
Abstract
Disturbances of the sleep-wake cycle are highly prevalent and diverse. The aetiology of some sleep disorders, such as circadian rhythm sleep-wake disorders, is understood at the conceptual level of the circadian and homeostatic regulation of sleep and in part at a mechanistic level. Other disorders such as insomnia are more difficult to relate to sleep regulatory mechanisms or sleep physiology. To further our understanding of sleep-wake disorders and the potential of novel therapeutics, we discuss recent findings on the neurobiology of sleep regulation and circadian rhythmicity and its relation with the subjective experience of sleep and the quality of wakefulness. Sleep continuity and to some extent REM sleep emerge as determinants of subjective sleep quality and waking performance. The effects of insufficient sleep primarily concern subjective and objective sleepiness as well as vigilant attention, whereas performance on higher cognitive functions appears to be better preserved albeit at the cost of increased effort. We discuss age-related, sex and other trait-like differences in sleep physiology and sleep need and compare the effects of existing pharmacological and non-pharmacological sleep- and wake-promoting treatments. Successful non-pharmacological approaches such as sleep restriction for insomnia and light and melatonin treatment for circadian rhythm sleep disorders target processes such as sleep homeostasis or circadian rhythmicity. Most pharmacological treatments of sleep disorders target specific signalling pathways with no well-established role in either sleep homeostasis or circadian rhythmicity. Pharmacological sleep therapeutics induce changes in sleep structure and the sleep EEG which are specific to the mechanism of action of the drug. Sleep- and wake-promoting therapeutics often induce residual effects on waking performance and sleep, respectively. The need for novel therapeutic approaches continues not at least because of the societal demand to sleep and be awake out of synchrony with the natural light-dark cycle, the high prevalence of sleep-wake disturbances in mental health disorders and in neurodegeneration. Novel approaches, which will provide a more comprehensive description of sleep and allow for large-scale sleep and circadian physiology studies in the home environment, hold promise for continued improvement of therapeutics for disturbances of sleep, circadian rhythms and waking performance.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
1 Quantifying the Quality of Sleep and Wakefulness
1.1 A Multivariate Phenomenology
Sleep is a major determinant of well-being, mental and physical health and understanding sleep-health relations, and sleep disorders are dependent on adequate quantification of sleep. Sleep and wake states are characterised by constellations of variables representing nearly all levels of system organisation ranging from gene expression (O’Callaghan et al. 2018), neuronal firing patterns (McKillop and Vyazovskiy 2018), neurotransmitter release (Zant et al. 2016; Luppi and Fort 2018), endocrine and autonomic nervous system status (Morris et al. 2012; Fink et al. 2018), body and brain temperature (Landolt et al. 1995), responsiveness to external stimuli (Ermis et al. 2010), motor behaviour (Horner and Peever 2017) to changes in consciousness (Casali et al. 2013). Which variables are essential to sleep quality and how these variables contribute to sleep’s associations with well-being, physical health and brain function remain, however, largely unknown even though several hypotheses have been proposed.
Here we will summarise some recent developments in research on sleep physiology, circadian rhythms and waking performance and their interrelations in humans without sleep complaints and discuss some implications for the understanding and development of non-pharmacological and pharmacological therapeutics for sleep and circadian disorders.
1.1.1 Sleep
Sleep has a rich phenomenology consisting of both subjective and objective aspects, and new facets continue to be reported. In humans, sleep comprises the subjective experience of the cessation of consciousness (falling asleep), the presence of dreams and nightmares or the feeling of not having slept all night. After waking up, the sleep experience can be reported as sleep quality and sleep depth. At another level sleep is a state of the brain and the body which in humans and animals can be quantified by objective behavioural criteria such as immobility and arousal thresholds and by a wide range of physiological variables. The electroencephalogram, electromyogram, electrooculogram, electrocardiogram, endocrine parameters, and respiratory parameters are among the physiological variables most commonly recorded in laboratory studies of human sleep. A recording of these state variables is referred to as a polysomnogram (PSG) (Berry et al. 2017) (see Fig. 1). Currently sleep is primarily quantified by sleep staging based on EEG, EMG, and EOG signals. Sleep is subdivided into non-rapid eye movement (NREM) sleep and rapid eye movement sleep (REM). In the current sleep staging guidelines for humans, NREM sleep will be further segmented in N1–N3 with N3 often referred to as slow-wave sleep (SWS). Previously NREM sleep was subdivided in stages 1–4 with stages 3 + 4 being combined as SWS. After sleep staging the sleep process is quantified by variables such as the latency to sleep onset, the duration of the various sleep stages, the relative contribution of sleep stages to total sleep time or the transitions between sleep stages. NREM sleep typically precedes REM sleep, and the ultradian cycle of the alternation of NREM and REM sleep is one characteristic of interest. The duration of the NREM-REM cycle scales in a lawful manner to body and brain size sleep suggesting that it is closely linked to a primordial but as yet unknown function of sleep (Frank and Heller 2019). Sleep can be further characterised by its continuity, i.e. are sleep and wake episodes consolidated or are they interrupted by brief intrusions of the other state. Sleep continuity can be quantified as sleep efficiency (i.e. total sleep time/time in bed), wake after sleep onset, the number of awakenings, EEG arousals or the distribution of the duration of uninterrupted sleep bouts as assessed by survival analysis or other methods (Klerman et al. 2013; Svetnik et al. 2018).

Nocturnal sleep in a young adult. Hypnogram, spectrogram and time course of slow-wave activity (SWA = EEG power in the 0.75–4.5 Hz range). W wakefulness, R REM sleep, N1–N3 NREM sleep stages 1–3
Signal analysis-based approaches such as spectral analysis have been used to further characterise sleep although these approaches are still not standard in most research and clinical studies. Quantification of specific electrophysiological phenomena such as slow waves and sleep spindle oscillations (Dijk et al. 1993; Lazar et al. 2015), muscle tone (Brunner et al. 1990a; Jeppesen et al. 2018) or heart rate variability (Yang et al. 2018; Viola et al. 2008a) and changes thereof across the sleep episode or in response to pharmacological and non-pharmacological sleep manipulations have provided new insights into the sleep process. Quantification of slow waves through spectral analysis as power density in the low-frequency range (0.75–4.5 Hz) and commonly referred to as slow-wave activity (SWA) has formed the basis for quantification of the homeostatic process in the two-process model of sleep regulation (Borbély 1982; Daan et al. 1984). Topographical analyses using multi-electrode EEG recordings have identified local aspects of sleep which may be relevant to local recovery processes (Kattler et al. 1994; Huber et al. 2006), memory consolidation (Rasch and Born 2013), the dream process (Siclari et al. 2017) or maybe the lack of cessation of consciousness despite the presence of global sleep as observed in insomnia (Riedner et al. 2016). Analyses of synchronisation across multiple EEG derivations and EEG frequencies have shown that the three vigilance states (Wakefulness, NREM and REM) are very different with REM sleep being the most synchronised state (Achermann et al. 2016), even though the REM sleep EEG is commonly described as desynchronised. Analyses of the temporal characteristics of the EEG have revealed phenomena such as phase locking between slow oscillations and sleep spindles (Klinzing et al. 2016) and ultra-slow oscillatory processes in spindle activity with periods of approximately 50–75 s (Lecci et al. 2017; Lazar et al. 2018).
1.1.2 Wakefulness
Sleep research tacitly assumes that the quality of wakefulness relates, at least in part, to the quality of sleep, although the reverse pathway is also plausible. Wakefulness is subjectively experienced, with alertness, sleepiness and fatigue being commonly used words to describe the quality of wakefulness. The subjective quality of wakefulness in terms of perceived alertness can be quantified with the Karolinska sleepiness scale (Akerstedt et al. 2017) or the Epworth sleepiness scale (Johns 1991) or objectively assessed as the ability to stay awake using the maintenance of wakefulness test or the propensity to fall asleep by the multiple sleep latency test (Sullivan and Kushida 2008). The quality of wakefulness can be characterised by absence or intrusion of sleep like electroencephalographic features such as theta activity (Greneche et al. 2008; Cajochen et al. 1995). The quality of wakefulness can be measured as the ability to remain vigilant and respond to stimuli in simple, and rather boring, test conditions such as in the psychomotor vigilance test (Lim and Dinges 2008). Finally, the quality of wakefulness may be assessed by the performance on tasks probing more complicated brain functions like working memory, executive function tests and the effort it takes to perform these tasks (Lo et al. 2012; Groeger et al. 2014) and tasks related to our professional and social life, e.g. driving (Shekari Soleimanloo et al. 2017).
The quality of wakefulness immediately following sleep is of special interest. Following the transition from sleep to wakefulness as defined by the PSG, it takes the brain some time to reach full waking performance (Balkin et al. 2002; Santhi et al. 2013). This process, referred to as sleep inertia, is relevant in operational conditions, for example, when pilots take naps on long haul flights, and may be exacerbated by non-pharmacological (e.g. sleep restriction) (Balkin and Badia 1988) and pharmacological (Boyle et al. 2012a; Cohen et al. 2010a) treatments of sleep disturbances.
Understanding how the different dimensions of sleep and wakefulness are interrelated, e.g. which physiologic aspect of sleep predicts the subjective quality of sleep, how sleep physiology relates to the quality of waking and how sleep- and wake-promoting therapeutics affect wake and sleep quality, respectively, is one of the challenges of sleep research and sleep medicine.
We will first discuss how sleep physiology is regulated in response to sleep loss.
2 Homeostatic Regulation of Sleep Physiology
Homeostatic regulation of sleep physiology has been investigated since the early days of modern sleep research. Most frequently used protocols are total sleep deprivation, e.g. not sleeping at all for 40 or 64 h, repeated partial sleep deprivation (e.g. a week of only 6 h of sleep per day), sleep extension, selective sleep deprivation (e.g. suppression of SWS) and nap studies. Sleep propensity and sleep structure of recovery sleep was the primary outcome measure in many of these studies. A major limitation of most of these studies is that time in bed during recovery sleep was restricted and sleep termination was thus not spontaneous. As a consequence the homeostatic regulation of human sleep duration is not well documented.
2.1 Sleep Propensity and Sleep Continuity
Total sleep deprivation, repeated partial sleep deprivation and selective disruption of SWS all lead to an increase in subjective and objective sleep propensity, i.e. subjective sleepiness and a reduction in the latency to sleep onset. These interventions also lead to a reduction in wake after sleep onset and the number of awakenings, i.e. sleep continuity increases with increasing homeostatic sleep pressure. Increasing time in bed, i.e. extending the nocturnal sleep opportunity (Bei et al. 2014, 2017; Skorucak et al. 2018) or taking naps and in particular naps in the later part of the day (Werth et al. 1996), leads to increases in the objective and subjective latency to sleep onset and also leads to a reduction in sleep continuity. Remarkably, a large-scale observational study in the community indicated that short sleep is associated with lower sleep efficiency and more awakenings, i.e. a pattern opposite to that observed in interventional laboratory studies (Akerstedt et al. 2019). This probably implies that short sleep in the community is caused by ‘sleep problems’ rather than imposed sleep restriction.
2.2 NREM Sleep, SWS and SWA
In humans NREM sleep is subdivided into N1, N2 and slow-wave sleep. Slow-wave sleep and slow-wave activity, i.e. EEG power density in the low-frequency range content of naps increases as naps are taken later in the day (Dijk et al. 1987a), nocturnal slow-wave sleep is increased after acute total sleep deprivation (Borbély et al. 1981), and slow-wave sleep in nocturnal sleep is decreased after a nap taken later in the day (Werth et al. 1996). Slow-wave sleep is only marginally increased after repeated partial sleep deprivation (Brunner et al. 1993). Slow-wave sleep deprivation leads to an increase of SWS in subsequent undisturbed sleep (Dijk et al. 1987b; Dijk and Beersma 1989). These responses are consistent with a saturating exponential increase of slow-wave sleep pressure with time awake (Dijk et al. 1990a) and an approximately exponential decline of slow-wave sleep pressure during sleep (Dijk et al. 1990b; Achermann et al. 1993). The time constants of these functions are such that most of the dynamic range of slow-wave sleep is covered within a normal 24-h sleep-wake cycle (Skorucak et al. 2018; Rusterholz et al. 2010). This implies that SWS is primarily responsive to acute variation in sleep and wakefulness. Some data suggest that increasing the intensity of wakefulness through physical exercise or exposure to particular waking experiences may lead to global or local enhancement of slow-wave sleep (Horne and Moore 1985; Melancon et al. 2015; Huber et al. 2004).
2.3 REM Sleep
The homeostatic regulation of REM sleep is different from NREM sleep. Acute total sleep deprivation has no major effect on REM sleep during subsequent recovery sleep when the duration of recovery sleep is experimentally constrained (Borbély et al. 1981). Repeated partial sleep deprivation, which is not associated with a loss of SWS but is associated with a loss of REM sleep, leads to a REM sleep rebound during recovery sleep (Brunner et al. 1990b; Skorucak et al. 2018). REM sleep deprivation in the beginning of the sleep period leads to a rebound in the second half of the same sleep period (Beersma et al. 1990). A typical characteristic of REM sleep deprivation is that attempts to initiate REM sleep occur in clusters and increases in the course of REM sleep deprivation (Endo et al. 1998). A pronounced REM sleep rebound was also observed during withdrawal from REM sleep suppressing antidepressants (Landolt and de Boer 2001). Some authors have suggested that REM sleep’s homeostatic regulation is primarily related to NREM sleep preceding REM sleep rather than preceding wakefulness (see Frank and Heller 2019).
It is often tacitly assumed that sleep after sleep loss is good sleep which implies that more SWS, shorter sleep latencies and fewer awakenings are the hallmarks of good sleep. Whether more SWS or more REM sleep is a positive characteristic depends on whether one considers total sleep deprivation or partial sleep deprivation the more natural challenge of sleep regulatory systems.
