
Abstract
Early progressive mobilization is a safe strategy in the intensive care unit (ICU), however, it is still considered challenging by the inherent barriers and poor adherence to early mobilization protocol. The aim of this study was to evaluate the effectiveness of a quality improvement (QI) multifaceted strategy with implementation of a specific visual tool, the “mobility clock”, in reducing non-compliance with the institutional early mobilization (EM) protocol in adult ICUs. A single-center QI with a retrospective before-after comparison study was conducted using data from medical records and hospital electronic databases. Patients from different periods presented similar baseline characteristics. After the QI strategy, a decline in “non-compliance” with the protocol was observed compared to the previous period (10.11% vs. 26.97%, p < 0.004). The proportion of patients walking was significantly higher (49.44% vs. 29.21%, p < 0.006) and the ICU readmission rate was lower in the “after” period (2.25% vs. 11.24%; p = 0.017). The multifaceted strategy specifically designed considering institutional barriers was effective to increase out of bed mobilization, to reduce the “non-compliance” rate with the protocol and to achieve a higher level of mobility in adult ICUs of a tertiary hospital.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
The continuous improvement in critical illness survival has led to increasing recognition of the long-term consequences of therapy in intensive care unit (ICU). This repercussion goes beyond the physical aspect and extends to social, cognitive, and mental health function1. At present, ABCDE bundle is considered a remarkable strategy to optimize ICU care recovery and outcomes2. Early progressive mobilization, represented as the “E” bundle component is a safe strategy to reduce ICU-acquired weakness (ICU-AW), which can cause a direct impairment of functional status. That condition can perpetuate after hospital discharge, affecting the quality of life and social reintegration1,2,3,4,5,6,7,8,9.
Although mobilization is considered essential and recommended to start immediately after physiologic stabilization, the number of patients in compliance with this recommendation that are mobilized out of bed is considered low and is less than predicted by known safety criteria and patient clinical condition10,11. In the ICU environment there are multifactorial barriers related to the structural context, process, culture, in addition to patient-related factors7,10,11,12,13,14,15. The improvement of patient’s mobility level must consider all those barriers present at the moment14 and, therefore, setting strategies to overcome them with a multidisciplinary approach towards early mobilization (EM) is recommended14,15,16,17,18,19,20,21,22,23,24.
The first EM protocol in our institution was developed in adult ICUs in 2011, and its use started in that same year. It contained four progressive intervention plans, the Medical Research Council (MRC) grading system and the Surgical Unit Optimal Mobilization Score (SOMS) were used, respectively, in patients who are alert and attentive and in those who were unable to follow commands25.
In 2018, ICU physical therapy team, based on the current literature, updated their EM knowledge. Due to that process, in our institution, EM came to be defined as activities with axial loading (sitting on the edge of the bed or greater levels of out of bed mobilization) as proposed by Harrold et al. in 2015 16. After this update in the EM concept, we started to monitor the proportion of patients mobilized out of bed in the institutional indicator named as “verticalization” rate. Likewise, the proportion of patients who do not have contraindications but are not mobilized out of bed as prioritized in our EM protocol, came to be accounted by the indicator named as “non-compliance” rate. These indicators are collected monthly by a physical therapist through the patient’s medical record from the preceding 24 h, without the team’s previous knowledge in a one-day point-prevalence. The reasons not to mobilize as well, the barriers perceived by the physical therapist on duty are investigated at this moment. For any data uncertainties, the responsible physical therapist could question the health employees on duty.
The preliminary data analysis of this indicator demonstrated that our “verticalization” and the “non-compliance” rate was 36.3% and 24%, respectively. This result was considered as a nonconformity, since some level of out of bed mobilization was expected from those patients considering they had clinical conditions to be “verticalized” without any contraindications 24.
Based on the data provided from the institutional mobilization indicator and the multidisciplinary perception consolidated in a workshop, a multifaceted improvement strategy was proposed. The aim of our study was to evaluate the effectiveness of these strategies in reducing non-compliance with the institutional EM protocol in adult ICUs of a tertiary hospital.
Methods
This study was a QI project that followed the revised Standards for Quality Improvement Reporting Excellence (SQUIRE2) guidelines26 (Supplementary).
