
Abstract
Background
Carbapenem resistant Enterobacterales (CRE) is on the rise globally, triggering a significant health threat and a substantial concern for infection control management. We aimed to detect and characterize carbapenemases producing Enterobacterales (CPE) clinical isolates over a period of nearly one-year duration in Theodor Bilharz Research Institute, a tertiary care hospital in Egypt through molecular and phenotypic methods using carbapenemase detection combination inhibitor disk set (Enterobacterales) MASTDISCS ID (MDI) (MAST, UK), with the addition of temocillin disk.
Results
CRE represented 6.5% of Enterobacterales. Healthcare-associated infections were frequently high representing 87% of the CRE isolated from hospitalized patients. Most of the CRE isolates were Klebsiella pneumonia (68%) followed by Escherichia coli (22%), Enterobacter cloacae (4%), Serratia marcescens (4%) and Citrobacter freundii (2%). Phenotypic detection revealed metallo-β lactamases in 84% of isolates, followed by oxacillinase-48 {(OXA-48) 6%} and Klebsiella pneumoniae carbapenemase in 2% of the isolates. The most prevalent gene detected by conventional PCR was blaNDM (84%) followed by blaOXA-48 (6%) and blaKPC (2%). Excellent agreement was found between PCR and MDI for detection of carbapenemase production.
Conclusions
NDM carbapenemase is prevalent in our hospital. Carbapenemase detection combination inhibitor disk set (Enterobacterales) MASTDISCS ID is a useful tool for rapid and precise confirmation of the detection of CPE.
Similar content being viewed by others


1 Background
Carbapenem-resistant Enterobacterales (CRE) is a worldwide urgent public health concern, causing serious outbreaks [1]. Resistance to carbapenems, the drugs of choice used for treatment of multi-drug resistant (MDR) bacterial strains, renders CRE as one of the biggest health challenges as it results in further limitation in therapeutic options and i increased likelihood of morbidity and mortality [2, 3].
Resistance to carbapenems among Enterobacterales isolates is predominantly attributed to carbapenemases; a diverse group of enzymes that possess carbapenem hydrolyzing activity with varying levels of carbapenem resistance [4]. Carbapenemases may confer resistance to nearly all β-lactams, and are readily transferable as they are mostly encoded by highly transferable plasmids [5]. Carbapenemases belong to one of three classes of β-lactamases, class A as Klebsiella pneumoniae carbapenemases (KPCs), class B metallo β-lactamases (MβLs) including NDM, IMP, and VIM, and class D with oxacillinases (OXAs) carbapenemases such as OXA-23 and OXA-48 [6]. Recognizing the mechanism of carbapenem resistance is crucial in choosing the most effective antimicrobial treatment and the appropriate infection control method. Although molecular identification of carbapenemase genes is the gold standard [7], rapid diagnostic phenotypic tests are extremely valuable and economic to be used routinely in reducing length and/or cost of hospitalization especially in the intensive care units and could detect the un-expressed genes [8].
This work aimed to detect and characterize carbapenemases producing Enterobacterales (CPE) clinical isolates over a period of nearly one-year duration in Theodor Bilharz Research Institute (TBRI), a tertiary care hospital in Egypt through molecular and phenotypic methods.
2 Methodology
2.1 Sample collection, bacterial identification and antimicrobial susceptibility testing
Fifty (50) CRE isolates out of a total of 775 Enterobacterales isolates were obtained from various clinical samples received and handled in the Microbiology Laboratory of TBRI, during the study period from June 2018 to July 2019.
2.1.1 Identification of bacterial isolates to the genus and species level
Bacterial isolates were identified preliminary by conventional methods and API 20E (BioMérieux, France), and then identification and antimicrobial susceptibility testing (AST) were confirmed using VITEK2 Compact System (BioMérieux, France).
Following the Epidemiological cut-off breakpoints (ECOFFs) recommended by the European Committee on Antimicrobial Susceptibility Testing (EUCAST) on detection of resistance mechanisms in CRE using Kirby Bauer disk diffusion method; Enterobacterales isolates that showed zone diameter < 25 mm for meropenem (MEM) (10 μg) and/or ertapenem (ERT) (10 μg) and/or < 23 mm for imipenem (IPM) (10 μg) were considered carbapenem resistant and used for subsequent investigations [9].
The CRE isolates were stored at − 70 °C as recommended until further phenotypic and genotypic carbapenemase production confirmatory tests were done [10].
All isolates included in the study were archived, and codes were used instead of patient names. The protocol of the study was approved by TBRI Research Ethics Committee (TBRI-REC) under Federal Wide Assurance (FWA00010609) and the work has been carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for Experiments in Humans and its later amendments (GCP guidelines) or comparable ethical standards.