2.4 Age- and Sex-Related Differences in Sleep Physiology
Slow-wave sleep and slow-wave activity decline during the adult life span but so do sleep spindle activity and REM sleep (Schwarz et al. 2017; Della Monica et al. 2018). Age-related reductions in REM sleep are probably underestimated because as mentioned, in most studies, time in bed was limited. Under ad libitum sleep conditions, age-related reductions in REM sleep may be as large as reductions in SWS (Klerman and Dijk 2008). Apart from changes in SWS and REM sleep, reductions in sleep efficiency and increases in the number of awakenings are consistently observed in healthy ageing. At the same time, the subjective quality of sleep as reported by the sleeper, rather than construed by sleep researchers, may not change much in healthy ageing (Akerstedt et al. 2016; Della Monica et al. 2018), and this is commonly interpreted as a habituation to reduced objective sleep quality.
Sex differences in sleep physiology primarily concern slow-wave sleep with women spending more time in slow-wave sleep and higher slow-wave activity (Dijk et al. 1989a; Svetnik et al. 2017). The age-related decline in SWA appears shallower in women than in men. Sleep continuity measures are not markedly different between the sexes (Carrier et al. 2017; Della Monica et al. 2018).
2.5 Sleep Physiology and the Subjective Quality of Sleep
A personal experience-oriented approach to sleep may define good sleep as sleep associated with sleep satisfaction or satisfactory alertness during the subsequent waking day. Sleep research may aim to understand how subjective sleep quality relates to objective aspects of sleep. When we only consider recent observational studies in which sleep in participants without sleep complaints were assessed by polysomnography, the consensus conclusion across these cross-sectional studies is that sleep efficiency/continuity is a significant determinant of reported sleep quality and the feeling of being refreshed upon awakening (Akerstedt et al. 2016; Kaplan et al. 2017a, b; Della Monica et al. 2018). This association is present across the adult life span and according to one study is much stronger in women than in men (Della Monica et al. 2018). Remarkably, these studies imply that deep sleep, i.e. SWS or N3, is not a main determinant of subjective measures of sleep quality. In one study REM sleep duration was positively associated with subjective sleep quality (Della Monica et al. 2018) (see Fig. 2). It should be noted that even though significant PSG predictors were identified, they explained only a small portion of the variance in subjective sleep quality.

Contribution of polysomnographically determined sleep variables to subjective sleep quality. Effect size is quantified with Kendall’s tau after correcting for age and sex. Vertical lines represent large, medium and small effect sizes. NAW number of awakenings, REM rapid eye movement sleep, TST total sleep time, SEFF sleep efficiency, LPS latency to persistent sleep, SWS slow-wave sleep, SWA slow-wave activity, SFA sleep spindle frequency activity. Modified from Della Monica et al. (2018)
2.6 Sleep Physiology and the Quality of Wakefulness
2.6.1 Observational Studies
How sleep is related to the quality of subsequent wakefulness is a key question when we consider sleep as a process of recovery and preparation for the next wake episode. Total sleep time is a correlate of subsequent waking quality such that in healthy participants, self-reported and objectively assessed total sleep time associates with alertness the next day as assessed by the multiple sleep latency test (MSLT) (Klerman and Dijk 2005). Longitudinal studies have demonstrated that the night-to-night variation in sleep duration is associated with subjective sleepiness (Akerstedt et al. 2013). When we consider performance on specific tasks as an indicator of the quality of wakefulness, the picture emerging from observational studies in which sleep duration was assessed by self-report becomes more complex. For example, in a large-scale Internet-based study, it was found that both short and long sleep were associated with reduced performance on reasoning and verbal skills and no relationship between sleep duration and short-term memory performance was observed (Wild et al. 2018). Similarly, in an analysis of UK biobank data, both short and long sleep (self-reported) were associated with impaired performance, and the complaint of insomnia was not associated with reduced performance (Kyle et al. 2017).
These observations imply that good sleep and waking function require an optimal balance between sleep and wake duration. If finding the right sleep-wake balance is indeed essential for obtaining good quality sleep and waking function, then a number of questions emerge. What is ‘normal/optimal’ sleep duration and how to assess sufficiency of sleep on an individual basis? In this context, individual differences in sleep need and changes in sleep need across the adult life span may be considered.
Whether and how specific sleep stages predict the quality of wakefulness or brain function, i.e. cognition, has been investigated in young and older participants. In a comprehensive review of the literature addressing this question, it was concluded that a specific contribution of a specific sleep stage to cognition has not been firmly established (Scullin and Bliwise 2015). In one recent study, the association between nocturnal sleep and waking function was quantified across the healthy adult life span by an extensive battery of subjective and objective measures. After a factor analysis of the waking performance measures, it was found that SWS relates to a latent factor labelled ‘Speed’ of performance and REM sleep to ‘Accuracy’. Importantly, sleep continuity was found to be the strongest predictor of ‘Accuracy’, which contains elements of executive function and working memory performance (Della Monica et al. 2018) (see Fig. 3).

Contribution of polysomnographically determined sleep variables to waking performance. Performance factors were derived from a factor analysis of performance measures. Colour coding represents Kendall’s correlation coefficient, after controlling for sex and age. Note the negative correlation between SWA measures and response time, i.e. more SWA implies faster response times. A number of awakenings are negatively and REM sleep is positively correlated with accuracy. Modified from Della Monica et al. (2018)
Several observational studies have focused on contributions of specific aspects of sleep to other aspects of waking/brain function such as the association between sleep spindles and memory consolidation (Lafortune et al. 2014) and slow-wave sleep and metabolic clearance (e.g. Ju et al. 2018; Hladky and Barrand 2017). In the specific contexts of these studies, evidence for the contribution of slow-wave sleep, sleep spindles, REM sleep and sleep continuity to brain function has been reported although the magnitude of these effects and relative importance of various aspects of sleep remains to be established.
2.6.2 Interventional Studies
Interventional studies may provide more definitive insights into the relation between sleep and waking function. Acute total sleep deprivation, selective disruption of SWS and chronic sleep restriction all lead to an increase in subjective sleepiness and a reduction in objectively or subjectively assessed latency to sleep onset, measured at either habitual bedtime or during the daytime in the multiple sleep latency test (Carskadon and Dement 1987; Dijk et al. 2010a; Lo et al. 2012). Many studies have investigated the effects of sleep loss on aspects of brain function beyond sleepiness. Most studies implemented acute total sleep deprivation, but some used chronic partial sleep deprivation or selective disruption of SWS or sleep continuity (Lowe et al. 2017; Lo et al. 2012; Skorucak et al. 2018; Groeger et al. 2014). The most consistent finding is that sleep loss leads to impairment of vigilant attention. Many other aspects of waking performance are also affected. These include working memory, executive function, etc. Several studies have reported effects on memory consolidation as well. Repeated partial sleep deprivation studies have established that there is a progressive deterioration of waking performance and in particular of sustained attention suggesting that adaptation to sleep restriction does not occur (Van Dongen et al. 2003; Lo et al. 2012). It should be noted that repeated partial sleep deprivation does not lead to a large deficit in SWS but primarily to a deficit in REM sleep and N2, implying that the cognitive deficits cannot be attributed to SWS, but should be attributed to TST or REM sleep (Skorucak et al. 2018). It has been hypothesised that the cognitive deficits of sleep restriction were related to extension of the wake period beyond 16 h (Van Dongen et al. 2003), but this hypothesis was dismissed in a forced desynchrony study in which sleep-wake ratio was manipulated within ‘days’ shorter than 20 h. Despite the fact that wake episodes were never longer than 16 h, increasing the wake-sleep ratio nevertheless led to deficits in vigilant attention (McHill et al. 2018). This implies that it is simply the balance between wake and sleep duration that determines waking function and not the absolute duration of wakefulness.
Few studies have simultaneously assessed multiple aspects of waking function but those studies that did have shown that higher cognitive functions are less affected than relatively simple functions (e.g. sustained attention on the PVT) (see Fig. 4). In fact, it appears that if the sleep-deprived brain is able to engage with a task, deficits are relatively small. However, at the same time, the self-reported effort markedly increases. This suggests that insufficient sleep, at least with the time span of a week or so, does not lead to a fundamental inability of the waking brain to function even when, for example, working memory tasks with a high executive load are to be performed (Lo et al. 2012). The brain primarily struggles to stay awake and allocates more effort to maintain performance. Increases in subjective sleepiness and objective sleepiness and measures of effort are among the first signs of experimentally induced insufficient sleep and are among the dependent variables with the largest effect sizes (Balkin et al. 2004; Groeger et al. 2014; Lo et al. 2012). One major limitation of these studies is that assessment of higher brain function in a realistic context was often not implemented. The implication is that functions such as creativity, complex decision-making and planning may still be markedly affected by insufficient sleep.

Effects on 1 week of sleep restriction (6 h time in bed) on the Karolinska sleepiness scale (KSS), the 10% slowest reaction times on the psychomotor vigilance task (PVT), accuracy on the sustained attention to response task (SART) and accuracy of the verbal 1-, 2-, and 3-back. Modified from Lo et al. (2012)
2.6.3 Individual Differences in Sleep Need and Response to Sleep Loss
Habitual long and short sleepers of approximately the same age differ in sleep propensity and sleep need when we consider total sleep time as the relevant measure of sleep propensity. However, nocturnal sleep latencies are longer in long sleepers, and short sleepers show more signs of intrusion of sleepiness-related theta activity during wakefulness (Aeschbach et al. 1996, 2001). Apparently long and short sleepers differ in their ‘preferred’ or ‘tolerated’ level of sleepiness. Whether and how this relates to homeostatic aspects of sleep regulation or to the longer circadian biological night observed in long sleepers remain unclear (Aeschbach et al. 2003).
Ageing is a major determinant of sleep propensity. Self-reported sleep duration and polysomnographically assessed total sleep time decline with age while at the same time daytime sleepiness decreases (Roenneberg 2013; Dijk et al. 2010a; Akerstedt et al. 2018). The most parsimonious explanation for these observations is that sleep need, at least as measured by sleep propensity, declines with age (Skeldon et al. 2016). An age-related reduction in the maximum capacity for sleep and reduction in sleep propensity has been demonstrated convincingly in protocols in which older and young adults spent 16 h in bed and this for several days. Older people slept 1.5 h less than young adults (who slept 8.7 h) but nevertheless were less sleepy (Klerman and Dijk 2008). That this reduction in the TST doesn’t just reflect a reduced capacity for sleep but also for sleep need is supported by interventional studies which demonstrate that in older people the detrimental effects of total acute and repeated partial sleep deprivation are much smaller than in young people (Adam et al. 2006; Landolt et al. 2012; Zitting et al. 2018; Schwarz et al. 2018). Observational studies have not always confirmed these observations (Wild et al. 2018).
Individual differences in the deterioration of waking performance in response to total sleep deprivation and repeated partial sleep deprivation are also observed when only young adults are considered (Van Dongen et al. 2004; Rupp et al. 2012).
Several genetic variants associated with individual variation in sleep duration, sleep timing and sleep structure have been identified (Doherty et al. 2018; Rhodes et al. 2018; Viola et al. 2007; Archer et al. 2018). How genetic variants may affect response to sleep manipulations and pharmacological agents for wake and sleep promotion has been reviewed elsewhere (Bachmann et al. 2012; Holst et al. 2014; Landolt et al. 2018).
2.7 Effects of Insufficient Sleep on Peripheral Physiology, Endocrinology and the Blood Transcriptome
Insufficient sleep not only affects brain function and waking performance but also peripheral systems. This has been assessed by monitoring physiology during recovery sleep from total or chronic partial sleep deprivation and during wakefulness following insufficient sleep. Autonomic tone changes in response to sleep loss such that during recovery sleep, there is shift to parasympathetic dominance as reflected in measures of heart rate variability (Viola et al. 2008a). Several hormones respond to insufficient sleep such that testosterone is suppressed, and appetite-regulating hormones ghrelin and leptin are up- and downregulated, respectively (Hanlon and Van Cauter 2011). Several markers of immune function respond to insufficient sleep such that immune function appears impaired (Irwin and Opp 2017). Finally genome-wide assessment of transcripts in whole blood has shown that sleep loss leads to changes in transcripts implicated in chromatin modification, gene expression regulation, macromolecular metabolism and inflammatory, immune and stress responses (Moller-Levet et al. 2013). Some of these changes may explain why and how insufficient sleep leads to adverse health outcomes such as obesity.
2.8 Sleep Physiology and Sleep Homeostasis as a Target for Pharmacological and Non-pharmacological Therapeutics
2.8.1 Sleep Promotion
Improving sleep quality in general focuses on latency to sleep onset, total sleep time and sleep continuity (maintenance) aspects such as wake after sleep onset or specific aspects of sleep structure such as slow-wave sleep. Peripheral correlates of sleep quality are in general not considered as target for sleep improvement.
Increasing homeostatic sleep pressure can improve latency to sleep onset, sleep continuity and total sleep time within a given time in bed period. This can be accomplished by increasing wake duration prior to sleep or by increasing the intensity of wakefulness through either physical or maybe mental activity. Such an approach may be useful in ageing and insomnia since in these conditions, optimal homeostatic sleep pressure may not be achieved because of daytime napping or excessive time in bed (Cross et al. 2015). Indeed, the recommended treatment of insomnia, which is the complaint of difficulties initiating and maintaining sleep, is cognitive behavioural therapy, the main component of which is thought to be sleep restriction (Maurer et al. 2018). An alternative approach to increase homeostatic sleep pressure may be to pharmacologically target the molecular signalling pathways of sleep homeostasis. Emerging pathways are adenosine and prostaglandins (Holst and Landolt 2018; Urade 2017; Korkutata et al. 2019) although approved drugs for these targets are not yet available.
Available pharmacological approaches of insomnia may target wake after sleep onset or sleep latency, but in general these approaches do not target the (largely unknown) molecular signalling pathways of sleep homeostasis but instead focus on inhibiting mechanisms related to ‘arousal’ and ‘wake promotion’, e.g. GABAergic, histaminergic and orexinergic mechanisms (Landolt et al. 2018).
