
Abstract
Background
Automatic tube compensation (ATC) is one of the newer weaning modes that seem promising to improve the weaning process.
Objective
To evaluate the benefit of ATC in hastening and improving the weaning process.
Patients and methods
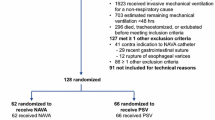
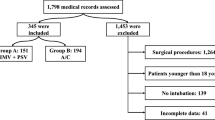
In a prospective randomized-controlled trial, all eligible patients of Assiut Chest Department who were mechanically ventilated were included during the period from April 2010 to March 2012. They were divided into two groups, 88 patients weaned by pressure support ventilation (PSV) and 78 patients weaned by ATC. The primary outcomes measure was the ability to maintain spontaneous breathing for more than 48 h after extubation and weaning duration.
Results
A total of 166 patients were included; the mean age was 58.6 ± 12.3 years; males represented 70%. The weaning duration was shorter in ATC than in PSV (19.7 vs. 29.9 h, respectively). Also, ATC had a higher trend toward successful extubation than PSV (88.5 vs. 78.4%). Patients who underwent weaning by ATC had a nonsignificant trend toward simple weaning. Moreover, hospital mortality was less in ATC (ATC 15.4% vs. PSV 22.7%). However, the difference did not reach significance in all primary and secondary outcomes.
Conclusion
In respiratory ICU patients, the weaning process can be usefully performed by ATC (at least as effective as PSV) but without significant hastening of the weaning process. All primary and secondary outcomes were potentially improved (weaning duration, extubation outcome, predictive value of ATC-assisted ratio of respiratory rate and tidal volume, number of spontaneous breathing trials, weaning category, reintubation rate, complications, and hospital mortality). Egypt J Broncho 2015 9:253–260 © 2015 Egyptian Journal of Bronchology
Article PDF
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.References
Boles JM, Bion J, Connors A, Herridge M, Marsh B, Melot C, et al. Weaning from mechanical ventilation. Eur Respir J 2007; 29:1033–1056.
Tallo FS, Sandre VL, Lopes RD, Simone SV, Lopes AC. Weaning from mechanical ventilation: approach for the internist. Rev Soc Bras Clin Med 2014; 12:57–63.
L’Her E. Automatic tube compensation: is it worthwhile? Respir Care 2012; 57:813–814.
Cohen JD, Shapiro M, Grozovski E, Singer P. Automatic tube compensation-assisted respiratory rate to tidal volume ratio improves the prediction of weaning outcome. Chest 2002; 122:980–984.
Cohen JD, Shapiro M, Grozovski E, Lev S, Fisher H, Singer P. Extubation outcome following a spontaneous breathing trial with automatic tube compensation versus continuous positive airway pressure. Crit Care Med 2006; 34:682–686.
Cohen J, Shapiro M, Grozovski E, Fox B, Lev S, Singer P. Prediction of extubation outcome: a randomised, controlled trial with automatic tube compensation vs. pressure support ventilation. Crit Care 2009; 13:R21.
Selek C, Ozcan PE, Orhun G, Şenturk E, Akinci IO, Cakar N. The comparison of automatic tube compensation (ATC) and T-piece during weaning. Turk J Anaesth Reanim 2014; 42:91–95.
Haberthur C, Mols G, Elsasser S, Bingisser R, Stocker R, Guttmann J. Extubation after breathing trials with automatic tube compensation, T-tube, or pressure support ventilation. Acta Anaesthesiol Scand 2002; 46:973–979.
Frutos-Vivar F, Esteban A. Weaning from mechanical ventilation: why are we still looking for alternative methods? Med Intensiva 2013; 37:605–617.
Oto J, Imanaka H, Nakataki E, Ono R, Nishimura M. Potential inadequacy of automatic tube compensation to decrease inspiratory work load after at least 48 hours of endotracheal tube use in the clinical setting. Respir Care 2012; 57:697–703.
Eskandar N, Apostolakos MJ. Weaning from mechanical ventilation. Crit Care Clin 2007; 23:263–274.
Aggarwal AN, Agarwal R, Gupta D. Automatic tube compensation as an adjunct for weaning in patients with severe neuroparalytic snake envenomation requiring mechanical ventilation: a pilot randomized study. Respir Care 2009; 54:1697–1702.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med 1985; 13: 818–829.
Le Gall Jr, Lemeshow S, Saulnier F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993; 270:2957–2963.
Bouakl I, Bou-Khalil P, Kanazi G, Ayoub C, El-Khatib M. Weaning from mechanical ventilation. Curr Opin Anaesthesiol 2012; 25:42–47.
Nemer SN, Barbas CS, Caldeira JB, Cárias TC, Santos RG, Almeida LC, et al. A new integrative weaning index of discontinuation from mechanical ventilation. Crit Care 2009; 13:R152.
Funk GC, Anders S, Breyer MK, Burghuber OC, Edelmann G, Heindl W, et al. Incidence and outcome of weaning from mechanical ventilation according to new categories. Eur Respir J 2010; 35:88–94.
Epstein SK. Decision to extubate. Intensive Care Med 2002; 28:535–546.
Figueroa-Casas JB, Montoya R, Arzabala A, Connery SM. Comparison between automatic tube compensation and continuous positive airway pressure during spontaneous breathing trials. Respir Care 2010; 55:549 –554.
Navalesi P, Frigerio P, Patzlaff A, Häußermann S, Henseke P, Kubitschek M. Prolonged weaning: from the intensive care unit to home. Rev Port Pneumol 2014; 20:264–272.
Thille AW, Harrois A, Schortgen F, Brun-Buisson C, Brochard L. Outcomes of extubation failure in medical intensive care unit patients. Crit Care Med 2011; 39:2612–2618.
Ferrer M, Sellares J, Torres A. NIV in withdrawal from mechanical ventilation. Eur Respir 2012; 55:191–205.
Tanios MA, Epstein SK. Spontaneous breathing trials: should we use automatic tube compensation? Respir Care 2010; 55:640–642.
Wilson AM, Gray DM, Thomas JG. Increases in endotracheal tube resistance are unpredictable relative to duration of intubation. Chest 2009; 136:1006–1013.
Author information
Authors and Affiliations
Corresponding author
Additional information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
Rights and permissions
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El-Shahat, H., Salama, S., Wafy, S. et al. Automatic tube compensation versus pressure support ventilation as a weaning mode: does it make a difference?. Egypt J Bronchol 9, 253–260 (2015). https://doi.org/10.4103/1687-8426.165905
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.4103/1687-8426.165905