
Abstract
Metabolic imbalance in chronic diseases such as type-1 diabetes may lead to detectable perturbations in the molecular composition of residual skin surface components (RSSC). This study compared the accumulation rate and the composition of RSSC in type-1 diabetic patients with those in matched controls in order to identify potential biomarkers of the disease. Samples of RSSC were collected from the foreheads of type-1 diabetic (n = 55) and non-diabetic (n = 58) volunteers. Samples were subsequently analysed to identify individual components (sebomic analysis). There was no significant difference in the rate of accumulation of RSSC between type-1 diabetics and controls. In terms of molecular composition, 171 RSSC components were common to both groups, 27 were more common in non-diabetics and 18 were more common in type-1 diabetic patients. Statistically significant (P < 0.05) differences between diabetic and non-diabetic volunteers were observed in the recovered amounts of one diacylglyceride (m/z 594), six triacylglycerides (m/z 726–860) and six free fatty acids (m/z 271–345). These findings indicate that sebomic analysis can identify differences in the molecular composition of RSSC components between type-1 diabetic and non-diabetic individuals. Further work is required to determine the practical utility and identity of these potential biomarkers.
Similar content being viewed by others


Introduction
The human integument is coated with a thin layer comprising sebum, sweat, corneocyte debris and natural moisturising factors. Whilst generically referred to as sebum, the mixture is more accurately referred to as “residual skin surface components” or RSSC1.
Changes in the molecular composition of RSSC may arise as a result of local and/or systemic disease states2,3,4. Indeed, clinical conditions such as acne are associated with changes in both the secretion rate and the composition of sebum (Table 1). In addition, perturbations in the rate of sebum secretion have also been reported for hypothyroidism5, Turner syndrome6, Behçet’s syndrome7, Parkinson’s disease8 and rheumatoid arthritis7. Thus, the detection and quantification of disease-specific molecules present on the skin surface offer potential for the development of non-invasive diagnostic and prognostic techniques.
Decreases in sebum secretion rates have previously been reported for diabetes mellitus9, 10. However, to date there are no reports of specific biochemical changes in RSSC associated with chronic disease conditions such as type-1 diabetes. Thus, the aim of this human volunteer study was to identify any differences in the secretion rate or composition of RSSC between type-1 diabetic and non-diabetic volunteers. The rationale for specifically considering type-1 diabetic patients in the current study was related to the lack of insulin observed in these individuals11, 12. Decreased insulin levels may affect lipid synthesis in the sebaceous glands, as insulin is considered to be an essential hormone for the normal growth and differentiation of sebaceous gland cells13. A successful outcome to this pilot study would provide proof of principle, allowing the design of further studies to investigate non-invasive biomarkers of type-1 diabetes present in RSSC that may have diagnostic or prognostic application. This study is novel in its approach to identifying diabetic patients based on skin lipid composition. Therefore, a broad method of analysis was required to allow for the detection of unknown lipid molecules and the identification of potential biomarkers (which are subject to future confirmatory studies).
Results
Rate of RSSC accumulation
The rate of RSSC accumulation did not differ significantly (P > 0.05, Mann–Whitney test) between type-1 diabetic (0.12 ± 0.06 mg cm−2, n = 55) and non-diabetic (0.13 ± 0.06 mg cm−2, n = 58) volunteers. There was no significant correlation (r2 = 0.004, P > 0.05, n = 51) between the amount of RSSC recovered and the clinically-confirmed duration of diabetes (data not shown). Blood concentrations of HbA1c in type-1 diabetic volunteers did not correlate (r2 = 0.001, P > 0.05, n = 54) significantly with the amount of RSSC recovered (data not shown).
Composition of RSSC
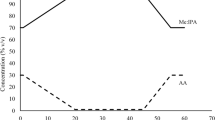
Analysis of RSSC by high-performance liquid chromatography (HPLC) with atmospheric pressure chemical ionization (APCI) mass spectrometry (MS) presented complex chromatograms indicating the presence of several RSSC components. A representative chromatogram constructed using the normalised abundance of compound ions is shown in Fig. 1.