Since SWA/SWS is accurately regulated in acute sleep manipulation protocols, is often considered a key indicator of sleep homeostasis, shows a marked age-related decline and has been implicated in memory consolidation, it has been and remains a target for sleep promotion and improvement (Mander et al. 2017; Wilckens et al. 2018). Non-pharmacological approaches include exercise and neuromodulation (Kredlow et al. 2015; Wilckens et al. 2018). In one type of neuromodulation, acoustic stimuli are phase locked to spontaneous slow waves. This has been reported to enhance slow waves in young people, but not in older people (Garcia-Molina et al. 2018). Whether this enhancement improves subjective sleep quality and waking function has not been firmly established. Rocking stimulation has recently been reported to increase SWS, spindle density in SWS and memory consolidation in healthy young adults (Perrault et al. 2019).
Pharmacological enhancement of slow-wave sleep has been accomplished by compounds that have different mechanisms of action. Agonists of the extra-synaptic GABAA receptor such as gaboxadol, also known as THIP, reliably induce SWS and SWA in healthy participants at baseline, in a model of transient insomnia (traffic noise, Dijk et al. 2012), a model of sleep onset insomnia (Mathias et al. 2001), a circadian phase advance model (Walsh et al. 2007), older participants (Lancel et al. 2001) and insomnia patients (Lankford et al. 2008). Interestingly, the effects of gaboxadol on sleep are much stronger in women than in men (Dijk et al. 2010b; Ma et al. 2011; Roth et al. 2010).
These enhancements of SWS were accompanied by modest improvement in sleep continuity and subjective sleep quality and in one report an improvement of daytime sleepiness and waking performance (Walsh et al. 2008). Gaboxadol was not fully developed as a treatment for insomnia, but its unique action on GABAA receptors containing the delta subunit and its effects on sleep and the EEG remain intriguing.
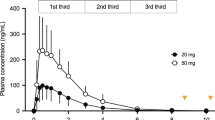
The most commonly used drugs for the treatment of insomnia are allosteric modulators of the GABAA receptor. In general these drugs do have hypnotic effects, e.g. improve wake after sleep onset (WASO), but do not enhance SWS, although zolpidem can enhance visually scored SWS (Bettica et al. 2012). Spectral analysis of the sleep EEG has revealed that the effects of all GABAA receptor allosteric modulators lead to a very similar spectral profile with reductions in delta and theta activity and enhancement in sigma activity (Arbon et al. 2015; Brunner et al. 1991; Trachsel et al. 1990) (see Fig. 5). This profile is very different from the spectral changes induced by physiological enhancement of homeostatic sleep pressure through sleep deprivation. The increase in visually scored SWS which is sometimes reported following zolpidem administration appears to be related to an increase in activity in very low-frequency slow waves (Landolt et al. 2000).

The hypnotic and EEG effects of GABAA receptor allosteric modulators can be separated, i.e. they are mediated by different receptor systems, and the rich variety of GABAA receptors remains a target for the pharmacological improvement of sleep (Wisden et al. 2017). In addition to GABAA, GABAB receptors also appear to be involved in sleep regulation. GABAB receptors mediate some of the effects of gamma-hydroxybutyrate (GHB) and its sodium salt: sodium oxybate (SO). SO is the current first-line treatment of excessive daytime sleepiness and cataplexy in narcolepsy type 1. GHB induces SWS (Van Cauter et al. 1997; Dornbierer et al. 2019) and sleep onset REM periods (Vienne et al. 2012) and has been reported to improve performance (Walsh et al. 2010).
Antagonists of serotonergic 5-HT2A and histaminergic H1 receptors the latter being widely used as nonprescription drugs for the treatment of sleep disturbances also enhance SWS. This maps on to the serotonergic and histaminergic pathways implicated in sleep-wake regulation generation (Landolt et al. 2018; Yu et al. 2018). The spectral profile of these effects is much more similar, although not identical, to the effects of sleep deprivation than the effects GABAA receptor allosteric modulators, i.e. these antagonists induce an increase in delta and theta activity (Dijk et al. 1989b; Landolt and Wehrle 2009). The pharmacological enhancement of SWS by 5-HT2A antagonists is in general not accompanied by a shortening of sleep latency, an improvement in sleep continuity or a subjective sleep quality (Landolt et al. 1999). Alcohol is by many used as a sleep facilitator. It indeed hastens sleep onset but leads to more wakefulness in the second half of the sleep period, especially in older participants (Landolt et al. 1996). The effects of alcohol on EEG power spectra are different from those induced by GABAA allosteric modulators (Dijk et al. 1992a).
Sleep spindles are not a target in drug development for insomnia, even though several benzodiazepines and z-drugs enhance sleep spindle activity, and these changes have been related to changes in plasticity (Wisden et al. 2017).
Even though REM sleep deficits have been reported in insomnia (Baglioni et al. 2014) and in other conditions such as Alzheimer’s disease (Winsky-Sommerer et al. 2018) and REM sleep is a positive predictor of subjective sleep quality and waking performance (Della Monica et al. 2018), REM sleep enhancement does not appear to have been a target for pharmacological treatments. In fact REM sleep enhancement and reduced latencies to REM sleep observed after administration of orexin antagonists, e.g. (Bettica et al. 2012), are considered as an unwanted effect because of its potential link with narcolepsy and cataplexy (Jacobson et al. 2017).
Negative effects of hypnotics on waking performance after drug-enhanced sleep remain widespread despite continuing efforts to reduce these residual effects. For example, in one detailed analysis of the effects of zopiclone and eszopiclone, it was found that for some aspects of performance residual effects lasted as long as 11 h after dosing, i.e. until mid-late morning (Boyle et al. 2012a).
2.8.2 Wake Promotion
Extending sleep is one approach to reduce sleepiness caused by sleep restriction although this approach is obviously not realistic in idiopathic hypersomnolence (Baumann 2018).
Non-pharmacological approaches, other than extra sleep, to improve waking function include light exposure. Light has now been shown in a large number of experiments (both in humans and animals) to have direct alerting effects (Pachito et al. 2018; Viola et al. 2008b; Gaggioni et al. 2014). The photoreceptor and molecular and neuroanatomical signalling pathways have in part been elucidated (LeGates et al. 2014). Considering characteristics of light as an important non-pharmacological approach to improving alertness is relevant in view of the time we spend indoors where we are exposed primarily to artificial light.
Pharmacological approaches to improve alertness/wakefulness include caffeine (Wyatt et al. 2004) which through its adenosinergic action is thought to interact with sleep homeostatic mechanisms and indeed disrupts sleep (Clark and Landolt 2017). Although widely used, some of the effects of caffeine remain poorly understood. For example, and somewhat paradoxical, caffeine consumption may be associated with sleepiness (Wyatt et al. 2004). Patterns of caffeine consumption may suggest that it is primarily used to reduce sleep inertia and new delivery systems for this application have been developed (Newman et al. 2013).
Pharmacological approaches target the main wake-promoting systems such as the dopaminergic and histaminergic (H3) systems (Landolt et al. 2018). More recently the glutamatergic (AMPA receptor) system has been targeted for wake promotion. In experimental medicine type of conditions, these compounds have been shown to exert wake promotion as evidenced by longer latencies on the maintenance of wakefulness test or reduction of theta activity in the wake EEG (Boyle et al. 2012b; James et al. 2011; Iannone et al. 2010). At the same time little evidence for enhancement of cognition was observed. Furthermore, analyses of sleep following administration of compounds to promote wakefulness have documented ‘residual’ effects such as prolonged sleep latency or changes in sleep structure and the sleep EEG. Remarkably these effects were not observed after administration of modafinil (James et al. 2011; Bodenmann et al. 2012).
3 Circadian Rhythmicity: Sleep and Waking Performance
Circadian rhythmicity together with sleep homeostasis shapes the timing and structure of the sleep-wake cycle in young and older people and in men and women (Dijk and Czeisler 1995; Dijk et al. 1999; Wyatt et al. 1999; Santhi et al. 2016). Humans are a diurnal species, and in adult humans, sleep normally occurs at night and wakefulness during the day, although in modern industrialised societies with access to artificial light and the many social constraints it may be unclear where the day ends and the night begins (Skeldon et al. 2017; Walch et al. 2016). Sleep is not always monophasic, and daytime naps occur in normal and pathological conditions. Sleep timing can be measured against clock time, relative to the natural light-dark cycle and relative to preferred sleep timing, and imposed work schedules but also in relation to the many rhythmic circadian processes such as the hormones cortisol, melatonin, core body temperature, etc. (Dijk and Lockley 2002).
The timing and duration of sleep are among the most accessible characteristics of sleep, and dysregulation of these aspects may be related to circadian rhythm sleep disorders, insomnia, hypersomnia, etc. (see below). The two-process model of sleep regulation describes sleep timing as the result of the interaction of a circadian process and a homeostatic process (Daan et al. 1984; Borbély et al. 2016). The homeostatic aspect of sleep regulation relates to the contribution of sleep debt – as accrued during wakefulness and dissipating during sleep – to overall sleep propensity. The circadian process represents a clock-like intrinsically generated rhythm in sleep propensity. Sleep timing is also strongly influenced by social constraints such as work schedules and social obligations. Age-related and genetically determined differences in these processes and their interactions as well as psychological phenomena such as rumination and apprehension will shape individual differences in sleep-wake timing and the risk for sleep disturbances and sleep disorders (see Fig. 6).

Schematic representation of the interaction between circadian rhythmicity, sleep homeostasis and the light-dark cycle in the regulation of the sleep-wake cycle. Modified from Dijk and Lockley (2002)
3.1 Circadian Regulation of Sleep and Wakefulness
3.1.1 Circadian Rhythm of Sleep-Wake Propensity
The circadian process drives a rhythm in sleep-wake propensity and persists in the absence of sleep. The sleep-wake propensity rhythm is closely associated with the melatonin rhythm and the core body temperature rhythm. The waveform and timing of this sleep-wake propensity rhythm are at first glance somewhat paradoxical (Dijk and Czeisler 1994). Multiple protocols have established that in participants without sleep disturbances, the circadian drive for wakefulness increases during the waking day and reaches a maximum in the evening hours. The zone of maximum circadian drive for wakefulness, located just before the nocturnal (9–11 p.m.) increase in plasma melatonin concentrations, has been referred to as the wake maintenance zone (Strogatz et al. 1987). This drive for wakefulness then dissipates rapidly after the rise of melatonin (see Fig. 7).

Circadian and homeostatic regulation of sleep. (a) Association between wakefulness in sleep episode and the plasma melatonin rhythm. Modified from Dijk et al. (1997). (b) Sleep disruption (% wakefulness) as a function of hours since start of sleep episode and circadian phase. The two yellow trajectories represent a typical nocturnal and diurnal sleep episode. Modified from Dijk and Czeisler (1994)
The maximum circadian drive for sleep is located close to the nadir of the body temperature rhythm which in healthy participant occurs at around 4–6 a.m. and has been referred to as the sleep maintenance zone. When this circadian-driven sleep-wake propensity rhythm is dysfunctional, a consolidated sleep-wake cycle is no longer observed (Dijk and von Schantz 2005; Czeisler and Gooley 2007).
3.1.2 Circadian Contribution to Sleep Structure, Sleep Continuity and the Sleep EEG
The circadian pacemaker actively promotes REM sleep such that even when expressed as a percentage of total sleep time, REM sleep propensity is maximal at around 2 h after the nadir of the core body temperature rhythm (Dijk and Czeisler 1995). The density of rapid eye movement is highest when sleep occurs in the evening hours, i.e. during the wake maintenance zone (Khalsa et al. 2002). Sleep continuity or sleep consolidation is an important determinant of sleep quality. The circadian process has a strong impact on this characteristic of sleep such that the duration of awakenings is much shorter during the biological night than during the biological day (Dijk et al. 2001).
The circadian pacemaker also modulates the EEG within sleep such that it actively promotes sleep spindle activity at night. The duration of sleep spindles is longer, their frequency is lower, and their amplitude is higher when sleep occurs at night (Wei et al. 1999). It has been hypothesised that this circadian modulation of sleep spindles may contribute to sleep consolidation (Dijk et al. 1997).
Slow waves are to a lesser extent modulated by circadian phase such that slow-wave activity is slightly lower and their slope is shallower when sleep occurs at night. The circadian modulation of the sleep and wake EEG, relative to the sleep-related modulation, is dependent on topography such that it is largest in occipital and smallest in frontal derivations (Lazar et al. 2015).
3.1.3 Intrinsic Circadian Period and Sleep Timing
Basic circadian rhythm research has established that the timing of the circadian clock relative to the 24 h cycle is determined by the strength (i.e. amplitude) of the light-dark cycle and the intrinsic, largely genetically determined, period of the circadian clock. Assessment of the intrinsic period of the circadian clock requires specialised protocols in which light input to the clock is absent (as in blind people) or distributed evenly across the circadian cycle in protocols in which the sleep-wake cycle is scheduled to a period several hours shorter or longer than the intrinsic circadian period and light levels during waking are very low (Duffy et al. 2011). These protocols have shown that on average, the intrinsic period is 24.15 h with a standard deviation of 0.2 h. Longer intrinsic periods are associated with later timing of the sleep-wake cycle, body temperature cycle, melatonin cycle and an evening-type diurnal preference and longer time in bed during weekends (Wright et al. 2001; Duffy et al. 2011; Lazar et al. 2013). Conversely, shorter periods are associated with earlier sleep timing, morning preference, etc.
Circadian rhythmicity is present not only in the suprachiasmatic nucleus (SCN) which hosts the master pacemaker driving the circadian sleep-wake propensity rhythm but also in the periphery. Intrinsic periods assessed through circadian reporter systems in cell cultures of fibroblasts have a weak association with SCN periods (Hasan et al. 2012).
3.1.4 Light Input
Under normal conditions, the circadian process is synchronised to the 24 h cycle, primarily by light. Exposure to light in the evening delays (slows down) the clock, i.e. clock-timed events like the rise of melatonin will occur later. Light in the morning will advance (speed up) the clock, and events such as the peak of the cortisol rhythm will occur earlier (Duffy and Wright 2005). The human circadian timing system is very sensitive to light, and ordinary room light exerts approximately 50% of the maximum effect of light (Zeitzer et al. 2000; Santhi et al. 2012). The discovery of melanopsin-expressing light-sensitive ganglion cells has drawn attention to the spectral composition of light as a determinant of the circadian effectiveness of light (Lucas et al. 2014). Blue light has been shown to be very effective, and the increasing blue light content of our LED home lighting and the blue light content of light emitted by the screens of our gadgets are now considered to be a determinant of sleep timing (Czeisler 2013; Gringras et al. 2015).