2.2 Phenotypic detection of carbapenemase activity
2.2.1 Combination disk test
Fifty CRE isolates; detected by Kirby Bauer and VITEK2 Compact system; were subjected to carbapenemase detection combination inhibitor disk set (Enterobacterales) (MDI) (MAST, UK). The test was performed according to manufacturer’s instructions. Four disks were included: disk A, containing meropenem (10 μg); disk B, consisting of meropenem (10 μg) and an MBL inhibitor; disk C, consisting of meropenem (10 μg) with a KPC inhibitor; and disk D, containing meropenem (10 μg) with an Amp C inhibitor. The interpretation of the test was as follows; the zone of inhibition of disk A is compared to the zones of inhibition of each of disks B, C, and D. If disk B shows a zone difference of ≥ 5 mm from disk A, the organism is considered as MBL producer. If disk C shows a zone difference of ≥ 4 mm from disk A, the organism is considered having KPC activity. If disk C and disk D both show a zone difference of ≥ 5 mm from disk A, the organism is considered as Amp C producer coupled with porin loss mechanism [9].
2.2.2 Detection of OXA-48
OXA-48 carbapenemase resistance was detected using Temocillin disk (30 μg). The temocillin zone diameter was only interpreted if no significant zone difference was observed with disks B, C or D. Isolates in which temocillin zone diameter ≤ 10 mm were considered OXA-48 carbapenemase positive [9, 11].
2.3 Genotypic detection of carbapenemase-encoded genes using conventional polymerase chain reaction (PCR) assay
Bacterial DNA was extracted from fresh overnight cultures by the boiling method; five colonies were added to 200 μl of sterile distilled water and boiled for 5 min, followed by centrifugation for 2 min at 8000 rpm. Supernatants were stored in duplicate copies at − 20 °C for further use [12]. PCR was performed for the following carbapenemase-encoding genes (blaKPC, blaNDM, blaVIM blaIMP and blaOXA-48 genes). Primers used in PCR assay are listed in (Table 1).
The PCR assay was performed as previously described by [13]. Briefly 2μL of extracted DNA was added to PCR reaction mixture (final volume of 50 μL) consisting of: 25 µl Maxima hot start green (ThermoScientific, USA), 22 µl nuclease free water (ThermoScientific, USA), 0.5 µl forward primer, 0.5 µl reverse primer. PCR amplifications were carried out in a T-personal PCR Thermal Cycler (Biometra, Uk) with the following PCR protocol; initial activation at 94 °C for 10 min, denaturation: 94 °C for 30 s., annealing at 52 °C for 50 s., extension at 72 °C for 50 s. Denaturation, annealing and extension steps were repeated for 30 successive cycles that were finally followed by a maintenance temperature of 4 °C.
Each PCR end-product was analyzed using a 1.5% agarose (Promega, USA) gel containing 0.5 μg/μl Ethidium Bromide (Promega, USA). The gel was electrophoresed in 1 × TBE buffer (Sigma, USA) at 120 V for 60 min in an electrophoreses system (Cleaver Scientific, UK). A 100 bp ladder (Promega, USA) was used as a molecular size marker. DNA bands were visualized with a gel documentation system (Bio-Rad, USA).
3 Results
Fifty (50) CRE isolates were identified out of 775 Enterobacterales isolates recovered from different clinical samples such as urine (n = 433), sputum (n = 96), wound swab (n = 108), blood (n = 97), ascitic fluid (n = 41). CRE isolates represented 6.5% of the isolated Enterobacterales. Most of the CRE isolates were obtained from the inpatients representing (46/50; 92%) while the outpatients represented (4/50; 8%).
Health-care associated CRE infections were 40/46 representing 87%, while community acquired infections were 6/46 representing 13% of infections caused by CRE isolates during the study period. The CRE healthcare-associated infections were mostly recovered from the ICU and the Urology Departments (12/46 each) each representing 26% from the 46 CRE isolates that were recovered from different hospital departments.
Most of CRE isolates were K. pneumoniae (34/50; 68%) followed by E. coli (11/50; 22%), E. cloacae (2/50; 4%), S. marcescens (2/50; 4%) and C. freundii (1/50; 2%).
MID set with the addition of a temocillin disk confirmed carbapenemase production in 92% (46/50) of the 50 tested CRE isolates. MBL represented the main class (42/50; 84%) (Fig. 1a) followed by OXA-48 (3/50; 6%) (Fig. 1b) and KPC (1/50; 2%) (Fig. 1c). Two isolates (2/50; 4%) had an Amp C activity (Fig. 1d) and two isolates (2/50; 4%) revealed a non-conclusive result (Fig. 1e).

