
Abstract
Background
Weaning off mechanical ventilation (MV) is a critical step in pediatric ICU; however, it lacks standardized criteria. Diaphragmatic ultrasound parameters like diaphragm thickening fraction (DTF), diaphragmatic excursion (DE) and time to peak inspiratory amplitude (TPIA) can be used to assess diaphragmatic muscle strength and to predict weaning success.
Aim of study
Is to assess the validity of diaphragmatic ultrasonography as a predictor of weaning outcome from mechanical ventilation in pediatric age group.
Methods
Prospective cohort study including 30 pediatric patients aged 0–18 years on mechanical ventilation. Ultrasound measurements of diaphragmatic thickening fraction, diaphragmatic excursion and time to peak inspiratory amplitude were taken during the spontaneous breathing trial (SBT) and compared between successful and failed weaning groups.
Results
Out of the included 30 patients (50% male), 19 patients (63.3%) were successfully weaned. Mechanical ventilation duration was significantly longer in the failed weaning group (P = 0.017). There was significant difference between both groups regarding right DE (P = 0.032) and left DE (P = 0.022) with cutoff values of > 4.1 mm and > 5.5 mm with AUC (Area under curve) of 0.737 and 0.831, respectively. There was no statistically significant difference between both groups regarding DTF or TPIA.
Conclusion
We have found that DE is a predictor of weaning success, while DTF and diaphragmatic TPIA had no correlation with weaning outcome.
Similar content being viewed by others


Background
Mechanical ventilation (MV) is widely used in pediatric intensive care units (PICU). About one-third of PICU patients need MV support. However, MV support is not the end of the treatment, and the goal is to help patients wean off MV support. Weaning is a crucial transition for every patient and its optimal timing can decrease the duration of MV and reduce complications [1].
In pediatric population, there is no defined standard for weaning, and no ideal ventilator settings that is agreed upon to wean children in PICU [2]. Currently, weaning from MV is mainly a clinical judgment subjective decision, leading to extreme variations in weaning decisions and inevitable weaning failure [3].
Multiple factors must be present for successful weaning, including hemodynamic stability and adequate ventilation/perfusion ratio of the patient in addition to ability to generate a strong cough, expectorate endotracheal secretions and generate a reliable ventilator pattern. All these factors are affected by decreasing lung aeration, alterations in pulmonary compliance and diaphragmatic dysfunction resulting from prolonged MV [4].
It has been established in adults that prolonged MV leads to ventilator-induced diaphragmatic dysfunction (VIDD) which is basically atrophy and dysfunction of the diaphragm, leading to MV-induced loss of diaphragmatic force-generating capacity contributing to a longer weaning time and higher mortality [2, 5].
Ultrasound being portable, fast and safe as well providing real-time morphologic and functional information, can play an important role in assessing two crucial factors among those that influence weaning: the aeration of the pulmonary parenchyma and the diaphragmatic function, providing clues on the probability of weaning success [4].
In adults, multiple studies have demonstrated the ability of diaphragmatic ultrasound to predict weaning success, leading to better decisions in weaning patients from MV. Conversely, in pediatric population, there are few studies exploring the role of diaphragmatic ultrasound in weaning in PICU, leading to insufficient conclusions. Moreover, children and adults vary widely in their respiratory physiology and anatomical characteristics [1].
Diaphragmatic ultrasound assesses the diaphragmatic function and contractility by measuring the diaphragm thickening during inspiration which is called diaphragmatic thickening fraction (DTF) and correlates strongly with diaphragmatic strength [5]. Another parameter measured is the diaphragmatic excursion (DE), which represents the vertical distance moved by the diaphragm during the respiratory cycle and reflects the respiratory effort exerted by the patient [4].
Time to peak inspiratory amplitude (TPIA) is a newly proposed diaphragmatic ultrasound parameter which is the time from the beginning of diaphragmatic contraction to the maximal amplitude of diaphragmatic inspiratory excursion. It was shown that longer TPIA correlated with more successful weaning from MV, suggesting that TPIA could be a marker for diaphragmatic strength [6].
The aim of this study is to assess the validity of diaphragmatic ultrasonography as a predictor of weaning outcome from mechanical ventilation in pediatric age group.
Methods
After ethical committee approval, a prospective cohort study was carried at our pediatric intensive care unit (PICU) of the children Hospital of Ain Shams University, Cairo, Egypt, starting from July 2021 to June 2023.