Representative chromatogram of human residual skin surface components. Distributions were reconstructed based on the normalised abundance of compound ions detected in both positive and negative ionisation analysis (A) and negative ionisation analysis only (B); showing inset zoom-in) by high performance liquid chromatography with atmospheric pressure chemical ionization mass spectrometry.
In total, 216 compound ions were consistently identified from samples of RSSC recovered from type-1 diabetic and non-diabetic participants: the majority (78%) were detected in positive ion mode, with the remainder (22%) in negative ion mode (Fig. 2).

Commonalities and differences in the number of compound ions detected in positive ionisation (bold) and negative ionisation (italics) mode between type-1 diabetic (n = 44) and non-diabetic (n = 58) residual skin surface component samples.
There were 171 compound ions common to both type-1 diabetic and non-diabetic RSSC. The majority (145) were detected in LC-MS positive ionisation mode, with 26 detected in negative ionisation mode (Fig. 2). The normalised abundance of 2 of the 145 common positive ions identified as triglycerides was more than twofold higher (P < 0.05) in non-diabetic volunteers (Table 2). No significant difference (P > 0.05) was observed in the normalised abundance of the 26 common negative ions.
Twenty-two positive compound ions were consistently present only in the RSSC of non-diabetic volunteers (Fig. 2), of which five (1 diglyceride and 4 triglycerides) had a normalised abundance that was more than twofold higher (P < 0.05) than that of type-1 diabetic volunteers (Table 2). Two positive ion compounds were consistently present only in type-1 diabetic volunteers. However, the normalised abundance of these compound ions did not differ significantly between the two groups (P > 0.05). In negative ionisation mode, five compound ions were consistently present only in RSSC recovered from non-diabetic volunteers (Fig. 2). No significant difference (P > 0.05) was observed in the normalised abundance of these five negative ions. A further 16 compound ions were consistently present only in the type-1 diabetic volunteers; the normalised abundance of six of these compound ions (all free fatty acids) was more than twofold higher (P < 0.05) than in non-diabetic volunteers (Table 3).
Discussion
This study identified a number of significant differences in the composition of RSSC recovered from type-1 diabetic and non-diabetic volunteers. In particular, there were significant perturbations in the frequency and abundance of certain free fatty acids and (di and tri) glycerides. However, this study identified no diabetes-related effects in the rate of accumulation of RSSC. Moreover, the duration and severity (measured by HbA1c) of type-1 diabetes also showed no correlation with the rate of accumulation of RSSC. Thus, there appear to be subtle differences in the composition but not the quantity of RSSC secreted by type-1 diabetic and non-diabetic individuals.
The rationale for specifically considering type-1 diabetic patients in the current study was related to the lack of insulin observed in these individuals11, 12. Decreased insulin levels in these individuals may affect lipid synthesis in the sebaceous glands, as insulin is considered to be an essential hormone for the normal growth and differentiation of sebaceous gland cells13. A level of biomarker HbA1c ≥ 47.5 mmol mol−1 indicates the presence of diabetes14, 15. In clinically diagnosed diabetic patients, a level of HbA1c below 53.0 mmol mol−1 can be considered as good control of diabetes, whereas a level exceeding 53.0 mmol mol−1 is generally considered poor16. Non-physiological insulin profiles have been reported in patients with apparently well controlled diabetes17. Insulin is also known to affect the differentiation and proliferation of keratinocytes in rats13, 18 and it has been suggested that abnormal insulin signalling may also contribute to the dermal manifestations of diabetes19. In sebocytes, insulin exerts its effects through insulin-like growth factor-I receptors and upregulation of sterol regulatory element-binding proteins that, in turn, stimulate lipogenesis in sebocytes20. Insulin is also necessary for maximising the effect of growth hormone13. Given these multiple potential pathways through which abnormal insulin levels may affect sebum production, differences in sebum production between diabetic and non-diabetic individuals would appear to be a physiological inevitability. The evidence from the studies cited above would tend to predict a decrease in sebum secretion in response to low levels of insulin.