a Confirmation of carbapenemase production through expression of MBL activity detected by the combination test: A carbapenem resistant isolate showing > 5 mm difference in zone diameter between disk A (meropenem 10 µg) and disk B (meropenem 10 µg + MBL inhibitor) indicating MBL activity. b Confirmation of carbapenemase production through expression of OXA-48 activity detected by the combination test: A carbapenem resistant isolate showing resistance to T (temocillin30 µg) disk &no significant zone difference was observed between disk A (meropenem 10µ) and disks B (meropenem 10 µg + MBL inhibitor), C (meropenem 10 µg + KPC inhibitor) or D (meropenem 10 µg + AmpC inhibitor) indicating OXA-48 activity. c Confirmation of carbapenemase production through expression of KPC activity detected by the combination test: A carbapenem resistant isolate showing > 4 mm difference in zone diameter between disk A (meropenem 10µg) and disk C (meropenem 10 µg + KPC inhibitor) indicating KPC activity. d Amp C activity detected by the combination test: A carbapenem resistant isolate in which both C (meropenem 10 µg + KPC inhibitor) and D (meropenem 10 µg + AmpC inhibitor) disks show significant zone differences (≥ 4 mm and ≥ 5 mm respectively) compared to disk A (meropenem 10 µg) while the zone difference between disks B (meropenem 10 µg + MBL inhibitor) and A (meropenem 10 µg) is less than 4 mm (B-A < 4 mm) indicating Amp-C activity. e Non-conclusive result by the combination test: A carbapenem resistant isolate in which a non-conclusive result was detected. Disk A: meropenem 10 µg, disk B: meropenem 10 µg + MBL inhibitor, disk C: meropenem 10 µg + KPC inhibitor, disk D: meropenem 10 µg + AmpC inhibitor, disk T: temocillin disk 30 µg.
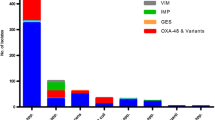
By applying conventional PCR to detect blaKPC, blaNDM, blaOXA–48, blaVIM and blaIMP genes in the isolates, 46 isolates harbored carbapenemase gene; blaNDM gene showed the highest percentage (92%) (Fig. 2) followed by blaOXA-48 (6%) (Fig. 3) and blaKPC (2%). Isolates harboring more than one carbapenem resistant gene, as well as blaVIM and blaIMP weren’t detected in any of the tested isolates.

Agarose gel electrophoresis of PCR products of Enterobacterales blaNDM positive gene (621 bp). Lane 1: Molecular weight marker (ladder 100 bp). Lane 2: Negative control. Lane 3: Positive control. Lane (4–18): Positive DNA samples. The arrow points to blaNDM PCR amplification product

Agarose gel electrophoresis of PCR products of Enterobacterales blaOXA-48 positive gene (438 bp). Lane 1: Molecular weight marker (ladder 100 bp). Lane 2: Negative control. Lane 3: Positive control. Lane (4, 5, 6): Positive DNA samples. The arrow points to blaOXA-48 PCR amplification product
Phenotypic combination carbapenemase detection disk test MASTDISCS ID (MDI) set with the addition of a temocillin disk showed 100% sensitivity and specificity with all tested genes in comparison to PCR assay as the gold standard method.
3.1 Statistical methods
Results were expressed as number (%). Comparison between categorical data was done using Chi Square test. Agreement between different methods of detection was done using kappa coefficient test. Diagnostic indices (sensitivity, specificity, positive, negative and efficacy) was performed according to Statistical Package for Social Sciences (SPSS) version 21. P values < 0.05 were considered significant and < 0.01 was considered highly significant.
4 Discussion
CRE has been disseminated and recognized globally causing serious hospital and community acquired infections, with significant limitation in treatment options. Carbapenemase production is the most common cause of carbapenem resistance [16] and therapy differs according to the type of β-Lactamases produced [17]. Rapid identification by simple methods is therefore crucial and allows for timely approaches in prevention and applying prevention control measures. Therefore, we aimed to detect and characterize CPE clinical isolates through molecular and phenotypic methods.
It has been established that CRE transmission is much more common in healthcare care facilities than in community [3, 18]. Therefore, it is obvious that most of the CRE isolates in the current study (87%) were obtained mainly from inpatients rather than from outpatients (13%). CRE isolates were chiefly recovered from ICU and Urology Departments being 26% in each, as patients are more prone to intense therapy regimens and invasive procedures. This is consistent with findings from Menoufia University Hospitals, Egypt, in which highest rate of CRE (32.5%) was obtained from hospital ICU [19]. Similarly, Kotb and colleagues [3] reported that CRE formed 54.1% of hospital acquired infections (HAI) in ICU cases. This drives more attention to antimicrobial and infection control policies implemented in ICUs.