Study population
We included patients < 18 years in our PICU with acute respiratory failure connected to invasive mechanical ventilation for more than 24 h and eligible for weaning according to the following criteria: Reversal of the principal cause of mechanical ventilation, PaO2 ≥ 60 mmHg, FiO2 ≤ 0.40, PEEP ≤ 5 cmH2O, ratio of PaO2 to FiO2 ≥ 200, PH ≥ 7.30; RR ≤ 45/m, HR ≤ 140/min, RSBI ≤ 8 breaths/min/ml/kg body weight, minimal use of inotropic or vasopressor drugs, stable body hemodynamics, adequate consciousness level, does not receive sedatives or neuromuscular blocking drugs, absence of hemorrhage or anemia and no electrolyte disturbance. We excluded patients having; chronic neuromuscular disorder, known congenital heart, lung, or pleural malformation, unilateral/bilateral absence of diaphragmatic mobility in ultrasound, cervical spinal cord injury, pneumothorax, pleural effusion, ascites and those undergone thoracic or esophageal surgeries needing diaphragmatic manipulation.
Sample size calculation
Based on data present in the literature in 2020 mainly the work of Xue et al. [1] and Abdel Rahman et al. [7] and expected rate of successful weaning = 60%, our study included a convenience sample of 30 patients.
Study procedures
Informed consent from the patients’ guardians was acquired. Detailed history and anthropometric measurements were recorded. Once the patient is eligible for weaning, a spontaneous breathing trial (SBT) was commenced using low level of pressure support (5 cm H2O). Diaphragm and lung ultrasound were performed during the SBT. Treating clinicians were blinded to the results of the lung ultrasound score and diaphragm measurements. If the patient is eligible for extubation, he was followed up for 48 h to record the need for assisted ventilation (Invasive or noninvasive) post-extubation, and accordingly, patients were divided into two groups:
-
Successful weaning group: Defined as successful extubation and no need for noninvasive ventilation (NIV) or reintubation within 48 h.
-
Failed weaning group: Failed SBT or when there is need for reintubation or NIV within 48 h.
Diaphragmatic ultrasound
All US measurements were performed using Samsung HM70A Ultrasound machine using the LA3-16AD 3–16 MHz Linear Array Transducer and the CF4-9 4–9 MHz Microconvex Array Transducer with all the US examinations done by a single trained radiologist to avoid any inter-observer variation. Patients were imaged in a semi-recumbent position with the head of bed at a 30-degree angle. Measurements were made of the right and left hemidiaphragms and repeated in three different respiratory cycles and an average was taken. For each side, three measurements were taken: DTF, DE and TPIA.
DTF was calculated by the following equation: DTF = (Thickness at the end inspiration – thickness at the end expiration)/Thickness at the end expiration × 100. It was measured in B-mode by placing the linear ultrasound probe in the 8th or 9th intercostal space between the anterior and midaxillary line in a perpendicular position to the chest wall an area designated the zone of apposition. Thickness of the diaphragmatic muscle was measured from the central point of the pleural line to the central point of the peritoneal line during the termination of inspiration and the termination of expiration (Fig. 1).

Measuring diaphragmatic thickness to calculate DTF using linear array probe. A Measuring at end inspiration with lung visible in the image due to caudal displacement of the diaphragm. B Measuring at end expiration
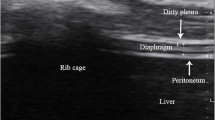
DE and TPIA were measured in M-mode by placing the microconvex 4–9 MHz ultrasound probe either a subcostally or intercostally in the mid-clavicular line, or in the right or left anterior axillary line. The liver or spleen was used as an acoustic window for each hemidiaphragm which appears as an echogenic line. The ultrasound probe was placed in the direction in which the ultrasound beam reaches the posterior third of the corresponding hemidiaphragm perpendicularly usually cranially, medially and dorsal. During inspiration, the normal diaphragm moves caudally toward the ultrasound transducer, which is recorded as an upward motion of the M-mode tracing and the reverse occurs during expiration.
DE is the vertical distance in millimeters between the highest and lowest peak points in the M-mode tracing while TPIA is the time from the beginning of diaphragmatic contraction to the maximal amplitude of diaphragmatic inspiratory excursion (Fig. 2).

Measuring right DE and diaphragmatic TPIA using microconvex probe in M-Mode. Liver is providing excellent acoustic window
Study outcome
Compare diaphragmatic ultrasound measurements (DTF, DE and TPIA) between successful and failure weaning groups to assess their value in prediction of weaning outcome.
