
Abstract
Background
We aimed to assess whether the levels of FFAs (free fatty acids) in ACS (acute coronary syndrome) patients depend on the extent of myocardial ischemia during the subacute phase of ACS attack.
Methods
A total of 892 consecutive CAD (coronary artery disease) subjects undergoing coronary angiography were enrolled. The FFAs contents were measured based on enzymatic assay. The relationship between FFAs and Gensini score and ACS susceptibility was assessed.
Results
In the overall population, the upper FFAs quartile was accompanied with higher ischemia parameters and increased occurrence of ACS and STEMI (ST-segment elevation myocardial infarction) (P < 0.05). The FFAs concentrations were approximately 1.5-fold higher in ACS than in stable CAD patients, roughly 1.3-fold higher in STEMI than non-STEMI ACS patients and probably 1.3-fold higher in non-STEMI ACS than in stable CAD patients. After adjusted for traditional cardiovascular risk factors, the FFAs level remained a risk factor for a higher Gensini score with more than 40 (P < 0.001) and prevalent ACS (P < 0.001). After adjusted for traditional risk factors, FFAs levels after natural logarithm transformation were associated with hs-CRP and WBC counts in ACS patients. A multiplicative interaction was found between hs-CRP, WBC counts and FFAs in incident ACS and higher Gensini score (P < 0.001).
Conclusions
Higher in-hospital levels of FFAs persist and may reflect the severity of ischemia and necrosis during the subacute phase of ACS attack.
Similar content being viewed by others

Background
Plasma free fatty acids (FFAs) levels are elevated within 12 h after the onset of acute myocardial infarction (AMI) [1], moreover, elevated FFAs are associated with worse outcomes including increased risk of arrhythmia [2], sudden cardiac death and total mortality [3]. Although most FFAs are bound to albumin, a small fraction is unbound FFA (FFAu); FFAu increases in the ischemic, under-perfused myocardium rapidly within 30 min, which is considered to be more sensitive in physiologic changes than bound FFAs.
Inflammation plays a critical role throughout the atherosclerotic stage in various vessels, ranging from fatty streak formation to cardiovascular events [4, 5]. Among the potential inflammation biomarkers, C-reactive protein, the classical acute-phase protein, functions as a highly sensitive systemic marker of inflammation and tissue damage and can be measured by high-sensitivity assay (hs-CRP). Numerous epidemiological studies have demonstrated that hs-CRP had a clear prognostic value for predicting major cardiovascular events and mortality [6, 7].
Increased FFAu is an early predictor of ischemia in ACS (acute coronary syndrome) [8]. Our previous study found that plasma FFA compositions were dysregulated in CAD (coronary artery disease) patients, partly influenced by age and gene polymorphisms [9, 10]. Therefore the objective of our study was to explore the association between total FFAs and the severity of myocardial ischemia of ACS during subacute phase, and further investigated whether this was influenced by hs-CRP.
Methods
Subjects
The study was approved by the medical ethical committee of Zhongnan Hospital of Wuhan University. All participants were Han population from China, who gave their informed, written consent. From 2012 to 2014, we consecutively recruited patients who underwent selective coronary angiography for suspected coronary atherosclerosis and who were admitted within 24 h from chest pain at cardiovascular department. The diagnosis of CAD was defined as the presence of coronary lesions ≥50 % in at least one major artery segment assessed by two independent cardiologists who had no information of the patients’ clinical characteristics and biochemical results. We excluded all patients with additional complications including viral hepatitis, tumor, autoimmune disease, serious liver or renal dysfunction, myocardiopathy or valvular heart disease and patients received with heparin treatment.
Serial blood samples were taken after admission for routine laboratory parameter tests, including liver function, kidney function, lipids and lipoproteins and myocardial enzymes. Estimated glomerular filtration rate (eGFR) was calculated using the Modification of Diet in Renal Disease (MDRD) study equation: eGFR = 186 × ((serumcreatinine)^(‐ 1.154)) × ((age)^(‐0.203)) × [0.742 if female]. AMI was defined by typical clinical symptoms, electrocardiograph changes and positive serum biomarkers [11, 12]. Unstable angina (UA) was established based on the criteria of Brawmwald using clinical symptoms, non-ST segment elevation and negative serum biomarkers [13].
