
Abstract
Background and objective
The effectiveness of immunosuppressive and corticosteroid treatments for Immunoglobulin A (IgA) nephropathy (IgAN) remains thoroughly evaluated. We undertook a meta-analysis to investigate the efficacy and safety of low-dose corticosteroids plus leflunomide for progressive IgA nephropathy.
Methods
Eligible studies were obtained from PubMed, Embase, and Cochrane Library databases. We also searched the references of the included studies. Our protocol followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) checklist. Eligibility criteria were defined using a PICOS framework.
Results
Our study included three articles presenting 342 patient cases. Findings revealed that low-dose corticosteroids combined with the leflunomide group were effective in relieving urine protein excretion (UPE) [mean difference (MD) = -0.35, 95% confidence interval (CI): -0.41 to -0.30, P < 0.00001] compared with the full-dose corticosteroids group. Regarding serum creatinine (SCr), estimated glomerular filtration rate (eGFR), complete remission rate, and overall response rate, there was no difference between the groups (p > 0.05). Regarding safety, low-dose corticosteroids combined with leflunomide significantly reduced the risk of serious adverse events [odds ratio (OR): 0.11, 95% CI: 0.01 to 0.91, P = 0.04]. Besides, no significant differences were observed between the two groups in the incidence of respiratory infection, abnormal liver function, diarrhea, herpes zoster, alopecia, pruritus, insomnia, pneumonia, diabetes, and urinary tract infection (P > 0.05).
Conclusions
Low-dose corticosteroids combined with leflunomide are a safe and effective treatment for progressive IgA nephropathy.
Trial registration
The PROSPERO registration number is CRD42022361883.
Similar content being viewed by others


Introduction
Immunoglobulin A (IgA) nephropathy (IgAN) is a glomerular disease characterised by IgA or IgA-dominated immune complexes deposited in the glomerular mesangium [1]. Since Berger and Hinglais described it in 1968 [2], IgAN has become the most common primary glomerulonephritis [3]. The incidence of IgAN varies markedly in different regions, with the highest incidence in Asian countries [4, 5]. Although IgAN is considered a benign disease, studies have shown that approximately 30-45% of IgAN patients progress to end-stage renal disease (ESRD) within 20 years of onset with the need for renal replacement therapy [6, 7]. The current treatment for IgAN remains in the exploratory stage of development. Angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) were recommended as first-line treatment for IgAN according to Kidney Disease Improving Global Outcomes (KDIGO) guidelines. In contrast, high-dose systemic corticosteroid therapy for six months is recommended for patients with proteinuria > 1 g/day and eGFR > 50 mL/min/1.73 m2 [8]. However, patients usually suffer many side effects from applying long-term and high-dose corticosteroids [9]. Therefore, control of corticosteroid dose is essential for the treatment of IgAN.
In recent years, immunosuppressants have gained attention as an adjuvant treatment option for IgAN [10, 11]. Leflunomide is a synthetic isoxazole derivative immunosuppressant that suppresses lymphocyte and B-cell proliferation by inhibiting pyrimidine biosynthesis [12, 13]. The effectiveness of leflunomide in treating rheumatoid arthritis, kidney disease, and organ transplant rejection has now been established [14]. Previous studies reported that leflunomide could significantly improve proteinuria and renal function deterioration in IgAN patients [15, 16]. However, few meta-analyses have been performed on the feasibility of leflunomide combined with corticosteroids for treating IgAN.
Therefore, we performed a meta-analysis to evaluate the efficacy and safety of low-dose corticosteroids combined with leflunomide for progressive IgAN. As far as we know, this meta-analysis reported the treatment effects of this combination for the first time.
Methods
Protocol
This meta-analysis has been registered on PROSPERO with registration number CRD42022361883. As the research method, our study adopted preferred reporting items for systematic reviews and meta-analyses (PRISMA) checklist [17].
Search strategy
The article search used the PubMed, Embase, and Cochrane Library databases with the keywords “IgA nephropathy”, “leflunomide”, and “corticosteroids”. Our search strategy is based on PICOS (populations, interventions, comparators, outcomes, and study designs), as detailed in Table 1. We only considered published research (until Sept 2022). The entire search process was completed independently by three authors.
