinho AB, Barra RR et al (2018) Contrast-enhanced mammography (CEM) for detecting residual disease after neoadjuvant chemotherapy: a comparison with breast magnetic resonance imaging (MRI). Biomed Res Int. https://doi.org/10.1155/2018/8531916
Iotti V, Ravaioli S, Vacondio R et al (2017) Contrast-enhanced spectral mammography in neoadjuvant chemotherapy monitoring: a comparison with breast magnetic resonance imaging. Breast Cancer Res 19:1–13
Patel BK, Hilal T, Covington M et al (2018) Contrast-enhanced spectral mammography is comparable to MRI in the assessment of residual breast cancer following neoadjuvant systemic therapy. Ann Surg Oncol 25:1350–1356
Tang S, Xiang C, Yang Q (2020) The diagnostic performance of CESM and CE-MRI in evaluating the pathological response to neoadjuvant therapy in breast cancer: a systematic review and meta-analysis. Br J Radiol 93:20200301. https://doi.org/10.1259/bjr.20200301
Fasching PA, Gaß P, Hein A (2016) Neoadjuvant treatment of breast cancer-advances and limitations. Breast Care (Basel) 11:313–314
Fowler AM, Mankoff DA, Joe BN (2017) Imaging neoadjuvant therapy response in breast cancer. Radiology 285:358–375
Moustafa AFI, Kamal RM, Gomaa MMM et al (2019) Quantitative mathematical objective evaluation of contrast-enhanced spectral mammogram in the assessment of response to neoadjuvant chemotherapy and prediction of residual disease in breast cancer. Egypt J Radiol Nucl Med 50:1–13. https://doi.org/10.1186/s43055-019-0041-8
Acknowledgements
The authors would like to acknowledge Dr. Magdy Ibrahim for providing the statistical advice for this manuscript and mammography radiographers at National Cancer Institute and Baheya Hospital.
Funding
The authors declare that they did not receive funding for this research.
Author information
Authors and Affiliations
Contributions
HE, SMS, AHR, and SWYG contributed to data collection and analysis, analysis and reporting CESM examinations, reviewing, and editing the manuscript. SME was involved in review of the literature, data collection and analysis, writing the original draft, reviewing, and editing the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
National Cancer Institute and Baheya Hospital Ethics Committee approval was obtained. Reference number is not applicable. Written informed consent was obtained from all patients who agreed to take part in this study.
Consent for publication
All patients included in this research gave written informed consent to publish the data contained within the study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Elkassas, H., El-Maadawy, S.M., Saad, S.M. et al. Role of contrast-enhanced spectral mammography in the assessment of residual disease following neoadjuvant chemotherapy in patients with breast cancer. Egypt J Radiol Nucl Med 53, 249 (2022). https://doi.org/10.1186/s43055-022-00935-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-022-00935-5