
Abstract
Background
Chronic obstructive pulmonary disease (COPD) is responsible for reduced bone mineral density (BMD).
Aim
The aim of this study was to explore and assess the association of low BMDwith systemic inflammation in patients with COPD.
Patients and methods
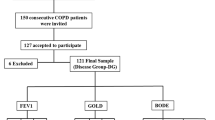
A total of 10 healthy normal control individuals and 30 patients with clinically stable COPD (Global Initiative for Chronic Obstructive Lung Disease stages I–III) were included in the study and divided into four groups. All patients underwent chest radiography; computed tomographic scan of the chest; spirometry; dual-energy X-ray absorptiometry for measurement of BMD of the lumbar (L) spines, forearm, and femur; and blood sampling for measurement of C-reactive protein (CRP) and total and ionized serum calcium.
Statistical analysis
Descriptive data are expressed as mean±SD. Pearson’s correlation analysis was used for drawing correlations.
Results
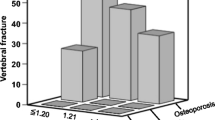
Osteoporosis in the spine was detected in 20% of both mild and moderate COPD cases and 100% of severe COPD cases, with statistical significant difference between patients with severe COPD and control group (P=0.027). Osteoporosis in the femur bone was shown in 30, 50, and 90% of mild, moderate, and severe COPD cases, respectively, whereas 20% of moderate and 30% of severe COPD cases had osteoporosis in the forearm. T-scores of BMD were different among the four studied groups (P=0.0001). BMD correlated positively with BMI and forced expiratory volume at timed interval 1 s (%) predicted. CRP values differed significantly between the four studied groups (P=0.0001). CRP correlated negatively with forced expiratory volume at timed interval 1 s (%) predicted and BMD.
Conclusion
CRP is seen in high levels with low BMD in severe COPD, indicating the association of low BMD with systemic inflammation in COPD.
Article PDF
Similar content being viewed by others

References
Sarkar M, Bhardwaj R, Madabhavi I, Khatana J. Osteoporosis in chronic obstructive pulmonary disease. Clin Med Insights Circ Respir Pulm Med 2015; 9:5–21.
Romme EA, Geusens P, Lems WF, Rutten EP, Smeenk FW, van den Bergh JP, et al. Fracture prevention in COPD patients; a clinical 5-step approach. Respir Res 2015; 7:16–32.
Choudhury G, Rabinovich R, MacNee W. Comorbidities and systemic effects of chronic obstructive pulmonary disease. Clin Chest Med 2014; 35:101–130.
Okazaki R, Watanabe R, Inoue D. Osteoporosis associated with chronic obstructive pulmonary disease. J Bone Metab 2016; 23: 111–120.
Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (updated 2015). 2014. Available at: http://www.goldcopd.org.
Decramer M, Janssens W, Miravitlles M. Chronic obstructive pulmonary disease. Lancet 2012; 379:1341–1351.
Frei A, Muggensturm P, Putchad N, Siebelinge L, Zollerb M, Boydf MC, et al. Five comorbidities reflected the health status in patients with chronic obstructive pulmonary disease: the newly developed COMCOLD index. J Clin Epidemiol 2014; 67:904–911.
Burgel PR, Escamilla R, Perez T, Carré P, Caillaud D, Chanez P, et al., INITIATIVES BPCO Scientific Committee. Impact of comorbidities on COPD-specific health-related quality of life. Respir Med 2013; 107:33–41.
WHO. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Geneva, Switzerland: WHO; 1994.
Cavaillès A, Brinchault-Rabin G, Dixmier A, Goupil F, Gut-Gobert C, Marchand-Adam S, et al. Comorbidities of COPD. Eur Respir Rev 2013; 22:454–475.
Fabbri LM. Smoking, not COPD, as the disease. N Engl J Med 2016; 374:1885–1886.
Inoue D, Watanabe R, Okazaki R. COPD and osteoporosis: links, risks, and treatment challenges. Int J Chron Obstruct Pulmon Dis 2016; 11:637–648.