The prevalence rate of carbapenem resistance among Enterobacterales in our hospital located in Giza Governorate was 6.5% compared to 19.9% in Sohag in the South [20]. Higher rates (40%) were detected in Benha [21] and Tanta cities (62.7%) [22] located to the north of Cairo. In Ismailia Governorate in the North-East of Cairo CRE rate was 34.1% [23]. Such variation in CRE rates could be attributed to differences in geographic distribution, specimen type, the causative pathogen, location prior to admission, length of stay in hospital and ICU stay, and most importantly to antibiotic policies used in different health care settings. Broad spectrum antibiotics aid in the selection for antimicrobial resistance by selective pressures, leading to higher prevalence of CRE. On the other hand, strict implementation of infection control measures and better selection of antibiotic policies may lead to lower CRE rates [24].
Comparable results were detected from Kuwait hospitals as 8% of isolates were CRE detected from different clinical samples [25]. In a study done by Zowawi et al. [26] Enterobacterales isolates collected from six participating institutes across the Gulf Corporate Council countries, (Saudi Arabia, United Arab Emirates, Kuwait, Qatar, Oman and Bahrain) showed that CRE prevalence was 15%. In North African countries, 11.4% CRE isolates were recovered from Tunisia and Libya [27].
Both K. pneumoniae and E. coli were the most prevalent CRE in the studied isolates (68%, 22% respectively) and comparable results in Egypt (51.4 K. pneumoniae and 28.6% E. coli) were found by [20]. El-Kholy and colleagues [28] revealed that the former pathogens were the mostly detected among their multi drug resistant (MDR) isolates.
The EUCAST recommended the combination disk test to identify and differentiate carbapenemases in Enterobacterales using zone size comparison of combined disks, incorporating specific enzyme inhibitors [9]. MDI set with an added temocillin disk showed 100% sensitivity and revealed that MBL was the dominating carbapenemase (84%), followed by OXA-48 (6%). Previous Egyptian study by Shaker et al. [29] using the same confirmatory detection set, showed that MBLs rate (82%) were comparable to ours (84%) although OXA-48 was the predominant enzyme (96%). A study previously done in Alexandria Main University Hospital (AMUH) revealed that 70% of their CRE isolates tested by carbapenemase production phenotypic tests were metallo- β Lactamase producing CRE of which NDM formed 67.5% [30].
The studied carbapenem resistance genes were detected by conventional PCR assay in 92% of the studied isolates. Interestingly, bla NDM producers prevailed among the isolates (84%) followed by blaOXA-48 (6%) and blaKPC (2%), blaVIM and blaIMP carbapenemase genes couldn’t be determined in any of the studied strains. In Egypt bla NDM was first detected in 2013 [31], but outbreaks of NDM were uncommon. Few recent studies reported that NDM is starting to predominate carbapenemase genes. Shawky et al. [32] reported that 75% of the isolates included in their study in Al Kasr AL-Ainy hospital, Egypt showed that the highest prevalence of carbapenemase encoded genes were blaNDM followed by blaOXA-48 (59%). In addition, Gamal and colleagues [33] confirmed the emerging threat of NDM variants dissemination in carbapenem resistant K. pneumoniae (CRKP) in 94% of the studied isolates. In addition, bla NDM was the most recognized carbapenemase genotype (68.88%) followed by blaOXA- 48 (32.59%) in cancer institutes in Egypt [34]. On the contrary, Shaker et al. [29] revealed that blaOXA- 48 gene showed the highest percentage of prevalence (96%) followed by bla VIM, blaNDM, blaKPC, and blaIMP in which they represented 94%, 54%, 46% and 40%, respectively, El-Kholy et al. [28] also showed that blaOXA-48 was the dominating (40.6%) carbapenem resistance gene, followed by blaNDM1 (23.7%) and blaOXA-232 (4.5%). NDM carbapenemase is considered a global health threat due to its ongoing worldwide dissemination and being linked to hospital recent outbreaks [35]. A recent review by El-Kholy and colleagues in Egypt reported that NDM and oxacillin carbapenemase 48 (OXA-48) genes were the most prevalent in Enterobacterales reaching 26.04–68.88% and 30–58.62%, respectively [36].
