
Abstract
The bedside Exhaled Drug MONitor – EDMON measures exhaled propofol in ppbv every minute based on multi-capillary column – ion mobility spectrometry (MCC-IMS). The MCC pre-separates gas samples, thereby reducing the influence of the high humidity in human breath. However, preliminary analyses identified substantial measurement deviations between dry and humid calibration standards. We therefore performed an analytical validation of the EDMON to evaluate the influence of humidity on measurement performance. A calibration gas generator was used to generate gaseous propofol standards measured by an EDMON device to assess linearity, precision, carry-over, resolution, and the influence of different levels of humidity at 100% and 1.7% (without additional) relative humidity (reference temperature: 37°C). EDMON measurements were roughly half the actual concentration without additional humidity and roughly halved again at 100% relative humidity. Standard concentrations and EDMON values correlated linearly at 100% relative humidity (R²=0.97). The measured values were stable over 100min with a variance ≤ 10% in over 96% of the measurements. Carry-over effects were low with 5% at 100% relative humidity after 5min of equilibration. EDMON measurement resolution at 100% relative humidity was 0.4 and 0.6 ppbv for standard concentrations of 3 ppbv and 41 ppbv. The influence of humidity on measurement performance was best described by a second-order polynomial function (R²≥0.99) with influence reaching a maximum at about 70% relative humidity. We conclude that EDMON measurements are strongly influenced by humidity and should therefore be corrected for sample humidity to obtain accurate estimates of exhaled propofol concentrations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Propofol is the most used intravenous anaesthetic for induction and maintenance of general anaesthesia and sedation. Anaesthetic effect can be measured by electroencephalographic systems like the Bispectral Index monitor (BIS). However, the electroencephalogram is influenced by opioids and neuromuscular blocking agents, and is subject to internal and external influences such as eye blinking or sensor movement which add noise to the signal [1,2,3]. An alternative approach is to incorporate pharmacokinetic models into infusion pumps which estimate propofol plasma and effect-site concentrations during target-controlled infusions (TCI) [4]. Despite recent development of a new pharmacokinetic model that include data from thousands of patients [5], errors still exceed 22% [6,7,8].
Inappropriate dosing may cause haemodynamic instability, delayed recovery, or (rarely) intraoperative awareness [9,10,11,12]. Real-time monitoring of propofol plasma concentrations is therefore desirable. Monitoring of the exhaled concentration, as routinely performed for volatile anaesthetics, has not previously been available for propofol. Thus, optimal propofol dosing can be challenging for clinicians, and is usually largely guided by experience. One promising non-invasive approach is measurement of exhaled propofol via multi-capillary column – ion mobility spectrometry (MCC-IMS) [13,14,15,16,17].
Real-time propofol monitoring from exhaled breath is a rapidly developing field of research. Harrison et al. were the first to perform online measurements of exhaled propofol, reported in 2003 [18]. Exhaled concentrations correlate reasonably well with blood concentrations [14], [19,20,21,22], and various analytical methods have since been used [13], [14], [19], [20], [23,24,25].
High humidity in breath influences the underlying technology of ion mobility spectrometry [26,27,28]. A multi-capillary column, which is included in the EDMON, pre-separates the gas sample thereby moderating the influence of high humidity in human breath. However, preliminary analyses suggested that residual humidity substantially degraded measurement performance.
The EDMON monitor is primarily intended to be used in mechanically ventilated patients. During mechanical ventilation, humidity of breath samples varies depending on various factors including use of heat and moisture exchange filter and fresh gas flow [29]. Under normal non ventilated conditions exhaled breath has a relative humidity of ~ 80–90% with ~ 100% during end tidal sampling with a reference temperature of 31,5°C [30]. We therefore performed an analytical validation of the EDMON monitor with a specific focus on the influence of humidity on measurement performance.
2 Materials and methods
2.1 Experimental setup
Propofol stock solution of 35.9µg mL-1 was freshly prepared by dissolving propofol ≥ 97% (Sigma-Aldrich, Steinheim, Germany) in 1% v/v absolute ethanol (Sigma-Aldrich, Steinheim, Germany) in HPLC-grade water or n-hexane ≥ 99% (VWR International, Geldenaaksebaan, Belgium) for all measurements and stored in a 250 mL glass bottle. To enhance accuracy, the exact propofol concentration of the stock solution was calculated according to the weight of the added propofol determined with an analytical scale (MSA225P-1CE-DU; Sartorius, Goettingen, Germany).
