
Abstract
Background
RV dysfunction is an important predictor of morbidity and mortality in cardiac patients, especially those having dilated cardiomyopathy (DCM). Deformation imaging parameters (strain and strain rate) are established as new echocardiographic measures that allow for both global and regional RV function assessment. Previous studies showed that heterogeneous segmental deformation affects global RV function differently in various disease states. Echo-Doppler parameters of RV and LV function including RV global longitudinal strain, basal & apical RV strain, LV ejection fraction and LV global longitudinal strain were evaluated in 42 DCM patients & 28 normal subjects, aiming to assess the value of apical versus basal RV strain in detection of RV dysfunction in patients with dilated cardiomyopathy.
Results
DCM patients had significantly lower values of both RV global longitudinal strain and apical RV strain compared to normal subjects (p < 0.001). Basal RV strain did not significantly differ in DCM from normal. The apical RV strain correlated significantly with RV global longitudinal strain, LV ejection fraction and LV global longitudinal strain (p < 0.001 for all). Using ROC curve, a cut-off value of apical RV strain ≤ 29.5 distinguished RV dysfunction from normal with 91.2% sensitivity & 100% specificity.
Conclusions
RV apical but not basal strain reflects the status of RV function, and it represents a valuable measure to diagnose RV dysfunction in patients with DCM.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Various studies demonstrated the essential role of right ventricular (RV) function in determining prognosis in nearly all cardiac disorders, and most particularly, in dilated cardiomyopathy (DCM) patients [1,2,3]. The RV function in dilated cardiomyopathy is connected to LV dysfunction in multiple ways (shared fibers and septal wall, biventricular cardiomyopathic process, increased LV filling pressures, ventricular interdependence, and inextensible pericardial space [4, 5].
For the past three decades, the LV anatomy and function have been extensively studied. The RV has been ignored probably due to the technical difficulties in its imaging as well as its complex anatomy and inadequate understanding of its function and hemodynamics [6].
The RV can be studied with many imaging and functional modalities such as cardiac magnetic resonance (CMR), which is increasingly used as a gold standard method in evaluation of ventricular structure and function. However, it is not a convenient method for some cardiac patients, especially those with non-compatible pacemakers and resynchronization devices. In clinical practice, echocardiography is the mainstay of evaluating RV structure and function [7], as it offers the advantages of feasibility, availability, and suitability to patients for whom CMR is not a convenient modality.
The complex shape and load dependency of the RV create challenges in echocardiographic assessment of RV function [8]. However, despite these challenges, echocardiography remains the most widely utilized clinical imaging modality for assessment of RV function [9].
Multiple echocardiographic parameters for RV contractility have been described and demonstrated clinical utility to quantitatively assess RV function. These parameters include tricuspid annular plane systolic excursion (TAPSE), RV fractional area change (FAC), RV myocardial performance index (RMPI or RV Tei index) and myocardial velocities measured by tissue Doppler imaging. However, there are common limitations for most of these parameters. RMPI, as with most RV functional indices, is load-dependent and can be falsely decreased in conditions with elevated right atrial pressure that causes earlier opening of the tricuspid valve, thus reducing isovolumic relaxation time and thereby underestimating the RV Tei index [10,11,12]. Both TAPSE and tissue Doppler systolic velocity are angle-dependent, reflect translational RV myocardial motion rather than true contraction and reflect only the longitudinal function of the RV basal portion, neglecting the apical and outflow tract components to RV ejection [13].
Deformation imaging parameters (strain and strain rate) are established as new echocardiographic measures that overcome many of the limitations of the conventional echo-Doppler parameters and allow for both global and regional RV function assessment.
RV Strain analysis can be performed using tissue Doppler methods, or speckle tracking echo (STE) which is a more contemporary angle‐independent technique. RV strain measured by STE has been reported to correlate with cardiac magnetic resonance. Thus, it offers a promising tool in assessment of RV function [14]. The aim of the current study was to assess the value of apical versus basal RV strain in detection of RV dysfunction in patients with dilated cardiomyopathy.