This study built on previous work that showed a decrease in the rate of sebum secretion in diabetic rats21 and humans9, 21. One previous study9 measured casual sebum levels using the Sebumeter™ technique; however, a limitation was the potential for sample-site contamination. In the present study, the subject’s forehead was cleaned before sample collection and protected for the duration of sample acquisition to ensure the measurement of RSSC accumulation was not unintentionally influenced by contamination of the measurement site, as per current recommendations and guidance21,22,23,24,25.
The results obtained in this study did not demonstrate any difference in the rate of accumulation of RSSC between type-1 diabetic and non-diabetic individuals, but did detect significant differences in composition. This is in agreement with a previous investigation that demonstrated no changes in the histological appearance of sebaceous glands, although a decrease in triglyceride synthesis following the onset of diabetes has been reported in mice26. The treatment with exogenous insulin in type-1 diabetic patients may be responsible for the non-significant difference in the rate of RSSC accumulation between the two groups (although according to the HbA1c data, diabetes was not well controlled in the majority of the individuals).
The biomarker HbA1c is a form of haemoglobin modified by the non-enzymatic attachment of glucose. As the lifespan of an erythrocyte is normally around 120 days27, HbA1c reflects average plasma glucose levels over an eight- to twelve-week period28. Sebocyte differentiation and sebum production normally takes 21–25 days29 and so the HbA1c marker provides a good indication of blood glucose over several sebum production cycles. In the current study, no correlation was observed between HbA1c level and the rate of RSSC accumulation. This result is in alignment with the observations of Sakai et al.10 in human subjects. The lack of correlation between HbA1c and RSSC recovery may be explained by the fact that HbA1c represents the overall accumulation of excess glucose and so does not take into account the dynamic nature of blood glucose concentrations, which may stimulate or inhibit the rate of sebum production.
Sebomic analysis using LC-MS indicated that several components of RSSC were common to type-1 diabetic and non-diabetic volunteers. However, the normalised abundance of two common triglycerides was higher in non-diabetic volunteers (Table 2). In addition to these components, one diglyceride and four triglycerides showed a higher prevalence (as well as an increased abundance) in non-diabetic volunteers. Such variability in the composition of RSSC may partly be attributable to the availability of substrates for lipogenesis pathways. Sebaceous glands use various substrates for lipid synthesis, including lactate, acetate, amino acids and glucose30, 31. Sebaceous glands also contain elevated concentrations of glycogen30. Studies using radioactive glucose with isolated sebaceous glands have demonstrated that glucose is incorporated into all sebaceous lipid classes32. However, the rate of incorporation of glucose is approximately half that of lactate and acetate30. Using lactate and acetate as precursors, the rate of squalene and wax ester synthesis is significantly higher than with glucose, whereas triglyceride synthesis is unaffected30. Lipids synthesised from glucose and lactate are very similar in composition33. Therefore, the effect of glucose on lipid synthesis could potentially alter RSSC composition, as postprandial hyperglycaemia and nocturnal hypoglycaemia are usually observed even in patients with well controlled type-1 diabetes34, 35. It is likely that diabetic patients use the same metabolic pathways of lipid synthesis as non-diabetics, but subtle differences in the availability of substrates for lipogenesis (caused by glucose imbalance) may introduce variability in the composition of sebum, which may explain the reduced abundance of diglycerides and triglycerides identified in the current study. Further work is required to investigate the effect of blood glucose concentrations on sebaceous gland activity in order to elucidate the mechanism through which glucose may influence the composition of skin surface lipids.
Interestingly, the abundance and prevalence of six fatty acids were greater in the diabetic group (Table 3), most probably as the result of increased lipase activity. Microbial lipase is responsible for the metabolism of triglycerides, resulting in the release of free fatty acids on the skin surface36, 37. A greater number of micro-organisms have been isolated from the skin surface of diabetic compared with non-diabetic individuals38. Enhanced lipase activity as a consequence of increased microbial density on the skin of diabetic patients may, therefore, be responsible for the higher abundance of fatty acids in diabetic volunteers observed in the current study. In contrast, non-diabetic volunteers would be expected to have a higher abundance of triglycerides on the skin surface, due to a correspondingly lower lipase activity: this was observed in the current study. A concurrent increase in diglyceride abundance (due to microbial hydrolysis of triglycerides) would also be expected in diabetic patients39. However, the only detectable change measured in this current study was a decrease in the normalised abundance of one diglyceride in diabetic patients (Table 2). This apparent anomaly cannot be explained without robust identification of this component and further work is required to identify alternative routes of diglyceride synthesis that might explain this result.