Propofol standard concentrations were generated with a reference gas generator (HovaCal 4836-VOC; IAS, Oberursel, Germany) at a flow of 730 mL min-1 N2 (purity ≥ 99,95%) [31]. Propofol stock solution was dosed with 12.5 µL and 50 µL syringes (Hamilton, Planegg, Germany), while purified water (HPLC-grade; VWR, Darmstadt, Germany) was dosed with 250 µL syringes. Vaporization temperature was set to 100°C. Humidity of the resulting gas was calculated for a reference temperature of 37°C to represent physiological conditions. ViewCAL 1.2.1 (IAS, Oberursel, Germany) software was used to control the HovaCal. For standard concentrations between 1 and 30 ppbv a 12.5 µL syringe was used, for higher concentrations a 50 µL syringe was used.
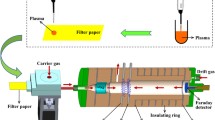
To prevent a loss of propofol and humidity during sampling through condensation and sorption effects, a heated (50°C) perfluoroalkoxy alkane (PFA) sample tube (IAS, Oberursel, Germany) was used and sample gas was constantly provided by the HovaCal. The EDMON was connected to this sample tube via a 1.8-meter long polytetrafluoroethylene (PTFE) tube (B.Braun Melsungen AG, Melsungen, Germany) and a stainless steel 1/8” t-piece (Swagelok, Frankfurt, Germany) open to atmospheric pressure to avoid overpressure. The EDMON was supplied with synthetic air (Air Liquide, Düsseldorf, Germany) with a purity ≥ 99.999% as drift and carrier gas. Values were generated within a minute cycle with a sampling time of 20s and a processing time of 40s. The sample was acquired with a flow of 150 mL/min. The aim was to simulate sampling inside the lung, choosing 37°C as the reference temperature and ~ 100% relative humidity for gas sampling [32], as body temperature does not change much during normal clinical conditions [33] resulting in the maximum concentration of humidity during ventilation, not including active humidification.
2.2 Linearity
Propofol standard concentrations of 100, 90, 80, 70, 60, 50, 40, 30, 20, 10, 5 and 1 ppbv with 100% relative humidity (RH; Treference = 37°C) and without additional humidity were generated with the HovaCal to determine linearity. Each standard concentration was measured for 30min in 1-minute intervals leading to 30 values. Initially and after each concentration step 15 blank measurements were carried out without propofol and without additional humidity to avoid carry-over effects. Limit of Detection (LOD) and Limit of Quantification (LOQ) were determined based on the standard deviation of the response and slope using the values gathered for linearity according to the European Medicines Agency guideline [34].
2.3 Precision, Carry-over, and Resolution
Precision, carry-over, and resolution were assessed at 100% relative humidity and without additional humidity. Therefore, standard concentrations of 20 ppbv and 40 ppbv were sustained for 100min before being reducing to 0 ppbv. To analyse carry-over effects, a standard concentration of 10 ppbv was maintained for 10min and then reduced to 0 ppbv. Resolution was graphically determined for low and high standard concentrations of 5 ppbv in a range of 1–10 ppbv and 40 ppbv in a range of 30–50 ppbv by measuring the distance between the 95% prediction interval and comparing it to values on the x-axis to receive the range in which the device can distinguish differences in concentration.
2.4 Influence of different levels of relative humidity
Under a constant standard concentration of 30 ppbv, relative humidity was increased in 10% increments from 0 to 100% every 15min. The process was then reversed, with relative humidity decreasing from 100 to 0% in increments of 10%. To exclude humidity deriving from the aqueous propofol stock solution, measurements were additionally carried out with a hexane-diluted propofol stock solution.
2.5 Data analysis and statistical analysis
EDMON data were recorded by the CLINEDMON software version 1.1 (B.Braun Melsungen AG, Melsungen, Germany). Statistical analysis was conducted in R (version 3.5.3, R Core Team, R Foundation for Statistical Computing, Vienna, Austria) with the following packages: ggsignif (0.6.0, Constantin Ahlmann-Eltze, Indrajeet Patil) and ggplot2 (3.3.0, Hadley Wickham, Thomas Lin Pedersen et al.).
Normality was determined by Shapiro-Wilk testing using standard residuals and visual inspection of histograms and quantile-quantile-plots. Normally distributed data are presented as means ± SDs, and non-normally distributed data are presented as medians and interquartile ranges. Comparisons were done using one-way ANOVA, followed by pairwise comparisons using the Tukey test. A two-sided p < 0.05 was considered statistically significant.