Ethics approval and consent to participate
This QI project received ethics approval from the research ethics committee of the Hospital Sírio Libanês/Sociedade Beneficiente de Senhoras (CEPesq/HSL), with a reference number: CEPesq HSL2019-84. This committee in addition to releasing the research protocol, waived the need of informed consent form since the study is a retrospective review of data from medical records and hospital electronic database. The methods were carried out in accordance with the relevant guidelines and regulation.
Project design
This single-center QI with retrospective before-after comparison study was conducted using data from medical records and hospital electronic databases in 2019 at the Sírio-Libanês Hospital, São Paulo, Brazil (Fig. 1).

Study design.
The primary study outcome was the “non- compliance” rate with the EM protocol. The mobility landmark achieved per period, a the lCU length of stay, the ICU and hospital mortality, and the ICU readmission rate were considered as secondary outcome parameters.
The data was collected based on the physiotherapy service “verticalization” rate. Consecutive patients who meet the inclusion and exclusion criteria of the study were part of the sample. Therefore, only patients aged ≥ 18 years who were included in the indicator screening, without a mobility contraindication was considered. Contraindication was defined as any hemodynamic, neurological, or respiratory instability; medical contraindications, medical indication to prioritize comfort measure, patient refusal; and patients admitted or discharged from the ICU on the day of collection.
The “before” period corresponded to the previous four months of the improvement strategy implementation in October 2018. The “after” period corresponded to the four months following the executed QI initiative. The data was obtained in a decreasing and growing way in the months until the sample size was achieved.
Setting
During the study period, the adult ICUs consisted of 49-beds. Two general ICUs (21 beds), one neurological ICU (8 beds), and two cardiologic ICUs (20 beds). The ICU staffing comprised of a physician (staff-to-patient ratio 1:5), registered nurse (staff-to-patient ratio 1:2), and physiotherapist (staff-to-patient ratio 1:5). A daily multidisciplinary round to determine the goals of care was performed in both periods, considering the ABCDE bundle. The EM goal in the before period was one of the discussion topics among the team during the rounds but without the use of a mobility tool to guide that decision.
Data collection
Data was retrospectively collected from admission to hospital discharge from medical records and hospital electronic databases. Patient baseline information including demographics, comorbidities, and severity of illness at ICU admission and readmission was obtained from Epimed Solutions®.
Using a standardized checklist (Supplementary), the same professional already in charge of the institutional indicator was responsible for the “verticalization” and “non-compliance” rate collection, in order to maintain greater reliability and validity. The “verticalization” and “non-compliance” rate were monitored for a period of four months before and after the QI initiative. The presence of ICU-AW was assessed as well with MRC in patients alert and able to follow commands, as recommended by the institutional mobilization protocol. It was defined by MRC < 48 in patients that had no plausible etiology for weakness other than critical illness27. SOMS scale was applied only to patients unable to follow commands, and the presence or absence of this form of evaluation was assessed on both groups.
Variables related to ICU-AW risk factors as mechanical ventilation > 72 h, use of sedation, analgesia, neuromuscular blockers, corticosteroids, sepsis, septic shock, and immobilism (defined as the permanence on bed for more than 50% of the day) were collected.
The project researchers, through our institutional electronic medical records, also collected variables related to the outcomes as ICU length of stay, mobilization barriers and the highest achieved mobility landmark of the day. All mobilization’s barriers perceived by the physical therapists during their care were also recorded; as presence of sedation, patient’s devices (urinary catheter, nasogastric tube, arterial or venous lines), mechanical circulatory assist device, vasoactive drugs, renal supplementation therapy, presence of pain, weakness, endotracheal intubation, tracheostomy, mechanical ventilation, non-invasive ventilation or high flow nasal cannula.
If any patient’s information was missing, the researchers or the professional in charge of the institutional indicator could access the assistance team to resolve relevant queries. The checklist and the spreadsheet used to compute the data were double-checked to avoid any data loss or incomplete data.
Improvement strategy
To elaborate the improvement strategy, initially, we performed a summary of the evidence considering out-of-bed mobilization. Posteriorly, we optioned to understand the problem from the perspective of the multidisciplinary team. We organized a brainstorming during a workshop freely listed by the participants (the results were grouped in an Ishikawa diagram) and an online multiple-choice questionnaire. Both addressing the modifiable barriers related to environment, patient, staff, and process. Finally, the team perception was paired with the data obtained from a meticulous verification of the patient’s medical records to elucidate modifiable barriers involved in the cases of patients who were moveable and those who were not28.