Whilst it is tempting to speculate that the statistically significant differences in RSSC composition measured in this present study may provide a basis for developing a non-invasive, diagnostic indicator of type-1 diabetes, further work is clearly required to (1) confirm the identity of the compound ions that differ between diabetic and non-diabetic individuals, and (2) identify the mechanism(s) underpinning the compositional differences between the diabetic and non-diabetic groups. Prior to instigating the study, no information existed regarding whether or which skin lipids were indicative of a diabetic condition; therefore, we were obliged to adopt a broad method of analysis. This effectively precluded the use of specific internal standards and external reference samples from which we could confirm the exact identity of the biomarkers putatively identified in this pilot study. Such pilot studies are important in identifying new areas of research that may have future impact. Thus, preliminary studies such as ours need to adopt an inherently flexible methodology to allow the detection of unknown outcomes, which would otherwise be precluded by adopting a hypothesis-driven approach that might limit detection to “known” lipid molecules. Sebomic analysis of RSSC may represent a promising strategy for identifying biomarkers of other chronic diseases that are known to be associated with changes in sebaceous gland biochemistry. For example, the presence of phosphorylated tau protein in the cytoplasm of sebaceous glands and altered sebum secretion rates have been reported in Alzheimer’s40 and Parkinson’s disease8.
In conclusion, a comparison of RSSC collected from type-1 diabetic and non-diabetic volunteers did not show differences in the rate of RSSC accumulation. However, significant differences in the composition of RSSC were noted between type-1 diabetic and non-diabetic individuals. The observed variability in the RSSC composition of diabetic volunteers may be indicative of an altered availability of substrates for lipogenesis. However, bacterial lipase activity is also likely to be a contributory factor in the decreased recovery of triglycerides and corresponding increase in free fatty acids observed in the RSSC of diabetic individuals. This study supports the feasibility of using RSSC as a non-invasive biomarker of type-1 diabetes.
Methods
This study was conducted in accordance with the principles of the Declaration of Helsinki and was independently approved by the NHS South Central–Hampshire A Research Ethics Committee.
Volunteers
Ethical approval to collect RSSC from non-diabetic volunteers was granted by the School of Pharmacy and Postgraduate Medicine Ethics Committee with Delegated Authority, University of Hertfordshire, Hatfield, UK (ethics approval number: PHAEC/10-25). For the collection of RSSC from type-1 diabetic patients, ethical approval was obtained from the National Research Ethics Service (NRES) Committee London-Bloomsbury (ethics approval number: 13/LO/1196). Collection of RSSC from non-diabetic volunteers was performed at the University of Hertfordshire (UK) while patients with clinically diagnosed type-1 diabetes were recruited at Watford General Hospital (UK) and Hemel Hempstead Hospital (UK). All volunteers participating in the study provided written informed consent. Demographic data were obtained using a questionnaire. Clinical information (e.g. duration of illness, glycated haemoglobin [HbA1c] blood concentrations, current medication, etc.) was obtained from each type-1 diabetic patient’s hospital record. Patients in the type-1 diabetic group remained on exogenous insulin treatment throughout the experiment. Type-1 diabetic and non-diabetic groups were matched as far as possible for age and sex. Previous studies1, 41 have indicated that the rate of RSSC production is not affected by an individual’s ethnicity. Table 4 summarises the self-reported demographics of all participants.
Collection of RSSC
Collection of RSSC from volunteers was performed using a previously validated cigarette paper method1, 42 over a four-month period (February-June, 2014). Briefly, volunteers were allowed to acclimatise to the study room conditions (18–26 °C, 50–60% relative humidity) for at least 15 minutes before their forehead was cleaned with an isopropyl alcohol-based wipe (Fastaid™, Robinsons Healthcare, Worksop, UK) prior to the application of four pieces of dry, pre-weighed cigarette paper (previously washed with diethyl ether). Each paper was covered with a piece of aluminium foil which was fixed to the forehead using Micropore™ (3 M UK Plc., Bracknell, UK) adhesive tape. This assembly was held in place with an elastic head band. After removal from the forehead, the cigarette papers were dehydrated (by passive evaporative loss) in plastic sample cups covered with pierced Parafilm™ in a fume cupboard for a minimum period of two hours prior to storage at ambient temperature.
Analysis of RSSC
The rate of RSSC production was determined by gravimetric analysis performed using a 10-µg resolution fine balance (Mettler Toledo AX205; Mettler-Toledo Ltd., Leicester, UK) placed on a vibration-proof table. The balance was encased in a weighing cabinet (Bigneat Ltd., Hampshire, UK) to reduce draught artefacts. Each piece of cigarette paper was weighed before and after RSSC collection, the difference in weight being ascribed to RSSC recovered from the skin surface.
To identify compositional differences, RSSC present on the cigarette papers was extracted using hexane. The solvated RSSC samples were then dried by purging with nitrogen gas until all the hexane was visibly removed. The dried sample was then resuspended in 1 mL chloroform:methanol (2:1) using a roller mixer (Stirling mixer, Sandrest Ltd., Sussex, UK) for a minimum period of two hours. The sample was then transferred to a clean vial for LC-APCI-MS analysis. Chemical analysis was performed using a ThermoScientific™ Ultimate 3000 HPLC system, comprising an RS 3000 quaternary pump, Ultimate 3000 RS auto-sampler and a column oven, connected to a ThermoScientific™ MSQ™ single quadrupole mass spectrometer (Thermo Fisher Scientific, Hemel Hempstead, UK). A reverse phase Zorbax SB C8 column (internal diameter 2.1 mm, length 150 mm, particle size 1.8 µm) was purchased from Agilent Technologies (Berkshire, UK) and used for chromatographic separation. The column was maintained at a temperature of 60 °C. The mobile phase was drawn from reservoirs containing 95:5 methanol:isopropyl alcohol (A) and 10 mM aqueous ammonium acetate (B). A gradient program was employed to optimise chromatographic separation: 0–1 min: 70% A; 20 min: 99% A; 45 min: 99% A; 55 min: 70% A; 60 min 70% A. The mobile phase flow rate was maintained at 0.25 mL min−1 throughout the 60-min run time. The APCI technique was used for ion generation (corona discharge 3 kV, probe temperature 400 °C, cone voltage 50 V). Ions were scanned in the range of 100 to 1000 Da to obtain a total ion scan in both positive and negative ionisation modes. ThermoScientific™ Chromeleon (version 3.8) software was used for the instrument control, data collection and initial data processing.
The data acquired for each sample were subsequently converted to “raw” file format and processed using Progenesis QI software (Nonlinear Dynamics, Newcastle Upon Tyne, UK). Spectral data alignment, peak detection (“peak picking”), background subtraction, normalisation and comparison of normalised abundance was performed using automated algorithms provided by the Progenesis QI software. Peak detection was performed on the intensity of compound ions, excluding events with a chromatographic (peak) width of less than 0.1 min. The abundance of compound ions in each sample was normalised against the abundance of compound ions in a reference chromatogram. An automated algorithm within the Progenesis QI software was used to select the most representative chromatogram among all the samples for use as a reference chromatogram. The final list of compound ion abundances was transformed using an inverse hyperbolic (arcsinh) function. The transformed data were then used to calculate any significant differences in the normalised abundance between groups. Such an “omics” approach is widely used in fields like metabolomics and proteomics for the processing of extremely complex biological data to enable a system level understanding of molecular interactions and dependencies in biological systems43,44,45. The prevalence of compound ions in each volunteer group was calculated as a percentage. A compound ion which was present in more than 75% of the population of a group was considered as a characteristic feature of that group (referred to as a “consistent” compound ion). The 75% threshold was adopted from previous (proteomic and metabolomics) biomarker studies46,47,48. The normalised abundance of consistent compound ions was then compared between the type-1 diabetic and non-diabetic volunteers. Using the mass-to-charge ratio (m/z), the components of RSSC were putatively identified based on literature reports49 and lipid databases50, namely the LIPID Metabolites and Pathways Strategy (LIPID MAPS®) databases.
Statistical analysis
A commercially available software package (Statistical Package for the Social Sciences; SPSS Inc., Chicago, IL, USA, version 20) was used to perform the statistical analysis. The Kolmogorov–Smirnov test was used to determine the normality of the dataset and groups were compared by Mann–Whitney test. The transformed normalised abundance of compound ions detected in LC-APCI-MS analysis was compared by t-test using Progenesis QI software. A P-value < 0.05 was considered to be significant.
References
Shetage, S. S. et al. Effect of ethnicity, gender and age on the amount and composition of residual skin surface components derived from sebum, sweat and epidermal lipids. Skin Res Technol 20, 97–107 (2014).
Paliwal, S., Hwang, B. H., Tsai, K. Y. & Mitragotri, S. Diagnostic opportunities based on skin biomarkers. Eur J Pharm Sci 50, 546–556 (2013).
Elias, P. M. Epidermal lipids, barrier function, and desquamation. J. Invest. Dermatol. 80, 44s–49s (1983).
Patel, L. M., Lambert, P. J., Gagna, C. E., Maghari, A. & Lambert, W. C. Cutaneous signs of systemic disease. Clin. Dermatol. 29, 511–522 (2011).
Goolamali, S. K., Evered, D. & Shuster, S. Thyroid disease and sebaceous function. Br Med J 1, 432–433 (1976).
Brazzelli, V. et al. Reduced sebum production in Turner syndrome: a study of twenty-two patients. Int J Immunopathol Pharmacol 24, 789–792 (2011).
Yazici, H. et al. Sebum production is increased in Behçet’s syndrome and even more so in rheumatoid arthritis. Clin. Exp. Rheumatol. 5, 371–374 (1987).
Pochi, P. E., Strauss, J. S. & Mescon, H. Sebum production and fractional 17-ketosteroid excretion in parkinsonism. J. Invest. Dermatol. 38, 45–51 (1962).
Seirafi, H. et al. Biophysical characteristics of skin in diabetes: a controlled study. J Eur Acad Dermatol Venereol 23, 146–149 (2009).
Sakai, S., Kikuchi, K., Satoh, J., Tagami, H. & Inoue, S. Functional properties of the stratum corneum in patients with diabetes mellitus: similarities to senile xerosis. Br. J. Dermatol. 153, 319–323 (2005).
American Diabetic Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 31(Suppl 1), S55–S60 (2008).
Alberti, K. G. & Zimmet, P. Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet. Med. 15, 539–553 (1998).
Deplewski, D. & Rosenfield, R. L. Growth hormone and insulin-like growth factors have different effects on sebaceous cell growth and differentiation. Endocrinology 140, 4089–4094 (1999).
American Diabetic Association. Standards of medical care in diabetes—2012. Diabetes Care 35(Suppl 1), S11–S63 (2012).
Farmer, A. Use of HbA1c in the diagnosis of diabetes. BMJ 345, e7293 (2012).
American Diabetic Association. 5. Glycemic targets. Diabetes Care 39(Suppl 1), S39–S46 (2016).
Olsson, P. O., Arnqvist, H. & von Schenck, H. Free insulin profiles in insulin-dependent diabetics treated with one or two insulin injections per day. Acta Med Scand 220, 133–141 (1986).
Spravchikov, N. et al. Glucose effects on skin keratinocytes: implications for diabetes skin complications. Diabetes 50, 1627–1635 (2001).
Wertheimer, E. et al. Differential roles of insulin receptor and insulin-like growth factor-1 receptor in differentiation of murine skin keratinocytes. J. Invest. Dermatol. 115, 24–29 (2000).