Methods
We studied 70 cases [42 patients with dilated cardiomyopathy (DCM) and 28 normal subjects (NL) as a control group]. All study cases were in sinus rhythm. Exclusion criteria included valvular or congenital heart disease, significant arrhythmia, and bad echogenicity. The study protocol complies with the Declaration of Helsinki and was approved by the Medical Ethics Committee of our institute. Informed verbal consent was obtained from all participants before enrollment into the study.
All studied cases were subjected to transthoracic echo-Doppler assessment using Vivid-E9 GE system attached to an echoPAC workstation version 201. Patients were examined in both supine and left lateral positions using multi-frequency (1.5/4.6 MHz) matrix probe M5S. From the standard views, images and cine-loops were obtained and digitally stored for later offline analysis.
Both left and right ventricular functions were assessed using various echo-Doppler modes including M-mode, 2-D echo, conventional Doppler flow imaging, tissue Doppler imaging (TDI) and speckle tracking echocardiography (STE).
Left ventricular echo-Doppler parameters included
-
LV end-diastolic and end-systolic dimensions (LVEDD & LVESD respectively).
-
Percent fractional shortening (PFS) calculated as 100*[(LVEDD-LVESD)/LVEDD]
-
Biplane 2D echo-measured LV ejection fraction (LVEF) calculated automatically by the machine using Simpson’s disk summation method.
-
LV-Tei index calculated from both trans-mitral & trans-aortic Doppler flow signals using the formula: [LV-Tei index = (a time − b time)/b time].
-
The LV “a time” was measured from the end of one trans-mitral flow signal to the start of the following one. It represents the sum of LV isovolumic contraction time, ejection time and isovolumic relaxation time. The LV “b time” represents LV ejection time and was measured from the start to the end of trans-aortic Doppler flow signal.
-
Left ventricular global longitudinal strain (LV-GLS) measured by speckle tracking echo (STE) and calculated automatically by the echo machine from the automated functional imaging with bull's eye display.
Right ventricular echo-Doppler parameters included
-
M-mode measured tricuspid annular plane systolic excursion (TAPSE) guided from 2D apical 4-chamber view. The total systolic displacement was measured from end-diastole to the highest points of contraction by using the leading edges of the echoes.
-
2D echo-measured RV end-diastolic area (RVEDA), RV end-systolic area (RVESA), RV fractional area change (RV-FAC) measured as (RVEDA − RVESA)/ RVEDA.
-
RV systolic pressure (RVSP): measured from tricuspid regurgitation Doppler signal applying the modified Bernoulli equation and adding RA pressure according to the level of jugular venous pulsation.
-
RV-Tei index calculated from both trans-tricuspid & trans-pulmonary Doppler flow signals using the formula: RV-Tei index = (RV-a time − RV-b time)/ RV-b time
-
The RV-“a” refers to the tricuspid valve closure-to-opening time and was measured from the end of one trans-tricuspid flow signal to the start of the following one, and the RV-“b” refers to the RV ejection time and was measured from the start to the end of trans-pulmonary Doppler flow signal.
-
Tissue Doppler imaging-derived RV strain obtained at both basal and apical RV segments (RV-St base & RV-St apex respectively).
-
Speckle tracking echo-derived RV global longitudinal strain (RV-GLS), obtained by manual tracing of the RV endocardial border at end-systole and calculated automatically using the same software applied on the LV as the mean of six segments (basal, mid, and apical segments of both RV free wall and interventricular septum), after further manual adjustment to include the RV wall thickness.
Statistical analysis
Quantitative data were expressed as means ± standard deviations. Age was expressed as range, median and interquartile range (IQR). Categorical data were expressed as numbers and percent (%). Statistical analysis was performed using SPSS software (version 23). Comparison between study groups (DCM & NL) was done using unpaired t test for normally distributed data or Mann–Whitney U-test in case of abnormal data distribution. Paired t test was used to compare RV basal strain with RV apical strain in each group separately (normal subjects and DCM patients). Both independent samples median test and Mann–Whitney U-test were used for comparison of age between the two groups. Chi-square test was used to compare sex distribution in both groups (DCM and NL groups). Pearson correlation coefficient with its significance was determined for parameters of TDI-derived RV strain (RV-St base & RV-St apex) with LV and other RV parameters of systolic function. ROC curve was plotted to determine the cut-off value of RV-St apex that could differentiate between normal and abnormal RV function. p value < 0.05 was considered statistically significant.