The timing of the circadian clock is determined by the overall 24-h pattern of light exposure, and sufficient exposure to daylight is now jeopardised because we spend most of our day indoors. Low levels of exposure to daylight, especially in the winter, will increase the delaying effects of artificial evening light.
3.1.5 Circadian Regulation of Waking Function
The circadian clock also modulates waking function. Thus many aspects of performance are impaired when performance is assessed in the early morning hours, at around the core temperature nadir, whereas in the evening hours, performance is at its maximum, even when homeostatic sleep pressure at these circadian phases is identical (Dijk et al. 1992b; Wyatt et al. 1999). Importantly, the effects of circadian phase on waking function interact with homeostatic sleep pressure. Deterioration of performance in the early morning is severe when it is combined with high homeostatic sleep pressure, either caused by acute sleep loss (Dijk et al. 1992b; Wyatt et al. 1999, 2004) or chronic sleep loss (Cohen et al. 2010b). These experiments have also shown that during the wake maintenance zone, the brain appears to be resilient against the effects of sleep loss. Brain correlates of the circadian and the wake duration-dependent deterioration of vigilant attention have been documented (Muto et al. 2016).
Although circadian misalignment affects many aspects of performance, effects are strongest for sleepiness, vigilant attention and effort (Santhi et al. 2016) although others have emphasised that the circadian system may significantly modulate aspects of higher cognitive function as well (Burke et al. 2015b).
3.1.6 Circadian Aspects of Sleep Disorders
The role of the circadian timing system in sleep disorders is well recognised. Circadian rhythm sleep-wake disorders are a separate diagnostic category in both the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) and the International Classification of Sleep Disorders, Third Edition. These disorders include delayed, advanced, irregular, non-24-h, shift work and jet lag disorders. Causes of all of these disorders may be intrinsic, environmental or behavioural and social, e.g. work schedules. The contribution of the circadian timing system to sleep disturbances in shift work and jet lag is obvious and in essence is caused by inertia of the circadian pacemaker. The circadian clock takes longer to shift than the acute displacement of the sleep-wake schedule imposed by either shift work or rapid travel across time zones. As a consequence people attempt to sleep during the biological day and to be awake and work during the biological night.
3.1.7 External Factors: Modern Light Exposure Patterns as an Environmental and Lifestyle Factor Contributing to Sleep-Wake Disturbances
Reduced or inappropriate light exposure or changes in light input pathways to the clock are obvious putative mechanisms of circadian sleep-wake disorders. Indeed, the contribution of the circadian timing system to the non-24-h sleep-wake disorders often observed in the blind is now well documented with 63% of blind individuals displaying circadian rhythms which are not appropriately synchronised to the 24-h day (Flynn-Evans et al. 2014). Inadequate or inappropriate light exposure, such as excessive evening light, may contribute to delayed sleep and evidence for this is now emerging. Indeed exposure to ordinary room light in the evening has been shown to suppress melatonin and sleepiness, delay bedtime and prolong sleep latency (Gooley et al. 2011; Santhi et al. 2012). Abnormal light exposure patterns are observed in delayed sleep-wake disorders (Van der Maren et al. 2018; Wilson et al. 2018). Furthermore individual differences in the circadian sensitivity to light are emerging (Santhi et al. 2012) and increased sensitivity to light may be a characteristic of delayed sleep-wake phase syndrome (DSPS) (Watson et al. 2018).
A major roadblock in the full exploration of the contribution of light exposure to circadian sleep-wake disturbances is the lack of adequate and acceptable longitudinal sensing systems for the intensity and spectral composition of retinal light exposure. Nevertheless, some studies combining light exposure measurements and mathematical modelling thereof have already shown that light exposure is a good predictor of circadian phase (Woelders et al. 2017).
3.1.8 Intrinsic Factors: Genetic Variants and Differences in Circadian Period Contributing to Sleep-Wake Disturbances
3.1.8.1 Genetic Variants
Evidence for the involvement of circadian rhythmicity in sleep timing abnormalities may be derived from the various polymorphisms and mutations in genes which are part of the molecular machinery generating circadian rhythms. Variations in the period genes have been associated with familial advanced sleep phase syndrome and DSPS. Some of these mutations and polymorphisms have been shown to shorten or lengthen circadian period when introduced in animal or cell culture models (Shi et al. 2017). Maybe somewhat surprising, other clock gene variants do not seem to affect circadian period even though they associate with variations in sleep timing (see below). Many clock gene variants associate with variation in diurnal preference (Kalmbach et al. 2017; Jones et al. 2016; Lane et al. 2016), and extremes of diurnal preferences may translate to circadian sleep timing disorders. The effects of circadian variants to aspects of sleep other than its timing remain poorly characterised. It is of interest that several studies have now shown that circadian variants not only affect sleep timing but also sleep structure. For example, variants of the period genes are associated with differences in N3, i.e. slow-wave sleep (Hasan et al. 2014; Archer et al. 2018; Chang et al. 2016; Dijk and Archer 2010).
3.1.8.2 Circadian Period
Direct evidence for a contribution of intrinsic circadian factors such as abnormally long or short intrinsic circadian periods to circadian sleep-wake disorders is growing. Assessments of intrinsic circadian period in sleep disorders are rare, but it has been reported that circadian period is longer in DSPS and non-24-h sleep-wake disorder (Micic et al. 2016). It is often implied that developmental and age-related changes in circadian period contribute to late sleep timing in adolescence and early sleep timing in old age, but there is no solid evidence that the intrinsic circadian periods change with age (Dijk et al. 2000; Crowley et al. 2018; Skeldon et al. 2016). However, differences in circadian period as small as a few minutes may lead to substantial difference in entrained phase (Wright et al. 2005), and few studies with the statistical power to detect these small differences have been conducted. One example of small differences in circadian period concerns sex differences with circadian period in women being approximately 6 min shorter than in men (Duffy et al. 2011). This sex difference in intrinsic period may explain the earlier preferred timing of bedtime relative to clock time in women (Diurnal preference) and the earlier timing of the melatonin and core body temperature rhythm relative to sleep in women (Cain et al. 2010).
3.1.8.3 Circadian Phase
Indirect evidence for a contribution of the circadian timing system to variation in sleep timing stems from the observed associations between the timing of the melatonin rhythm and the timing of sleep in people without sleep timing complaints and in DSPS (Archer et al. 2008). Although this association implies that later timing of the melatonin rhythm may lead to later sleep timing, it cannot be excluded that the later sleep timing and associated light exposure lead to the delay of the melatonin rhythm. Recent data show that the intrinsic timing of the melatonin rhythm, as assessed by the dim light melatonin onset, is not delayed in almost half of DSPD patients (Murray et al. 2017).
The circadian timing system may also contribute to non-circadian sleep disorders. Insomnia with the prominent and persistent symptoms of difficulties initiating and maintaining sleep is in general not considered a circadian sleep disorder. Yet excessive strength of the evening wake maintenance zone or reduced circadian promotion of sleep during the night may contribute to these symptoms. Recently it was reported that in 10–22% of insomnia patients, the timing of sleep relative to the melatonin rhythm is abnormal such that sleep is attempted to be initiated at an early ‘melatonin time’ (Flynn-Evans et al. 2017).
3.1.9 Circadian Approaches to Treatment of Sleep-Wake Disturbances
In cases in which the cause of sleep-wake disturbances is clearly circadian, such as in jet lag disorder or non-24-h sleep-wake disorders in the blind, treatments are typically directed at the circadian timing system. Currently, abnormal timing of the circadian sleep-wake propensity rhythm may be corrected by either timed light exposure and light avoidance or administration of melatonin.
3.1.9.1 Light Treatment
Effects of time light exposure have been most extensively investigated in DSPS. Exposure to bright light in the morning, sometimes combined with instructions to avoid light in the evening, which theoretically should advance the sleep propensity rhythm, has been shown to be effective in DSPS (Richardson et al. 2018; Auger et al. 2015a, b). Optimisation of light treatment will require further quantitative understanding of the effects of light exposure patterns on the phase and amplitude of the circadian sleep-wake propensity rhythm. Current models for the effects of light do neither account for the spectral composition of light or the effects of prior light history on the sensitivity to light. Successful implementation of light therapy may also require assessment of circadian phase because effects of light depend on circadian phase, and, in some situation, like jet lag, circadian phase is not easily predicted. Light treatment also requires light delivery or light input manipulation systems that are easy to use and acceptable to users. Recent light treatment approaches have focused on reducing the blue light content of light to which the retina is exposed (Zerbini et al. 2018), and further development of methods by which the 24-h light exposure pattern, at the work place and at home, can be manipulated is a promising avenue for the treatment of some circadian rhythm sleep-wake disorders.
Development of novel therapeutics focusing on the light input pathway to the circadian system could target the anatomical and molecular pathways involved in entrainment.
3.1.9.2 Melatonin Therapy
Melatonin therapy has been successfully implemented in circadian rhythm sleep-wake disorders (Auger et al. 2015a, b) although the need for more research is recognised (Auger et al. 2015a, b). Melatonin is in the first instance an output of the circadian timing system. Its synthesis in the pineal is driven by sympathetic input, the rhythmicity of which is driven by the SCN such that in both nocturnal and diurnal species plasma melatonin concentrations are high during the biologically night and low during the biological day. This rhythm persists in constant darkness, but light at night suppresses melatonin. Melatonin administration leads to an increase in sleep propensity and shift of the sleep propensity rhythm, when it is administered when endogenous levels are low. This has been demonstrated in forced desynchrony protocols (Wyatt et al. 2006) and daytime sleep experiments (Rajaratnam et al. 2004) in participants without melatonin deficiency or sleep timing complaints. This effect is commonly referred to as the direct sleep-facilitating effect of melatonin. Melatonin can also induce a change in the timing of the endogenous phase of rhythms driven by the SCN. Some of these phase markers include the cortisol, core body temperature and endogenous melatonin rhythm (Rajaratnam et al. 2003). The direction of the shift depends on the endogenous circadian phase at which melatonin is administered (Lewy et al. 1998). Circadian rhythms will be advanced when melatonin is administered several hours before the endogenous rise of melatonin, although the optimal timing has not been explored in great detail. Evidence for melatonin’s effectiveness in delaying endogenous circadian rhythms is more limited. The phase-advancing effects of melatonin have been successfully exploited in several disorders such as DSPS (Sletten et al. 2018). Melatonin is also used to treat sleep disturbances in developmental disorders such as autism (Gringras et al. 2017). In all of these conditions, the largest effects are observed for latency to sleep onset. The effectiveness of melatonin in these conditions may be related to a combination of its direct sleep-facilitating and phase-shifting effects. Compared to allosteric modulators of the GABAA receptor, melatonin has very minor effects on slow-wave activity and EEG power spectra (Arbon et al. 2015).
Daily administration of melatonin can entrain non-synchronised rhythms, such as observed in the blind, to the 24 h day (Lockley et al. 2000). Melatonin treatment has also been advocated for the treatment of insomnia and in particular insomnia in older people (Lemoine and Zisapel 2012). The rationale for this approach is that endogenous melatonin levels may be too low in this particular patient group. The evidence for melatonin deficiency in insomnia is however rather limited although timing of melatonin may be abnormal in insomnia (see above).
Efforts have been made to optimise the dose of melatonin as well as the kinetics by, for example, slow-release preparations for oral or dermal delivery (Lemoine and Zisapel 2012; Aeschbach et al. 2009).
Effects of melatonin are mediated by M1 and M2 melatonin receptors which are abundant in the SCN but also in other brain areas. Melatonin receptor agonists have been developed for the treatment of insomnia (ramelteon) (Liu and Wang 2012) and non-24 h sleep-wake disorders (tasimelteon) (Lockley et al. 2015). Whether these agonists which have been approved are more effective than melatonin itself has not been investigated.
Further development of the melatonin-based treatment of sleep-wake disorders may benefit from new methods to assess endogenous circadian phase, which now requires collection of multiple samples under carefully controlled conditions. Several promising approaches based on analyses of the blood transcriptome have recently been developed (Laing et al. 2017; Wittenbrink et al. 2018).
3.1.10 Other Circadian Outputs and Novel Therapeutics for Sleep-Wake Disturbances
Further exploitation of the profound circadian influence on the sleep-wake propensity rhythm will require a better understanding of the neuroanatomical and molecular pathways by which the circadian system interacts with sleep executive systems generating sleep and wakefulness. An interesting example of interactions between sleep and circadian mechanisms relates to adenosinergic mechanisms. Caffeine, well known to affect sleep, also appears to affect the circadian timing system such that it delays phase, lengthens circadian period (Burke et al. 2015a) and affects light sensitivity of the circadian timing system (van Diepen et al. 2014). Another example relates to orexin. The orexin system is under circadian control but is also affected by sleep deprivation (Deboer et al. 2004) and is implicated in sleep-wake regulation. Orexin antagonists have been successfully developed for the treatment of insomnia (Herring et al. 2018).
4 Novel Therapeutics and Sleep-Wake Regulation: Outlook
4.1 Continued Need and Opportunities
Given the high prevalence of sleep-wake disturbances and the imperfection of current treatments of these disturbances, efforts to develop novel therapeutics will continue and are warranted. These efforts will be informed by a better understanding of the multifaceted nature of sleep-wake regulation and disturbances thereof. The need for novel therapeutics is likely to increase because of the continued high prevalence of shift work and associated sleep-wake disorders, demographic changes with more people living longer and the increase in the number of people living with dementia and associated disruption of sleep-wake cycles. The multidimensional phenomenology of sleep and wakefulness implies that the treatment of disorders of sleep and wakefulness, and the development of new sleep-wake therapeutics, continues to require the input from a variety of scientific disciplines ranging from molecular biology to clinical and cognitive psychology.