In Kuwait [25] reported that bla NDM was the most common carbapenem resistant gene detected (34%) in Enterobacterales strains, collected from four governmental hospitals in Kuwait. Also, Perovic et al. [37] stated that bla NDM was the most common detected carbapenemase producing gene in Enterobacterales strains (59%) collected from National Health Laboratory Service in South Africa, followed by blaOXA-48 (29%) then blaKPC (1%).
Dominance of the blaNDM in the current study and other studies from the Middle-East may be attributed to the existence of favorable conditions, such as dense populations, neglected hygienic practices, high selective pressure caused by the irrational antibiotic use and increased migration especially from the Indian continent [38]. In addition, strains carrying NDM gene are frequently MDR, as the plasmid which carry the NDM gene also carries resistance genes against aminoglycosides, macrolides and sulphamethoxazole, which leaves very few therapeutic options [39].
Rapid diagnostics in routine Laboratoy work are promptly required to detect MDR bacteria including carbapenemases with reliable sensitivity and specificity. Using MDI inhibitor set (Enteobacterales) with the addition of a temocillin disk in this study, showed 100% sensitivity and specificity with all tested genes in comparison to PCR assay as the gold standard method. Comparable results were obtained by Morsi [40] at Zagazig University Hospitals as the test showed 100% sensitivity and 88.9% specificity for bla OXA-48, bla NDM bla IMP, bla VIM and bla KPC.
The predominant carbapenemase in our study was blaNDM unlike that previously detected by Shaker and colleagues [29] as blaOXA-48 was the main carbapenemase. In addition, the sensitivity and specificity of the test for whole carbapenemases were 82.1% and 70% respectively. The predominance of the weak OXA-48 in the previous study, may have lowered the specificity for the temocillin disk as well as the specificity of combined use of temocillin disk (50%) as it was often missed in detection. This difference in carbapenemase types has major clinical outcome that completely alters therapeutic options to patients, as with OXA-48 we still may use carbapnemes in high concentration and over prolonged infusion period or we may use the novel expensive antimicrobial available now in Egypt; ceftazidime/avibactam which on the contrary will not be effective against NDM-producing isolates and mandates the usage of colistin combination therapy with all its known side effects. Recent studies stated that NDM is the predominant carbapenemase in contrast to previous older studies indicating continuous and expected change of the type of prevalent carbapenemase reported over the time within each country and region [41, 42]. Previously, OXA-48 was the predominant carbapenemase in Egypt until few years ago where metallo beta- lactamases took the upper hand, as in our work.
5 Conclusion
As the use of carbapenems has significantly increased over time in our region, it is associated with increased incidence of CRE. The prevalent NDM carbapenemase in our hospital, with its high tendency to disseminate, represents a threatening health issue. The carbapenemase detection combination inhibitor disk set (Enterobacterales) MASTDISCS ID (MID) is a useful tool for rapid and precise confirmation of the diagnosis of CPE. Effective antimicrobial stewardship strategy and infection control measures are urgently required to slow down the dissemination of these CRE isolates.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- CRE:
-
Carbapenem resistant Enterobacterales
- MDR:
-
Multi-drug resistance
- KPC:
-
Klebsiella pneumoniae Carbapenemase
- MβLs:
-
Metallo β-lactamases
- OXAs:
-
Oxacillinases
- OXA-23:
-
Oxacillinase-23
- OXA-48:
-
Oxacillinase-48
- CPE:
-
Carbapenemases producing Enterobacterales
- TBRI:
-
Theodor Bilharz Research Institute
- AST:
-
Antimicrobial susceptibility testing
- ECOFFs:
-
Epidemiological cut-off breakpoints
- EUCAST:
-
European Committee on Antimicrobial Susceptibility Testing
- MEM:
-
Meropenem
- ERT:
-
Ertapenem
- IPM:
-
Imipenem
- TBRI-REC:
-