Statistical methods
The quantitative data were presented as mean, standard deviations and ranges when parametric and median, inter-quartile range (IQR) when data found nonparametric. Qualitative variables were presented as number and percentages. The comparison between groups with qualitative data was done by using Chi-square test. The comparison between two independent groups with quantitative data and parametric distribution was done by using independent t test while with nonparametric distribution was done using Mann–Whitney test.
Results
The study was conducted on 30 PICU patients. Nineteen patients (63.3%) were successfully weaned. Demographic, clinical and US data of our study is summarized in Table 1. We found no significant association between both groups in regard to their age, gender or BMI.
Clinically there was a statistically significant correlation between duration of ventilation and weaning outcome (P = 0.017) where successful weaning group had shorter duration of MV.
Regarding diaphragmatic US measurements, we were only able to visualize the left diaphragm using the microconvex probe to measure DE and TPIA in 17 patients (56.7%). We found statistically significant correlation between the right and left DE and the weaning outcome (P = 0.032 and 0.022, respectively). We found no statistically significant correlation between right and left DTF or TPIA and weaning outcome.
ROC analysis of the right and left DE performance for the prediction of weaning failure or success was done (Table 2). The best cutoff value of excursion on the right side for predicting weaning success was ≥ 4.1 with an AUC of 0.737, the application of this threshold resulted in a sensitivity of 84.2% and a specificity of 54.55%. The best cutoff value of excursion on the left side for predicting weaning success was ≥ 5.5 with an AUC of 0.831, the application of this threshold resulted in a sensitivity of 54.5% and a specificity of 100%.
Discussion
The feasibility of using diaphragmatic ultrasound indices in predicting the weaning success from MV in adults has been demonstrated in multiple studies [8, 9] and although US is extensively employed in PICUs for echocardiographic and lung assessments, its application for diaphragm studies within pediatric intensive care settings is relatively recent. At the start of this study, there was limited studies regarding this topic in the pediatric age group [1, 2, 7] with more yet conflicting data emerging during the study period [10,11,12,13,14]. In our study, we included 30 pediatric patients who underwent prolonged MV and assessed the feasibility of measuring three diaphragmatic ultrasound indices (DE, DTF and TPIA) as well as lung ultrasound score during SBT to predict MV weaning success.
Clinically our data showed similar results to what was presented in some of the previous studies where MV duration was significantly longer in the weaning failure group [1, 7, 11] with other studies showed no significant correlation between MV duration and weaning success [10, 12,13,14].
Regarding diaphragmatic US, DE was a significant predictor of weaning success in our study which agrees with most studies done in adults [9]. However, this is not the case in pediatric studies as only Abdel Rahman et al. [7] found significant association between DE and weaning outcome albeit only in Infants’ age group, while Xue et al. [1] found no significant correlation. Our DE cutoff values were different values than those of Abdel Rahman et al. [7]. However, their right DE cutoff value was 6.5 mm ours was 4.1 mm while their left DE cutoff value was 6.1 mm ours was 5.5 mm.
We did not find a significant correlation between DTF and weaning outcome. DTF significance in recent literature is controversial, while most adult studies consensus that it is a significant predictor [9], a recent large multicenter study found no association between DTF and weaning outcome [15]. While in pediatric studies the disagreement increases, as four earlier studies have found significant association [1, 2, 7, 12] while another more recent four studies did not. [10, 11, 13, 14]. The differences between the results of various studies could be attributed to multiple heterogenicities between them; first of which is the duration of the SBT and the exact time of acquiring the US measurement during it, where a longer SBT (As was imposed by our PICU team-up to 12 h) enables the diaphragm to regain its function before extubation. SBT duration by Xue et al. [1] was 30 min, by Abdel Rahman et al. [7] was 30–120 min and by Duyndam et al. [13] was 120 min, while the rest of the studies did not specify the exact duration of the SBT. Acquiring the US measurements at the end of a long SBT will lead to different measurements than acquiring it at the beginning. The second heterogenicity is caused by the difference in measurement technique, where some studies measured in B-mode and others measured in M-mode. Most studies were measured from the mid-point of the pleural echogenic line to the mid-point of the peritoneum echogenic line, while other studies were included only the hypoechoic muscle layer [1, 10]. The prevailing agreement now suggests measuring only the muscle contained within the pleura and peritoneum, a perspective that was not available to us when we commenced our research. This is due to the biological activity of membranes, where mechanical forces associated with ventilation could potentially trigger inflammation, leading to tissue remodeling and thickening. Such tissue remodeling may have contributed to fluctuations in the size and thickness of the diaphragm [13]. Differences in the patient posture, sedation protocol and SBT ventilator settings are also a major source of heterogenicities between the studies.