4.2 A More Comprehensive Phenomenology of Sleep and Sleep Disturbances
Understanding the subjective complaints about sleep quality or complaints of waking function attributed to poor sleep will remain a first point of entry for sleep medicine and the development of novel therapeutics. A better understanding of how sleep complaints relate to sleep and circadian physiology will require a more comprehensive phenomenology of healthy sleep and disturbed sleep. This extended phenomenology may open up new avenues for the development of novel therapeutics. Examples of this are already available. The complaint of not being able to fall asleep is common to insomnia and circadian rhythm sleep-wake disorders (delayed). The observation that insomnia patients experience difficulties sleeping irrespective of time of day, whereas in delayed or advanced sleep phase syndromes, there are times of day at which sleep-ability is normal, distinguishes the two disorders. Although this may now appear to be trivial, it is only the recognition of the importance of the circadian timing system in sleep-wake regulation that allowed for this distinction and development of specific treatments. Within this context it may be relevant to point out that in the treatment of circadian rhythm sleep-wake disorders, sleep remains the relevant outcome measure, but the target for the pharmacological and non-pharmacological therapeutics is far removed from classical sleep neurotransmitter systems. By contrast, in insomnia, neurotransmitter systems directly involved in sleep-wake regulation and associated processes such as arousal remain the target. Early on in these programmes, sleep physiology measures such as latency to sleep onset and wake after sleep onset are primary outcome measures, even though in at least a sizable fraction of insomnia patients, physiologically determined total sleep time is not severely abnormal (Vgontzas et al. 2013), and the complaint appears to be more related to the persistent mentation in the presence of physiological sleep. A better understanding of the sleep experience or the absence thereof and new EEG measures that better capture the sleep experience are needed. Efforts in this direction are already underway and can be guided by a simple question: what is the relation between sleep physiology and the sleep experience?
No doubt the discovery of other novel therapeutics will be parsimonious and not informed by any biased approach. Examples of current parsimoniously discovered therapeutics include the wake-promoting compound modafinil. It is only now that the important role of the dopaminergic system in wake (and sleep) regulation is recognised, providing a rational basis for modafinil’s effects.
4.3 Short-Term vs Long-Term Treatment and Consequences of Short and Long Sleep as a Risk Factor for Ill Health
It is understandable that approaches to the development of novel therapeutics are primarily targeting acute and ongoing complaints about sleep. Successful treatments of these complaints may not only resolve the acute complaints but also have long-term health implications. Epidemiological studies indeed show that, for example, the complaint of insomnia is associated with adverse physical and mental health outcomes such as depression in particular (Sivertsen et al. 2014). Population-based epidemiological studies also show that not only short sleep duration but also long self-reported sleep duration predict negative health outcomes (Jike et al. 2018). Whereas the sleep research field, in which the ‘sleep as a recovery process’ is the prevailing view, can easily envision pathways from short sleep to ill health, although even these remain poorly defined, the pathways from long sleep to ill health remain unclear. In fact, it currently remains uncertain whether long sleep is an early consequence of covert ill health or a cause. Whereas approaches to lengthen short sleep can include advocating lifestyle changes, no currently accepted policy for long sleep including excessive napping, which, for example, is highly prevalent in dementia, is available.
A major limitation of the currently available epidemiology is that the exposure assessment (sleep duration) is to the larger extent based on self-report. Limitations of self-reported sleep duration are considerable, in particular, because the reporting error appears to be correlated with health outcomes (Miller et al. 2015).
4.4 Symptom Based vs Disorder (Nosology) Based
Traditionally the development of therapeutics was nosology or disorder based, and the underlying assumption is that specific disorders have a specific aetiology which can be targeted. This approach may work well in cases in which the disease or disorder and its aetiology are clearly defined. However, many disorders may be rather heterogenous, symptoms may be common to several disorders, and disorders may be closely related. For example, insomnia patients may display several anxiety-related symptoms. In fact GWAS studies of insomnia show that the genetic associations with insomnia and anxiety overlap to a considerable extent (Hammerschlag et al. 2017). Furthermore, insomnia disorder may consist of various subtypes with different aetiologies (Blanken et al. 2019). Thus insomnia with objectively reduced TST and insomnia without objectively reduced TST may have a different aetiology, different adverse consequences, etc. One approach to the development of therapeutics may be to target symptoms, e.g. anxiety, rather than a disorder, e.g. insomnia, and then target those insomnia patients who specifically suffer from anxiety symptoms. Precise and comprehensive phenomenology is obviously key to such an approach.
4.5 Sleep as a Whole-Body Phenomenon
Quantification of sleep often focuses on the brain. The EEG is a major source of information about the sleep process, but sleep is obviously much more than changed in neuronal firing patterns. Changes affecting both the brain and the body include temperature, cardiovascular, endocrine and many other variables. How peripheral physiology contributes to the sleep process and its recovery value remains somewhat under-investigated. For example, skin, body and brain temperatures are affected by sleep, and as early as 1967, Monroe reported body temperature during sleep to be higher in poor sleepers compared to good sleepers (Monroe 1967). Indeed, manipulating peripheral and central thermoregulatory processes have been shown to improve sleep in, for example, ageing (Te Lindert and Van Someren 2018). There is extensive epidemiology pointing to associations between sleep duration and obesity, and effects of sleep manipulation on appetite- and glucose-regulating hormones have been reported. Yet, relatively little is known about the effects of obesity or food intake on sleep. Future approaches to the development of novel therapeutics may exploit some of these peripheral phenomena to improve sleep for the brain and the body.
4.6 Interactions: Circadian Rhythmicity and Sleep-Wake History
The separate contribution of circadian rhythmicity and sleep-wake history (sleep homeostasis) to sleep propensity and waking functions is well recognised. However, the most important determinant of both sleep propensity and waking function is the combined action of circadian rhythmicity and sleep homeostasis. Thus, waking performance at 6 a.m. close to the core body temperature nadir is not much impaired at all if the participant has had sufficient sleep prior to this time point. However, performance at this circadian phase is severely impaired when the participant is carrying an acute or chronic sleep debt. The implication for the development of novel therapeutics is that identification of the locus and mechanism of the interaction between circadian and homeostatic signals may offer new insights and targets. Some approaches are now emerging in preclinical research programmes in which local circadian clocks in arousal-related structures are manipulated and their effects on sleep-wake cycles are documented (Yu et al. 2014).
4.7 Monogenetic-Polygenetic, Monopharmacy vs Polypharmacy
Developing treatments of disorders of sleep and wakefulness necessarily implies the targeting of relevant circuits, receptor systems, etc. The ever more detailed description of the multitude of, for example, receptor subtypes offers opportunities for developing compounds with greater specificity for specific receptor subtypes. Likewise the ever more detailed description of the neuronal cell types regulating and contributing to specific aspects of sleep, e.g. sleep initiation vs REM sleep regulation, or EEG synchronisation. Such a specific targeted approach will be fruitful of specific receptor subtypes contributing to specific sleep disorders. This may be true in some cases, e.g. narcolepsy, even though even in this disorder, multiple neuromodulators have been implicated, but not in other cases. For example, it is unlikely that insomnia is caused by a deficiency in one particular GABAA receptor subtype. These states such as insomnia are likely to be associated with changes in constellations of biochemical signalling pathways. The implication is that a less specific treatment approach or drug development programme may be more effective.
4.8 The Sleep Environment
One defining aspect of sleep is partial disengagement from the environment, but the sleeper is not completely disconnected from its environment. Environmental influences on sleep and sleep disturbances may deserve more attention. Environmental variables that can be considered to be relevant include temperature, humidity, noise and light. With modern humans spending most of their time indoors, a closer look at the indoor environmental environment may be warranted. Sleep-wake cycles and their circadian regulation evolved in part as adaptation to environmental cycles related to the earth rotation around its axis. The light-dark cycle is one prominent example, but the natural darkness of the night is often hard to find in urban environments and the bedroom. Profound daily cycles in environmental temperature in the natural environment are to some extent mirrored in the circadian rhythm of body temperature which reaches a maximum during the later part of the day and a minimum close to dawn. Yet, temperature cycles in our home environments including bedrooms are very different, and little is known about the potential impact of environmental temperature cycles on sleep-wake cycles and their quality.
4.9 Large-Scale Sleep Studies in the Home Environment
New developments in electronics, electrode technologies and signal analysis have enabled new recording and analyses approaches which have revealed novel aspects of sleep phenomenology. New recording technologies and new scoring approaches based on machine learning techniques using reduced montages will soon enable large-scale sleep studies in the home environment (Peake et al. 2018; Mikkelsen et al. 2019).
References
Achermann P, Dijk DJ, Brunner DP, Borbély AA (1993) A model of human sleep homeostasis based on EEG slow-wave activity: quantitative comparison of data and simulations. Brain Res Bull 31(1–2):97–113
Achermann P, Rusterholz T, Durr R, Konig T, Tarokh L (2016) Global field synchronization reveals rapid eye movement sleep as most synchronized brain state in the human EEG. R Soc Open Sci 3(10):160201
Adam M, Rétey JV, Khatami R, Landolt HP (2006) Age-related changes in the time course of vigilant attention during 40 hours without sleep in men. Sleep 29(1):55–57
Aeschbach D, Cajochen C, Landolt H, Borbély AA (1996) Homeostatic sleep regulation in habitual short sleepers and long sleepers. Am J Phys 270(1 Pt 2):R41–R53
Aeschbach D, Postolache TT, Sher L, Matthews JR, Jackson MA, Wehr TA (2001) Evidence from the waking electroencephalogram that short sleepers live under higher homeostatic sleep pressure than long sleepers. Neuroscience 102(3):493–502
Aeschbach D, Sher L, Postolache TT, Matthews JR, Jackson MA, Wehr TA (2003) A longer biological night in long sleepers than in short sleepers. J Clin Endocrinol Metab 88(1):26–30
Aeschbach D, Lockyer BJ, Dijk DJ, Lockley SW, Nuwayser ES, Nichols LD, Czeisler CA (2009) Use of transdermal melatonin delivery to improve sleep maintenance during daytime. Clin Pharmacol Ther 86(4):378–382
Akerstedt T, Axelsson J, Lekander M, Orsini N, Kecklund G (2013) The daily variation in sleepiness and its relation to the preceding sleep episode – a prospective study across 42 days of normal living. J Sleep Res 22(3):258–265
Akerstedt T, Schwarz J, Gruber G, Lindberg E, Theorell-Haglow J (2016) The relation between polysomnography and subjective sleep and its dependence on age – poor sleep may become good sleep. J Sleep Res 25(5):565–570