Theodor Bilharz Research Institute Research Ethics Committee
- MDI set:
-
Mast discs combination detection inhibitor set
- PCR:
-
Polymerase chain reaction
- ICU:
-
Intensive Care Unit
- K. pneumonia :
-
Klebsiella pneumonia
- E. coli :
-
Escherichia coli
- E. cloacae :
-
Enterobacter cloacae
- S. marcescens :
-
Serratia marcescens
- C. freundii :
-
Citrobacter freundii
- MASTDISCS ID:
-
Mast discs detection inhibitor
- CRKP:
-
Carbapenem resistant Klebsiella pneumoniae
References
Jean S-S, Lee N-Y, Tang H-J, Lu M-C, Ko W-C, Hsueh (2018) Carbapenem-resistant Enterobacteriaceae infections: Taiwan aspects. Front Microbiol 9:2888. https://doi.org/10.3389/Ffmicb.2018.02888
Van Loon K, Voor in‘t holt AF, Vos MC (2018) A systematic review and meta-analyses of the clinical epidemiology of carbapenem resistant Enterobacteriaceae. Antimicrob Agents Chemother 62:e01730-17. https://doi.org/10.1128/aac.01730-17
Kotb S, Lyman M, Ismail G, Abd El Fattah M, Girgis S, Etman A et al (2020) Epidemiology of Carbapenem-resistant Enterobacteriaceae in Egyptian intensive care units using National Healthcare-associated Infections Surveillance Data, 2011–2017. Antimicrob Resist Infect Control 9:2. https://doi.org/10.1186/s13756-019-0639-7
Sheu CC, Chang YT, Lin SY, Chen YH, Hsueh PR (2019) Infections caused by carbapenem-resistant Enterobacteriaceae: an update on therapeutic options. Front Microbiol 30(10):80. https://doi.org/10.3389/fmicb.2019.00080
Al-Zahrani I, Alasiri B (2018) The emergence of carbapenem-resistant Klebsiella pneumoniae isolates producing OXA-48 and NDM in the Southern (Asir) province, Saudi Arabia. Saudi Med J 39(1):23–30. https://doi.org/10.15537/smj.2018.1.21094
Bandari N, Keyvani H, Zargar M, Talebi M, Zolfaghari M (2020) Epidemiological and genetic overview of the Klebsiella pneumoniae Carbapenemases (KPCs) in K. pneumoniae Isolated from the clinical samples in Iran. Intern J. Adv Biol Biomed Res (IJABBR) 8(1):75–85. https://doi.org/10.33945/SAMI/IJABBR.2020.1.8
Kamel NA, El-tayeb WN, El-Ansary MR, MansourMT AKM (2018) Phenotypic screening and molecular characterization of carbapenemase-producing Gram-negative bacilli recovered from febrile neutropenic pediatric cancer patients in Egypt. PLoS ONE 13(8):e0202119. https://doi.org/10.1371/journal.pone.0202119
Nordmann P, Poirel L (2019) Epidemiology and diagnostics of carbapenem resistance in gram-negative bacteria. Clin Infec Dis. 69(Suppl 7):S521–S528. https://doi.org/10.1093/cid/ciz824
EUCAST (2017) The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters, version 8.0. http://www.eucast.org/clinical_breakpoints/
Sambrook J, Fritsch EF, Maniatis T (1989) Bacterial media, antibiotics and bacterial strains. In: Zahlreiche S, editor. Molecular cloning, 2nd edn. Coldspring Harbor Laboratory Press, USA, p A5
Aguirre-Quiñonero A, Martínez-Martínez L (2017) Non-molecular detection of carbapenemases in Enterobacteriaceae clinical isolates. J Infect Chemother 23(1):1–11. https://doi.org/10.1016/j.jiac.2016.09.008
Higgins PG, Lehmann M, Wisplinghoff H, Harald S (2010) gyrB multiplex PCR to differentiate between Acinetobacter genomic species. J Clin Microbiol 48(12):4592–4594. https://doi.org/10.1128/FJCM.01765-10
Ashayeri-Panah M, Feizabadi MM, Eftekhar F (2014) Correlation of multi-drug resistance, integron and blaESBL gene carriage with genetic fingerprints of extended-spectrum β-lactamase producing Klebsiella pneumoniae. Jundishapur J Microbiol 7(2):e8747. https://doi.org/10.5812/Fjjm.8747
Gheorghe I, Czobor I, Chifiriuc MC, Borcan E, Ghita C, Banu O (2014) Molecular screening of carbapenemase-producing Gram negative strains in Romanian intensive care units during a one year survey. J Med Microbiol 63:1303–1310. https://doi.org/10.1099/jmm.0.074039-0
Poirel L, Potron A, Nordmann P (2012) OXA-48-like carbapenemases: the phantom menace. J Antimicrob Chemother 67:1597–1606. https://doi.org/10.1016/j.ijantimicag.2012.08.015
Dong L, Espinoza H, Espinoza J (2020) Emerging superbugs: the threat of carbapenem resistant Enterobacteriaceae. AIMS Microbiol 6(3):176–182. https://doi.org/10.3934/microbiol.2020012