3 Results
3.1 Linearity
Linearity was confirmed under 100% relative humidity for calibration standard concentrations between 5 and 100 ppbv with standard deviations being ≤ 10% of the mean measured concentrations (Fig.1, red line) and only ~ 22% of the actual concentration of the calibration standard. The standard deviation exceeded 10% of the measured concentration only when the standard concentration was 90 ppbv. Without additional humidity, linearity was measured between 1 and 100 ppbv and confirmed for calibration standard concentrations between 1 and 60 ppbv with standard deviations being ≤ 10% of the mean measured concentrations (Fig.1, blue line) and only ~ 43% of the calibration standard concentration.

Linear calibration between HovaCal standard concentrations from 0 ppbv to 100 ppbv and EDMON measurements with and without additional humidity
Mean measured concentrations were in a range of 0.57 to 23 ppbv with 100% relative humidity and 1.8 to 23 ppbv without additional humidity. Measured concentrations at 100% relative humidity were significantly lower than without additional humidity. Measurements of the standard concentration of 1 ppbv at 100% relative humidity were excluded because measured concentrations were ≤ 0.2 ppbv.
Dots represent the raw data, thick dashes the means, and error bars the SDs. 95% confidence intervals are displayed as dotted lines. Measured concentrations with 100% relative humidity (red; R²= 0.97; y = 4.29x + 2.77) were significantly lower than without additional humidity (blue; R² = 0.99; y = 2.52x − 1.76) apart from standard concentrations ≤ 5 ppbv. The black line represents the upper measurement limit of the EDMON at 23 ppbv. The Limit of Detection (LOD) and Limit of Quantification (LOQ) resulted in 0.19 ppbv, 0.59 ppbv without additional humidity and 0.79 ppbv, 2.4 ppbv at 100% relative humidity respectively.
3.2 Precision and carry-over
After a 10-minute equilibration period, values were within ± 10% of the mean measured concentration for 96.5% of the measurements at 100% relative humidity and for 98.5% of the measurements without additional humidity (Fig.2A). At a standard concentration of 20 ppbv, measured concentrations had a relative standard deviation of 6.5% at 100% relative humidity and 5.4% without additional humidity; at 40 ppbv, relative standard deviations were 4.8% at 100% relative humidity and 1.2% without additional humidity (Fig.2B).

Bland-Altman plot of measured concentrations over 100min with a steady standard concentration of 20 ppbv (A) and 40 ppbv (B) at 100% relative humidity and without additional humidity. Upper and lower reference line are presented as dashed lines
To evaluate carry-over effects, a standard concentration of 10 ppbv was generated for 10min, resulting in mean measured concentrations of 3.9, 3.6, and 3.7 ppbv at 100% relative humidity, and 5.4, 5.7, and 6.1 ppbv without additional humidity (Fig.3). After switching to 0 ppbv, mean measured concentrations dropped to 0.2, 0.2, and 0.2 ppbv at 100% relative humidity and to 0.7, 0.7, and 0.6 ppbv without additional humidity after 5min. Mean measured concentrations finally dropped to 0, 0, and 0 ppbv at 100% relative humidity and to 0.4, 0.3, and 0.4 ppbv without additional humidity after 10min. Average carry-over was 5.3% after 5min and 0% after 10min at 100% relative humidity, and 11.6% after 5min and 6.4% after 10min without additional humidity.

Evaluation of carry-over effects. Measured concentrations over time with 10-minute intervals of 10 ppbv and 0 ppbv standard concentration for measurements with 100% relative humidity and without additional humidity. Concentration changes were evaluated, after changing standard concentration from 10 ppbv to 0 ppbv
3.3 Resolution
Resolution was graphically determined based on the calibration curves given in Fig.1. Measurement resolution at 100% relative humidity was 1.3 ppbv at the standard concentration 5 ppbv, and 3.8 ppbv at 40 ppbv. Without additional humidity, resolution was 0.9 ppbv at 5 ppbv, and 4 ppbv at 40 ppbv (Fig.4).

Graphical determination of resolution for standard HovaCal concentrations of 5 ppbv in a range of 1–10 ppbv and 40 ppbv in a range of 30–40 ppbv.