Akerstedt T, Hallvig D, Kecklund G (2017) Normative data on the diurnal pattern of the Karolinska sleepiness scale ratings and its relation to age, sex, work, stress, sleep quality and sickness absence/illness in a large sample of daytime workers. J Sleep Res 26(5):559–566
Akerstedt T, Discacciati A, Miley-Akerstedt A, Westerlund H (2018) Aging and the change in fatigue and sleep – a longitudinal study across 8 years in three age groups. Front Psychol 9:234
Akerstedt T, Schwarz J, Gruber G, Theorell-Haglow J, Lindberg E (2019) Short sleep-poor sleep? A polysomnographic study in a large population-based sample of women. J Sleep Res 4:e12812
Arbon EL, Knurowska M, Dijk DJ (2015) Randomised clinical trial of the effects of prolonged-release melatonin, temazepam and zolpidem on slow-wave activity during sleep in healthy people. J Psychopharmacol 29(7):764–776
Archer SN, Viola AU, Kyriakopoulou V, von Schantz M, Dijk DJ (2008) Inter-individual differences in habitual sleep timing and entrained phase of endogenous circadian rhythms of BMAL1, PER2 and PER3 mRNA in human leukocytes. Sleep 31(5):608–617
Archer SN, Schmidt C, Vandewalle G, Dijk DJ (2018) Phenotyping of PER3 variants reveals widespread effects on circadian preference, sleep regulation, and health. Sleep Med Rev 40:109–126
Auger RR, Burgess HJ, Emens JS, Deriy LV, Sharkey KM (2015a) Do evidence-based treatments for circadian rhythm sleep-wake disorders make the GRADE? Updated guidelines point to need for more clinical research. J Clin Sleep Med 11(10):1079–1080
Auger RR, Burgess HJ, Emens JS, Deriy LV, Thomas SM, Sharkey KM (2015b) Clinical practice guideline for the treatment of intrinsic circadian rhythm sleep-wake disorders: advanced sleep-wake phase disorder (ASWPD), delayed sleep-wake phase disorder (DSWPD), non-24-hour sleep-wake rhythm disorder (N24SWD), and irregular sleep-wake rhythm disorder (ISWRD). An update for 2015: an American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med 11(10):1199–1236
Bachmann V, Klaus F, Bodenmann S, Schafer N, Brugger P, Huber S, Berger W, Landolt HP (2012) Functional ADA polymorphism increases sleep depth and reduces vigilant attention in humans. Cereb Cortex 22(4):962–970
Baglioni C, Regen W, Teghen A, Spiegelhalder K, Feige B, Nissen C, Riemann D (2014) Sleep changes in the disorder of insomnia: a meta-analysis of polysomnographic studies. Sleep Med Rev 18(3):195–213
Balkin TJ, Badia P (1988) Relationship between sleep inertia and sleepiness: cumulative effects of four nights of sleep disruption/restriction on performance following abrupt nocturnal awakenings. Biol Psychol 27(3):245–258
Balkin TJ, Braun AR, Wesensten NJ, Jeffries K, Varga M, Baldwin P, Belenky G, Herscovitch P (2002) The process of awakening: a PET study of regional brain activity patterns mediating the re-establishment of alertness and consciousness. Brain 125(Pt 10):2308–2319
Balkin TJ, Bliese PD, Belenky G, Sing H, Thorne DR, Thomas M, Redmond DP, Russo M, Wesensten NJ (2004) Comparative utility of instruments for monitoring sleepiness-related performance decrements in the operational environment. J Sleep Res 13(3):219–227
Baumann CR (2018) Clinical sleep-wake disorders I: focus on hypersomnias and movement disorders during sleep. Handb Exp Pharmacol. https://doi.org/10.1007/164_2018126
Beersma DG, Dijk DJ, Blok CG, Everhardus I (1990) REM sleep deprivation during 5 hours leads to an immediate REM sleep rebound and to suppression of non-REM sleep intensity. Electroencephalogr Clin Neurophysiol 76(2):114–122
Bei B, Allen NB, Nicholas CL, Dudgeon P, Murray G, Trinder J (2014) Actigraphy-assessed sleep during school and vacation periods: a naturalistic study of restricted and extended sleep opportunities in adolescents. J Sleep Res 23(1):107–117
Bei B, Manber R, Allen NB, Trinder J, Wiley JF (2017) Too long, too short, or too variable? Sleep intraindividual variability and its associations with perceived sleep quality and mood in adolescents during naturalistically unconstrained sleep. Sleep 40(2):zsw067
Berry RB, Brooks R, Gamaldo C, Harding SM, Lloyd RM, Quan SF, Troester MT, Vaughn BV (2017) AASM scoring manual updates for 2017 (version 2.4). J Clin Sleep Med 13(5):665–666
Bettica P, Squassante L, Groeger JA, Gennery B, Winsky-Sommerer R, Dijk DJ (2012) Differential effects of a dual orexin receptor antagonist (SB-649868) and zolpidem on sleep initiation and consolidation, SWS, REM sleep, and EEG power spectra in a model of situational insomnia. Neuropsychopharmacology 37(5):1224–1233
Blanken TF, Benjamins JS, Borsboom D, Vermunt JK, Paquola C, Ramautar J, Dekker K, Stoffers D, Wassing R, Wei Y, Van Someren EJW (2019) Insomnia disorder subtypes derived from life history and traits of affect and personality. Lancet Psychiatry 6(2):151–163
Bodenmann S, Hohoff C, Freitag C, Deckert J, Rétey JV, Bachmann V, Landolt HP (2012) Polymorphisms of ADORA2A modulate psychomotor vigilance and the effects of caffeine on neurobehavioural performance and sleep EEG after sleep deprivation. Br J Pharmacol 165(6):1904–1913
Borbély AA (1982) A two process model of sleep regulation. Hum Neurobiol 1(3):195–204
Borbély AA, Baumann F, Brandeis D, Strauch I, Lehmann D (1981) Sleep deprivation: effect on sleep stages and EEG power density in man. Electroencephalogr Clin Neurophysiol 51(5):483–495
Borbély AA, Daan S, Wirz-Justice A, Deboer T (2016) The two-process model of sleep regulation: a reappraisal. J Sleep Res 25(2):131–143
Boyle J, Groeger JA, Paska W, Cooper JA, Rockett C, Jones S, Gandhi P, Scott J, Atzori G, Dijk DJ (2012a) A method to assess the dissipation of the residual effects of hypnotics: eszopiclone versus zopiclone. J Clin Psychopharmacol 32(5):704–709
Boyle J, Stanley N, James LM, Wright N, Johnsen S, Arbon EL, Dijk DJ (2012b) Acute sleep deprivation: the effects of the AMPAKINE compound CX717 on human cognitive performance, alertness and recovery sleep. J Psychopharmacol 26(8):1047–1057
Brunner DP, Dijk DJ, Borbély AA (1990a) A quantitative analysis of phasic and tonic submental EMG activity in human sleep. Physiol Behav 48(5):741–748
Brunner DP, Dijk DJ, Tobler I, Borbély AA (1990b) Effect of partial sleep deprivation on sleep stages and EEG power spectra: evidence for non-REM and REM sleep homeostasis. Electroencephalogr Clin Neurophysiol 75(6):492–499
Brunner DP, Dijk DJ, Munch M, Borbély AA (1991) Effect of zolpidem on sleep and sleep EEG spectra in healthy young men. Psychopharmacology 104(1):1–5
Brunner DP, Dijk DJ, Borbély AA (1993) Repeated partial sleep deprivation progressively changes in EEG during sleep and wakefulness. Sleep 16(2):100–113
Burke TM, Markwald RR, McHill AW, Chinoy ED, Snider JA, Bessman SC, Jung CM, O’Neill JS, Wright KP Jr (2015a) Effects of caffeine on the human circadian clock in vivo and in vitro. Sci Transl Med 7(305):305ra146
Burke TM, Scheer F, Ronda JM, Czeisler CA, Wright KP Jr (2015b) Sleep inertia, sleep homeostatic and circadian influences on higher-order cognitive functions. J Sleep Res 24(4):364–371
Cain SW, Dennison CF, Zeitzer JM, Guzik AM, Khalsa SB, Santhi N, Schoen MW, Czeisler CA, Duffy JF (2010) Sex differences in phase angle of entrainment and melatonin amplitude in humans. J Biol Rhythm 25(4):288–296
Cajochen C, Brunner DP, Krauchi K, Graw P, Wirz-Justice A (1995) Power density in theta/alpha frequencies of the waking EEG progressively increases during sustained wakefulness. Sleep 18(10):890–894
Carrier J, Semba K, Deurveilher S, Drogos L, Cyr-Cronier J, Lord C, Sekerovick Z (2017) Sex differences in age-related changes in the sleep-wake cycle. Front Neuroendocrinol 47:66–85
Carskadon MA, Dement WC (1987) Daytime sleepiness: quantification of a behavioral state. Neurosci Biobehav Rev 11(3):307–317
Casali AG, Gosseries O, Rosanova M, Boly M, Sarasso S, Casali KR, Casarotto S, Bruno MA, Laureys S, Tononi G, Massimini M (2013) A theoretically based index of consciousness independent of sensory processing and behavior. Sci Transl Med 5(198):198ra105
Chang AM, Bjonnes AC, Aeschbach D, Buxton OM, Gooley JJ, Anderson C, Van Reen E, Cain SW, Czeisler CA, Duffy JF, Lockley SW, Shea SA, Scheer FA, Saxena R (2016) Circadian gene variants influence sleep and the sleep electroencephalogram in humans. Chronobiol Int 33(5):561–573
Clark I, Landolt HP (2017) Coffee, caffeine, and sleep: a systematic review of epidemiological studies and randomized controlled trials. Sleep Med Rev 31:70–78
Cohen DA, Wang W, Klerman EB, Rajaratnam SM (2010a) Ramelteon prior to a short evening nap impairs neurobehavioral performance for up to 12 hours after awakening. J Clin Sleep Med 6(6):565–571
Cohen DA, Wang W, Wyatt JK, Kronauer RE, Dijk DJ, Czeisler CA, Klerman EB (2010b) Uncovering residual effects of chronic sleep loss on human performance. Sci Transl Med 2(14):14ra13
Cross N, Terpening Z, Rogers NL, Duffy SL, Hickie IB, Lewis SJ, Naismith SL (2015) Napping in older people ‘at risk’ of dementia: relationships with depression, cognition, medical burden and sleep quality. J Sleep Res 24(5):494–502
Crowley SJ, Wolfson AR, Tarokh L, Carskadon MA (2018) An update on adolescent sleep: new evidence informing the perfect storm model. J Adolesc 67:55–65
Czeisler CA (2013) Perspective: casting light on sleep deficiency. Nature 497(7450):S13
Czeisler CA, Gooley JJ (2007) Sleep and circadian rhythms in humans. Cold Spring Harb Symp Quant Biol 72:579–597
Daan S, Beersma DG, Borbély AA (1984) Timing of human sleep: recovery process gated by a circadian pacemaker. Am J Phys 246(2 Pt 2):R161–R183
Deboer T, Overeem S, Visser NA, Duindam H, Frolich M, Lammers GJ, Meijer JH (2004) Convergence of circadian and sleep regulatory mechanisms on hypocretin-1. Neuroscience 129(3):727–732
Della Monica C, Johnsen S, Atzori G, Groeger JA, Dijk DJ (2018) Rapid eye movement sleep, sleep continuity and slow wave sleep as predictors of cognition, mood, and subjective sleep quality in healthy men and women, aged 20-84 years. Front Psych 9:255
Dijk DJ, Archer SN (2010) PERIOD3, circadian phenotypes, and sleep homeostasis. Sleep Med Rev 14(3):151–160
Dijk DJ, Beersma DG (1989) Effects of SWS deprivation on subsequent EEG power density and spontaneous sleep duration. Electroencephalogr Clin Neurophysiol 72(4):312–320
Dijk DJ, Czeisler CA (1994) Paradoxical timing of the circadian rhythm of sleep propensity serves to consolidate sleep and wakefulness in humans. Neurosci Lett 166(1):63–68
Dijk DJ, Czeisler CA (1995) Contribution of the circadian pacemaker and the sleep homeostat to sleep propensity, sleep structure, electroencephalographic slow waves, and sleep spindle activity in humans. J Neurosci 15(5 Pt 1):3526–3538
Dijk DJ, Lockley SW (2002) Integration of human sleep-wake regulation and circadian rhythmicity. J Appl Physiol 92(2):852–862
Dijk DJ, von Schantz M (2005) Timing and consolidation of human sleep, wakefulness, and performance by a symphony of oscillators. J Biol Rhythm 20(4):279–290
Dijk DJ, Beersma DG, Daan S (1987a) EEG power density during nap sleep: reflection of an hourglass measuring the duration of prior wakefulness. J Biol Rhythm 2(3):207–219
Dijk DJ, Beersma DG, Daan S, Bloem GM, Van den Hoofdakker RH (1987b) Quantitative analysis of the effects of slow wave sleep deprivation during the first 3 h of sleep on subsequent EEG power density. Eur Arch Psychiatry Neurol Sci 236(6):323–328
Dijk DJ, Beersma DG, Bloem GM (1989a) Sex differences in the sleep EEG of young adults: visual scoring and spectral analysis. Sleep 12(6):500–507
Dijk DJ, Beersma DG, Daan S, van den Hoofdakker RH (1989b) Effects of seganserin, a 5-HT2 antagonist, and temazepam on human sleep stages and EEG power spectra. Eur J Pharmacol 171(2–3):207–218
Dijk DJ, Brunner DP, Beersma DG, Borbély AA (1990a) Electroencephalogram power density and slow wave sleep as a function of prior waking and circadian phase. Sleep 13(5):430–440
Dijk DJ, Brunner DP, Borbély AA (1990b) Time course of EEG power density during long sleep in humans. Am J Phys 258(3 Pt 2):R650–R661
Dijk DJ, Brunner DP, Aeschbach D, Tobler I, Borbély AA (1992a) The effects of ethanol on human sleep EEG power spectra differ from those of benzodiazepine receptor agonists. Neuropsychopharmacology 7(3):225–232
Dijk DJ, Duffy JF, Czeisler CA (1992b) Circadian and sleep/wake dependent aspects of subjective alertness and cognitive performance. J Sleep Res 1(2):112–117
Dijk DJ, Hayes B, Czeisler CA (1993) Dynamics of electroencephalographic sleep spindles and slow wave activity in men: effect of sleep deprivation. Brain Res 626(1–2):190–199
Dijk DJ, Shanahan TL, Duffy JF, Ronda JM, Czeisler CA (1997) Variation of electroencephalographic activity during non-rapid eye movement and rapid eye movement sleep with phase of circadian melatonin rhythm in humans. J Physiol 505(Pt 3):851–858
Dijk DJ, Duffy JF, Riel E, Shanahan TL, Czeisler CA (1999) Ageing and the circadian and homeostatic regulation of human sleep during forced desynchrony of rest, melatonin and temperature rhythms. J Physiol 516(Pt 2):611–627