It should be noted that all the studies that have found no significant association between DTF and weaning outcome have found significant association between MV and diaphragmatic atrophy as well as decrease in DTF, proving that VIDD is an entity that needs to be further investigated in how to measure it and prevent it [10, 11, 13, 14].
TPIA was a parameter proposed by Theerawit et al. [6] in adults and has found that longer TPIA correlated with successful weaning. It had also strong association with RSBI, suggesting that TPIA could be an indicator for diaphragmatic strength. However, in our study we found no association between TPIA and weaning outcome. This could be attributed to the difference in SBT protocol as well as anatomical or physiological differences between adult and children that impact respiratory mechanics and the fact that weaning failure may be secondary to pathologies other than VIDD.
We were only able to measure DE and TPIA in 56.7% (17 out of 30) of the left diaphragms using the microconvex probe. This was due to inability to visualize the left diaphragm due to the smaller acoustic window offered by the spleen as compared to the liver on the right side and masking by intestinal gases. Nonetheless, we should state that we were able to visualize the left diaphragm motion in all patients by changing the probe position and placing it cranio-caudally in mid axillary or posterior axillary line, yet this will place the diaphragmatic motion at 90° to the US beam rendering M-mode ineffective in measuring the DE or TPIA. Most of the studies examined only the right diaphragm [1, 2, 10,11,12,13,14] depending on data from multiple previous studies, showing that there was significant difference regarding both sides in their US measurements [8]. Even so, we do recommend examining the left diaphragm in any available view primarily to exclude the absence of diaphragmatic motility or the presence of severe diaphragmatic dysfunction.
This study had multiple limitations. First of which is the smaller sample size that included all pediatric population. We do recommend further studies to include larger sample with stratification of pediatric population into infants, children and adolescent age groups. Secondly, we did not fix the time of US examination during our relatively long SBT which could have led to heterogeneous data. Finally, while diaphragm muscle strength is the focus of the current study, it is worth noting that diaphragmatic endurance also holds significance in the weaning from MV. Consequently, examining indicators like the diaphragmatic time-tension index alongside others could provide insights into how diaphragmatic endurance relates to the success of weaning.
Conclusion
We have found that DE is a predictor of weaning success while DTF and diaphragmatic TPIA had no correlation with weaning outcome. Further studies should be done using standardized weaning protocol and US examination time as well as investigate other measurements assessing diaphragmatic endurance.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- DE:
-
Diaphragmatic excursion
- DTF:
-
Diaphragmatic thickening fraction
- FiO2 :
-
Fraction of inspired oxygen
- MV:
-
Mechanical ventilation
- NIV:
-
Noninvasive ventilation
- PaO2 :
-
Partial pressure of arterial oxygen
- PEEP:
-
Positive end-expiratory pressure
- PICU:
-
Pediatric intensive care unit
- RSBI:
-
Rapid shallow breathing index
- SBT:
-
Spontaneous breathing trial
- TPIA:
-
Time to peak inspiratory amplitude
- US:
-
Ultrasound
- VIDD:
-
Ventilator-induced diaphragmatic dysfunction
References
Xue Y, Zhang Z, Sheng CQ, Li YM, Jia FY (2019) The predictive value of diaphragm ultrasound for weaning outcomes in critically ill children. BMC Pulm Med 19(1):1–8. https://doi.org/10.1186/s12890-019-1034-0
Lee EP, Hsia SH, Hsiao HF, Chen MC, Lin JJ, Chan OW, Lin CY, Yang MC, Liao SL, Lai SH (2017) Evaluation of diaphragmatic function in mechanically ventilated children: an ultrasound study. PLoS ONE 12(8):1–11. https://doi.org/10.1371/journal.pone.0183560