Smith, T. M., Cong, Z., Gilliland, K. L., Clawson, G. A. & Thiboutot, D. M. Insulin-like growth factor-1 induces lipid production in human SEB-1 sebocytes via sterol response element-binding protein-1. J. Invest. Dermatol. 126, 1226–1232 (2006).
Toh, Y. C. Effect of streptozotocin-induced diabetes on the activity of the sebaceous glands in rats. Endokrinologie 80, 56–59 (1982).
Piérard, G. E., Piérard-Franchimont, C., Marks, R., Paye, M. & Rogiers, V. EEMCO guidance for the in vivo assessment of skin greasiness. The EEMCO Group. Skin Pharmacol. Appl. Skin Physiol. 13, 372–389 (2000).
Clarys, P. & Barel, A. Quantitative evaluation of skin surface lipids. Clin. Dermatol. 13, 307–321 (1995).
El Gammal, C., El Gammal, S., Pagnoni, A., Kligman, A.M. Quantification of sebum output using sebum-absorbent tapes (Sebutapes®) in Handbook of non-invasive methods and the skin, Second Edition (eds. Serup, J., Jemec, G. B. E. & Grove, G. L.) 835–840 (CRC Press, 2006).
Ayres J. D. Methods for evaluating sebum removal in Cosmetic claims substantiation (ed. Aust, L.) 115–130 (Marcel Dekker, 1997).
Sakai, S. et al. Characteristics of the epidermis and stratum corneum of hairless mice with experimentally induced diabetes mellitus. J. Invest. Dermatol. 120, 79–85 (2003).
Shemin, D. & Rittenberg, D. The life span of the human red blood cell. J. Biol. Chem. 166, 627–636 (1946).
Nathan, D. M., Turgeon, H. & Regan, S. Relationship between glycated haemoglobin levels and mean glucose levels over time. Diabetologia 50, 2239–2244 (2007).
Plewig, G. & Christophers, E. Renewal rate of human sebaceous glands. Acta Derm. Venereol. 54, 177–182 (1974).
Middleton, B., Birdi, I., Heffron, M. & Marsden, J. R. The substrate determines the rate and pattern of neutral lipid synthesized by isolated human sebaceous glands. FEBS Lett. 231, 59–61 (1988).
Im, M. J. & Hoopes, J. E. Enzymes of carbohydrate metabolism in normal human sebaceous glands. J. Invest. Dermatol. 62, 153–160 (1974).
Cassidy, D. M., Lee, C. M., Laker, M. F. & Kealey, T. Lipogenesis in isolated human sebaceous glands. FEBS Lett. 200, 173–176 (1986).
Downie, M. M. & Kealey, T. Lipogenesis in the human sebaceous gland: glycogen and glycerophosphate are substrates for the synthesis of sebum lipids. J. Invest. Dermatol. 111, 199–205 (1998).
Tamborlane, W. V. et al. Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group Continuous glucose monitoring and intensive treatment of type 1 diabetes. N. Engl. J. Med. 359, 1464–1476 (2008).
Bode, B. W., Schwartz, S., Stubbs, H. A. & Block, J. E. Glycemic characteristics in continuously monitored patients with type 1 and type 2 diabetes: normative values. Diabetes Care 28, 2361–2366 (2005).
Marples, R. R., Downing, D. T. & Kligman, A. M. Control of free fatty acids in human surface lipids by Corynebacterium acnes. J. Invest. Dermatol. 56, 127–131 (1971).
Cove, J. H., Holland, K. T. & Cunliffe, W. J. An analysis of sebum excretion rate, bacterial population and the production rate of free fatty acids on human skin. Br. J. Dermatol. 103, 383–386 (1980).
Pam, S. D., Mawak, J. D. & Chuhwak, E. K. Bacterial skin flora of diabetic patients in the Jos University Teaching Hospital. Jos. J Med Trop 7, 9–13 (2005).
Rebillo, T. & Hawk, J. L. Skin surface glycerol levels in acne vulgaris. J. Invest. Dermatol. 70, 352–354 (1978).
Rodriguez-Leyva, I. et al. Presence of phosphorylated tau, alpha-synuclein and amyloid protein in the skin of patients with clinical diagnosis of Alzheimer disease. Neurology 82(S38), 003 (2015).