Dijk DJ, Duffy JF, Czeisler CA (2000) Contribution of circadian physiology and sleep homeostasis to age-related changes in human sleep. Chronobiol Int 17(3):285–311
Dijk DJ, Duffy JF, Czeisler CA (2001) Age-related increase in awakenings: impaired consolidation of nonREM sleep at all circadian phases. Sleep 24(5):565–577
Dijk DJ, Groeger JA, Stanley N, Deacon S (2010a) Age-related reduction in daytime sleep propensity and nocturnal slow wave sleep. Sleep 33(2):211–223
Dijk DJ, James LM, Peters S, Walsh JK, Deacon S (2010b) Sex differences and the effect of gaboxadol and zolpidem on EEG power spectra in NREM and REM sleep. J Psychopharmacol 24(11):1613–1618
Dijk DJ, Stanley N, Lundahl J, Groeger JA, Legters A, Trap Huusom AK, Deacon S (2012) Enhanced slow wave sleep and improved sleep maintenance after gaboxadol administration during seven nights of exposure to a traffic noise model of transient insomnia. J Psychopharmacol 26(8):1096–1107
Doherty A, Smith-Byrne K, Ferreira T, Holmes MV, Holmes C, Pulit SL, Lindgren CM (2018) GWAS identifies 14 loci for device-measured physical activity and sleep duration. Nat Commun 9(1):5257
Dornbierer D, Baur DM, Stucky B, Quednow BB, Krämer T, Seifritz E, Bosch OG, Landolt H-P (2019) Neurophysiological signature of gamma-hydroxybutyrate augmented sleep in healthy male volunteers may reflect biomimetic sleep enhancement: a randomized controlled trial. Neuropsychopharmacology. (in press). https://doi.org/10.1038/s41386-019-0382-z
Duffy JF, Wright KP Jr (2005) Entrainment of the human circadian system by light. J Biol Rhythm 20(4):326–338
Duffy JF, Cain SW, Chang AM, Phillips AJ, Munch MY, Gronfier C, Wyatt JK, Dijk DJ, Wright KP Jr, Czeisler CA (2011) Sex difference in the near-24-hour intrinsic period of the human circadian timing system. Proc Natl Acad Sci U S A 108(Suppl 3):15602–15608
Endo T, Roth C, Landolt HP, Werth E, Aeschbach D, Achermann P, Borbély AA (1998) Selective REM sleep deprivation in humans: effects on sleep and sleep EEG. Am J Phys 274(4 Pt 2):R1186–R1194
Ermis U, Krakow K, Voss U (2010) Arousal thresholds during human tonic and phasic REM sleep. J Sleep Res 19(3):400–406
Fink AM, Bronas UG, Calik MW (2018) Autonomic regulation during sleep and wakefulness: a review with implications for defining the pathophysiology of neurological disorders. Clin Auton Res 28(6):509–518
Flynn-Evans EE, Tabandeh H, Skene DJ, Lockley SW (2014) Circadian rhythm disorders and melatonin production in 127 blind women with and without light perception. J Biol Rhythm 29(3):215–224
Flynn-Evans EE, Shekleton JA, Miller B, Epstein LJ, Kirsch D, Brogna LA, Burke LM, Bremer E, Murray JM, Gehrman P, Rajaratnam SMW, Lockley SW (2017) Circadian phase and phase angle disorders in primary insomnia. Sleep 40(12):zsx163. https://doi.org/10.1093/sleep/zsx163
Frank MG, Heller HC (2019) The function(s) of sleep. Handb Exp Pharmacol. https://doi.org/10.1007/164_2018140
Gaggioni G, Maquet P, Schmidt C, Dijk DJ, Vandewalle G (2014) Neuroimaging, cognition, light and circadian rhythms. Front Syst Neurosci 8:126
Garcia-Molina G, Tsoneva T, Jasko J, Steele B, Aquino A, Baher K, Pastoor S, Pfundtner S, Ostrowski L, Miller B, Papas N, Riedner B, Tononi G, White DP (2018) Closed-loop system to enhance slow-wave activity. J Neural Eng 15(6):066018
Gooley JJ, Chamberlain K, Smith KA, Khalsa SB, Rajaratnam SM, Van Reen E, Zeitzer JM, Czeisler CA, Lockley SW (2011) Exposure to room light before bedtime suppresses melatonin onset and shortens melatonin duration in humans. J Clin Endocrinol Metab 96(3):E463–E472
Greneche J, Krieger J, Erhardt C, Bonnefond A, Eschenlauer A, Muzet A, Tassi P (2008) EEG spectral power and sleepiness during 24 h of sustained wakefulness in patients with obstructive sleep apnea syndrome. Clin Neurophysiol 119(2):418–428
Gringras P, Middleton B, Skene DJ, Revell VL (2015) Bigger, brighter, bluer-better? Current light-emitting devices – adverse sleep properties and preventative strategies. Front Public Health 3:233
Gringras P, Nir T, Breddy J, Frydman-Marom A, Findling RL (2017) Efficacy and safety of pediatric prolonged-release melatonin for insomnia in children with autism spectrum disorder. J Am Acad Child Adolesc Psychiatry 56(11):948–957.e4
Groeger JA, Stanley N, Deacon S, Dijk DJ (2014) Dissociating effects of global SWS disruption and healthy aging on waking performance and daytime sleepiness. Sleep 37(6):1127–1142
Hammerschlag AR, Stringer S, de Leeuw CA, Sniekers S, Taskesen E, Watanabe K, Blanken TF, Dekker K, Te Lindert BHW, Wassing R, Jonsdottir I, Thorleifsson G, Stefansson H, Gislason T, Berger K, Schormair B, Wellmann J, Winkelmann J, Stefansson K, Oexle K, Van Someren EJW, Posthuma D (2017) Genome-wide association analysis of insomnia complaints identifies risk genes and genetic overlap with psychiatric and metabolic traits. Nat Genet 49(11):1584–1592
Hanlon EC, Van Cauter E (2011) Quantification of sleep behavior and of its impact on the cross-talk between the brain and peripheral metabolism. Proc Natl Acad Sci U S A 108(Suppl 3):15609–15616
Hasan S, Santhi N, Lazar AS, Slak A, Lo J, von Schantz M, Archer SN, Johnston JD, Dijk DJ (2012) Assessment of circadian rhythms in humans: comparison of real-time fibroblast reporter imaging with plasma melatonin. FASEB J 26(6):2414–2423
Hasan S, van der Veen DR, Winsky-Sommerer R, Hogben A, Laing EE, Koentgen F, Dijk DJ, Archer SN (2014) A human sleep homeostasis phenotype in mice expressing a primate-specific PER3 variable-number tandem-repeat coding-region polymorphism. FASEB J 28(6):2441–2454
Herring WJ, Roth T, Krystal AD, Michelson D (2018) Orexin receptor antagonists for the treatment of insomnia and potential treatment of other neuropsychiatric indications. J Sleep Res 28(2):e12782
Hladky SB, Barrand MA (2017) Metabolite clearance during wakefulness and sleep. Handb Exp Pharmacol. https://doi.org/10.1007/164_2017_37
Holst SC, Landolt HP (2018) Sleep-wake neurochemistry. Sleep Med Clin 13(2):137–146
Holst SC, Bersagliere A, Bachmann V, Berger W, Achermann P, Landolt HP (2014) Dopaminergic role in regulating neurophysiological markers of sleep homeostasis in humans. J Neurosci 34(2):566–573
Horne JA, Moore VJ (1985) Sleep EEG effects of exercise with and without additional body cooling. Electroencephalogr Clin Neurophysiol 60(1):33–38
Horner RL, Peever JH (2017) Brain circuitry controlling sleep and wakefulness. Continuum (Minneap Minn) 23(4, Sleep Neurology):955–972
Huber R, Ghilardi MF, Massimini M, Tononi G (2004) Local sleep and learning. Nature 430(6995):78–81
Huber R, Ghilardi MF, Massimini M, Ferrarelli F, Riedner BA, Peterson MJ, Tononi G (2006) Arm immobilization causes cortical plastic changes and locally decreases sleep slow wave activity. Nat Neurosci 9(9):1169–1176
Iannone R, Palcza J, Renger JJ, Calder N, Cerchio K, Gottesdiener K, Hargreaves R, Dijk DJ, Boyle J, Murphy MG (2010) Acute alertness-promoting effects of a novel histamine subtype-3 receptor inverse agonist in healthy sleep-deprived male volunteers. Clin Pharmacol Ther 88(6):831–839
Irwin MR, Opp MR (2017) Sleep health: reciprocal regulation of sleep and innate immunity. Neuropsychopharmacology 42(1):129–155
Jacobson LH, Chen S, Mir S, Hoyer D (2017) Orexin OX2 receptor antagonists as sleep aids. Curr Top Behav Neurosci 33:105–136
James LM, Iannone R, Palcza J, Renger JJ, Calder N, Cerchio K, Gottesdiener K, Hargreaves R, Murphy MG, Boyle J, Dijk DJ (2011) Effect of a novel histamine subtype-3 receptor inverse agonist and modafinil on EEG power spectra during sleep deprivation and recovery sleep in male volunteers. Psychopharmacology 215(4):643–653
Jeppesen J, Otto M, Frederiksen Y, Hansen AK, Fedorova TD, Knudsen K, Nahimi A, Brooks DJ, Borghammer P, Sommerauer M (2018) Observations on muscle activity in REM sleep behavior disorder assessed with a semi-automated scoring algorithm. Clin Neurophysiol 129(3):541–547
Jike M, Itani O, Watanabe N, Buysse DJ, Kaneita Y (2018) Long sleep duration and health outcomes: a systematic review, meta-analysis and meta-regression. Sleep Med Rev 39:25–36
Johns MW (1991) A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 14(6):540–545
Jones SE, Tyrrell J, Wood AR, Beaumont RN, Ruth KS, Tuke MA, Yaghootkar H, Hu Y, Teder-Laving M, Hayward C, Roenneberg T, Wilson JF, Del Greco F, Hicks AA, Shin C, Yun CH, Lee SK, Metspalu A, Byrne EM, Gehrman PR, Tiemeier H, Allebrandt KV, Freathy RM, Murray A, Hinds DA, Frayling TM, Weedon MN (2016) Genome-wide association analyses in 128,266 individuals identifies new morningness and sleep duration loci. PLoS Genet 12(8):e1006125
Ju YS, Zangrilli MA, Finn MB, Fagan AM, Holtzman DM (2018) Obstructive sleep apnea treatment, slow wave activity, and amyloid-beta. Ann Neurol 85(2):291–295
Kalmbach DA, Schneider LD, Cheung J, Bertrand SJ, Kariharan T, Pack AI, Gehrman PR (2017) Genetic basis of chronotype in humans: insights from three landmark GWAS. Sleep 40(2):zsw048. https://doi.org/10.1093/sleep/zsw048
Kaplan KA, Hardas PP, Redline S, Zeitzer JM; Sleep Heart Health Study Research Group (2017a) Correlates of sleep quality in midlife and beyond: a machine learning analysis. Sleep Med 34:162–167
Kaplan KA, Hirshman J, Hernandez B, Stefanick ML, Hoffman AR, Redline S, Ancoli-Israel S, Stone K, Friedman L, Zeitzer JM, Osteoporotic Fractures in Men (MrOS), Study of Osteoporotic Fractures SOF Research Groups (2017b) When a gold standard isn’t so golden: lack of prediction of subjective sleep quality from sleep polysomnography. Biol Psychol 123:37–46
Kattler H, Dijk DJ, Borbély AA (1994) Effect of unilateral somatosensory stimulation prior to sleep on the sleep EEG in humans. J Sleep Res 3(3):159–164
Khalsa SB, Conroy DA, Duffy JF, Czeisler CA, Dijk DJ (2002) Sleep- and circadian-dependent modulation of REM density. J Sleep Res 11(1):53–59
Klerman EB, Dijk DJ (2005) Interindividual variation in sleep duration and its association with sleep debt in young adults. Sleep 28(10):1253–1259
Klerman EB, Dijk DJ (2008) Age-related reduction in the maximal capacity for sleep – implications for insomnia. Curr Biol 18(15):1118–1123
Klerman EB, Wang W, Duffy JF, Dijk DJ, Czeisler CA, Kronauer RE (2013) Survival analysis indicates that age-related decline in sleep continuity occurs exclusively during NREM sleep. Neurobiol Aging 34(1):309–318
Klinzing JG, Molle M, Weber F, Supp G, Hipp JF, Engel AK, Born J (2016) Spindle activity phase-locked to sleep slow oscillations. Neuroimage 134:607–616
Korkutata M, Saitoh T, Cherasse Y, Ioka S, Duo F, Qin R, Murakoshi N, Fujii S, Zhou X, Sugiyama F, Chen JF, Kumagai H, Nagase H, Lazarus M (2019) Enhancing endogenous adenosine A2A receptor signaling induces slow-wave sleep without affecting body temperature and cardiovascular function. Neuropharmacology 144:122–132
Kredlow MA, Capozzoli MC, Hearon BA, Calkins AW, Otto MW (2015) The effects of physical activity on sleep: a meta-analytic review. J Behav Med 38(3):427–449
Kyle SD, Sexton CE, Feige B, Luik AI, Lane J, Saxena R, Anderson SG, Bechtold DA, Dixon W, Little MA, Ray D, Riemann D, Espie CA, Rutter MK, Spiegelhalder K (2017) Sleep and cognitive performance: cross-sectional associations in the UK Biobank. Sleep Med 38:85–91
Lafortune M, Gagnon JF, Martin N, Latreille V, Dube J, Bouchard M, Bastien C, Carrier J (2014) Sleep spindles and rapid eye movement sleep as predictors of next morning cognitive performance in healthy middle-aged and older participants. J Sleep Res 23(2):159–167
Laing EE, Moller-Levet CS, Poh N, Santhi N, Archer SN, Dijk DJ (2017) Blood transcriptome based biomarkers for human circadian phase. Elife 6:e20214
Lancel M, Wetter TC, Steiger A, Mathias S (2001) Effect of the GABAA agonist gaboxadol on nocturnal sleep and hormone secretion in healthy elderly subjects. Am J Physiol Endocrinol Metab 281(1):E130–E137
Landolt HP, de Boer LP (2001) Effect of chronic phenelzine treatment on REM sleep: report of three patients. Neuropsychopharmacology 25(5 Suppl):S63–S67
Landolt HP, Wehrle R (2009) Antagonism of serotonergic 5-HT2A/2C receptors: mutual improvement of sleep, cognition and mood? Eur J Neurosci 29(9):1795–1809
Landolt HP, Moser S, Wieser HG, Borbély AA, Dijk DJ (1995) Intracranial temperature across 24-hour sleep-wake cycles in humans. Neuroreport 6(6):913–917
Landolt HP, Roth C, Dijk DJ, Borbély AA (1996) Late-afternoon ethanol intake affects nocturnal sleep and the sleep EEG in middle-aged men. J Clin Psychopharmacol 16(6):428–436
Landolt HP, Meier V, Burgess HJ, Finelli LA, Cattelin F, Achermann P, Borbély AA (1999) Serotonin-2 receptors and human sleep: effect of a selective antagonist on EEG power spectra. Neuropsychopharmacology 21(3):455–466
Landolt HP, Finelli LA, Roth C, Buck A, Achermann P, Borbély AA (2000) Zolpidem and sleep deprivation: different effect on EEG power spectra. J Sleep Res 9(2):175–183