After analyzing the results of these activities, we verified the importance of improving communication between the characters involved, planning, and process individualization considering the specific barriers, in addition to patient and family participation. Considering these points, a visual tool was developed named as “mobility clock” (Fig. 2) to simultaneously quantify, inform, and monitor the patient's functional level. Instead of hours, it displays the different landmarks of mobility based on the ICU mobility scale29.

The mobility clock monitors the level of mobility in the intensive care units of Hospital Sírio-Libanês and is based on the ICU mobility scale. It presents ten mobility milestones (the higher the score, the higher the mobility level achieved by the patient). One of the hands of the clock represents the mobility level planned by the multidisciplinary team for the patient during the shift (goal), and the other, represents what was achieved. In the example above, the objective elaborated by the team was to “march on spot” (level 6) and the milestone achieved was to “sit on the edge of bed” (level 3). Thus, the objective was not reached because the level of mobility achieved was lower than planned.
An action plan was prepared and set in motion to inaugurate the “mobility clock” during the “mobilization week”. It consisted in various activities created for the multidisciplinary team regarding the importance of ICU mobilization. To sensitize the team about the importance of EM, the week initiated with a talk show from a patient who developed quadriplegia due to immobilization. The patient, his family members and the professionals involved shared their personal experience during the period of ICU hospitalization and the impact after hospital discharge. During that week, a lecture with updated literature data on out-of-bed ICU mobilization was ministered.
The internal audit results along with institutional modifiable barriers were presented along with the “mobility clock” through an animation specifically produced to explain its development and application. To conclude it, the “mobilization challenge” was released. It consisted in a four-week competition between the ICU units with the purpose of establishing the use of the “mobility clock” by the team. The winning unit would be the one that mobilized the largest number of eligible patients using the “mobility clock”. During this period, a podcast explaining how to use the “mobility clock” and the challenge rules was broadcasted on the institution’s channels. Banners referring to mobility were displayed at the entrance of each unit. To motivate the staff to the cause, stickers encouraging mobilization and chocolate treats were distributed 28.
The “mobility clock” was placed in the ICU rooms to be visible to the patient, family, and staff. One clock pointer marked the mobility level that was set as the goal and the other the landmark that the patient achieved. To improve communication in the multidisciplinary round, the expected goal per patient was determined considering the barriers presented, as well as the physical condition of each individual. At this time, if possible, the importance of reaching the chosen mobility landmark on the day was explained to the patient and family. The clock hand that corresponded to the landmark achieved by the patient was moved during the day as soon as the mobility level was reached.
During the before-after period, no other institutional strategy regarding EM was employed.
Statistical analysis
The sample size (at least 88 patients per period) was calculated based on a previous pilot study considering the number necessary to reduce the “non-compliance” with the protocol on 10%, given a two-tailed type 1 error of 5% and a power of 80%. Quantitative continuous variables were compared using the Mann–Whitney U test for non-normally distributed variables with interquartile values used to represent data dispersion. The means of normally distributed variables were compared using Student’s t-test. Pearson’s chi-squared test and Fisher’s exact test were used to compare the categorical variables. The significance level was set at p ≤ 0.05 (two-tailed).
Results
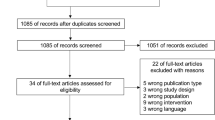
The EM protocol “verticalization” rate was monitored for a period of four months before and after the strategy to achieve the sample. In the “before” period, 179 patients were screened. Of these, 90 were excluded because they presented at least one mobility contraindication. During the “after” period, 177 patients were screened, with the exclusion of 88 patients, for the same reason as mentioned above, remaining 89 patients on this period (Fig. 3). Both groups had similar baseline characteristics (Table 1).

Study sample flowchart.
The risk factors for ICU-AW presented at indicator data were similar between the groups except for the use of corticosteroids that was significantly greater in the “after” period (29.21% vs. 14.61%, p = 0.02) (Table 2). Regarding the perceived barriers, the need of non-invasive ventilation (6.74% vs 1.12%, p = 0.12) and mechanical ventilation (11.24% vs 4.49%, p = 0.16) was greater in the “after” period; however, no statistical significance was achieved (Table 3).
The ICU-AW identified by means of an MRC < 48 was similar between the groups. The proportion of patients whose MRC was not possible to be applied, requiring SOMS to be performed, was higher in the “after” period but without statistical significance (Table 4).
After the QI, a lower “non-compliance” rate with the protocol was observed, compared to the previous period (10.11% vs. 26.97%, p < 0.004) (Fig. 4). Considering the mobility landmark, the proportion of patients walking was higher in the “after” period compared to the “before” period (49.44% vs. 29.21%, p = 0.006), as well marching on spot that was performed in 4.49% of the patients on the “after” period while it was not performed on the period before QI (p = 0.04) (Fig. 5).

Institutional protocol “non-compliance” rate.

Proportion of highest mobility landmark achieved.
No differences between the periods were observed in the hospital and lCU length of stay, as well as in the mortality rate. However, the ICU readmission rate was lower on the “after” period (2.25% vs. 11.24%, p = 0.017) (Table 5).
Discussion
The non-compliance rate reduction with the QI strategy, suggests an effectiveness in the short term to achieve our goals, in accordance with results from previous QI studies18,19,20. These, with the increase observed in highest level of mobility landmark archived in after period, may be a consequence of the QI strategies, that provided an individualized discussion per patient during the definitions of multidisciplinary goals. That practice along enhanced the adherence and performance of the multidisciplinary team in addition to improving the communication.
ICU EM is essential to prevent a loss of functional status that can perpetuate after hospital discharge, affecting the quality of life and social reintegration1,2,3,4,5,6,7. Besides considered feasible in cases of a favorable clinical condition, it is frequent that not out of bed mobilization occur due to modifiable barriers. In this way, “non-compliance” with EM protocols can be secondary to failure to identify institutional barriers as well as failure to develop strategies to overcome it12,14,24.
The “non-compliance” rate indicator was used to verify the effectiveness of our strategy as the last stage foreseen in the QI process30. Except for the proposed strategy aimed at EM, in the after period there was no difference between the units to the other items proposed in the evidence-based guide ABCDE bundle.
The mobility clock was created after understanding the problem of our institution with the barriers not only perceived by the professionals in clinical practice, but also those verified through an active search for specific cases of “non-compliance” with our protocol. After its development, strategies to sensitize and educate healthcare professionals, patients, and family members to prioritize out-of-bed mobilization were developed as well an execute strategic plan was done as recommended in literature8,18,20.
The visualization of the mobilization objective of the day, moreover, to continually demonstrating to the team the landmark to be reached on the day, may have led the patient and/or family members to perceive that out-of-bed mobilization in addition to being important, is feasible and safety in the ICU. Making them partner in the process.
It is known that the family participation throughout the rehabilitation process, as recommended most recently with the inclusion of the item “F” in the ICU bundle, can optimize patient recovery2,7. In this QI project, the purpose of the “mobility clock” was explained to the family and, although we have noticed their greater involvement in achieving higher mobility levels by their relatives, no family-related outcomes were measured.
During the monitored periods the results were similar regarding the risk factors for ICU-AW and perceived barriers.
In the post-strategy period, a decrease in readmission rate was observed. It is important to note that sample size of this study was not calculated to investigate this primary purpose. Certainly, it is an important data to be confirmed in further studies since after a long-term ICU stay (> 72 h), one year mortality was approximately 28% and was related to age, disease severity, comorbidities, and ICU re-admissions31.
A limitation of our study was the before-and-after design that carries the biases inherent to the temporal variation and the impact of confounders that were not considered, as well as the single-center QI limiting the external validity. Further research on this topic should be implemented, including multicenter prospective randomized studies focusing on the clinical and economic outcomes of mobilization QI projects.
Conclusion
The multifaceted strategy was effective to reduce “non-compliance” rate to EM protocol of a tertiary hospital. In addition, promoted a higher level of mobility landmark. In further research, it would be interesting to study the effectiveness of these strategies in different centers, with more suitable study designs involving clinical outcomes as the readmission rate. Furthermore, considering hospital and ICU length of stay, the economic impact of these mobilization-QI projects is also an important field of study and may encourage future investigations.
A QI multidisciplinary approach in a brief period can positively influence patient mobilization and team engagement without additional costs for the service and with a simple and intuitive tool.
Data availability
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
Abbreviations
- ICU:
-
Intensive care unit
- MRC:
-
Medical Research Council
- SOMS:
-
Surgical Intensive Care Unit Optimal Mobilization Score
- ICU-AW:
-
Intensive care unit acquired weakness
- BMI:
-
Body mass index
- SAPS 3:
-
Simplified Acute Physiology Score
- SOFA:
-
Sequential Organ Failure Assessment
- DM:
-
Diabetes mellitus
- SAH:
-
Systemic arterial hypertension
- CKD:
-
Chronic kidney disease
- HF:
-
Heart failure
- COPD:
-
Chronic obstructive pulmonary disease
- MV:
-
Mechanical ventilation
- NMB:
-
Neuromuscular blocker
- MCAD:
-
Mechanical circulatory assist device
- VADs:
-
Vasoactive drugs
- RST:
-
Renal supplementation therapy
- ETT:
-
Endotracheal intubation
- NIV:
-
Non-invasive ventilation
- HFNC:
-
High flow nasal cannula.
- QI:
-
Quality improvement
References
Mikkelsen, M.E., Hopkins., R.O., & Sevin, C.M. Post-intensive care syndrome (PICS) and strategies to mitigate PICS. ICU Lib. 89, 97–109 (2012).
Pun, B. T. et al. Caring for critically ill patients with the ABCDEF bundle: Results of the ICU liberation collaborative in over 15,000 adults. Crit. Care Med. 47, 3–14 (2019).
Kress, J. P. & Hall, J. B. ICU-acquired weakness and recovery from critical illness. N. Engl. J. Med. 24, 1626–1635 (2014).
Parry, S. M. & Puthucheary, Z. A. The impact of extended bed rest on the musculoskeletal system in the critical care environment. Extreme Physiol. Med. https://doi.org/10.1186/s13728-015-0036-7 (2015).
Needham, D. M. et al. Improving long-term outcomes after discharge from intensive care unit: Report from a stakeholders’ conference. Crit. Care Med. 40, 502–509 (2012).
Herridge, M. S. et al. One-year outcomes in survivors of the acute respiratory distress syndrome. N. Engl. J. Med. 348, 683–693 (2003).
Dinglas, V. D. et al. Muscle weakness and 5-year survival in acute respiratory distress syndrome survivors. Crit. Care Med. 45, 446–453 (2017).
Nedergaard, H. K., Jensen, H. I. & Toft, P. Interventions to reduce cognitive impairments following critical illness: A topical systematic review. Acta Anaesthesiol. Scand. 61, 135–148 (2017).
Marra, A., Ely, E. W., Pandharipande, P. P. & Patel, M. B. The ABCDEF bundle in critical care. Crit. Care Clin. 33, 225–243 (2017).
Berney, S. C. et al. Intensive care unit mobility practices in Australia and New Zealand: A point prevalence study. Crit. Care Resusc. 15, 260–265 (2013).
Nydahl, P. et al. Early mobilization of mechanically ventilated patients: A 1-day point-prevalence study in Germany. Crit. Care Med. 42, 1178–1186 (2014).
Dubb, R. et al. Barriers and strategies for early mobilization of patients in intensive care units. Ann. Am. Thorac. Soc. 13, 724–730 (2016).
Hodgson, C. L. et al. Expert consensus and recommendations on safety criteria for active mobilization of mechanically ventilated critically ill adults. Crit. Care. 18, 658 (2014).
Dafoe, S., Chapman, M. J., Edwards, S. & Stiller, K. Overcoming barriers to the mobilization of patients in an intensive care unit. Anaesth. Intensive Care. 43, 719–727 (2015).
Jolley, S. E., Regan-Baggs, J., Dickson, R. P. & Hough, C. L. Medical intensive care unit clinician attitudes and perceived barriers towards early mobilization of critically ill patients: A cross-sectional survey study. BMC Anesthesiol. 14, 84 (2014).
Harrold, M. E., Salisbury, L. G., Webb, S. A. & Allison, G. T. Australia and Scotland ICU Physiotherapy Collaboration. Early mobilization in intensive care units in Australia and Scotland: A prospective, observational cohort study examining mobilization practices and barriers. Crit. Care. https://doi.org/10.1186/s13054-015-1033-3 (2015).
Engel, H. J., Tatebe, S., Alonzo, P. B., Mustille, R. L. & Rivera, M. J. Physical therapist-established intensive care unit early mobilization program: Quality improvement project for critical care at the University of California San Francisco Medical Center. Phys. Ther. 93, 975–985 (2013).
van Willigen, Z. V., Collings, N., Richardson, D. & Cusack, R. Quality improvement: The delivery of true early mobilization in an intensive care unit. BMJ Qual. Improv. Rep. 5, 1–6 (2016).
Hopkins, R. O., Miller, R. R., Rodriguez, L., Spuhler, V. & Thomsen, G. E. Physical therapy on the wards after early physical activity and mobility in the intensive care unit. Phys. Ther. 92, 1518–1523 (2012).
Harris, C. L. & Shahid, S. Physical therapy-driven quality improvement to promote early mobility in the intensive care unit. Proc. (Bayl Univ. Med. Cent.). 27, 203–207 (2014).
Engel, H. J., Needham, D. M., Morris, P. E. & Gropper, M. A. ICU early mobilization: From recommendation to implementation at three medical centers. Crit. Care Med. https://doi.org/10.1097/CCM.0b013e3182a240d5 (2013).
Needham, D. M. et al. Early physical medicine and rehabilitation for patients with acute respiratory failure: A quality improvement project. Arch. Phys. Med. Rehabil. 91, 536–542 (2010).
Drolet, A. et al. Move to improve: The feasibility of using an early mobility protocol to increase ambulation in the intensive and intermediate care settings. Phys. Ther. 93, 197–207 (2013).
Moore, J. E. et al. Mapping barriers and intervention activities to behavior change theory for Mobilization of Vulnerable Elders in Ontario (MOVE ON), a multi-site implementation intervention in acute care hospitals. Implement Sci. https://doi.org/10.1186/s13012-014-0160-6 (2014).
Murakami, F. M. et al. Evolução funcional de pacientes graves submetidos a um protocolo de reabilitação precoce. Rev. Bras. Ter Intensiva. 27, 161–169 (2015).
Ogrinc, G. S. et al. SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence): Revised publication guidelines from a detailed consensus process. BMJ Qual. Saf. 25, 986–992. https://doi.org/10.1136/bmjqs-2015-004411 (2016).
Stevens, R. D. et al. A framework for diagnosing and classifying intensive care unit-acquired weakness. Crit. Care Med. https://doi.org/10.1097/CCM.0b013e3181b6ef67 (2009).
Ligeiro, A.S., Nawa, R.K., & Souza, P.N. Estratégias de enfrentamento de barreiras para a mobilização precoce na UTI. [Trabalho de conclusão de curso]. (Residência multiprofissional em cuidado ao paciente crítico, Hospital Sírio Libanês, 2018).
Kroth, J.B., & Souza, P.N. Verticalização dos pacientes nas unidades de terapia intensiva adulto do hospital sírio libanês. [Trabalho de conclusão de curso]. (Residência multiprofissional em cuidado ao paciente crítico-Hospital Sírio Libanês, 2018).
Silver, S. A. et al. How to begin a quality improvement project. Clin. J. Am. Soc. Nephrol. https://doi.org/10.2215/CJN.11491015 (2016).
Steenbergen, S. et al. Long-term treated intensive care patients’ outcomes: The one-year mortality rate quality of life, health care use and long-term complications as reported by general practitioners. BMC Anesthesiol. https://doi.org/10.1186/s12871-015-0121-x (2015).
Acknowledgements
The authors thank the ICU physical therapists for their valuable support during data collection.
Author information
Authors and Affiliations
Contributions
P.N.S. conceptualized and designed the study, developed the visual tool, analyzed the data, reviewed, and revised the manuscript and approved the final manuscript as submitted. J.B.K. conceptualized and designed the study, developed the visual tool, collected the data, reviewed, and revised the manuscript and approved the final manuscript as submitted. A.S.L. collected the data, approved the final manuscript as submitted, J.M.M.: collected the data, approved the final manuscript as submitted A.L.V.M.: revised the manuscript, developed the visual tool, and approved the final manuscript as submitted L.P.: revised the manuscript and approved the final manuscript as submitted. W.P.Y.: Provided intellectual contribution during the project elaboration, developed the visual tool, reviewed, and revised the manuscript and approved the final manuscript as submitted.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
de Souza, P.N., Kroth, J.B., dos Santos Ligero, A. et al. Effectiveness of a quality improvement strategy with implementation of a specific visual tool to promote ICU early mobilization. Sci Rep 12, 17206 (2022). https://doi.org/10.1038/s41598-022-21227-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-21227-y
- Springer Nature Limited