Solid lines represent linear regression lines. Dotted lines represent 95% confidence intervals and dashed lines represent 95% prediction intervals
3.4 Influence of different amounts of relative humidity
Concentrations measured by the EDMON in percent of the generated standard concentrations are presented in Fig.5 as a function of the additional humidity. The measured proportion decreased following a sigmoidal function with increasing humidity. When additional humidity ranged between 70% and 100%, measured concentrations reached a plateau implicating no further influence on measurement performance at an additional humidity greater than 70%.
Two measurement series with an aqueous propofol stock solution were congruent to each other (p = 0.054), except for values at 50% additional humidity (p = 0.007). In comparison to the measurement series with a hexane-diluted stock solution, the obtained values did not significantly differ between 20% and 40% additional humidity for Increasing 1 (p = 0.64, 0.91, 0.2) and between 20% and 50% for Increasing 2 (p = 0.22, 0.99, 0.98, 0.67). Measured concentrations were significantly greater with increasing than decreasing humidity (p = 0). The mean concentrations measured by the EDMON were 24% (± 1.5) of the generated standard concentrations at 100% relative humidity and 46% (± 4) without additional humidity.

Influence of humidity on the EDMON measurement performance
A propofol standard concentration of 30 ppbv was constantly generated by a reference gas generator (HovaCal) and measured by the EDMON under increasing and decreasing relative humidity. Values are presented as the proportional difference between concentrations measured by the EDMON and the generated standard concentrations. Data are presented as means ± SDs (n = 13). Values in black were measured with propofol diluted in n-hexane instead of water. Values for 10% additional humidity were removed, as the SD was unreasonably high (9.7%; imprecision 23.5%). Increasing levels of humidity: y = 0.0026x²-0.46x + 46, R²=0.99 (red, Increasing 1); y = 0.0021x²-0.42x + 45, R²=0.99, (blue, Increasing 2); decreasing levels of humidity: y = 0.0032x²-0.49x + 42, R²=0.99 (green, Decreasing); hexane-diluted propofol standards: y = 0.0035x²-0.58x + 49, R²=0.99 (black, n-hexane).
4 Discussion
Analytical validation of the EDMON device confirmed a wide linear range, high precision, good resolution, and low limits of detection and quantification which are consistent with the manufacturer’s specifications [35]. We excluded strong carry-over effects with the recommended measurement setup, confirming that the inert tubing material perfluoroalkoxy alkane and polytetrafluoroethylene is unlikely to bind propofol as previously reported [36]. Additionally, propofol is highly hydrophobic with a solubility of only 124mg/L [37], and is therefore unlikely to accumulate in condensate building up in the tubing at any humidity level.
Our results are generally consistent with a previous analytical validation of a prototype of the EDMON [38]. Linearity, precision and carry-over were comparable. However, limits of quantification (LOQ, 0.3) and detection (LOD, 0.1), and resolution (> 0.5, 2–4 ppbv; >0.9, 28–30 ppbv) were previously lower than in our validation. This is most likely caused by using raw signal intensities during the previous validation which has been disabled in recent EDMON versions. We therefore had to use the values displayed by the EDMON which are based on the manufacturer’s calibration. Access to raw signal intensities may thus have produced slightly better results for LOQ, LOD, and resolution.
Most interestingly, we found that standard concentrations, generated without additional humidity by the calibration gas generator HovaCal, differed from the concentrations measured by the EDMON device. Standard concentrations generated by the HovaCal were previously validated by liquid injection gas chromatography - mass spectrometric measurements (R²=0.89) [39]. Therefore, we presume that deviations between standard concentrations and EDMON-measured concentrations result from the manufacturer’s calibration process using permeation tubes. The calibration works by heating propofol-containing tubes to evaporate propofol at a specific rate and standard concentrations are generated by adjusting the flow rate of carrier gas around the permeation tubes [40]. The accuracy of permeation tubes is ± 5% (communication from Valco Instruments Co. Inc.) – a range that does not explain the differences we observed between standard and EDMON-measured concentrations.
We additionally observed a reduction in EDMON signal intensity of up to 50% by adding humidity to the calibration gas. EDMON signals from humid and dry gas samples thus substantially differ, additional to the already observed deviation between HovaCal-generated standard concentrations and EDMON-measured concentrations under dry conditions. Exhaled air contains up to 100% relative humidity corresponding to temperatures of exhaled air. Consequently, a calibration of the EDMON device with dry gas standards, as performed by the manufacturer, produces falsely low propofol estimates during clinical use of the EDMON. We therefore suggest using at least humidified gas standards to calibrate the EDMON to ensure accurate measurements under physiological conditions.
In contrast to Buchinger et al. [41] who state that there is no influence of humidity on the propofol signal of MCC-IMS measurements when tailing of the reactant ion peak is compensated, we observed a distinct and clinically important relationship between sample humidity and EDMON measurements which almost perfectly fit a second order polynomial function. Presumably the under-estimate results from reactant ions forming water clusters (H*(H2O)n) with high humidity [28][42]. The resulting proton affinity of 808kJ mol-1 ((H2O)2) is similar to the estimated proton affinity of propofol (Phenol: 817kJ mol-1; Toluene: 784kJ mol-1) [43][44] hampering ionisation. Additionally, an increase in humidity reduces the intensities of negative reactant ions and formation of negative reactant ion clusters [45].
Relative humidities between 70% and 100% roughly halved the EDMON measured concentrations compared to measurements without additional humidity. Considering the typical humidity of 27g/m³ in the mouth [46], which corresponds to 62% relative humidity (Tref = 37°C), clinical samples will always contain substantial humidity, but may lay under the 70% threshold. Therefor influences on measured propofol concentrations are prone to differ during changing clinical conditions. Such, the amount of humidity in clinical samples is influenced by patient conditions, heat-and-moisture-exchanging filters, ventilation settings, active humidification, oxygen concentration, fresh mixture volume, inspiratory and expiratory settings, lung-protective ventilation, etc. [46,47,48,49,50]. EDMON measurements will thus be inaccurate unless corrected for humidity.
Jiang et al. [51] propose a correction for photoionization IMS that does not require measuring humidity. Specifically, the method is based on a quantitative influence of humidity on both the product ion peak (PIP) and the reactant ion peak (RIP), leading to nearly constant values for intensity ratio of Propofol/ (RIP + Propofol) at relative humidity levels of 0–98%. However, this approach may not work with the EDMON system since the in-build IMS uses atmospheric pressure chemical ionisation (APCI) [52]. Most accurately, the EDMON device should therefore monitor sample humidity to calculate propofol concentrations from calibrations at several levels of sample humidity.
In summary, linearity with and without additional humidity was observed for measured concentrations between 1 ppbv and 23 ppbv, while imprecision over 100 measurements was ≤ 10%. Resolution is comparable for measurements with and without additional humidity whereas carry-over effects are smaller with additional humidity. The influence of humidity was substantial and results in a sigmoidal decrease in measured propofol concentration by up to 50% at relative humidities exceeding 70%. Quantitative propofol measurements must therefore be adjusted for sample humidity on-line, or at least at the beginning of the measurement, for sample humidity if it can be ensured that the humidity remains stable throughout the procedure, preferably above the 70% threshold. The equations we provide suggest an easy way to adjust for sample humidity.
Data Availability
Not Applicable.
Code Availability
Not Applicable.
References
Mertens MJ, Olofsen E, Engbers FHM, Burm AGL, Bovill JG, Vuyk J, “Propofol reduces perioperative remifentanil requirements in a synergistic manner: Response surface modeling of perioperative remifentanil-propofol interactions,” Anesthesiology, vol.99, no. 2, pp.347–359, Aug. 2003, doi: https://doi.org/10.1097/00000542-200308000-00016.
Aydemir O, Kayikcioglu T, Pourzare S, “Classifying various EMG and EOG artifacts in EEG signals BCI based on rotating vanes View project Classification of EEG based BCI signals imagined hand closing and opening View project Classifying Various EMG and EOG Artifacts in EEG Signals,” Accessed: Apr. 28, 2021. [Online]. Available: https://www.researchgate.net/publication/289614615.
Fingelkurts AA, et al., “Reorganization of the composition of brain oscillations and their temporal characteristics in opioid dependent patients,” Prog. Neuro-Psychopharmacology Biol. Psychiatry, vol.30, no. 8, pp.1453–1465, Dec. 2006, doi: https://doi.org/10.1016/j.pnpbp.2006.06.005.
“US5522798A. - Control of a multi-channel drug infusion pump using a pharmacokinetic model - Google Patents.” https://patents.google.com/patent/US5522798A/en (accessed Apr. 28, 2021).
Eleveld DJ, Colin P, Absalom AR, Struys MMRF. Pharmacokinetic–pharmacodynamic model for propofol for broad application in anaesthesia and sedation. Br J Anaesth. May 2018;120(5):942–59. doi:https://doi.org/10.1016/j.bja.2018.01.018. “,”, , .
Hüppe T, Maurer F, Sessler DI, Volk T, Kreuer S, “Retrospective comparison of Eleveld, Marsh, and Schnider propofol pharmacokinetic models in 50 patients,” British Journal of Anaesthesia, vol.124, no. 2. Elsevier Ltd, pp. e22–e24, Feb. 01, 2020, doi: https://doi.org/10.1016/j.bja.2019.10.019.
Glen JBB, Servin F. Evaluation of the predictive performance of four pharmacokinetic models for propofol. Br J Anaesth. May 2009;102(5):626–32. doi:https://doi.org/10.1093/bja/aep043. “,”, , .
Vellinga R, et al. Prospective clinical validation of the Eleveld propofol pharmacokinetic-pharmacodynamic model in general anaesthesia. Br J Anaesth. Feb. 2021;126(2):386–94. doi:https://doi.org/10.1016/j.bja.2020.10.027. “,”, , .
Gürkan Y, Kiliçkan L, Toker K. Propofol-nitrous oxide versus sevoflurane-nitrous oxide for strabismus surgery in children. Pediatr Anesth. Nov. 1999;9(6):495–9. doi:https://doi.org/10.1046/j.1460-9592.1999.00399.x. “,”, , .
Cohen IT, Finkel JC, Hannallah RS, Hummer KA, Patel KM. Rapid emergence does not explain agitation following sevoflurane anaesthesia in infants and children: a comparison with propofol. Pediatr Anesth. Jan. 2003;13(1):63–7. doi:https://doi.org/10.1046/j.1460-9592.2003.00948.x. “,”, , .
Uezono S, et al., “Emergence Agitation After Sevoflurane Versus Propofol in Pediatric Patients,” Anesth. Analg., vol.91, no. 3, pp.563–566, Sep. 2000, doi: https://doi.org/10.1213/00000539-200009000-00012.
Hino H, Matsuura T, Kihara Y, Tsujikawa S, Mori T, Nishikawa K, “Comparison between hemodynamic effects of propofol and thiopental during general anesthesia induction with remifentanil infusion: a double-blind, age-stratified, randomized study,” J. Anesth., vol.33, no. 4, pp.509–515, Aug. 2019, doi: https://doi.org/10.1007/s00540-019-02657-x.
Zhou Q, et al., “Trap-and-release membrane inlet ion mobility spectrometry for on-line measurement of trace propofol in exhaled air,” Anal. Methods, vol.6, no. 3, pp.698–703, Feb. 2014, doi: https://doi.org/10.1039/c3ay41545g.
Perl T, et al., “Determination of serum propofol concentrations by breath analysis using ion mobility spectrometry,” Br. J. Anaesth., vol.103, no. 6, pp.822–827, Dec. 2009, doi: https://doi.org/10.1093/bja/aep312.
Carstens E, et al. On-Line determination of serum propofol concentrations by expired air analysis. Int J Ion Mobil Spectrom. Mar. 2010;13(1):37–40. doi:https://doi.org/10.1007/s12127-010-0036-7. “,”, , .
Kreuder AE, Buchinger H, Kreuer S, Volk T, Maddula S, Baumbach JI, “Characterization of propofol in human breath of patients undergoing anesthesia,” Int. J. Ion Mobil. Spectrom., vol.14, no. 4, pp.167–175, Dec. 2011, doi: https://doi.org/10.1007/s12127-011-0080-y.
Müller-Wirtz LM, et al., “Exhaled Propofol Concentrations Correlate With Plasma and Brain Tissue Concentrations in Rats,” Anesth. Analg., vol.132, no. 1, pp.110–118, Jan. 2021, doi: https://doi.org/10.1213/ANE.0000000000004701.
Harrison GR, Critchley ADJ, Mayhew CA, Thompson JM, “Real-time breath monitoring of propofol and its volatile metabolites during surgery using a novel mass spectrometric technique: a feasibility study,” Br. J. Anaesth., vol.91, no. 6, pp.797–799, Dec. 2003, doi: https://doi.org/10.1093/bja/aeg271.
Hornuss C, et al., “Real-time monitoring of propofol in expired air in humans undergoing total intravenous anesthesia,” Anesthesiology, vol.106, no. 4, pp.665–674, Apr. 2007, doi: https://doi.org/10.1097/01.anes.0000264746.01393.e0.
Chen X, et al., “Gas chromatograph–surface acoustic wave for quick real-time assessment of blood/exhaled gas ratio of propofol in humans,” Br. J. Anaesth., vol.113, no. 5, pp.807–814, Nov. 2014, doi: https://doi.org/10.1093/bja/aeu193.