Singh N, McNally MJ, Darnall RA (2018) Does diaphragmatic electrical activity in preterm infants predict extubation success. Respir Care 63(2):203–207. https://doi.org/10.4187/RESPCARE.05539
Llamas-Álvarez AM, Tenza-Lozano EM, Latour-Pérez J (2017) Diaphragm and lung ultrasound to predict weaning outcome: systematic review and meta-analysis. Chest 152(6):1140–1150. https://doi.org/10.1016/j.chest.2017.08.028
Glau CL, Conlon TW, Himebauch AS, Yehya N, Weiss SL, Berg RA, Nishisaki A (2018) Progressive diaphragm atrophy in pediatric acute respiratory failure. Pediatr Crit Care Med 19(5):406–411. https://doi.org/10.1097/PCC.0000000000001485
Theerawit P, Eksombatchai D, Sutherasan Y, Suwatanapongched T, Kiatboonsri C, Kiatboonsri S (2018) Diaphragmatic parameters by ultrasonography for predicting weaning outcomes. BMC Pulm Med 18(1):1–11. https://doi.org/10.1186/s12890-018-0739-9
Abdel Rahman DA, Saber S, El-Maghraby A (2020) Diaphragm and lung ultrasound indices in prediction of outcome of weaning from mechanical ventilation in pediatric intensive care unit. Indian J Pediatr 87(6):413–420. https://doi.org/10.1007/s12098-019-03177-y
Weber MD, Lim JKB, Glau C, Conlon T, James R, Lee JH (2021) A narrative review of diaphragmatic ultrasound in pediatric critical care. Pediatr Pulmonol 56(8):2471–2483. https://doi.org/10.1002/ppul.25518
Parada-Gereda HM, Tibaduiza AL, Rico-Mendoza A, Molano-Franco D, Nieto VH, Arias-Ortiz WA, Perez-Terán P, Masclans JR (2023) Effectiveness of diaphragmatic ultrasound as a predictor of successful weaning from mechanical ventilation: a systematic review and meta-analysis. Crit Care 27(1):174. https://doi.org/10.1186/s13054-023-04430-9
Mistri S, Dhochak N, Jana M, Jat KR, Sankar J, Kabra SK, Lodha R (2020) Diaphragmatic atrophy and dysfunction in critically ill mechanically ventilated children. Pediatr Pulmonol 55(12):3457–3464. https://doi.org/10.1002/ppul.25076
Vadivelu S, Khera D, Choudhary B, Toteja N, Sureka B, Singh K, Singh S (2023) Evaluation of diaphragmatic thickness and dysfunction by ultrasonography in mechanically ventilated children for assessment of extubation success. Indian Pediatr 60(3):212–216
Shah AJ, Wai K, Sharron MP, Mize M, Cohen J, Basu S (2022) Diaphragmatic thickening fraction by ultrasound in mechanically ventilated pediatric patients: pilot observations during spontaneous breathing trials. J Ultrasound Med 41(12):3043–3050. https://doi.org/10.1002/jum.16035
Duyndam A, Smit J, Houmes RJ, Heunks L, Molinger J, IJland M, van Rosmalen J, van Dijk M, Tibboel D, Ista E (2023) No association between thickening fraction of the diaphragm and extubation success in ventilated children. Front Pediatr. https://doi.org/10.3389/fped.2023.1147309
Montoro DV, García Soler P, Hernández Yuste A, Camacho Alonso JM (2021) Ultrasound assessment of ventilator-induced diaphragmatic dysfunction in mechanically ventilated pediatric patients. Paediatr Respir Rev 40:58–64. https://doi.org/10.1016/j.prrv.2020.12.002
Vivier E, Muller M, Putegnat J-B, Steyer J, Barrau S, Boissier F, Bourdin G, Mekontso-Dessap A, Levrat A, Pommier C, Thille AW (2019) Inability of diaphragm ultrasound to predict extubation failure. Chest 155(6):1131–1139. https://doi.org/10.1016/j.chest.2019.03.004
Acknowledgements
Not applicable.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by AME, AMA, NMO, SMM and GEE. The first draft of the manuscript was written by AME. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethical committee of Faculty of Medicine, Ain Shams University (FMASU REC) under Federal wide assurance No. FWA00017585 (FMASU MD 94/2021).
Consent for publication
Identifying information about participants (patients’ identity) did not appear in any part of the manuscript; therefore, consent for publication was not required.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Eskander, A.M., Abd-Elhameed, A.M., Osman, N.M. et al. Role of diaphragmatic ultrasound in predicting weaning success from mechanical ventilation in pediatric intensive care unit. Egypt J Radiol Nucl Med 55, 114 (2024). https://doi.org/10.1186/s43055-024-01285-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-024-01285-0