Assay of FFAs content
Serum samples were collected, separated and stored at −80 °C within 24 h of admission. Samples were incubated for 15 min at room temperature and then a single determination of FFAs content was tested by enzymatic assay (Clinimate NEFA, Tokyo, Japan).
Angiographic analysis
Catheterization and multiple views were imaged and maximal stenosis in each coronary artery segment was evaluated by a cardiologist according to the segmental classification system of the Coronary Artery Surgery Study. The extent of angiographically documented CAD was quantified in the left anterior descending artery, the left circumflex artery, and the right coronary artery, the criteria were as follows: normal coronary arteries (smooth, with either no stenosis or stenosis of <10 % of the luminal diameter), mild coronary arteries (stenosis of 10 % to 50 % of the luminal diameter in ≥ 1 coronary artery), or 1, 2 or 3-vessel disease, defined as stenosis of more than 50 % of the luminal diameter.
Gensini score
To assess coronary artery disease burden based on coronary angiogram, the Gensini score was calculated according to Gensini scoring system [14]. The Gensini score equaled the sum of all segment scores (where each segment score equaled the segment weighting factor multiplied by the severity score). Severity scores assigned to the specific percentages of luminal diameter reduction of the coronary artery segment were 32 for 100 %, 16 for 99 %, 8 for 90 %, 4 for 75 %, 2 for 50 %, and 1 for 5 %.
Statistical analysis
Variables were expressed as the mean ± SD, median (25th–75th percentile) or proportions and compared using Mann–Whitney U-test, Kruskal-Wallis H-test or the χ2 test in univariable analysis. Binary logistic regression analysis was used to identify correlated risk factors. All analyses were performed using PASW Statistics, version 13.0 (SPSS, Chicago, IL, USA).
Results
Clinical characteristic
The study population consisted of 404 SCAD (stable coronary artery disease) patients, including 294 chronic stable angina patients (male 56.1 %, aged 68 ± 11),110 old myocardial infarction patients (male 76.4 %, aged 66 ± 12) and 488 ACS patients, including 108 UA patients (male 56.6 %, aged 68 ± 11), 191 NSTEMI (non-ST segment elevation myocardial infarction) patients (male 76.2 %, aged 67 ± 13) and 189 STEMI (ST segment elevation myocardial infarction) patients (male 82.4 %, aged 62 ± 13).
The baseline demographic, clinical characteristics and laboratory parameters according to the quartiles of the FFAs levels (Q1 0.12–0.37, n = 223; Q2 0.38–0.54, n = 218; Q3 0.55–0.78, n = 228; Q4 0.79–4.57, n = 223) for the study population were summarized in Table 1. The distribution of FFAs quartiles were slightly unbalanced with traditional cardiovascular risk factors such as age, smoking, fasting blood glucose, hs-CRP and the atherogenic lipid parameters including TC, LDL-C, TG (P < 0.05). In addition, the necrosis and ischemia parameters dramatically increased according to FFAs quartiles such as cTnT, CK-MB, maximal stenosis and Gensini score (P < 0.05).
Association of FFAs with severity of ischemia and necrosis
The FFAs levels in ACS patients were higher than in SCAD patients ((0.68 mmol/l (0.45, 0.911) vs. 0.44 mmol/l (0.3, 0.63), P < 0.001, respectively)) (Fig. 1a), which remained a significant correlation after adjustment for age and gender (P < 0.001). Among patients with ACS, the higher FFAs levels remained significant between STEMI and UA + NSTEMI patients ((0.77 mmol/l (0.55, 1.1) vs. 0.58 mmol/l (0.4, 0.83), P < 0.001, respectively)) (Fig. 1b), which was significant after adjustment for age and gender (P < 0.001). Meanwhile, the FFAs levels in UA + NSTEMI patients were higher than in SCAD patients ((0.58 mmol/l (0.4, 0.83) vs. 0.44 mmol/l (0.3, 0.63), P < 0.001, respectively)) (Fig. 1c), and the difference still remained significant after adjustment for age and gender (P < 0.001), suggesting that FFAs content increased closely with the severity of coronary artery lesions in CAD.