Results
This study included 70 cases (42 DCM patients and 28 age and sex matched normal subjects). The DCM group included 35 males and 7 females, and the control group included 10 females and 18 males (χ2 = 3.3, p = 0.69). Comparison of age between DCM and NL group revealed no significant difference. The age of the 70 study cases ranged from 30 to 65 years, grand median: 50 years, IQR: 12.5 years (median test asymptotic significance “p” = 0.106). The age of DCM patients ranged from 30 to 65 years (mean: 51.5 ± 8.6 years, median 52 years, IQR: 14.75), while the age of NL subjects ranged from 40 to 64 years (mean: 49.1 ± 6.4, median 47.5 years, IQR: 8,25), Mann–Whitney U-test p value = 0.225.
Among the DCM group 19 patients (45.2%) were diabetic, 23 patients (54.8%) were smokers and 25 patients (59.5%) had history of hypertension. These patients were under the specific treatment of the associated condition in addition to heart failure treatment. Systolic blood pressure of the DCM patients was 123.3 ± 15.6 mmHg and diastolic blood pressure was 79.8 ± 8.1 mmHg.
Comparison between the DCM group and the NL group in respect to the LV echo-Doppler parameters is shown in Table 1.
Comparison of conventional RV echo-Doppler parameters between DCM & NL group revealed significantly higher values of RVEDA, RVESA & RV-Tei index with lower values of TAPSE & RV-FAC in DCM patients compared to NL subjects (Table 2).
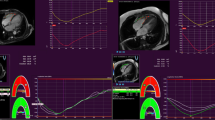
Analysis of RV strain data revealed lower value of RV-St apex, and RV-GLS in DCM patients compared to normal subjects (Fig. 1), while RV-St base did not significantly differ in the two groups (Table 3). RV-St apex was higher than RV-St base in normal subjects (p < 0.0001), but lower than RV-St base in the DCM group (p = 0.002) (Fig. 2).

A & B: RV-GLS in a dilated cardiomyopathy patient (A), and in a normal subject (B). Six strain curves are shown in each case representing basal, mid and apical segments of both RV free wall and interventricular septum. The value of right ventricular global longitudinal strain was 15.9% in the dilated cardiomyopathy patient and 24% in the normal subject

Bar chart demonstrating values of RV-St apex & RV-St base in normal subjects, and in DCM patients. The RV-St apex was significantly higher than the RV-St base in normal subjects, while it had lower value than the basal strain in DCM patients having RV systolic dysfunction. This finding supports the presence of a heterogenous response of the RV free wall segments to the impaired RV systolic function, with the apical segment being mostly affected. [DCM: dilated cardiomyopathy, NL: normal subjects, RV-St apex: Apical RV strain, RV-St base: Basal RV strain, ($): p < 0.0001, (*): p = 0.011]
The RV-St apex showed significant correlation with other parameters of RV and LV systolic function (Table 4), while the RV-St base showed no significant correlation with any parameter except for weak but significant correlation with TAPSE (r = 0.41, p < 0.001) and RV-Tei (r = -0.29, p = 0.02).
Using ROC curve, a cut-off value of apical RV strain ≤ 29.5% distinguished DCM patients having RV dysfunction from normal subjects with 91.2% sensitivity and 100% specificity (AUC = 0.951, p < 0.001) (Fig. 3).

ROC curve demonstrating the sensitivity and specificity of apical RV strain cut-off value differentiating normal subjects from DCM patients. A cut-off value of apical RV strain ≤ 29.5 distinguished DCM patients having RV dysfunction from normal subjects with 91.2% sensitivity and 100% specificity. [ROC curve: receiver operating characteristic curve]
A graphical abstract (Fig. 4) summarizes the major findings in this manuscript.