Luther, N., Darvin, M. E., Sterry, W., Lademann, J. & Patzelt, A. Ethnic differences in skin physiology, hair follicle morphology and follicular penetration. Skin Pharmacol Physiol 25, 182–191 (2012).
Strauss, J. S. & Pochi, P. E. The quantitative gravimetric determination of sebum production. J Invest Dermatol 36, 293–298 (1961).
Zhang, X., Asara, J. M., Adamec, J., Ouzzani, M. & Elmagarmid, A. K. Data pre-processing in liquid chromatography-mass spectrometry-based proteomics. Bioinformatics 21, 4054–4059 (2005).
Di Luca, A., Henry, M., Meleady, P. & O’Connor, R. Label-free LC-MS analysis of HER2+ breast cancer cell line response to HER2 inhibitor treatment. Daru 23, 40 (2015).
Liu, F. et al. UPLC/Q-TOFMS-Based Metabolomics Studies on the Protective Effect of Panax notoginseng Saponins on Alcoholic Liver Injury. Am. J. Chin. Med. 43, 695–714 (2015).
Gruber, M. et al. Analysis of exhaled breath for diagnosing head and neck squamous cell carcinoma: a feasibility study. Br. J. Cancer 111, 790–798 (2014).
Miller, J. C. et al. Antibody microarray profiling of human prostate cancer sera: antibody screening and identification of potential biomarkers. Proteomics 3, 56–63 (2003).
Sato, Y. et al. Identification of a new plasma biomarker of Alzheimer’s disease using metabolomics technology. J. Lipid Res. 53, 567–576 (2012).
Camera, E., Ludovici, M., Galante, M., Sinagra, J. L. & Picardo, M. Comprehensive analysis of the major lipid classes in sebum by rapid resolution high-performance liquid chromatography and electrospray mass spectrometry. J. Lipid Res. 51, 3377–3388 (2010).
Sud, M. et al. LMSD: LIPID MAPS structure database. Nucleic Acids Res. 35, D527–D532 (2007).
Youn, S-W., Park, E. S., Lee, D. H., Huh, C. H. & Park, K. C. Does facial sebum excretion really affect the development of acne? British Journal of Dermatology 153(5), 919–924 (2005).
Pappas, A., Johnsen, S., Liu, J-C. & Eisinger, M. Sebum analysis of individuals with and without acne. Dermato-Endocrinology 1(3), 157–161 (2014).
Harris, H. H., Downing, D. T., Stewart, M. E. & Strauss, J. S. Sustainable rates of sebum secretion in acne patients and matched normal control subjects. Journal of the American Academy of Dermatology 8(2), 200–203 (1983).
Piérard-Franchimont, C., Piérard, G. E., Saint-Léger, D., Lévêque, J.L., Kligman, A.M. Comparison of the Kinetics of Sebum Secretion in Young Women with and without Acne. Dermatology 183(2), 120–122 (2004).
Leyden, J. J. New understandings of the pathogenesis of acne. Journal of the American Academy of Dermatology 32(5), S15–S25 (1995).
Pochi, P. E., Strauss, J. S. & Downing, D. T. Age-related Changes in Sebaceous Gland Activity. Journal of Investigative Dermatology 73(1), 108–111 (1979).
Acknowledgements
The authors would like express their gratitude to all volunteers, with special thanks to Watford General Hospital (UK) and Hemel Hempstead Hospital (UK) for their participation in this study.
Author information
Authors and Affiliations
Contributions
S.S., M.T., M.B., T.G. and R.C. contributed equally to the design and execution of the study. S.S., M.T., M.B., T.G. and R.C. reviewed and approved the manuscript. R.C. supervised the study and accepts responsibility as the corresponding author.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shetage, S.S., Traynor, M.J., Brown, M.B. et al. Application of sebomics for the analysis of residual skin surface components to detect potential biomarkers of type-1 diabetes mellitus. Sci Rep 7, 8999 (2017). https://doi.org/10.1038/s41598-017-09014-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-09014-6
- Springer Nature Limited