Tilahun M, Kassa Y, Gedefie A, Ashagire M (2021) Emerging carbapenem-resistant Enterobacteriaceae infection, its epidemiology and novel treatment options: a review. Infect Drug Resist 14:4363–4374. https://doi.org/10.2147/IDR.S337611
Tamma P, Simner P (2018) Phenotypic detection of carbapenemase-producing organisms from clinical isolates. J Clin Microbiol 56(11):e01140-e1218. https://doi.org/10.1128/jcm.01140-18
Melake N, Mahmoud A, Elraghy N, Labib A, Hassan D, Elbrolosy A (2016) Detection of Klebsiella pneumoniae carbapenemases and metallo-β-lactamases among Klebsiella pneumoniae isolates from hospitalized patients at Menoufia University Hospitals, Egypt. Menoufia Med J 29(4):801–811. https://doi.org/10.4103/1110-2098.202524
Ali A, Mohamed T (2019) Detection and characterization of carbapenem resistant Enterobacteriaceae in Sohag University Hospitals. Eur Respir J. https://doi.org/10.1183/13993003.congress-2019.PA2905
El-Gazzar AM, Matta AM, Fouad NA, Azab MS (2016) Phenotypic and genotypic detection of Klebsiella pneumoniae carbapenemase and New Delhi metallo-β-lactamase of Enterobacteriaceae in Benha University Hospitals. Egypt J Med Microbiol 25:19–24
Amer WH, Khalil HS, Abd EL, Wahab MA (2016) Risk factors, phenotypic and genotypic characterization of carbapenem resistant Enterobacteriaceae in Tanta University Hospitals, Egypt. Int J Infect Control. https://doi.org/10.3396/ijic.v12i2.15905
Raheel A, Azab H, Hessam W, Abbadi S, Ezzat A (2020) Detection of carbapenemase enzymes and genes among carbapenem-resistant Enterobacteriaceae isolates in Suez Canal University Hospitals in Ismailia, Egypt. Microb Infec Dis 1(1):24–33. https://doi.org/10.21608/mid.2020.25702.1007
Murray JC, Ikuta KS, Sharara F, Swetschinski L, Aguilar GR, Gray A et al (2022) Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet 399(910325):629–655. https://doi.org/10.1016/S0140-6736(21)02724-0
Jamal WY, Albert MJ, Rotimi VO (2016) High Prevalence of New Delhi metallo-β-lactamase-1 (NDM-1) producers among carbapenem-resistant Enterobacteriaceae in Kuwait. PLoS ONE 11(3):e0152638. https://doi.org/10.1371/journal.pone.0152638
Zowawi HM, Sartor AL, Balkhy HH, Walsh TR, Al Johani SM, AlJindan RY et al (2014) Molecular characterization of carbapenemase-producing Escherichia coli and Klebsiella pneumoniae in the countries of the Gulf Cooperation Council: dominance of OXA-48 and NDM producers. Antimicrob Agents Chemother 58:3085–3090. https://doi.org/10.1128/aac.02050-13
Mathlouthi N, Al-Bayssari C, El Salabi A, Bakour S, Gwierif SB, Zorgani AA et al (2016) Carbapenemases and extended-spectrum β-lactamases producing Enterobacteriaceae isolated from Tunisian and Libyan hospitals. J Infect Dev Ctries 10(07):718–727. https://doi.org/10.3855/jidc.7426
El-Kholy AA, Girgis SA, Shetta MAF, Abdel-Hamid D, Elmanakhly A (2020) Molecular characterization of multidrug-resistant Gram-negative pathogens in three tertiary hospitals in Cairo, Egypt. Eur J Clin Microbiol Infect Dis 2020(39):987–992. https://doi.org/10.1007/s10096-020-03812-z
Shaker O, Gomaa H, ElMasry S, Abdel Halim R, Abdelrahman A, Kamal J (2018) Evaluation of combined use of temocillin disk and mastdisks inhibitor combination set against polymerase chain reaction for detection of carbapenem-resistant Enterobacteriaceae. Maced J Med Sci 6(2):242–247. https://doi.org/10.3889/oamjms.2018.090
El-Ghazzawy IF, Meheissen MA, Younis DA (2016) Phenotypic and genotypic methods for detection of metallo beta lactamases among carbapenem resistant Enterobacteriaceae clinical isolates in Alexandria Main University Hospital. Afr J Microbiol Res 10(1):32–40. https://doi.org/10.5897/AJMR2015.7821
Abdelaziz MO, Bonura C, Aleo A, Fasciana T, Mammina C (2013) NDM-1- and OXA-163-producing Klebsiella pneumoniae isolates in Cairo, Egypt, 2012. J Glob Antimicrob Resist 1(4):213–215. https://doi.org/10.1016/j.jgar.2013.06.003
Shawky AM, Tolba TM, Hamouda HM (2019) Emergence of New Delhi metallo beta lactamase blaNDM-1 and oxacillinases blaOXA-48 Producing Klebsiella pneumoniae in an Egyptian hospital. Egypt J Microbiol 54:25–37