Romme EA, Smeenk FW, Rutten EP, Wouters EF. Osteoporosis in chronic obstructive pulmonary disease. Expert Rev Respir Med 2013; 7:397–410.
Fucito L, Czabafy S, Hendricks P. Pairing smoking-cessation services with lung cancer screening: a clinical guideline from the association for the treatment of tobacco use and dependence and the society for research on nicotine and tobacco. Cancer 2016; 122:1150–1159.
Launois C, Barbe C, Bertin E, Nardi J, Perotin JM, Dury S, et al. The modified Medical Research Council scale for the assessment of dyspnea in daily living in obesity: a pilot study. BMC Pulm Med 2012; 12:61.
ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med 2002; 166:111–117.
Cote CG, Pinto-Plata VM, Marin JM, Nekach H, Dordelly LJ, Celli BR, et al. The modified BODE index: validation with mortality in COPD. Eur Respir J 2008; 32:1269–1274.
Crapo R, Hankinson JL, Irvin C, Maclntyre N, Voter K, Wise RA, et al. American Thoracic Society. Standardization of spirometry, 1994 update. Am J Respir Crit Care Med 1995; 152:1107–1136.
Hwang YI, Kim CH, Kang HR, Shin T, Park SM, Jang SH, et al. Comparison of the prevalence of chronic obstructive pulmonary disease diagnosed by lower limit of normal and fixed ratio criteria. J Korean Med Sci 2009; 24:621–626.
Swanney MP, Ruppel G, Enright PL, Pedersen OF, Crapo RO, Miller MR, et al. Using the lower limit of normal for the FEV1/FVC ratio reduces the misclassification of airway obstruction. Thorax 2008; 63:1046–1051.
López-Campos JL, Arellano E, Calero C, Delgado A, Márquez E, Cejudo P, et al. Determination of inflammatory biomarkers in patients with COPD: a comparison of different assays. BMC Med Res Methodolo 2012; 12:40.
Karloh M, Mayer AF, Maurici R, Pizzichini MM, Jones PW, Pizzichini E. The COPD Assessment Test: what do we know so far? A systematic review and meta-analysis about clinical outcomes prediction and classification of patients into GOLD stages. Chest 2016; 149:413–425.
Woodruff PG, Barr GR, Bleecker E, Christenson SA, Couper D, Curtis JL, et al. Clinical significance of symptoms in smokers with preserved pulmonary function. N Engl J Med 2016; 374:1811–1821.
Sim YS, Lee JH, Kim Y. Association of bone mineral density with airway obstruction and emphysema. Tuberc Respir Dis (Seoul) 2012; 72:310–317.
Haute Autorité de Santé. High authority of health. Synthesis sheet: how to prevent fractures due to osteoporosis? 2013. Available at: http://www. plan-retraite.fr/prevenir_fractures_osteoporose.
Ward KD, Klesges RC. A meta-analysis of the effects of cigarette smoking on bone mineral density. Calcif Tissue Int 2001; 68:259–270.
Yoon V, Maalouf NM, Sakhaee K. The effects of smoking on bone metabolism. Osteoporos Int 2012; 23:2081–2092.
Dam TT, Harrison S, Fink HA, Ramsdell J, Barrett-Connor E. Bone mineral density and fractures in older men with chronic obstructive pulmonary disease or asthma. Osteoporos Int 2010; 21:1341–1349.
Duckers MJ, Evans BAJ, Fraser WD, Stone MD, Bolton CE, Shale DJ, et al. Low bone mineral density in men with chronic obstructive pulmonary disease. Respir Res 2011; 12:101.
Liu WT, Kuo HP, Liao TH, Chiang LL, Chen LF, Hsu MF, et al. Low bone mineral density in COPD patients with osteoporosis is related to low daily physical activity and high COPD assessment test scores. Int J Chron Obstruct Pulmon Dis 2015; 10:1737–1744.