Graphical abstract summarizing the major findings of the current study. Both apical and basal RV strain were measured in two study groups (DCM patients and NL subjects). The upper panel (A) is a diagram demonstrating 2 sites at the RV free wall for strain measurement. The red arrow & rectangle point to the RV apical segment; the green arrow & rectangle point to the RV basal segment. The lower two panels are 2 graphs illustrating RV-St apex mean value in DCM patients (B) and in normal subjects (C). A cut-off value ≤ 29.5% of the RV-St apex distinguished NL from DCM (sensitivity 91.2%, specificity 100%). [DCM: dilated cardiomyopathy, LA: left atrium, LV: left ventricle, NL: normal subject, RA: right atrium, RV: right ventricle/ventricular, RV-St apex: apical RV strain, RV-St base: basal RV strain]
Discussion
The RV plays an essential role in determining functional status and prognosis in nearly all cardiovascular disorders studied to date. Thus, an early diagnosis of RV dysfunction would allow for the timely treatment and prevention of its progression to cardiac failure.
The normal RV is anatomically and functionally different from the LV, which precludes direct extrapolation of knowledge of left-sided pathophysiology to the right heart. The response of the RV to disease is a consequence of various combinations of pressure and/or volume overload as well as RV intrinsic myocardial deficits, where the predominant abnormality may determine clinical presentation and course. The close relationship between the RV and LV (ventricular interdependence) and its coupling to the pulmonary circulation further modulate RV behavior in different clinical scenarios including DCM [15].
The orientation of RV myofibers and their arrangement into layers is responsible for the distinct contraction pattern of this chamber, with an outer layer of circumferential subepicardial fibers, and an inner layer of longitudinal subendocardial fibers [16]. Unlike the LV, no proper middle layer can be defined in the RV. The superficial layer of the RV is approximately 25% of its wall thickness and is formed by predominantly circumferential aggregates while the subendocardial layer is composed of preferentially arranged longitudinal myocytes that pass through the apex toward the papillary muscles, tricuspid annulus, and RV outflow tract, and are continuous with those of the septum [17]. Probably because of the predominance of longitudinal subendocardial myocytes, longitudinal shortening accounts for approximately 75% of RV contraction [15].
Strain echocardiography is a relatively recent imaging modality that provides information about global and regional RV function. Strain can be obtained from either tissue Doppler imaging (TDI) or more recently by speckle tracking echo (STE). Tissue Doppler-derived strain and strain rate (SR) are based upon mathematical processing of tissue Doppler velocities. Nearly all previous studies have reported tissue velocity gradient from base (higher velocity) to apex (lower velocity); this is because tissue velocity is a function of motion, and the cardiac base moves toward the apex during systole. On the other hand, TDI-derived strain represents intrinsic myocardial deformation regardless of the degree or direction of motion of cardiac segments, thus overcoming the tethering effect limitation of tissue velocity imaging [18, 19].
STE-derived RV longitudinal strain represents the cornerstone of RV mechanics evaluation with high reproducibility, high predictive value, high sensitivity, and specificity in the detection of subclinical RV damage in patients with different cardiovascular diseases including pulmonary hypertension [20,21,22], heart failure, and cardiomyopathies [23,24,25,26]. The investigations that combined echocardiographic analysis with myocardial histologic analysis reported that RV free-wall longitudinal strain was the main determinant of myocardial fibrosis, which may explain a high prognostic value of this parameter in DCM and heart failure patients. RV free-wall strain was reported to have the highest diagnostic accuracy for detecting severe myocardial fibrosis, much better than TAPSE and other conventional parameters of RV systolic function [27, 28].
Regional RV function can be evaluated by myocardial velocities and deformation imaging (strain and strain rate) in the different RV segments. Changes in preload and afterload alter regional RV myocardial velocities, but do not appear to affect strain or strain rate. Regional RV function whether assessed by tissue Doppler or 2D speckle tracking echo has been reported in different studies whose results varied in respect to values of basal and apical strain in healthy subjects and in patients with different pathologies [29,30,31,32,33,34].
In the current study, both global and regional RV function in DCM patients was assessed using different echocardiographic parameters with special emphasis on RV global longitudinal strain (RV-GLS) using speckle tracking echo (STE), in addition to tissue Doppler-derived apical and basal RV strain.
Considering the limitations and strength points of both TDI-derived and STE-derived strain, we preferred to measure TDI-derived strain rather than STE-derived strain for regional RV assessment (apical and basal segments) to justify a more precise strain signal related to the RV myocardial segment to be studied with the special fiber orientation that differs from the LV myocardium. Reasons justifying this selection included: (a) the machine software used for 2D strain by STE in the current study was the same automated functional imaging software applied on the LV; (b) TDI-derived strain has been initially validated with sonomicrometry and also with magnetic resonance imaging [35,36,37], (c) TDI-derived strain was reported to have the highest temporal resolution among all non-invasive imaging modalities, thus recording of the segmental peak strain value would not be missed, (d) TDI-derived strain allows very fast assessment of a single region function with direct display of measured data immediately after image acquisition [38].
Values of basal RV strain in the current study did not show significant difference between DCM patients and normal subjects, in contrast to the values of apical strain that were lower in patients with DCM compared to normal subjects. Also, we demonstrated higher values of apical RV strain than the basal strain in normal subjects but lower values of apical than basal strain in patients with DCM having RV systolic dysfunction. These findings support the presence of a heterogeneous pattern of RV segmental contraction not only in patients with RV dysfunction but also in normal subjects.
Comparable with the findings of the current study, Lopez-Candales et al. [29] reported reduced values of apical strain than basal strain in patients with pulmonary hypertension (PH) in contrast to higher strain values in the mid and apical segments than in the basal segment in individuals without PH. Likewise, a recent study on patients with systemic sclerosis [39] reported significantly impaired peak longitudinal systolic strain at the apical segment of the RV-free wall in PH patients compared to patients without PH.
On the other hand, Li et al. [31] reported higher strain values of basal RV segment compared to apical segment in both healthy individuals and those with PH, but with lower values in all segments in patients with PH compared to normal subjects. Another study reported higher values of apical RV strain than basal and mid segment strain in patients with RV infarction associating inferior myocardial infarction [40]; however, these findings would be explained by the site of coronary lesion affecting more the basal rather than the apical RV segment.
The differences in the heterogenous pattern of the RV (basal versus apical) strain between the various studies would be explained by the different RV pathology, the acquisition views (apical 4-chamber versus RV focused view) and the method of measurement (TDI-derived versus STE-derived strain). Also, the differences in the cut-off strain values that distinguish normal from those with RV dysfunction in the different studies might be attributed to different pathologies affecting the right ventricle and variable analysis algorisms in the different machine vendors.
Regardless of the discrepancy in the results of different studies in respect to heterogeneity of RV regional strain values (basal versus apical), to our knowledge, no previous study reported higher apical strain values in any disease state compared to normal subjects. This would highlight the importance of apical RV strain as an indicator of RV dysfunction in various disease states and recommend it to be considered in routine evaluation of cardiac patients especially being a simple measure to obtain, does not rely on geometric assumption or clear endocardial delineation, in addition to its prognostic value in these patients. However, additional longitudinal studies on a larger number of patients with various RV pathologies, with or without pulmonary hypertension are needed to validate our findings, to detect changes in apical RV strain values along disease progression and to confirm its value as a predictor of morbidity and mortality in the different cardiac disease states.
Study limitations
The machine software used for STE-derived RV strain was the same automated functional imaging software applied on the LV. The use of a dedicated RV software would provide more accurate results whether for global or regional RV function assessment.
Considering regional RV strain, there is no definitive unifying cut-off values for normality that can reliably and consistently be applicable in all RV pathologies and across all vendor platforms. Thus, the cut-off value identified in the current study as a discriminator of RV systolic function status might not be applied on other diseases affecting the RV. Also, other study cohort size might reveal somewhat different cut-off value. Angle dependency of TDI-derived strain used in the current study is another limitation affecting our reported cut-off value; the use of 2D-STE software dedicated to the RV would also be of value in overcoming the limitation of angle dependency in the current study.
Conclusions
The findings in the current study support the presence of a heterogeneous response of the RV free wall segments to the impaired RV systolic function, with the apical segment being mostly affected. Right ventricular apical but not basal strain reflects the status of right ventricular function, and it represents a valuable measure to diagnose RV dysfunction in patients with dilated cardiomyopathy.
Availability of data and materials
All relevant data are incorporated into the manuscript. Other raw data underlying this article will be provided on a reasonable request to the corresponding author.
Abbreviations
- RV:
-
Right ventricle/ventricular
- DCM:
-
Dilated cardiomyopathy
- LV:
-
Left ventricle/ventricular
- ROC curve:
-
Receiver operating characteristic curve
- CMR:
-
Cardiac magnetic resonance
- TAPSE:
-
Tricuspid annular plane systolic excursion
- FAC:
-
Fractional area change
- RMPI or RV Tei index:
-
RV myocardial performance index
- STE:
-
Speckle tracking echocardiography
- NL:
-
Normal subjects
- TDI:
-
Tissue Doppler imaging
- LVEDD:
-
LV end-diastolic dimension
- LVESD:
-
LV end-systolic dimension
- PFS:
-
Percent fractional shortening
- LVEF:
-
LV ejection fraction
- LV-GLS:
-
Left ventricular global longitudinal strain
- RVEDA:
-
RV end-diastolic area
- RVESA:
-
RV end-systolic area
- RV-FAC:
-
RV fractional area change
- RVSP:
-
RV systolic pressure
- RV-St base:
-
Basal RV strain
- RV-St apex:
-
Apical RV strain
- RV-GLS:
-
RV global longitudinal strain
- IQR:
-
Interquartile range
- SPSS:
-
Statistical package for social sciences
- χ2 :
-
Chi-square (with Yates correction)
- AUC:
-
Area under curve
- PH:
-
Pulmonary hypertension
References
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH et al (2013) American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 62:e147-239
Meluzin J, Spinarova L, Hude P, Krejcí J, Dusek L, Vítovec J et al (2005) Combined right ventricular systolic and diastolic dysfunction represents a strong determinant of poor prognosis in patients with symptomatic heart failure. Int J Cardiol 105:164–173
Meyer P, Filippatos GS, Ahmed MI, Iskandrian AE, Bittner V, Perry GJ et al (2010) Effects of right ventricular ejection fraction on outcomes in chronic systolic heart failure. Circulation 121:252–258
Champion HC, Michelakis ED, Hassoun PM (2009) Comprehensive invasive and noninvasive approach to the right ventricle-pulmonary circulation unit: state of the art and clinical and research implications. Circulation 120:992–1007
Voelkel NF, Quaife RA, Leinwand LA, Barst RJ, McGoon MD, Meldrum DR et al (2006) Right ventricular function and failure: report of a National Heart, Lung, and Blood Institute working group on cellular and molecular mechanisms of right heart failure. Circulation 114:1883–1891
Vitarelli A, Terzano C (2010) Do we have two hearts? New insights in right ventricular function supported by myocardial imaging echocardiography. Heart Fail Rev 15:39–61
Haddad F, Hunt SA, Rosenthal DN, Murphy DJ (2008) Right ventricular function in cardiovascular disease, part I: anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation 117:1436–1448
Haddad F, Doyle R, Murphy DJ, Hunt SA (2008) Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation 117:1717–1731
Zaidi A, Knight DS, Augustine DX, Harkness A, Oxborough D, Pearce K et al (2020) Echocardiographic assessment of the right heart in adults: a practical guideline from the British Society of Echocardiography. Echo Res Pract 7:G19–G41
Ghio S, Recusani F, Klersy C, Sebastiani R, Laudisa ML, Campana C et al (2000) Prognostic usefulness of the tricuspid annular plane systolic excursion in patients with congestive heart failure secondary to idiopathic or ischemic dilated cardiomyopathy. Am J Cardiol 85:837–842
Damy T, Viallet C, Lairez O, Deswarte G, Paulino A, Maison P et al (2009) Comparison of four right ventricular systolic echocardiographic parameters to predict adverse outcomes in chronic heart failure. Eur J Heart Fail 11:818–824
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L et al (2015) Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 16:233–270
Giusca S, Dambrauskaite V, Scheurwegs C, D’Hooge J, Claus P, Herbots L et al (2010) Deformation imaging describes right ventricular function better than longitudinal displacement of the tricuspid ring. Heart 96:281–288
Lu KJ, Chen JXC, Profitis K, Kearney LG, DeSilva D, Smith G et al (2015) Right ventricular global longitudinal strain is an independent predictor of right ventricular function: a multimodality study of cardiac magnetic resonance imaging, real time three-dimensional echocardiography and speckle tracking echocardiography. Echocardiography 32:966–974