Gamal D, Egea P, Elías C, Fernández-Martínez M, Causse M, Pérez-Nadales E, Salem D et al (2020) (2020): High-risk clones and novel sequence type ST4497 of Klebsiella pneumoniae clinical isolates producing different alleles of NDM-type and other carbapenemases from a single tertiary-care center in Egypt. Intern J Antimicrob Agents 56:106164. https://doi.org/10.1016/j.ijantimicag.2020.106164
Tawfick MM, Alshareef WA, Bendary HA, Elmahalawy H, Abdulall AK (2020) The emergence of carbapenemase blaNDM genotype among carbapenem-resistant Enterobacteriaceae isolates from Egyptian cancer patients. Eur J Clin Microbiol Infect Dis 39:1251–1259. https://doi.org/10.1007/s10096-020-03839-2
Mendes G, Ramalho JF, Duarte A, Pedrosa A, Silva AC, Méndez L, First CC (2022) Outbreak of NDM-1-producing Klebsiella pneumoniae ST11 in a Portuguese Hospital Centre during the COVID-19 pandemic. Microorganisms 10(2):251. https://doi.org/10.3390/microorganisms10020251
El-Kholy A, El-Mahallawy HA, Elsharnouby N, Abdel Aziz M, Helmy AM, Kotb R (2021) Landscape of multidrug-resistant gram-negative infections in Egypt: survey and literature review. Infect Drug Resist 24(14):1905–1920. https://doi.org/10.2147/idr.s298920
Perovic O, Britz E, Chetty V, Singh-Moodley A (2016) Molecular detection of carbapenemase-producing genes in referral Enterobacteriaceae in South Africa: a short report. S Afr Med J 106(10):975–977. https://doi.org/10.7196/samj.2016.v106i10.11300
Nordmann P, Poirel L (2014) The difficult-to-control spread of carbapenemase producers among Enterobacteriaceae worldwide. Clin Microbiol Infect 20(9):821–830. https://doi.org/10.1111/1469-0691.12719
Peterson E, Kaur P (2018) Antibiotic resistance mechanisms in bacteria: relationships between resistance determinants of antibiotic producers, environmental bacteria, and clinical pathogens. Front Microbiol. https://doi.org/10.3389/fmicb.2018.02928
Morsi S (2016) Comparative evaluation of phenotypic and genotypic methods for detection of carbapenemases in clinically significant Klebsiella pneumoniae isolates. Egyp J Med Microbiol 25(1):109–116
Abdelaziz NA (2022) Phenotype-genotype correlations among carbapenem-resistant Enterobacterales recovered from four Egyptian hospitals with the report of SPM carbapenemase. Antimicrob Resist Infect Control 11(1):13. https://doi.org/10.1186/Fs13756-022-01061-7
Elrahem AA, El-Mashad N, Elshaer M, Ramadan H, Damiani G, Bahgat M et al (2023) Carbapenem resistance in gram-negative bacteria: a hospital-based study in Egypt. Medicina 59(2):285. https://doi.org/10.3390/medicina59020285
Acknowledgements
Not applicable.
Funding
This work was supported by Theodor Bilharz Research Institute (TBRI) as a part of an internal project No. 99D [Detection of Carbapenemase-Producing Enterobacterales (CPE) in Infected and Colonized Carriers.]
Author information
Authors and Affiliations
Contributions
EI is the PI of TBRI internal project 99D; from which this study aroused. EI and DM designed the study, supervised all the work, and contributed in the analysis of the results. SD and GD Contributed in the research work, supervised of technical work, and analyzed the data. SD is a major contributor in writing and revising the manuscript. AG performed laboratory work, interpreted the results, and performed statistical analyses. EE supervised the molecular work and contributed in data analysis. AAS and SM supervised all the work and contributed in data analysis. All authors critically revised the manuscript, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All specimens included in the study were archived, and codes were used instead of patient names. The protocol of the study was approved by TBRI Research Ethics Committee (TBRI-REC) under Federal Wide Assurance (FWA00010609) and the work has been carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for Experiments in Humans and its later amendments (GCP guidelines) or comparable ethical standards.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El Defrawy, I., Salem, D., Ali, G. et al. Carbapenemase producing Enterobacterales clinical isolates from a tertiary care hospital in Egypt. Beni-Suef Univ J Basic Appl Sci 12, 98 (2023). https://doi.org/10.1186/s43088-023-00437-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43088-023-00437-x