Vrieze A, de Greef MH, Wijkstra PJ, Wempe JB. Low bone mineral density in COPD patients related to worse lung function, low weight and decreased fat-free mass. Osteoporos Int 2007; 18:1197–1202.
Gan WQ, Man SF, Sin DD. The interactions between cigarette smoking and reduced lung function on systemic inflammation. Chest 2005; 127:558–564.
Pinto VM, Mullerova H, Toso JF, Feudjo-Tepie M, Soriano JB, Vessey RS, et al. C-reactive protein in patients with COPD, control smokers and nonsmokers. Thorax 2006; 61:23–28.
Albert MA, Danielson E, Rifai N, Ridker PM, PRINCE Investigators. Effects of statin therapy on C-reactive protein levels. The Pravastatin Inflammatory/CRP Evaluation (PRINCE): a randomized trial and cohort study. JAMA 2001; 286:64–70.
Iqbal F, Michaelson J, Thaler L, Rubin J, Roman J, Nanes MS. Declining bone mass in men with chronic pulmonary disease: contribution of glucocorticoid treatment, body mass index, and gonadal function. Chest 1999; 116:1616–1624.
Katsura H, Kida K. A comparison of bone mineral density in elderly female patients with COPD and bronchial asthma. Chest 2002; 122:1949–1955.
Bolton CE, Cannings-John R, Edwards PH, Ionescu AA, Evans WD, Pettit RJ, et al. What community measurements can be used to predict bone disease in patients with COPD? Respir Med 2008; 102:651–657.
Incalzi RA, Caradonna P, Ranieri P, Basso S, Fuso L, Pagano F, et al. Correlates of osteoporosis in chronic obstructive pulmonary disease. Respir Med 2000; 94:1079–1084.
Kjensli A, Mowinckel P, Ryg MS, Falch JA. Low bone mineral density is related to severity of chronic obstructive pulmonary disease. Bone 2007; 40:493–497.
Ohara T, Hirai T, Muro S, Haruna A, Terada K, Kinose D, et al. Relationship between pulmonary emphysema and osteoporosis assessed by CT in patients with COPD. Chest 2008; 134:1244–1249.
Van Vliet M, Spruit MA, Verleden G, Kasran A, van Herck E, Pitta F, et al. Hypogonadism, quadriceps weakness, and exercise intolerance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2005; 172:1105–1111.
Cavanagh PR, Licata AA, Rice AJ. Exercise and pharmacological counter measures for bone loss during long-duration space flight. Gravit Space Biol Bull 2005; 18:39–58.
Choi JW, Pai SH. Association between respiratory function and osteoporosis in pre- and postmenopausal women. Maturitas 2004; 48:253–258.
Lekamwasam S, Trivedi DP, Khaw KT. An association between respiratory function and bone mineral density in women from the general community: a cross sectional study. Osteoporos Int 2002; 13:710–715.
Urboniene D, Sakalauskas R, Sitkauskiene B. C-reactive protein levels in patients with chronic obstructive pulmonary disease and asthma. Medicina (Kaunas) 2008; 44:833–840.
Fogarty AW, Jones S, Britton JR, Lewis SA, McKeever TM. Systemic inflammation and decline in lung function in a general population: a prospective study. Thorax 2007; 62:515–520.
Rasmussen F, Lambrechtsen J, Siersted HC, Hansen HS, Hansen NC. Increased C-reactive protein level in COPD patients. The Odense Schoolchild Study. Int Arch Allergy Immunol 2000; 121:129–136.
Author information
Authors and Affiliations
Corresponding author
Additional information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work noncommercially, as long as the author is credited and the new creations are licensed under the identical terms.
Rights and permissions
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El-Hoshy, M.S., El-Sayed, E. & El-Neely, D.A.M. Assessment of reduced mineral bone density in COPD. Egypt J Bronchol 11, 111–119 (2017). https://doi.org/10.4103/1687-8426.203803
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.4103/1687-8426.203803