Inclusion criteria and trial selection
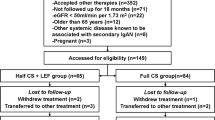
To be qualified for inclusion in our meta-analysis, included studies were required to meet the following criteria: (I) the study examined the effect of low-dose corticosteroids combined with leflunomide on IgAN; (II) the study contained sufficient valuable data, including the number of patients enrolled and the results of each observed indicator; (III) full text is available; (IV) the type of study was a clinical trial. We analysed the most recent study of identical reports published in a different journal. The process of inclusion and exclusion is outlined in Fig. 1, a PRISMA flowchart. The PRISMA 2020 checklist is supplied in the Supplemental material “PRISMA Checklist.”

PRISMA of the study selection process
Quality assessment
The randomized controlled trials (RCTs) were assessed according to guidelines published in the Cochrane Handbook for Systematic Reviews of Interventions v.5.1.0 [18]. For the retrospective cohort study, the methodological index for nonrandomised studies (MINORS) score was used for evaluation [19]. Three independent investigators conducted a quality assessment of the included studies, and disagreements were resolved by discussion. Each study was graded for quality as (+) low risk of bias, (?) unclear risk of bias, and (-) high risk of bias. Quality assessment of non-randomized controlled trials was undertaken by MINORS score. The quality of evidence was classified as 0–12 for low quality, 13–18 for moderate quality, and 19–24 for high quality.
Data extraction
The following information extracted from each included study was: (I) the first author’s name; (II) the study type; (III) the sample size (IV) the administration strategy; (V) the timing and dosage of medication; (VI) the other medications; (VII) the evaluation indicators, including urine protein excretion, serum creatinine, eGFR, serious adverse events, respiratory infection, abnormal liver function, diarrhea, herpes zoster, alopecia, pruritus, insomnia, pneumonia, diabetes, and urinary tract infection.
Statistical and meta-analysis
All analyses used the statistical software Review Manager (RevMan, version 5.3.0, Cochrane Collaboration) [20]. For continuous data, we employed the mean difference (MD) with their corresponding 95% confidence intervals (95% CIs) for evaluation. Dichotomous data were evaluated by odds ratio (OR) with 95% CIs [21]. If the P value was more significant than 0.05, the meta-analysis estimate was pooled using a fixed-effects model with between-study heterogeneity quantified using the I2 statistic. A random effects model was used otherwise.
Results
Study selection and characteristics of the trials
According to the inclusion criteria, we obtained 50 articles from the databases and registers. 4 articles were considered duplicates and excluded. After browsing through the titles and abstracts, 28 articles were eliminated. 9 articles were excluded because of a lack of valuable data. In addition, two articles were excluded because the full text was unavailable. Ultimately, three studies were included in our meta-analysis [22,23,24], with two RCTs [22, 23]. Table 2 summarises the patient characteristics of the three studies.
Risk of bias in the studies
Two included studies were RCTs, and one was a retrospective cohort study. Both RCTs were randomised, controlled, prospective, open-label, controlled trials. Each RCT study described the randomisation process in detail, while the concealment procedures were not sufficiently described. Based on the MINORS, the included retrospective cohort study scores were 19 and considered high-quality. The results regarding the quality assessment are presented in Table 3.
Efficacy
We determined the effectiveness of low-dose corticosteroids combined with leflunomide by comparing the impact of low-dose corticosteroids combined with leflunomide (Low CS + LEF) versus full-dose corticosteroids (Full CS) therapy in patients with IgAN. Complete remission refers to 24-h urine protein excretion < 0.4 g/d with a stable serum creatinine level (No more than 30% of baseline level).
Urine protein excretion (UPE)
We found two RCTs encompassing 193 patients, including 12-month follow-up data (99 in the Low CS + LEF group, 94 in the Full CS group) that evaluated the UPE. The pooled data displayed an MD of − 0.35 and a 95% CI of − 0.41 to -0.30 (P < 0.00001) from a fixed-effects model (Fig. 2A). Results demonstrated that the UPE was significantly decreased in the Low CS + LEF group compared with the Full CS group.

Forest plots showing changes in: A Urine protein excretion (UPE); B Serum creatinine (SCr); C Estimated glomerular filtration rate (eGFR); D Complete remission; E Overall response
Serum creatinine (SCr)
Two RCTs (193 patients; 99 in the Low CS + LEF group, 94 in the Full CS group) included data after 12 months of follow-up on the SCr. Fixed-effects models revealed no differences in Scr levels observed between the two groups (MD = − 5.62, 95% CI: −17.61 to 6.38, P = 0.36) (Fig. 2B).
Estimated glomerular filtration rate (eGFR)
A total of two RCTs recorded the eGFR in 193 patients. We conducted a fixed-effects model for the analysis (Fig. 2C). The heterogeneity test showed P = 0.56 and I2 = 0%. The 12-month follow-up information of the included patients. The findings demonstrated that the eGFR did not differ significantly between the Low CS + LEF and Full CS groups (MD = 0.60, 95% CI: −6.18 to 7.37, P = 0.86).
Complete remission
The forest plot yielded an OR of 1.06 with a 95% CI of 0.63 to 1.79 (P = 0.83), which suggested that the Low CS + LEF group and Full CS group were similar regarding complete remission (Fig. 2D). The 18-month follow-up information of the included patients.
Overall response
The forest plot yielded an OR of 1.55 with a 95% CI of 0.87 to 2.77 (P = 0.14), which concluded that there was no difference between the two groups in overall response (Fig. 2E). The 18-month follow-up information of the included patients.
Safety
Serious adverse events
Two studies, including 342 patients with at least 12 months of follow-up (164 in the Low CS + LEF group and 178 in the Full CS group), reported severe adverse events. The results from a fixed-effects model demonstrated that the Low CS + LEF group had an advantage in improving the incidence of serious adverse events (OR = 0.11, 95% CI: 0.01 to 0.91, P = 0.0.04) (Fig. 3A).

Forest plots showing changes in: A Serious adverse events; B Respiratory infection; C Abnormal liver function; D Diarrhea; E, Herpes zoster; F Alopecia; G Urinary tract infection
Respiratory infection
Three studies analysed the incidence of respiratory infection in 342 patients. The 18-month follow-up information of the included patients. We conducted a fixed-effects model for the analysis (Fig. 3B). The heterogeneity test showed P = 0.43 and I2 = 0%. The findings demonstrated no significant difference between the two groups in respiratory infection (OR = 0.57, 95% CI: 0.29 to 1.11, P = 0.10) (Fig. 3B).
Abnormal liver function
Three studies (342 patients; 164 in the Low CS + LEF group, 178 in the Full CS group) recorded the risk of abnormal liver function. The 18-month follow-up information of the included patients. Fixed-effects models revealed no differences in liver function were observed between the two groups (OR = 1.20, 95% CI: 0.53 to 2.70, P = 0.67) (Fig. 3C).
Diarrhea
Three studies, including 342 patients, examined the risk of diarrhea. The 18-month follow-up information of the included patients. A fixed-effects model was utilised to analyse the data. Based on the analysis results, we found no significant differences between the Low CS + LEF group and the Full CS group for diarrhea (OR = 1.11, 95% CI: 0.31–4.01, P = 0.87, Fig. 3D).
Herpes zoster
Three studies, including 342 patients with at least 12 months of follow-up data, reported the incidence of herpes zoster. We conducted a fixed-effects model for the analysis (Fig. 3E). Based on the analysis results, we suggested no significant difference between the two groups in herpes zoster (OR = 0.35, 95% CI: 0.07–1.71, P = 0.19).
Alopecia
Three studies analysed alopecia in 342 patients with at least 12 months of follow-up data. We conducted a fixed-effects model for the analysis (Fig. 3F). The findings demonstrated no significant difference between the two groups in alopecia (OR = 4.07, 95% CI: 0.67 to 24.84, P = 0.13) (Fig. 3F).
Urinary tract infection
The forest plot identified an OR of 0.80 with a 95% CI of 0.16 to 4.03 (P = 0.78), which suggested that the Low CS + LEF group and Full CS group were similar regarding urinary tract infection (Fig. 3G). The 18-month follow-up information of the included patients.
Pruritus and insomnia
Two RCTs involving 193 patients with at least 12 months of follow-up data (99 in the Low CS + LEF group, 94 in the Full CS group) had data on pruritus and insomnia. The pooled results from the fixed-effects model indicated that the Low CS + LEF group and Full CS group were similar in terms of pruritus (OR = 3.91, 95% CI: 0.42 to 35.98, P = 0.23) and insomnia (OR = 0.24, 95% CI: 0.03 to 2.19, P = 0.21) (Supplementary Figures 1 and 2).