Sanz J, Sánchez-Quintana D, Bossone E, Bogaard HJ, Naeije R (2019) Anatomy, function, and dysfunction of the right ventricle. J Am Coll Cardiol 73:1463–1482
Ho SY, Nihoyannopoulos P (2006) Anatomy, echocardiography, and normal right ventricular dimensions. Heart 92(Suppl 1):i2–i13
Naeije R, Badagliacca R (2017) The overloaded right heart and ventricular interdependence. Cardiovasc Res 113:1474–1485
Dandel M, Lehmkuhl H, Knosalla C, Suramelashvili N, Hetzer R (2009) Strain and strain rate imaging by echocardiography—basic concepts and clinical applicability. Curr Cardiol Rev 5:133–148
Mor-Avi V, Lang RM, Badano LP, Belohlavek M, Cardim NM, Derumeaux G et al (2011) Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE Consensus Statement on Methodology and Indications Endorsed by the Japanese Society of Echocardiography. Eur j Echocardiogr 12:167–205
Stolfo D, Albani S, Biondi F, De Luca A, Barbati G, Howard L et al (2020) Global right heart assessment with speckle-tracking imaging improves the risk prediction of a validated scoring system in pulmonary arterial hypertension. J Am Soc Echocardiogr 33:1334–1344
Hardegree EL, Sachdev A, Villarraga HR, Frantz RP, McGoon MD, Kushwaha SS et al (2013) Role of serial quantitative assessment of right ventricular function by strain in pulmonary arterial hypertension. Am J Cardiol 111:143–148
Sachdev A, Villarraga HR, Frantz RP, McGoon MD, Hsiao JF, Maalouf JF et al (2011) Right ventricular strain for prediction of survival in patients with pulmonary arterial hypertension. Chest 139:1299–1309
Motoki H, Borowski AG, Shrestha K, Hu B, Kusunose K, Troughton RW et al (2014) Right ventricular global longitudinal strain provides prognostic value incremental to left ventricular ejection fraction in patients with heart failure. J Am Soc Echocardiogr 27:726–732
Guendouz S, Rappeneau S, Nahum J, Dubois-Rande JL, Gueret P, Monin JL et al (2012) Prognostic significance and normal values of 2D strain to assess right ventricular systolic function in chronic heart failure. Circ J 76:127–136
Iacoviello M, Citarelli G, Antoncecchi V, Romito R, Monitillo F, Leone M et al (2016) Right ventricular longitudinal strain measures independently predict chronic heart failure mortality. Echocardiography 33:992–1000
Carluccio E, Biagioli P, Alunni G, Murrone A, Zuchi C, Coiro S et al (2018) Prognostic value of right ventricular dysfunction in heart failure with reduced ejection fraction: superiority of longitudinal strain over tricuspid annular plane systolic excursion. Circ Cardiovasc Imaging 11:e006894
Lisi M, Cameli M, Righini FM, Malandrino A, Tacchini D, Focardi M et al (2015) RV longitudinal deformation correlates with myocardial fibrosis in patients with end-stage heart failure. JACC Cardiovasc Imaging 8:514–522
Lee J-H, Park J-H (2018) Strain analysis of the right ventricle using two-dimensional echocardiography. J Cardiovasc Imaging 26:111–124
López-Candales A, Rajagopalan N, Gulyasy B, Edelman K, Bazaz R (2009) Differential strain and velocity generation along the right ventricular free wall in pulmonary hypertension. Can J Cardiol 25:e73–e77
Lindqvist P, Waldenstrom A, Henein M, Morner S, Kazzam E (2005) Regional and global right ventricular function in healthy individuals aged 20–90 years: a pulsed Doppler tissue imaging study: Umea General Population Heart Study. Echocardiography 22:305–314
Li Y, Xie M, Wang X, Lu Q, Fu M (2013) Right ventricular regional and global systolic function is diminished in patients with pulmonary arterial hypertension: a 2-dimensional ultrasound speckle tracking echocardiography study. Int J Cardiovasc Imaging 29:545–551
Mukherjee M, Chung S-E, Ton VK, Tedford RJ, Hummers LK, Wigley FM et al (2016) Unique abnormalities in right ventricular longitudinal strain in systemic sclerosis patients. Circ Cardiovasc Imaging 9:e003792
Badano LP, Muraru D (2016) Subclinical right ventricular dysfunction by strain analysis: Refining the targets of echocardiographic imaging in systemic sclerosis. Circ Cardiovasc Imaging 9:e005009
Hamdy AM, Fereig H, Abdel-Aziz K, Attia N. Alteration of segmental right ventricular strain pattern in patients with pulmonary hypertension: an indicator of systolic dysfunction; 2009. https://doi.org/10.1093/ejechocard/jep132. Paper presented at EuroEcho 2009 (oral session III), Madrid, Spain 9–12 December 2009.