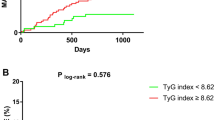
Distributions of FFAs among CAD patients (a, b, c) and prevalence of ACS, STEMI and Gensini score more than 40 based on the FFAs quartiles (d, e, f). Asterisks (*) represent a P-value <0.05. Q = quartile.
Meanwhile, the occurrence of ACS and STEMI increased according to the FFAs quartiles (P value for trend = 0.003, 0.001) (Fig. 1d, e). To explore the relationship of FFAs and the prevalent ACS and STEMI, a binary logistic regression analysis was performed. After adjusted for traditional cardiovascular risk factors including age, SBP, DBP, smoking, history of hypertension, diabetes mellitus and hyperlipidemia, the FFAs levels remained positively associated with prevalent ACS and STEMI ((for the occurrence of ACS, OR(95 % CI) = 9.956(5.21, 19.023), P < 0.001; for the occurrence of STEMI, OR(95 % CI) = 8.428(4.619, 15.376), P < 0.001)) (Tables 2 and 3).
To further explore whether the FFAs levels could reflect the severity of ischemia and necrosis focus in ACS patients, we performed Spearman’s correlation analysis. It showed that FFA level was positively correlated with Gensini score and maximal stenosis (r = 0.224, P < 0.001 and r = 0.224, P < 0.001) and remained significant after adjustment for age and gender (P = 0.001 and P = 0.003). The occurrence of a higher Gensini score with more than 40 increased according to the FFAs quartiles (P value for trend < 0.001) (Fig. 1f), after adjusted for traditional cardiovascular risk factors including age, SBP, DBP, smoking, history of hypertension, diabetes mellitus and hyperlipidemia, the FFAs levels remained a risk factor for a higher Gensini score with more than 40 ((OR(95 % CI) = 3.741 (1.826, 7.664), P < 0.001)) (Table 4). Correlations of FFAs content with the infarct size in ACS patients, estimated by CK-MB and cTnT were performed, showing that FFA levels had positively weak correlations with infarct size (r = 0.09, P < 0.001 and r = 0.022, P < 0.001).
Interaction between WBC, hs-CRP and FFAs
We constructed the multivariate linear regression analysis to elucidate the association of FFAs with inflammation parameters, after adjusting for traditional cardiovascular risk factors including age, SBP, DBP, smoking, history of hypertension, diabetes mellitus and hyperlipidemia, which showed after natural logarithm transformation that FFAs were associated with hs-CRP (β = 0.003, p = 0.048) and WBC (β = 0.042, p = 0.008), respectively.
The whole study population were divided into four groups according to the FFAs quartiles and each group was sectionalized into 2 subgroups according to their high/low levels of WBC (≤10×109, >10×109) or hs-CRP (≤3.0 mg/l, >3.0 mg/l) respectively [15]. As shown in Fig. 2a, among all FFAs quartile groups, patients with hs-CRP more than 3.0 mg/l were more susceptible to ACS, compared to patients with hs-CRP less than 3.0 mg/l (P <0.05); the trend for ACS occurrence in both high and low hs-CRP groups was significantly elevated with the distribution of higher FFA level (P value for trend < 0.05) (Additional file 1: Figure S1A). The occurrence of STEMI was elevated with higher hs-CRP, except in the lowest FFAs quartile Q1 group (P < 0.05) (Fig. 2b); a similar trend was observed in STEMI susceptibility and FFAs level in both high and low hs-CRP groups (P value for trend < 0.05) (Additional file 1: Figure S1B). Meanwhile, higher hs-CRP level was associated with a higher Gensini score in the FFAs quartile Q2 group (P < 0.05) (Fig. 2c); the percentage of Gensini score for more than 40 dramatically increased according to FFAs quartiles in both high and lowe hs-CRP groups (P value for trend <0.001) (Additional file 1: Figure S1C). The similar trendsexist in WBC counts and ACS susceptibility (Fig. 2d, Additional file 1: Figure S1D), WBC counts and STEMI susceptibility (Fig. 2e, Additional file 1: Figure S1E), WBC counts and higher Gensini score (Fig. 2f, Additional file 1: Figure S1 F), respectively.

Interaction between WBC counts, hs-CRP and FFAs levels in ACS (a, d, g), STEMI (b, e, h), Gensini Score (c, f, i). Asterisks (*) showed significant difference in high/low hs-CRP and WBC levels by χ2 analysis. Pound key(#) represented significant difference in the comparison of interaction to non-interaction between FFAs and hs-CRP. Joint mark (&) showed significant difference in the comparison of interaction to non-interaction between FFAs and WBC counts. Q = quartile.
The trend of ACS occurrence, STEMI attack and higher Gensini score with higher FFAs in high hs-CRP and WBC levels versus low hs-CRP and WBC levels were suggestive of an interaction between hs-CRP, WBC counts and FFAs in relation to the progress of myocardial ischemia. After performed by logistic regression analysis, we found a multiplicative interaction between hs-CRP, WBC and FFAs in ACS and STEMI susceptibility and a higher Gensini score ((in relation to ACS susceptibility, FFAs*hs-CRP, OR(95 % CI) = 1.029(1.016, 1.043), P < 0.001, FFAs*WBC, OR(95 % CI) = 1.357(1.281, 1.438), P < 0.001; in relation to STEMI susceptibility, FFAs*hs-CRP, OR(95 % CI) = 1.016(1.008, 1.024), FFAs*WBC, OR(95 % CI) = 1.246(1.194, 1.3), P < 0.001; in relation to a higher Gensini score, FFAs*hs-CRP, OR(95 % CI) = 1.033(1.013, 1.054), P = 0.001, FFAs*WBC, OR(95 % CI) = 1.065(1.02, 1.112), P = 0.004)) (Fig. 2g, h, i), which suggests that FFAs influence the progress of ischemia involved by inflammation processes.
Discussion
The major findings of our study confirmed that FFAs level might serve as a predictor of the severity of myocardial ischemia during the subacute onset of ACS attack. First and foremost, FFAs levels were higher in the ACS patients than the SCAD population, especially in STEMI patients. Second, the FFAs increased with the severity of necrosis and ischemia, such as cTnT and Gensini score. Moreover, we observed an association between WBC counts, hs-CRP and FFAs levels in incident ACS and higher Gensini score, which implied a possible interaction between FFAs and inflammation processes influenced the severity of ischemia.
According to the previous studies, elevated FFAs levels in AMI are associated with increased lipolytic activity, owing to an immediate increase of catecholamine with the activated sympathetic nervous system [16]. Although increasing evidence has shown that an elevation of FFAs level occurs after the onset of AMI and that higher FFAs are associated with a greater incidence of major cardiovascular events [17], no study has resolved the principal mystery whether FFAs directly trigger serious cardiovascular disease or only predict cardiometabolic dysfunction [18]. There are several mechanisms illustrating high FFAs concentration may be toxic in acute ischemic myocardium, such as mitochondrial uncoupling, activation of lipids in mitochondria, inhibition of β-oxidation, inhibition of the Na+-K+-ATPase pump leading to high intracellular sodium and calcium, or reduction of GLU-4 causing reduced insulin-stimulated glucose transport [19]. Therefore, it is a top priority to monitor and reduce concentrations of FFAs in the post phase of ACS [20].
Moreover, we found hs-CRP, WBC and FFAs had a multiple effect in relation to ACS susceptibility and severe myocardial ischemia (Fig. 2), which implied a possible mechanism relating FFAs together with inflammatory factors influenced the progress of ischemia. Inflammatory cytokines such as IL-6 and TNF-α were added to isolated adipocytes, resulting in increased lipolysis and FFAs levels in several in-vivo and in-vitro studies [21, 22], also, elevated circulating FFA levels led to endothelial dysfunction in-vivo via activation of PKC-mediated inflammatory pathways and excess generation of oxidants [23, 24], which would partially explain the clinically demonstrated proarrhythmogenic potential of FFAs. Further investigations in the underlying mechanisms for the joint effect of elevated FFA and inflammatory factors on myocardial ischemia are apparently warranted.
Interestingly, preexisting hypertension had been diagnosed in SCAD, ACS and STEMI patients with the prevalence of 70.5 %, 60.2 % and 48.1 %, respectively and that decreased ratio of hypertension was associated with higher occurrence of ACS and STEMI (Additional file 2). The role of hypertension history in the prevalence of ACS was difficult to explain. A large observational study showed that patients with preexisting hypertension had a more favorable in-hospital outcome [25]. Despite with a higher risk, hypertensive patients was paradoxically associated with a more favorable in-hospital diagnosis. Underlied the mystery, awareness and treatment of hypertension with potentially cardio-protective antihypertensive drugs might function as a ‘protective’ effect [25].
Conclusions
FFAs levels may be indicative of the severity of myocardial ischemia at subacute ACS onset and the combined effect of FFAs and activated inflammation might play a role in myocardial ischemia of ACS.
Abbreviations
- ACS:
-
acute coronary syndrome
- AMI:
-
acute myocardial infarction
- CAD:
-
coronary artery disease
- DBP:
-
diastolic blood pressure
- FBG:
-
fasting blood glucose
- FFAs:
-
free fatty acids
- FFAu:
-
unbound FFA
- HDL-C:
-
high density lipoprotein cholesterol
- HR:
-
heart rate
- hs-CRP:
-
high-sensitivity C-reactive protein
- LDL-C:
-
low density lipoprotein cholesterol
- Lp(a):
-
lipoprotein(a)
- Q:
-
quartile
- SBP:
-
systolic blood pressure
- SCAD:
-
stable coronary artery disease
- STEMI:
-
ST-segment elevation myocardial infarction
- TC:
-
total cholesterol
- TG:
-
triglyceride
- UA:
-
unstable angina
- WBC:
-
white blood cell
References
Kurien VA, Oliver MF. Serum-free-fatty-acids after acute myocardial infarction and cerebralvascular occlusion. Lancet. 1966;2:122–7.
Tansey MJ, Opie LH. Relation between plasma free fatty acids and arrhythmias within the first twelve hours of acute myocardial infarction. Lancet. 1983;2:419–22.
Oliver MF, Kurien VA, Greenwood TW. Relation between serum-free-fatty acids and arrhythmias and death after acute myocardial infarction. Lancet. 1968;1:710–4.
Ross R. Atherosclerosis--an inflammatory disease. N Engl J Med. 1999;340:115–26.
Matsuura E, Atzeni F, Sarzi-Puttini P, Turiel M, Lopez LR, Nurmohamed MT. Is atherosclerosis an autoimmune disease? BMC Med. 2014;12:47.
Koenig W. High-sensitivity C-reactive protein and atherosclerotic disease: from improved risk prediction to risk-guided therapy. Int J Cardiol. 2013;168:5126–34.
Ridker PM. Inflammation, C-reactive protein, and cardiovascular disease: moving past the marker versus mediator debate. Circ Res. 2014;114:594–5.
Bhardwaj A, Truong QA, Peacock WF, Yeo KT, Storrow A, Thomas S, et al. A multicenter comparison of established and emerging cardiac biomarkers for the diagnostic evaluation of chest pain in the emergency department. Am Heart J. 2011;162:276–82.
Li SW, Lin K, Ma P, Zhang ZL, Zhou YD, Lu SY, et al. FADS Gene Polymorphisms Confer the Risk of Coronary Artery Disease in a Chinese Han Population through the Altered Desaturase Activities: Based on High-Resolution Melting Analysis. PLoS ONE. 2013;8:e55869.
Shen F, Qi J, Xu F, Ning L, Pang R, Zhou X, et al. Age-related distributions of nine fasting plasma free fatty acids in a population of Chinese adults. Clin Chim Acta. 2013;415:81–7.
O’Gara PT, Kushner FG, Ascheim DD, Casey DJ, Chung MK, de Lemos JA, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the American College of Emergency Physicians and Society for Cardiovascular Angiography and Interventions. 2013;82:E1-27.
Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, et al. Third universal definition of myocardial infarction. J Am Coll Cardiol. 2012;60:1581–98.
Braunwald E. Unstable angina and non-ST elevation myocardial infarction. Am J RespirCrit Care Med. 2012;185:924–32.
Gensini GG. A more meaningful scoring system for determining the severity of coronary heart disease. Am J Cardiol. 1983;51:606.
Ridker PM, Buring JE, Cook NR, Rifai N. C-reactive protein, the metabolic syndrome, and risk of incident cardiovascular events: an 8-year follow-up of 14719 initially healthy American women. Circulation. 2003;107:391–7.
Oliver MF. Sudden cardiac death: the lost fatty acid hypothesis. QJM. 2006;99:701–9.
Khawaja O, Bartz TM, Ix JH, Heckbert SR, Kizer JR, Zieman SJ, et al. Plasma free fatty acids and risk of atrial fibrillation (from the Cardiovascular Health Study). Am J Cardiol. 2012;110:212–6.
Mozaffarian D. Free fatty acids, cardiovascular mortality, and cardiometabolic stress. Eur Heart J. 2007;28:2699–700.
Pilz S, Marz W. Free fatty acids as a cardiovascular risk factor. ClinChem Lab Med. 2008;46:429–34.
Oliver MF. Control of free fatty acids during acute myocardial ischaemia. Heart. 2010;96:1883–4.
Mattacks CA, Pond CM. Interactions of noradrenalin and tumour necrosis factor alpha, interleukin 4 and interleukin 6 in the control of lipolysis from adipocytes around lymph nodes. Cytokine. 1999;11:334–46.
Van Hall G, Steensberg A, Sacchetti M, Fischer C, Keller C, Schjerling P, et al. Interleukin-6 stimulates lipolysis and fat oxidation in humans. J Clin Endocrinol Metab. 2003;88:3005–10.
Li H, Li H, Bao Y, Zhang X, Yu Y. Free fatty acids induce endothelial dysfunction and activate protein kinase C and nuclear factor-κB pathway in rat aorta. Int J Cardiol. 2011;152:218–24.
Tang Y, Li G. Chronic exposure to high fatty acids impedes receptor agonist-induced nitric oxide production and increments of cytosolic Ca2+ levels in endothelial cells. J Mol Endocrinol. 2011;47:315–26.
Erne P, Radovanovic D, Schoenenberger AW, Bertel O, Kaeslin T, Essig M, et al. Impact of hypertension on the outcome of patients admitted with acute coronary syndrome. J Hypertens. 2015;33:860–7.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (81271919, 27 81472023), the National Basic Research Program of China (973 Program) (2012CB720600, 2012CB720605) and the Special Health Standards Infrastructure Program (20120904). We thank Professor Chunhong Wang of School of Public Health, Wuhan University for assistance of statistical analysis and PhD Baozhu Wei of cardiovascular department, Zhongnan Hospital of Wuhan University for collection and interpretation of clinical data. We would like to acknowledge the reviewers for their helpful comments on this paper.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
PM carried out collection of samples and data, analysis and interpretation of data, and drafting of the manuscript. LH and Z-H L participated in collection of samples and data. WC and H-HN helped in technical and material support. J-C T made critical discussion, carried out critical revision of the manuscript and obtained funding. S-M L participated in critical discussion, critical revision of the manuscript for important intellectual content. XZ: conceived of study design and participated in critical revision of the manuscript. All authors read and approved the final manuscript.
Additional files
Additional file 1: Figure S1.
The occurrence of ACS, STEMI and percentage of Gensini score more than 40 according to high/low WBC and hs-CRP levels. Asterisks (*) showed significant difference among the FFAs quartiles by χ2 analysis. Q=quartile. (TIF 97015 kb)
Additional file 2: Table S1.
The results of χ2 analysis for occurrence of hypertension in study population (DOCX 13 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Ma, P., Han, L., Lv, Z. et al. In-hospital free fatty acids levels predict the severity of myocardial ischemia of acute coronary syndrome. BMC Cardiovasc Disord 16, 29 (2016). https://doi.org/10.1186/s12872-016-0199-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-016-0199-1