Landolt HP, Rétey JV, Adam M (2012) Reduced neurobehavioral impairment from sleep deprivation in older adults: contribution of adenosinergic mechanisms. Front Neurol 3:62
Landolt HP, Holst SC, Valomon A (2018) Clinical and experimental human sleep-wake pharmacogenetics. Handb Exp Pharmacol. https://doi.org/10.1007/164_2018175
Lane JM, Vlasac I, Anderson SG, Kyle SD, Dixon WG, Bechtold DA, Gill S, Little MA, Luik A, Loudon A, Emsley R, Scheer FA, Lawlor DA, Redline S, Ray DW, Rutter MK, Saxena R (2016) Genome-wide association analysis identifies novel loci for chronotype in 100,420 individuals from the UK Biobank. Nat Commun 7:10889
Lankford DA, Corser BC, Zheng YP, Li Z, Snavely DB, Lines CR, Deacon S (2008) Effect of gaboxadol on sleep in adult and elderly patients with primary insomnia: results from two randomized, placebo-controlled, 30-night polysomnography studies. Sleep 31(10):1359–1370
Lazar AS, Santhi N, Hasan S, Lo JC, Johnston JD, Von Schantz M, Archer SN, Dijk DJ (2013) Circadian period and the timing of melatonin onset in men and women: predictors of sleep during the weekend and in the laboratory. J Sleep Res 22(2):155–159
Lazar AS, Lazar ZI, Dijk DJ (2015) Circadian regulation of slow waves in human sleep: topographical aspects. Neuroimage 116:123–134
Lazar ZI, Dijk DJ, Lazar AS (2018) Infraslow oscillations in human sleep spindle activity. J Neurosci Methods 316:22–34
Lecci S, Fernandez LM, Weber FD, Cardis R, Chatton JY, Born J, Luthi A (2017) Coordinated infraslow neural and cardiac oscillations mark fragility and offline periods in mammalian sleep. Sci Adv 3(2):e1602026
LeGates TA, Fernandez DC, Hattar S (2014) Light as a central modulator of circadian rhythms, sleep and affect. Nat Rev Neurosci 15(7):443–454
Lemoine P, Zisapel N (2012) Prolonged-release formulation of melatonin (Circadin) for the treatment of insomnia. Expert Opin Pharmacother 13(6):895–905
Lewy AJ, Bauer VK, Ahmed S, Thomas KH, Cutler NL, Singer CM, Moffit MT, Sack RL (1998) The human phase response curve (PRC) to melatonin is about 12 hours out of phase with the PRC to light. Chronobiol Int 15(1):71–83
Lim J, Dinges DF (2008) Sleep deprivation and vigilant attention. Ann N Y Acad Sci 1129:305–322
Liu J, Wang LN (2012) Ramelteon in the treatment of chronic insomnia: systematic review and meta-analysis. Int J Clin Pract 66(9):867–873
Lo JC, Groeger JA, Santhi N, Arbon EL, Lazar AS, Hasan S, von Schantz M, Archer SN, Dijk DJ (2012) Effects of partial and acute total sleep deprivation on performance across cognitive domains, individuals and circadian phase. PLoS One 7(9):e45987
Lockley SW, Skene DJ, James K, Thapan K, Wright J, Arendt J (2000) Melatonin administration can entrain the free-running circadian system of blind subjects. J Endocrinol 164(1):R1–R6
Lockley SW, Dressman MA, Licamele L, Xiao C, Fisher DM, Flynn-Evans EE, Hull JT, Torres R, Lavedan C, Polymeropoulos MH (2015) Tasimelteon for non-24-hour sleep-wake disorder in totally blind people (SET and RESET): two multicentre, randomised, double-masked, placebo-controlled phase 3 trials. Lancet 386(10005):1754–1764
Lowe CJ, Safati A, Hall PA (2017) The neurocognitive consequences of sleep restriction: a meta-analytic review. Neurosci Biobehav Rev 80:586–604
Lucas RJ, Peirson SN, Berson DM, Brown TM, Cooper HM, Czeisler CA, Figueiro MG, Gamlin PD, Lockley SW, O’Hagan JB, Price LL, Provencio I, Skene DJ, Brainard GC (2014) Measuring and using light in the melanopsin age. Trends Neurosci 37(1):1–9
Luppi PH, Fort P (2018) Neuroanatomical and neurochemical bases of vigilance states. Handb Exp Pharmacol. https://doi.org/10.1007/164_2017_84
Ma J, Dijk DJ, Svetnik V, Tymofyeyev Y, Ray S, Walsh JK, Deacon S (2011) EEG power spectra response to a 4-h phase advance and gaboxadol treatment in 822 men and women. J Clin Sleep Med 7(5):493–501A
Mander BA, Winer JR, Walker MP (2017) Sleep and human aging. Neuron 94(1):19–36
Mathias S, Steiger A, Lancel M (2001) The GABA(A) agonist gaboxadol improves the quality of post-nap sleep. Psychopharmacology 157(3):299–304
Maurer LF, Espie CA, Kyle SD (2018) How does sleep restriction therapy for insomnia work? A systematic review of mechanistic evidence and the introduction of the Triple-R model. Sleep Med Rev 42:127–138
McHill AW, Hull JT, Wang W, Czeisler CA, Klerman EB (2018) Chronic sleep curtailment, even without extended (>16-h) wakefulness, degrades human vigilance performance. Proc Natl Acad Sci U S A 115(23):6070–6075
McKillop LE, Vyazovskiy VV (2018) Sleep- and wake-like states in small networks in vivo and in vitro. Handb Exp Pharmacol. https://doi.org/10.1007/164_2018174
Melancon MO, Lorrain D, Dionne IJ (2015) Sleep depth and continuity before and after chronic exercise in older men: electrophysiological evidence. Physiol Behav 140:203–208
Micic G, Lovato N, Gradisar M, Burgess HJ, Ferguson SA, Lack L (2016) Circadian melatonin and temperature taus in delayed sleep-wake phase disorder and non-24-hour sleep-wake rhythm disorder patients: an ultradian constant routine study. J Biol Rhythm 31(4):387–405
Mikkelsen KB, Ebajemito JK, Bonmati-Carrion MA, Santhi N, Revell VL, Atzori G, Della Monica C, Debener S, Dijk DJ, Sterr A, de Vos M (2019) Machine-learning-derived sleep-wake staging from around-the-ear electroencephalogram outperforms manual scoring and actigraphy. J Sleep Res 28(2):e12786
Miller CB, Gordon CJ, Toubia L, Bartlett DJ, Grunstein RR, D’Rozario AL, Marshall NS (2015) Agreement between simple questions about sleep duration and sleep diaries in a large online survey. Sleep Health 1(2):133–137
Moller-Levet CS, Archer SN, Bucca G, Laing EE, Slak A, Kabiljo R, Lo JC, Santhi N, von Schantz M, Smith CP, Dijk DJ (2013) Effects of insufficient sleep on circadian rhythmicity and expression amplitude of the human blood transcriptome. Proc Natl Acad Sci U S A 110(12):E1132–E1141
Monroe LJ (1967) Psychological and physiological differences between good and poor sleepers. J Abnorm Psychol 72(3):255–264
Morris CJ, Aeschbach D, Scheer FA (2012) Circadian system, sleep and endocrinology. Mol Cell Endocrinol 349(1):91–104
Murray JM, Sletten TL, Magee M, Gordon C, Lovato N, Bartlett DJ, Kennaway DJ, Lack LC, Grunstein RR, Lockley SW, Rajaratnam SM; Delayed Sleep on Melatonin Study Group (2017) Prevalence of circadian misalignment and its association with depressive symptoms in delayed sleep phase disorder. Sleep 40(1):zsw002
Muto V, Jaspar M, Meyer C, Kusse C, Chellappa SL, Degueldre C, Balteau E, Shaffii-Le Bourdiec A, Luxen A, Middleton B, Archer SN, Phillips C, Collette F, Vandewalle G, Dijk DJ, Maquet P (2016) Local modulation of human brain responses by circadian rhythmicity and sleep debt. Science 353(6300):687–690
Newman RA, Kamimori GH, Wesensten NJ, Picchioni D, Balkin TJ (2013) Caffeine gum minimizes sleep inertia. Percept Mot Skills 116(1):280–293
O’Callaghan EK, Green EW, Franken P, Mongrain V (2018) Omics approaches in sleep-wake regulation. Handb Exp Pharmacol. https://doi.org/10.1007/164_2018125
Pachito DV, Eckeli AL, Desouky AS, Corbett MA, Partonen T, Rajaratnam SM, Riera R (2018) Workplace lighting for improving alertness and mood in daytime workers. Cochrane Database Syst Rev 3:CD012243
Peake JM, Kerr G, Sullivan JP (2018) A critical review of consumer wearables, mobile applications, and equipment for providing biofeedback, monitoring stress, and sleep in physically active populations. Front Physiol 9:743
Perrault AA, Khani A, Quairiaux C, Kompotis K, Franken P, Muhlethaler M, Schwartz S, Bayer L (2019) Whole-night continuous rocking entrains spontaneous neural oscillations with benefits for sleep and memory. Curr Biol 29(3):402–411.e3
Rajaratnam SM, Dijk DJ, Middleton B, Stone BM, Arendt J (2003) Melatonin phase-shifts human circadian rhythms with no evidence of changes in the duration of endogenous melatonin secretion or the 24-hour production of reproductive hormones. J Clin Endocrinol Metab 88(9):4303–4309
Rajaratnam SM, Middleton B, Stone BM, Arendt J, Dijk DJ (2004) Melatonin advances the circadian timing of EEG sleep and directly facilitates sleep without altering its duration in extended sleep opportunities in humans. J Physiol 561(Pt 1):339–351
Rasch B, Born J (2013) About sleep’s role in memory. Physiol Rev 93(2):681–766
Rhodes JA, Lane JM, Vlasac IM, Rutter MK, Czeisler C, Saxena R (2018) Association of DAT1 genetic variants with habitual sleep duration in the UK biobank. Sleep 42(1):zsy193
Richardson C, Cain N, Bartel K, Micic G, Maddock B, Gradisar M (2018) A randomised controlled trial of bright light therapy and morning activity for adolescents and young adults with Delayed Sleep-Wake Phase Disorder. Sleep Med 45:114–123
Riedner BA, Goldstein MR, Plante DT, Rumble ME, Ferrarelli F, Tononi G, Benca RM (2016) Regional patterns of elevated alpha and high-frequency electroencephalographic activity during nonrapid eye movement sleep in chronic insomnia: a pilot study. Sleep 39(4):801–812
Roenneberg T (2013) Chronobiology: the human sleep project. Nature 498(7455):427–428
Roth T, Lines C, Vandormael K, Ceesay P, Anderson D, Snavely D (2010) Effect of gaboxadol on patient-reported measures of sleep and waking function in patients with Primary Insomnia: results from two randomized, controlled, 3-month studies. J Clin Sleep Med 6(1):30–39
Rupp TL, Wesensten NJ, Balkin TJ (2012) Trait-like vulnerability to total and partial sleep loss. Sleep 35(8):1163–1172
Rusterholz T, Durr R, Achermann P (2010) Inter-individual differences in the dynamics of sleep homeostasis. Sleep 33(4):491–498
Santhi N, Thorne HC, van der Veen DR, Johnsen S, Mills SL, Hommes V, Schlangen LJ, Archer SN, Dijk DJ (2012) The spectral composition of evening light and individual differences in the suppression of melatonin and delay of sleep in humans. J Pineal Res 53(1):47–59
Santhi N, Groeger JA, Archer SN, Gimenez M, Schlangen LJ, Dijk DJ (2013) Morning sleep inertia in alertness and performance: effect of cognitive domain and white light conditions. PLoS One 8(11):e79688
Santhi N, Lazar AS, McCabe PJ, Lo JC, Groeger JA, Dijk DJ (2016) Sex differences in the circadian regulation of sleep and waking cognition in humans. Proc Natl Acad Sci U S A 113(19):E2730–E2739
Schwarz JFA, Akerstedt T, Lindberg E, Gruber G, Fischer H, Theorell-Haglow J (2017) Age affects sleep microstructure more than sleep macrostructure. J Sleep Res 26(3):277–287
Schwarz J, Axelsson J, Gerhardsson A, Tamm S, Fischer H, Kecklund G, Akerstedt T (2018) Mood impairment is stronger in young than in older adults after sleep deprivation. J Sleep Res 25:e12801. https://doi.org/10.1111/jsr.12801
Scullin MK, Bliwise DL (2015) Sleep, cognition, and normal aging: integrating a half century of multidisciplinary research. Perspect Psychol Sci 10(1):97–137
Shekari Soleimanloo S, White MJ, Garcia-Hansen V, Smith SS (2017) The effects of sleep loss on young drivers’ performance: a systematic review. PLoS One 12(8):e0184002
Shi G, Wu D, Ptacek LJ, Fu YH (2017) Human genetics and sleep behavior. Curr Opin Neurobiol 44:43–49
Siclari F, Baird B, Perogamvros L, Bernardi G, LaRocque JJ, Riedner B, Boly M, Postle BR, Tononi G (2017) The neural correlates of dreaming. Nat Neurosci 20(6):872–878
Sivertsen B, Lallukka T, Salo P, Pallesen S, Hysing M, Krokstad S, Simon O (2014) Insomnia as a risk factor for ill health: results from the large population-based prospective HUNT Study in Norway. J Sleep Res 23(2):124–132
Skeldon AC, Derks G, Dijk DJ (2016) Modelling changes in sleep timing and duration across the lifespan: changes in circadian rhythmicity or sleep homeostasis? Sleep Med Rev 28:96–107
Skeldon AC, Phillips AJ, Dijk DJ (2017) The effects of self-selected light-dark cycles and social constraints on human sleep and circadian timing: a modeling approach. Sci Rep 7:45158
Skorucak J, Arbon EL, Dijk DJ, Achermann P (2018) Response to chronic sleep restriction, extension, and subsequent total sleep deprivation in humans: adaptation or preserved sleep homeostasis? Sleep 41(7):zsy078
Sletten TL, Magee M, Murray JM, Gordon CJ, Lovato N, Kennaway DJ, Gwini SM, Bartlett DJ, Lockley SW, Lack LC, Grunstein RR, Rajaratnam SMW, Delayed Sleep on Melatonin (DelSoM) Study Group (2018) Efficacy of melatonin with behavioural sleep-wake scheduling for delayed sleep-wake phase disorder: a double-blind, randomised clinical trial. PLoS Med 15(6):e1002587
Strogatz SH, Kronauer RE, Czeisler CA (1987) Circadian pacemaker interferes with sleep onset at specific times each day: role in insomnia. Am J Phys 253(1 Pt 2):R172–R178
Sullivan SS, Kushida CA (2008) Multiple sleep latency test and maintenance of wakefulness test. Chest 134(4):854–861
Svetnik V, Snyder ES, Ma J, Tao P, Lines C, Herring WJ (2017) EEG spectral analysis of NREM sleep in a large sample of patients with insomnia and good sleepers: effects of age, sex and part of the night. J Sleep Res 26(1):92–104
Svetnik V, Snyder ES, