
Abstract
Introduction
Injection drug use is the main transmission route of hepatitis C virus (HCV) in China. The prevalence of HCV remains high at 40–50% among people who inject drugs (PWID). We developed a mathematical model to predict the impacts of different HCV intervention strategies on the HCV burden in Chinese PWID by 2030.
Methods
We developed a dynamic deterministic mathematical model to simulate the transmission of HCV among PWID in China between 2016 and 2030, using domestic data based on the real cascade of HCV care. We considered various intervention scenarios, including treatment regimens, harm reduction program (HRP) coverage, enhanced testing and referral for treatment.
Results
HCV incidence will exhibit a gradual but slow declining trend from 12,970 in 2016 to 11,761 in 2030 based on current screening and treatment practices among PWID (scenario 1). Scaled-up HCV screening and treatment integrated with HRPs (scenario 8) demonstrated the most substantial reduction in HCV burden, being the only intervention scenario that could achieve the World Health Organization’s (WHO’s) HCV elimination target. Specifically, the HCV incidence in 2030 is projected to be reduced by 81.42%, and HCV-related deaths are projected to be reduced by 91.94%.
Conclusion
Our study indicates that achieving WHO elimination targets is an extremely challenging goal that requires substantial improvements in HCV testing and treatment among PWID (scenario S8). The findings suggest that coordinated improvements in testing, treatment, and harm reduction programs could greatly reduce the HCV burden among PWID in China, and urgent policy changes are needed to integrate HCV testing and treatment into existing HRPs.
Plain Language Summary
China has the largest number of people living with the hepatitis C virus. The prevalence of hepatitis C among people who inject drugs is high at 40–50%, significantly higher than the prevalence among other high-risk groups. Preventing the transmission of hepatitis C among people who inject drugs is essential to avoid future liver diseases. We used a mathematical model to evaluate the impacts of different intervention strategies on the incidence, prevalence and mortality of hepatitis C among people who inject drugs in China by 2030. We found that scaled-up hepatitis C screening and treatment integrated with harm reduction programs demonstrated the most substantial reduction in the burden of hepatitis C; specifically, the incidence of hepatitis C in 2030 is reduced by 81.42% and hepatitis-C-related deaths are reduced by 91.94%. Increasing harm reduction program coverage among people who inject drugs has a greater impact in terms of reducing the burden of hepatitis C virus compared with enhanced linkage to care or test frequency alone. Substantial improvements in both testing and treatment integrated with existing harm reduction programs are essential to achieve the goal of eliminating hepatitis C in China by 2030.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
China has the largest number of hepatitis C virus (HCV) infections, with an estimated 9.5 million HCV-infected individuals. |
Preventing HCV transmission among people who inject drugs (PWID) is essential to avoid future liver disease and achieve the World Health Organization’s (WHO’s) HCV elimination goal in China by 2030. |
To assess the impacts of different HCV intervention strategies on HCV burden in Chinese PWID by 2030. |
What was learned from the study? |
Scaled-up HCV screening and treatment integrated with harm reduction programs (HRPs) demonstrated the most substantial reduction in HCV burden. Specifically, the HCV incidence in 2030 is projected to be reduced by 81.42%, and HCV-related deaths are projected to be reduced by 91.94%. |
Substantial improvements in both testing and treatment integrated with existing harm reduction programs are essential to achieve the WHO HCV elimination goal in China by 2030. |
Introduction
Chronic hepatitis C virus (HCV) infection poses a significant health threat globally, with an estimated 56.8 million infections and 400,000 deaths worldwide in 2020 [1, 2]. Due to its large population, China has the largest number of HCV-infected individuals—an estimated 9.5 million, accounting for approximately one-sixth of all HCV-infected individuals worldwide [1, 3]. Without timely treatment, chronic HCV can be a lifelong infection that leads to serious complications, including liver disease, cirrhosis (scarring of the liver), hepatocellular carcinoma (HCC), and even death [4]. Chronic HCV is now one of the most preventable and treatable diseases, and HCV treatment and prevention can be achieved at the primary health care level through timely screening and referral for treatment [5]. In 2016, the World Health Organization (WHO) established goals to eliminate HCV as a public health threat by 2030.
Injection drug use (IDU) is the main HCV transmission route in China. Despite the introduction of harm reduction programs (HRPs) since the 1980s, the prevalence of HCV remains high at 40–50% among people who inject drugs (PWID) [6, 7], which is substantially higher than that noted in other high-risk populations [8]. Preventing HCV transmission among PWID is essential to avoid future liver disease and achieve the WHO HCV elimination goal in China by 2030. Although several studies indicate that needle and syringe programs (NSPs) and opioid substitution therapy (OST) can reduce the risk of HCV transmission among PWID [9, 10], it is unlikely that a significant reduction in HCV prevalence will be achieved given the high baseline HCV prevalence and high possibility of reinfection in this population [11].
The emergence of highly effective direct-acting antivirals (DAAs) with a sustained viral response (SVR) of greater than 90% renders HCV “treatment as prevention” a distinct possibility. However, many studies have reported barriers to accessing regular health services for PWID, making the expansion of HCV testing and treatment very difficult for PWID. Currently existing HRPs offer an opportunity for early HCV diagnosis and treatment, providing an achievable solution for HCV elimination in PWID. To aid policy-making in China, we developed a mathematical model to assess the impacts of different HCV detection and treatment strategies based on HRPs on HCV incidence, prevalence and mortality in PWID in China by 2030.
Methods
The analysis in this article is based on previously publicly available data and does not involve any new studies of human or animal subjects performed by any of the authors.
Analytic Overview
We developed a dynamic deterministic mathematical model to simulate the transmission of HCV in a population of PWID in China between 2016 and 2030. The model integrates important elements related to HCV prevention and treatment, including HCV infection, the cascade of HCV care, and the natural history of HCV. We considered a range of intervention scenarios, including treatment regimens, HRP coverage, enhanced testing and referral to treatment.
PWID Population and Size
We aimed to model the PWID population in China. The initial distribution of the population of PWID in 2015 was derived from the following sources: China's Drug Situation Report 2016 [12], the data of the National HIV Sentinel Surveillance System (HSSS) [13], and the 2015 China Acquired Immunodeficiency Syndrome (AIDS) Response Progress Report [14]. The accurate estimation of active PWID in China is difficult. We therefore set a stable population of 800,000 PWID by approximating current demographic trends, and the initial HCV prevalence was set as 30% based on published literature [14]. The initial distribution across the HCV cascade of care was assumed as 50% non-diagnosed, 35% diagnosed and 15% in care, based on prior knowledge. More detailed information on the distribution of the PWID population in 2015 is provided in Appendix A S1 in the Supplementary Information.
Model Structure
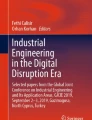
The model structure is presented in Fig. 1. Our compartment model stratifies PWID according to enrollment status (no HRPs or HRPs) along with HCV infection and HCV care cascade status (susceptible and acutely infected, undiagnosed, diagnosed, on treatment, and treatment failure). A PWID enters this model by initiating drug use and exits the model by permanently stopping injection or dying. All PWID are assumed to be initially susceptible to HCV infection. Susceptible PWID can become infected with a force of infection (λ) that is a product of group-specific transmission rates and the time-dependent HCV prevalence in the cohort. The force of infection can be expressed by the following equation: \({\lambda }_{r}={\beta }_{r}\times \frac{I}{N}\), where \({\beta }_{r}\) represents the transmission rate for risk group r, I is the number of infectious individuals and N is the total number of individuals in the population. We assumed homogeneous mixing, i.e., no mixing preferences. However, we assume that people who are enrolled in HRPs have a lower risk than PWID who are not enrolled in HRPs. The relative risk (RR) of HCV infection for PWID without HRPs compared with PWID with HRPs was determined so that different risks of transmission were considered in the model. Thus, if \({\beta }_{L}\) (\({\beta }_{H})\) indicates the transmission rate for individuals in different risk groups, then \({\beta }_{H}=RR\times {\beta }_{L}\). Transmission is reduced by a cofactor (RR) dependent on HRPs. Mathematical formulas used in the model and detailed information are presented in Appendices A S2 and S3 in the Supplementary Information.

Schematics of state transitions in the model. A HCV infection and cascade of care compartments. B Natural history of the HCV compartments. Boxes represent compartments of the model and arrows denote annual transition rates; these can depend upon the risk group, which can vary over time. Spontaneous clearance occurs in a fraction of those acutely infected who then return to the susceptible population. Treatment can result in cure, and reinfection can occur after successful treatment. Infection results in people entering the natural history model (B): HCV disease progresses through five METAVIR fibrosis stages from F0 (no fibrosis) to F4 (compensated cirrhosis). People in the cured compartment of the treatment cascade have no risk of disease progression. HCV hepatitis C virus
After HCV infection, disease progression is assumed to occur according to a widely recognized natural history [4]. Susceptible individuals can become infected. A fraction of the acutely infected individuals achieve spontaneous clearance and then return to the susceptible population. The rest progress to chronic infection through the five METAVIR fibrosis stages. An increased HCV-related death rate occurs from decompensated cirrhosis (DC) and HCC. We assumed that the risk of disease progression and death could be reduced to zero following cure. Individuals may experience various statuses based on the cascade of care for HCV: undiagnosed, diagnosed, or treated. In addition, individuals with HCV infection can receive treatment, which can result in either failure or success. In the case of success, the individual is considered cured (post-SVR) and can be reinfected with HCV. However, the disease will continue to progress in those who experience treatment failures.
Model Parameterization and Calibration
Inputs for model parameters were derived from published studies, especially those conducted among Chinese PWID. Table S1 and Appendix A S4 in the Supplementary Information present the input values for the important model parameters. The value of the transmission parameter for PWID enrolled in HRPs (βL) was determined via the calibration of the HCV incidence observed between 2014 and 2019 among a cohort of PWID who were enrolled in HRPs [15]. The relative risk (RR) of HCV infection for PWID enrolled in HRPs compared with PWID not enrolled in HRPs was determined to be 0.48, which was determined by pooling evidence [16].
Scenarios
We simulated a total of eight scenarios, corresponding to differences in HRP enrollment and HCV testing, linkage to care, and SVR rates (Table 1). The status quo scenario (S1) represents the estimate of the HCV epidemic with no changes made to HRP enrollment, HCV screening and treatment. The status quo scenario (S1) represents the current cascade of care in the Chinese PWID population. Specifically in this scenario, the HRPs only cover 30% of active PWID, PWID admitted to HRPs are only tested once for HCV, and only 15% of PWID diagnosed with HCV receive the interferon-based treatment. Scenario S2 represents the recent breakthrough in HCV treatment. In this scenario, novel DAAs become the main treatment, but no changes are made to HRP enrollment, screening and treatment. Scenario S3 represents an enhanced linkage to care intervention scenario in which 30% of diagnosed HCV-infected PWID receive treatment. S4 and S5 represent the increased HCV screening frequency intervention in which PWID in HRPs are screened every 6 months and the linkage to care is set at 15% and 30%, respectively. Scenarios S6–S8 represent enhanced scenarios of the abovementioned interventions. Details of the intervention scenarios are provided in Table 1.
Model Analysis and Outcomes
The trends in HCV and its complications among China’s PWID from 2016 to 2030 were simulated using the model. The primary outcomes included HCV incidence and prevalence among China’s PWID, and the secondary outcomes were HCV-related complications, including DC, HCC and HCV-related deaths. We obtained estimates of HCV-related outcomes among PWID in China by 2030 under each intervention scenario and compared them to the status quo scenario (S1). We then considered which scenario is needed to reduce China’s HCV epidemic to low levels, as advocated by the WHO. The specific reduction goals included an 80% reduction in incidence and a 65% reduction in HCV-related death by 2030 compared with 2016 levels.
Sensitivity Analysis
We conducted a probabilistic sensitivity analysis by drawing 1000 samples from the prior distributions of important parameters. The model was run 1000 times with each parameter sampling, and medians and credible intervals (CrIs; 2.5th and 97.5th percentiles) for all quantities of interest were estimated (Table 2 and Table S2 in the Supplementary Information). One-way sensitivity analyses were also undertaken with a baseline scenario to test the impacts of several important parameters: initial prevalence of HCV among PWID, initial proportion of PWID enrolled in HRPs, enrollment and loss follow-up rates of HRPs, and time from infection to diagnosis for PWID enrolled in HRPs and not enrolled in HRPs. All analyses were performed using R (version 3.5.1) [17] and the packages deSolve [18], ggplot2 [19] and tidyverse [20].
Results
Impacts of the Different Intervention Scenarios on the Outcomes
Figure 2 presents the trends in projected HCV incidence and prevalence from 2016 to 2030 under different scenarios. Under current screening and treatment practices among PWID (scenario 1), we projected that the HCV incidence will show a gradual but slow declining trend from 12,970 in 2016 to 11,761 in 2030. All simulated scenarios were projected to accelerate the declining trends in HCV incidence, with scenario 8 having the most notable effect on HCV incidence, with it reducing from 12,437 in 2016 to 2311 in 2030, representing a 81.42% reduction [95% credible interval (CI) − 92.33%, − 52.56%]. Under the status quo scenario (S1), HCV prevalence was projected to show a gradual but increasing trend through 2030, with an increase from 239,187 in 2016 to 307,203 in 2030. All simulated scenarios except scenario 1 are expected to reduce the incidence of HCV by 2030. In 2030, the prevalence of HCV was predicted to decline by 28.83% (95% CI − 41.22%, − 9.24%) for scenario 2 and by 86.16% (95% CI − 97.22%, − 62.11%) for scenario 8 compared to prevalence rates noted in 2016.

Trends in the incidence and prevalence of HCV cases in different scenarios. A Incidence of HCV infections by scenario. B Prevalence of HCV infections by scenario
Impacts of the Intervention Scenarios Relative to the Status Quo Scenario (S1) on the Outcomes
Figure 3 illustrates the impacts of different intervention scenarios on total HCV incidence and prevalence in 2030 compared to S1. Scenarios S6–S8 with high HRP coverage and enhanced linkage to care were projected to result in a 47.05% to 80.35% reduction in HCV incidence compared with scenario 1. The reductions in DC, HCC, and HCV-related deaths were also substantial for the S6–S8 scenarios in 2030 compared with scenario S1. Among all simulated scenarios, increasing HRP coverage among PWID (S6–S8) was projected to have a greater impact in reducing HCV outcomes compared with scenarios with enhanced linkage to care (S3) or test frequency (S4–S5) alone. Table S2 and Fig. S1 in the Supplementary Information present the relative reduction in the cumulative number of new HCV infections and their complications from 2016 to 2030. Scenario S8 was the most effective intervention scenario. Compared to the status quo scenario (S1), scenario S8 was estimated to reduce new HCV infections by 47.39% (95% CI − 63.12%, − 29.32%), DC cases by 75.10% (95% CI − 88.32%, − 53.43%), HCC cases by 75.29% (95% CI − 95.76%, − 63.23%), and HCV-related deaths by 65.57% (95% CI − 97.32%, − 31.23%) from 2016 to 2030.

Relative change in HCV burden in 2030 among PWID for different interventions compared to the status quo scenario. A Total HCV incidence in 2030, B DC incidence in 2030, C HCC incidence in 2030, D HCV-related deaths in 2030. HCV hepatitis C, DC decompensated cirrhosis, HCC hepatocellular carcinoma
Impacts of the Different Intervention Scenarios on Achieving the WHO HCV Elimination Target
Table 2 demonstrates the impacts of the simulated scenarios on the HCV burden in 2030 relative to 2016. Compared to 2016, the HCV incidence was reduced by 81.42% (95% CI − 92.33%, − 52.56%) in scenario 8 and 9.33% (95% CI − 18.33%, 1.23%) in scenario 1 in 2030. Scenario 8 is the only intervention scenario that could achieve the WHO’s HCV elimination target. In this scenario, the HCV incidence in 2030 is projected to be reduced by 81.42% (95% CI − 92.33%, − 52.56%), and HCV-related deaths are projected to be reduced by 91.94% (95% CI − 99.76%, − 76.54%).
Sensitivity Analysis
Figure S2 in the Supplementary Information indicates the results of the sensitivity analysis on six parameters that produced variations in the prevalence and incidence in 2030 when we varied them across their uncertainty intervals. Both incidence and prevalence in 2030 are the most sensitive to the initial prevalence rate among PWID and the initial coverage rate of HRPs. The parameter time from infection to HCV diagnosis generally had limited impact on prevalence and incidence in 2030. Figure S2 in the Supplementary Information presents the results of a sensitivity analysis of six parameters that produced variations in other outcomes of interest in 2030.
Discussion
This study is the first modeling study to evaluate the potential impacts of different intervention strategies on HCV incidence, prevalence, advanced diseases and mortality among PWID in China. Several main findings can be derived from this modeling study. First, the HCV burden (i.e., incidence and prevalence) will continue to be substantial among PWID under current testing and treatment practice in China. Second, all simulated intervention scenarios (S2–S8) were projected to have an impact on reducing HCV burden among Chinese PWID, and the scenario of scaled-up HCV screening and treatment integrated with HRPs demonstrated the most substantial reduction in HCV burden. Third, our results suggest that substantial improvements in both testing and treatment integrated with existing HRPs are essential to achieve the WHO’s target of decreasing HCV incidence by 80% and HCV mortality by 65% among PWID in China by 2030.
Our modeling suggests that the incidence of HCV in Chinese PWID was already exhibiting a declining trend under current HCV screening and treatment practice in China. However, this decline is modest, and it will be difficult to achieve the WHO’s 2030 target based on the current rate. In addition, given the cumulative effect of existing infections, the prevalence of HCV and the HCV-related disease burden are projected to increase through 2030, imposing a substantial burden on the health care system. Since 2004, the Chinese government has gradually implemented HRPs with the initial aim of controlling human immunodeficiency virus (HIV) infection in PWID [21]. Although many studies have suggested that the combination of opioid substitution therapy (OST) and needle and syringe programs (NSP) can reduce HCV incidence by up to 80% [9, 22], studies in China suggested that harm reduction programs are more efficient at constraining HIV than HCV among PWID, and this finding may partially be due to the high HCV prevalence in and high probability of reinfection of PWID [23]. In addition, many modeling studies have suggested that the effectiveness of HRPs is closely related to their coverage [24, 25]. Moreover, by expanding HRPs to approximately 80% coverage, the HCV prevalence in various countries, such as the United Kingdom, is expected to decrease by 50%. However, 80% coverage will be very difficult to achieve for PWID and is unlikely to be sustained or funded by policy-makers [11]. Therefore, a substantial reduction in HCV burden in PWID cannot be achieved alone by HRPs, and novel intervention approaches are urgently needed.
Since 2016, a large body of modeling studies have estimated the type and level of interventions that are needed for HCV elimination among PWID in many countries, including Europe [26], Australia [27], Pakistan [28], and the United States [29]. These studies demonstrated that the increased use of DAAs over a short period could lead to the control of the HCV epidemic, especially when combined with OST/NSP interventions [30]. Our modeling study suggested that switching interferon-based treatment to DAAs alone (S2) may reduce the HCV incidence by 35.05% (95% CI − 49.77%, − 17.34%) in 2030 relative to 2016 and may reduce the HCV prevalence by 28.83% (95% CI − 41.22%, − 9.24%). However, HCV infection is a chronic disease that may cause long-term complications, and our modeling results suggested that changing interferon-based treatment to DAAs has a slight impact on the further burden of DC, HCV and HCV-related deaths. The introduction of DAAs in the context of current HCV testing and treatment practice may prevent HCV transmission. However, without expanded HCV testing and referral to treatment strategies, most PWID who are already infected with HCV will continue to progress to advanced liver disease. Our results suggest that the increased use of DAAs in combination with more case identification strategies (a high coverage of HRPs) or enhanced referral to treatment strategies could lead to a substantial reduction in HCV incidence as well as advanced HCV diseases in 2030.
PWID typically experience considerable stigma and discrimination and have poor access to regular health care, including HCV testing [31]. However, the well-designed HRPs in China may offer considerable opportunities to facilitate HCV intervention among PWID. According to the estimates of the National Health and Family Planning Commission in China, there were 184,000 OST and 56,000 NSP clients in 2015, accounting for 30% of all active PWID in China. Therefore, the integration of HCV screening and treatment into the existing HRPs for PWID in China may foster HCV testing and treatment. However, according to our modeling, expanding HRPs to cover at least 60% of active PWID and 90% of diagnosed PWID referred to DAA treatment (scenario 8) is crucial in order to reach the WHO’s elimination goal by 2030. Despite the challenges posed, some Western countries have achieved an HRP coverage of 64 per 100 clients [32], and there is evidence from studies to suggest that a high uptake of DAAs (90%) is attainable with government-subsidized modes [33]. Achieving this requires robust and sustained political commitment in order to overcome barriers such as limited HRP coverage and the high cost of DAAs.
Our model suggests that an increase in HCV testing frequency to twice a year may result in a substantial reduction in HCV burden, and expanding HRP coverage or enhancing the linkage to HCV treatment within HRPs may have more gains for PWID. With the advent of novel HCV testing (using point-of-care HCV screening tests), it is possible to quickly diagnose individuals and guide them to DAA treatment, even in the same visit (integration into existing HIV and drug health services). The current 12-week oral interferon-free DAA treatment for HCV may also reduce loss to follow-up and increase treatment completion among PWID.
This is the first model to explore the impacts of different HCV intervention scenarios on HCV burden among Chinese PWID. The findings suggest that scaled-up HCV screening and treatment among PWID is essential to reduce the HCV burden of Chinese PWID. Our results are based on model projections and must be interpreted with the recognition of several limitations. First, as noted in earlier studies of HCV among PWID, the data required to parameterize the model are lacking in China. We used data specific for China when available, and we also included large ranges of uncertainty for the parameters. Second, we failed to take into account the effects of HIV-HCV coinfection or other comorbidities, which may significantly alter HCV disease progression. Third, some of the assumptions are difficult to test. For example, we assumed homogeneous mixing due to insufficient data. In addition, we assumed that the reinfection risk is the same as the risk of primary infection, which may not hold in the real world. People may change their behaviors after primary HCV infection.
Conclusions
Our study indicates that achieving WHO elimination targets is a challenging aim that requires a substantial improvement in HCV testing and treatment among PWID (scenario S8). The findings indicate that coordinated improvements in testing, treatment, and harm reduction programs could greatly reduce the HCV burden among PWID in China, and they highlight the need for urgent policy changes to integrate HCV testing and treatment into existing HRPs.
References
The Polaris Observatory HCV Collaborators. Global change in hepatitis C virus prevalence and cascade of care between 2015 and 2020: a modelling study. Lancet Gastroenterol Hepatol. 2022;7:396–415.
Dusheiko G, Carey I. Global elimination of hepatitis C: a warning from the data. Lancet Gastroenterol Hepatol. 2022;7:380–1.
Thrift AP, El-Serag HB, Kanwal F. Global epidemiology and burden of HCV infection and HCV-related disease. Nat Rev Gastroenterol Hepatol. 2017;14:122–32.
Hajarizadeh B, Grebely J, Dore GJ. Epidemiology and natural history of HCV infection. Nat Rev Gastroenterol Hepatol. 2013;10:553–62.
WHO. Guidelines for the screening care and treatment of persons with chronic hepatitis C infection. Updated version, April 2016. Geneva: World Health Organization; 2016.
Robaeys G, Bielen R, Azar DG, Razavi H, Nevens F. Global genotype distribution of hepatitis C viral infection among people who inject drugs. J Hepatol. 2016;65:1094–103.
Bao Y, Larney S, Peacock A, et al. Prevalence of HIV, HCV and HBV infection and sociodemographic characteristics of people who inject drugs in China: a systematic review and meta-analysis. Int J Drug Policy. 2019;70:87–93.
Qin Q, Smith MK, Wang L, et al. Hepatitis C virus infection in China: an emerging public health issue. J Viral Hepatitis. 2015;22:238–44.
Platt L, Minozzi S, Reed J, et al. Needle and syringe programmes and opioid substitution therapy for preventing HCV transmission among people who inject drugs: findings from a Cochrane review and meta-analysis. Addiction. 2018;113:545–63.
Zou X, Ling L, Zhang L. Trends and risk factors for HIV, HCV and syphilis seroconversion among drug users in a methadone maintenance treatment programme in China: a 7-year retrospective cohort study. BMJ Open. 2015;5: e008162.
Vickerman P, Martin N, Turner K, Hickman M. Can needle and syringe programmes and opiate substitution therapy achieve substantial reductions in hepatitis C virus prevalence? Model projections for different epidemic settings. Addiction. 2012;107:1984–95.
National Anti-Drug Commission, China Anti-Drug Foundation. China's drug situation report 2016. 2016. http://www.nncc626.com/2017-03/27/c_129519255.htm. Accessed Nov 2022.
Ge L, Li D, Li P, Qu S, Chen F, Lyu F. HIV and HCV infection status among drug users—China, 2010–2018. China CDC Wkly. 2020;2:109–12.
National Health and Family Planning Commission of the People’s Republic of China. 2015 China AIDS response progress report. 2015. https://www.unaids.org/sites/default/files/country/documents/CHN_narrative_report_2015.pdf. Accessed Dec 2022.
Luo W, Li L, Kong JP, Wu ZY. A five-year prospective cohort study of HIV/HCV infections in community-related injecting drug users. Zhonghua Liu Xing Bing Xue Za Zhi. 2021;42:1067–70.
Turner KM, Hutchinson S, Vickerman P, et al. The impact of needle and syringe provision and opiate substitution therapy on the incidence of hepatitis C virus in injecting drug users: pooling of UK evidence. Addiction. 2011;106:1978–88.
R Core Team. R: a language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2022.
Soetaert K, Petzoldt T, Setzer RW. Solving differential equations in {R}: package de{S}olve. J Stat Softw. 2010;33:1–25.
Wickham H. ggplot2: elegant graphics for data analysis. New York: Springer; 2016.
Wickham H, Averick M, Bryan J, et al. Welcome to the tidyverse. J Open Source Softw. 2019;4:1686.
Wu Z, Wang Y, Detels R, Bulterys M. Towards ending HIV/AIDS among drug users in China. Addiction. 2015;110(l):1–3.
MacArthur GJ, van Velzen E, Palmateer N, et al. Interventions to prevent HIV and Hepatitis C in people who inject drugs: a review of reviews to assess evidence of effectiveness. Int J Drug Policy. 2014;25:34–52.
Ruan Y, Liang S, Zhu J, et al. Evaluation of harm reduction programs on seroincidence of HIV, hepatitis B and C, and syphilis among intravenous drug users in southwest China. Sex Transm Dis. 2013;40:323–8.
Stone J, Fraser H, Walker JG et al. Modelling the impact of HIV and HCV prevention and treatment interventions among people who inject drugs in Kenya. AIDS. 2022;36:2191–201.
Fraser H, Stone J, Wisse E, et al. Modelling the impact of HIV and HCV prevention and treatment interventions for people who inject drugs in Dar es Salaam. Tanzania J Int AIDS Soc. 2021;24: e25817.
Fraser H, Martin NK, Brummer-Korvenkontio H, et al. Model projections on the impact of HCV treatment in the prevention of HCV transmission among people who inject drugs in Europe. J Hepato. 2018;68:402–11.
Scott N, McBryde ES, Thompson A, Doyle JS, Hellard ME. Treatment scale-up to achieve global HCV incidence and mortality elimination targets: a cost-effectiveness model. Gut. 2017;66:1507–15.
Lim AG, Walker JG, Mafirakureva N, et al. Effects and cost of different strategies to eliminate hepatitis C virus transmission in Pakistan: a modelling analysis. Lancet Glob Health. 2020;8:e440–50.
Fraser H, Vellozzi C, Hoerger TJ, et al. Scaling up hepatitis C prevention and treatment interventions for achieving elimination in the United States: a rural and urban comparison. Am J Epidemiol. 2019;188:1539–51.
Blake A, Smith JE. Modeling hepatitis C elimination among people who inject drugs in New Hampshire. JAMA Netw Open. 2021;4: e2119092.
Grebely J, Dore GJ, Morin S, Rockstroh JK, Klein MB. Elimination of HCV as a public health concern among people who inject drugs by 2030—what will it take to get there? J Int AIDS Soc. 2017;20:22146.
Larney S, Peacock A, Leung J, et al. Global, regional, and country-level coverage of interventions to prevent and manage HIV and hepatitis C among people who inject drugs: a systematic review. Lancet Glob Health. 2017;5:e1208–20.
Wade AJ, Doyle JS, Gane E, et al. Outcomes of treatment for hepatitis C in primary care, compared to hospital-based care: a randomized, controlled trial in people who inject drugs. Clin Infect Dis. 2020;70:1900–6.
Acknowledgements
Funding
This work was supported by the National Natural Science Foundation of China (71904170), the Fundamental Research Funds for the Central Universities (2022ZFJH003) and the Mega-Project of National Science and Technology for the 13th Five-Year Plan of China (2018ZX10715013-003-003). The rapid service fee was funded by the authors.
Author Contributions
Conception and design: Jie Wu, Kailu Fang. Financial support: Jie Wu. Administrative support: Hong-liang Wang, Yushi Lin, Shuwen Li. Acquisition of data: Kailu Fang. Data analysis and interpretation: Kailu Fang, Yushi Lin, Shuwen Li. Manuscript writing: Jie Wu, Kailu Fang. Critical revision of the manuscript for important intellectual content. Jie Wu, Hong-liang Wang. All authors read and approved the final version of the article, including the authorship list.
Disclosures
All the authors, including Kailu Fang, Hong-liang Wang, Yushi Lin, Shuwen Li and Jie Wu, have nothing to disclose.
Compliance with Ethics Guidelines
The analysis in this article is based on previously publicly available data and does not involve any new studies of human or animal subjects performed by any of the authors.
Data Availability
All data relevant to the study are included in the article or uploaded as supplementary information.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Fang, K., Wang, Hl., Lin, Y. et al. Modeling the Impacts of Prevention and Treatment Interventions on Hepatitis C Among People Who Inject Drugs in China. Infect Dis Ther 12, 1043–1055 (2023). https://doi.org/10.1007/s40121-023-00779-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40121-023-00779-0