Pneumonia and diabetes
Two studies, including 234 patients (105 in the Low CS + LEF group and 129 in the Full CS group), contained data on pneumonia and diabetes. The 12-month follow-up information of the included patients. With a fixed effects model, the OR for pneumonia was 0.46 (95% CI, 0.10–2.03, P = 0.30), and the OR for diabetes was 0.40 (95% CI, 0.09–1.73, P = 0.22). Based on the above results, we found no significant differences in pneumonia and diabetes between the two groups (Supplementary Figures 3 and 4).
Discussion
At present, the aetiology and pathogenesis of IgAN remain controversial. Because mechanisms leading to disease are likely multifactorial, no standard treatment for IgAN patients currently exists. Its corresponding treatment mainly relies on ACEIs and CS, which have inconsistent effects [25]. Moreover, the adverse effects caused by the long-term application of corticosteroids, such as infection, abnormal glucose and lipid metabolism, and femoral head necrosis [9], limit the application of corticosteroids. Therefore, a refinement of treatment and alternative treatment protocols is much needed.
A growing body of evidence supports the contribution of immunosuppressants in the treatment of IgAN [26, 27]. Leflunomide can be rapidly converted in vivo to active metabolites, inhibiting the production and action of inflammatory mediators and cytokines inextricably linked to kidney disease [16]. These may be the mechanism of leflunomide in treating IgAN. Besides that, combination protocols that include leflunomide have shown significant advantages in efficacy and safety. Lv et al. [28] reported the beneficial effects of combined treatment with leflunomide and corticosteroids for IgAN. In an RCT, Cheng et al. [15] demonstrated that valsartan combined with clopidogrel and leflunomide could protect renal function with minimal adverse effects.
Our meta-analysis focused on the efficacy and safety of low-dose corticosteroids combined with leflunomide for progressive IgA nephropathy. Many studies have shown that urinary protein can cause damage to renal tubular epithelial cells. Thus, proteinuria is considered a risk factor for IgAN progression. Xie et al. [29] reported that relief of proteinuria is essential for long-term renal function protection in IgAN patients. Our results showed that low-dose corticosteroids combined with leflunomide were superior to full-dose corticosteroids in improving urine protein excretion. The SCr and eGFR are also associated with the prognosis of IgAN patients. The present study concluded that there appeared to be no difference between these two treatment options concerning SCr, eGFR, complete remission rate, and overall response rate. In addition, the present study found that low-dose corticosteroids plus leflunomide significantly reduced the incidence of serious adverse events compared to full-dose corticosteroids, suggesting that this combination protocol was relatively safe for treating progressive IgAN.
In contrast to previous studies [28], our study focuses more on the safety and efficacy of low-dose corticosteroids combined with leflunomide in treating progressive IgA nephropathy. In addition, our study also found that the low-dose corticosteroids combined with leflunomide significantly reduced UPE and the incidence of serious adverse events, which was not mentioned in the previous study. Lower doses of corticosteroids minimised adverse effects, and the combination with leflunomide did not affect therapeutic efficacy. This program may be a preferable alternative for IgAN patients with full-dose corticosteroid-associated contraindications. In a mouse model of IgAN, leflunomide and corticosteroids reduced deposition of the glomerular mesangial immune complex, with leflunomide exhibiting a more pronounced effect [30].
Our study had certain limitations. First, a relatively small number of patients was included in the study. We will continue to follow the latest RCTs, allowing us to comprehensively address this limitation in the future. Second, the included studies had qualitative weaknesses, mainly in study design, allocation concealment, and blinding. These limitations may lead to the risk of selection bias and information bias. So, our results should be interpreted with caution. Third, the other limitation of our study is that most patients included were from Asian populations. Therefore, there may be ethnic differences in our findings, and further studies are still needed to evaluate the effect of this combination therapy in a global population. Fourth, the follow-up period was brief and subsequent analyses with long-term follow-up were necessary. A more significant number of high-quality RCTs would still be needed to validate our conclusions.
Conclusions
This meta-analysis suggested that low-dose corticosteroids combined with leflunomide for progressive IgAN provide similar results to full-dose corticosteroids and have advantages in relieving urinary protein and reducing SAEs. This protocol promises to be a new option for treating progressive IgAN.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- UPE:
-
Urine protein excretion
- MD:
-
Mean difference
- CI:
-
Confidence interval
- Scr:
-
Serum creatinine
- OR:
-
Odds ratio
- IgAN:
-
Immunoglobulin A nephropathy
- ESRD:
-
End-stage renal disease
- ACEIs:
-
Angiotensin-converting enzyme inhibitors
- ARBs:
-
Angiotensin receptor blockers
- KDIGO:
-
Kidney Disease Improving Global Outcomes
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- MINORS:
-
Methodological index for nonrandomized studies
- RCTs:
-
Randomized controlled trials
- CS:
-
Corticosteroids
- LEF:
-
Leflunomide
References
Conley ME, Cooper MD, Michael AF. Selective deposition of immunoglobulin A1 in immunoglobulin A nephropathy, anaphylactoid purpura nephritis, and systemic lupus erythematosus. J Clin Invest. 1980;66(6):1432–6. https://doi.org/10.1172/JCI109998.
Berger J. IgA glomerular deposits in renal disease. Transpl Proc. 1969;1(4):939–44.
Robert J, Wyatt, Bruce A, Julian. IgA nephropathy. N Engl J Med. 2013;368(25):2402–14. https://doi.org/10.1056/NEJMra1206793.
Anita McGrogan, Casper FM, Franssen, Corinne S, de Vries. The incidence of primary glomerulonephritis worldwide: a systematic review of the literature. Nephrol Dial Transpl. 2011;26(2):414–30. https://doi.org/10.1093/ndt/gfq665.
Koyama A, Igarashi M, Kobayashi M. Natural history and risk factors for immunoglobulin A nephropathy in Japan. Research Group on Progressive Renal diseases. Am J Kidney Dis. 1997;29(4):526–32. https://doi.org/10.1016/s0272-6386(97)90333-4.
Giuseppe DA. Natural history of idiopathic IgA nephropathy and factors predictive of disease outcome. Semin Nephrol. 2004;24(3):179–96. https://doi.org/10.1016/j.semnephrol.2004.01.001.
François C, Berthoux H, Mohey. Aïda Afiani. Natural history of primary IgA nephropathy. Semin Nephrol. 2008;28(1):4–9. https://doi.org/10.1016/j.semnephrol.2007.10.001.
Chapter 10. Immunoglobulin A nephropathy. Kidney Int Suppl (2011). 2012;2(2):209–217. https://doi.org/10.1038/kisup.2012.23.
Lv J, Zhang H, Chen Y, et al. Combination therapy of prednisone and ACE inhibitor versus ACE-inhibitor therapy alone in patients with IgA nephropathy: a randomized controlled trial. Am J Kidney Dis. 2009;53(1):26–32. https://doi.org/10.1053/j.ajkd.2008.07.029. Epub 2008 Oct 19.
Patrizia Natale, Suetonia C, Palmer M, Ruospo, et al. Cochrane Database Syst Rev. 2020;3(3):CD003965. https://doi.org/10.1002/14651858.CD003965.pub3.
Ali I, Al-Lawati, Heather N, Reich. Is there a role for immunosuppression in immunoglobulin A nephropathy? Nephrol Dial Transpl. 2017;32(suppl1):i30–6. https://doi.org/10.1093/ndt/gfw342.
Zhang C, Chu M. Leflunomide: a promising drug with good antitumor potential. Biochem Biophys Res Commun. 2018;496(2):726–30.
Jiang X-Y, Mo Y, Sun L-Z, et al. Efficacy of methylprednisolone, cyclophosphamide in pediatric IgA nephropathy assessed by renal biopsy. Clin Nephrol. 2009;71(6):625–31. https://doi.org/10.5414/cnp71625.
Josef S, Smolen R, Landewé, Ferdinand C, Breedveld, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2013 update. Ann Rheum Dis. 2014;73(3):492–509. https://doi.org/10.1136/annrheumdis-2013-204573. Epub 2013 Oct 25.
Genyang Cheng D, Liu P, Margetts, et al. Valsartan combined with clopidogrel and/or leflunomide for the treatment of progressive immunoglobulin a nephropathy. Nephrol (Carlton). 2015;20(2):77–84. https://doi.org/10.1111/nep.12359.
Tanqi Lou C, Wang Z, Chen, et al. Randomised controlled trial of leflunomide in the treatment of immunoglobulin A nephropathy. Nephrol (Carlton). 2006;11(2):113–6. https://doi.org/10.1111/j.1440-1797.2006.00547.x.
Moher D, Liberati A, Tetzlaff J, et al. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009;62(10):1006–12. https://doi.org/10.1016/j.jclinepi.2009.06.005. Epub 2009 Jul 23.
Miranda Cumpston T, Li MJ, Page, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev. 2019;10:ED000142. https://doi.org/10.1002/14651858.ED000142.
Karem Slim E, Nini D, Forestier, et al. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. 2003;73(9):712–6. https://doi.org/10.1046/j.1445-2197.2003.02748.x.
Higgins JP, Green S, editors. Cochrane handbook for systematic reviews of interventions. Version 5.3.0. The Cochrane Collaboration. Available from: www.cochrane-handbook.org.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin T Rials. 1986;7:177–88. https://doi.org/10.1016/0197-2456(86)90046-2.
Lulin Min Q, Wang L, Cao, et al. Comparison of combined leflunomide and low-dose corticosteroid therapy with full-dose corticosteroid monotherapy for progressive IgA nephropathy. Oncotarget. 2017;8(29):48375–84. https://doi.org/10.18632/oncotarget.16468.
Ni Z, Zhang Z. Leflunomide plus low-dose prednisone in patients with progressive IgA nephropathy: a multicenter, prospective, randomized, open-labeled, and controlled trial. Ren Fail. 2021;43(1):1214–21. https://doi.org/10.1080/0886022X.2021.1963775.
Li Y, Xiong Y, Huang T, et al. Clinical efficacy and safety of full-dose versus half-dose corticosteroids plus leflunomide for IgA nephropathy. BMC Nephrol. 2021;22(1):364. https://doi.org/10.1186/s12882-021-02555-z.
Cabral DBC, de Sandes-Freitas TV, Medina-Pestana JO, et al. Clinical features, treatment and prognostic factors of post-transplant immunoglobulin A nephropathy. Ann Transplant. 2018;23:166–75. https://doi.org/10.12659/AOT.907167.
Thomas Rauen C, Fitzner F, Eitner, et al. Effects of two immunosuppressive treatment protocols for IgA Nephropathy. J Am Soc Nephrol. 2018;29(1):317–25. https://doi.org/10.1681/ASN.2017060713. Epub 2017 Oct 17.
Thomas Rauen F, Eitner C, Fitzner, et al. Intensive supportive care plus Immunosuppression in IgA Nephropathy. N Engl J Med. 2015;373(23):2225–36. https://doi.org/10.1056/NEJMoa1415463.
Lv G. Efficacy and safety of leflunomide combined with corticosteroids for the treatment of IgA nephropathy: a Meta-analysis of randomized controlled trials. Ren Fail. 2022;44(1):1011–25. https://doi.org/10.1080/0886022X.2022.2085576.
Linshen Xie C, Tan J. Mycophenolic acid reverses IgA1 aberrant glycosylation through up-regulating cosmc expression in IgA nephropathy. Int Urol Nephrol. 2013;45(2):571–9. https://doi.org/10.1007/s11255-012-0313-y. Epub 2012 Nov 8.
Chen Yi-zhi, Zhao Xue-zhi, Wu J, et al. Combination regimen of leflunomide plus methylprednisolone in a female patient with reactive arthritis and concomitant IgA nephropathy. Chin Med J (Engl). 2010;123(3):375–8.
Acknowledgements
All authors have no acknowledgments to disclose.
Reporting checklist
The authors have completed the PRISMA checklist.
Funding
No specific funding.
Author information
Authors and Affiliations
Contributions
HXP and LP designed the research, interpreted the data, and revised the paper. ZDX, XBW, and ZX performed the data extraction and meta-analysis. ZDX drafted the paper. All of the authors approved the submitted and final versions.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, D., Xia, B., Zhang, X. et al. Efficacy and safety of low-dose corticosteroids combined with leflunomide for progressive IgA nephropathy: a systematic review and meta-analysis. BMC Urol 24, 56 (2024). https://doi.org/10.1186/s12894-024-01438-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12894-024-01438-3