Colin P, et al. Propofol Breath Monitoring as a Potential Tool to Improve the Prediction of Intraoperative Plasma Concentrations. Clin Pharmacokinet. Jul. 2016;55(7):849–59. doi:https://doi.org/10.1007/s40262-015-0358-z. “,”, , .
Kamysek S, et al. Drug detection in breath: Effects of pulmonary blood flow and cardiac output on propofol exhalation. Anal Bioanal Chem. Oct. 2011;401(7):2093–102. doi:https://doi.org/10.1007/s00216-011-5099-8. “,”, , .
Takita A, Masui K, Kazama T. On-line monitoring of end-tidal propofol concentration in anesthetized patients. Anesthesiology. Apr. 2007;106(4):659–64. doi:https://doi.org/10.1097/01.anes.0000264745.63275.59. “,”, , .
Boshier PR, et al., “On-line, real time monitoring of exhaled trace gases by SIFT-MS in the perioperative setting: A feasibility study,” Analyst, vol.136, no. 16. Royal Society of Chemistry, pp.3233–3237, Aug. 21, 2011, doi: https://doi.org/10.1039/c1an15356k.
Grossherr M, Varadarajan B, Dibbelt L, Schmucker P, Gehring H, Hengstenberg A, “Time course of ethanol and propofol exhalation after bolus injection using ion molecule reaction-mass spectrometry,” Anal. Bioanal. Chem., vol.401, no. 7, pp.2063–2067, Oct. 2011, doi: https://doi.org/10.1007/s00216-010-4042-8.
Izadi Z, Tabrizchi M, Borsdorf H, Farrokhpour H. Humidity Effect on the Drift Times of the Reactant Ions in Ion Mobility Spectrometry. Anal Chem. 2019;91(24):15932–40. doi:https://doi.org/10.1021/acs.analchem.9b04450. “,”, , .
Borsdorf H, Fiedler P, Mayer T. The effect of humidity on gas sensing with ion mobility spectrometry. Sens Actuators B Chem. 2015;218:184–90. doi:https://doi.org/10.1016/j.snb.2015.04.102. “,”, .
Mäkinen M, Sillanpää M, Viitanen AK, Knap A, Mäkelä JM, Puton J. The effect of humidity on sensitivity of amine detection in ion mobility spectrometry. Talanta. 2011;84(1):116–21. doi:https://doi.org/10.1016/j.talanta.2010.12.030. “,”, , .
Kleemann PP. Humidity of anaesthetic gases with respect to low flow anaesthesia. Anaesth Intensive Care. Aug. 1994;22(4):396–408. doi:https://doi.org/10.1177/0310057x9402200414. “,”, , .
Ferrus L, Guenard H, Vardon G, Varene P, “Respiratory water loss,” Respir. Physiol., vol.39, no. 3, pp.367–381, Mar. 1980, doi: https://doi.org/10.1016/0034-5687(80)90067-5.
Vautz W, Schmäh M. “HovaCAL ®-a generator for multi-component humid calibration gases,” doi: https://doi.org/10.1007/s12127-009-0030-0.
Green J, Dyer I. Measurement of humidity. Anaesth Intensive Care Med. Jan. 2009;10(1):45–7. doi:https://doi.org/10.1016/J.MPAIC.2008.11.016. “,”, , .
Bickler PE, Sessler DI. “Efficiency of Airway Heat and Moisture Exchangers in Anesthetized Humans.”.
ICH Expert Working Group. “ICH Topic Q 2 (R1) Validation of Analytical Procedures: Text and Methodology Step 5 NOTE FOR GUIDANCE ON VALIDATION OF ANALYTICAL PROCEDURES: TEXT AND METHODOLOGY (CPMP/ICH/381/95) APPROVAL BY CPMP November 1994 DATE FOR COMING INTO OPERATION,” 1995. [Online]. Available: http://www.emea.eu.int.
“Manual. Exhaled Drug Monitor - EDMON®, Version: 23.06.2020/DE 110.”.
Maurer F, et al. Adherence of volatile propofol to various types of plastic tubing. J Breath Res. Mar. 2017;11(1):016009. doi:https://doi.org/10.1088/1752-7163/aa567e. “,”, , .
“Propofol | C12H18O - PubChem.” https://pubchem.ncbi.nlm.nih.gov/compound/4943#section=Pharmacology (accessed May 14, 2021).
Maurer F, et al. Calibration and validation of a MCC/IMS prototype for exhaled propofol online measurement. J Pharm Biomed Anal. 2017;145:293–7. doi:https://doi.org/10.1016/j.jpba.2017.06.052. “,”, .
Maurer F, Geiger M, Volk T, Sessler DI, Kreuer S, “Validation of liquid and gaseous calibration techniques for quantification of propofol in breath with sorbent tube Thermal Desorption System GC–MS,” J. Pharm. Biomed. Anal., vol.143, pp.116–122, Sep. 2017, doi: https://doi.org/10.1016/j.jpba.2017.05.042.
Mitchell GD, “A review of permeation tubes and permeators,” Separation and Purification Methods, vol.29, no. 1. Taylor & Francis Group, pp.119–128, 2000, doi: https://doi.org/10.1081/SPM-100100005.
Buchinger H, et al., “Minimal retarded Propofol signals in human breath using ion mobility spectrometry,” doi: https://doi.org/10.1007/s12127-012-0118-9.
Eiceman GA, Nazarov EG, Rodriguez JE, Bergloff JF. Positive Reactant Ion Chemistry for Analytical, High Temperature Ion Mobility Spectrometry (IMS): Effects of Electric Field of the Drift Tube and Moisture, Temperature, and Flow of the Drift Gas. Ijims. 1998;1(1):28–37. “,”, .
Blake RS, Monks PS, Ellis AM, “Proton-transfer reaction mass spectrometry,” Chemical Reviews, vol.109, no. 3. American Chemical Society, pp.861–896, Mar. 11, 2009, doi: https://doi.org/10.1021/cr800364q.
Hunter EPL, Lias SG, “Evaluated gas phase basicities and proton affinities of molecules: An update,” J. Phys. Chem. Ref. Data, vol.27, no. 3, pp.413–656, Oct. 1998, doi: https://doi.org/10.1063/1.556018.
Mayer T, Borsdorf H. Accuracy of ion mobility measurements dependent on the influence of humidity. Anal Chem. May 2014;86(10):5069–76. doi:https://doi.org/10.1021/ac5007393. “,”, , .
Shelly MP, Lloyd GM, Park GR. “Intensive Care Medicine A review of the mechanisms and methods of humidification of inspired gases,” 1988.
Solomita M, Daroowalla F, LeBlanc DS, Smaldone GC. “Y-Piece Temperature and Humidification During Mechanical Ventilation,” Respir. Care, vol.54, no. 4, 2009.
Johansson A, Lundberg D, Luttropp HH. The effect of heat and moisture exchanger on humidity and body temperature in a low-flow anaesthesia system. Acta Anaesthesiol Scand. May 2003;47(5):564–8. doi:https://doi.org/10.1034/j.1399-6576.2003.00108.x. “,”, , .
Dyer I, “Measurement of humidity,” Anaesthesia and Intensive Care Medicine, vol.13, no. 3. Elsevier Ltd, pp.121–123, Mar. 01, 2012, doi: https://doi.org/10.1016/j.mpaic.2011.12.011.
Restrepo RD, Walsh BK. Humidification during invasive and noninvasive mechanical ventilation: 2012. Respir Care. May 2012;57(5):782–8. doi:https://doi.org/10.4187/RESPCARE.01766. “,”, , .
Jiang D, et al. Breath-by-breath measurement of intraoperative propofol by unidirectional anisole-assisted photoionization ion mobility spectrometry via real-time correction of humidity. Anal Chim Acta. Mar. 2021;1150:338223. doi:https://doi.org/10.1016/j.aca.2021.338223. “,”, .
Baumbach JI, “Ion mobility spectrometry coupled with multi-capillary columns for metabolic profiling of human breath,” Journal of Breath Research, vol.3, no. 3. IOP Publishing, p.034001, May 15, 2009, doi: https://doi.org/10.1088/1752-7155/3/3/034001.
Funding
The department of Anaesthesiology, Intensive Care and Pain Therapy, Saarland University Medical Center, financed this work. All devices are loan from B. Braun Melsungen (Melsungen, Germany).
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
Not Applicable.
Consent to participate
Not Applicable.
Consent for publication
Not Applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Teucke, T., Maurer, F., Müller-Wirtz, L. et al. Humidity and measurement of volatile propofol using MCC-IMS (EDMON). J Clin Monit Comput 37, 493–500 (2023). https://doi.org/10.1007/s10877-022-00907-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10877-022-00907-0