Voigt JU, Cvijic M (2019) 2- and 3-dimensional myocardial strain in cardiac health and disease. JACC Cardiovasc Imaging 12(9):1849–1863
Sutherland GR, Stewart MJ, Groundstroem KW, Moran CM, Fleming A, Guell-Peris FJ et al (1994) Color Doppler myocardial imaging: a new technique for the assessment of myocardial function. J Am Soc Echocardiogr 7:441–458
Urheim S, Edvardsen T, Torp H, Angelsen B, Smiseth OA (2000) Myocardial strain by Doppler echocardiography: Validation of a new method to quantify regional myocardial function. Circulation 102:1158–1164
Edvardsen T, Gerber BL, Garot J, Bluemke DA, Lima JA, Smiseth OA (2002) Quantitative assessment of intrinsic regional myocardial deformation by Doppler strain rate echocardiography in humans: Validation against three-dimensional tagged magnetic resonance imaging. Circulation 106:50–56
Hekimsoy V, Kaya EB, Akdogan A, Sahiner L, Evranos B, Canpolat U et al (2018) Echocardiographic assessment of regional right ventricular systolic function using two-dimensional strain echocardiography and evaluation of the predictive ability of longitudinal 2D-strain imaging for pulmonary arterial hypertension in systemic sclerosis patients. Int J Cardiovasc Imaging 34:883–892
Sevimli S, Gundogdu F, Aksakal E, Arslan S, Tas H, Islamoglu Y et al (2007) Right ventricular strain and strain rate properties in patients with right ventricular myocardial infarction. Echocardiography 24:732–738
Acknowledgements
The authors thank Dr. Noura Tolba Mohamed for her contribution to the collection and tabulation of data.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
AAA: collection of data, analysis of data, and revision of the manuscript. SAM: collection & interpretation of data, and revision of the manuscript. AMH: idea, design of work, statistical analysis of data, manuscript writing and revision. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol complies with the Declaration of Helsinki and was approved by the Medical Ethics Committee of the Faculty of Medicine for Girls, Al-Azhar University. Informed consent was obtained from all participants before enrollment into the study. However, consent was only verbal, and all were informed that their echo-Doppler measures would be included in the research without any of their personal data or photographs. Written consent was not required, because all dilated cardiomyopathy patients included in this study were selected from those who were admitted for management in the Cardiology Department, Al-Zahraa University Hospital, and echo-Doppler examination was indicated for their clinical evaluation, moreover, it carries no possible risk. All participants of the control group were colleagues or employees in the Cardiology Department, Al-Zahraa University Hospital and all were cordially welcoming to share in this study. No personal data or photographs of any participant were included in this manuscript. None of the study participants was under 16 years old (age range of the patients’ group was 30 to 65 years, and that of the normal subjects was 40 to 64 years).
Consent for publication
Not applicable
Competing interests
All authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ali, A.A., Mohammed, S.A.A. & Hamdy, A.M. Apical but not basal RV strain reflects right ventricular dysfunction in patients with dilated cardiomyopathy. Egypt J Radiol Nucl Med 54, 92 (2023). https://doi.org/10.1186/s43055-023-01033-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-023-01033-w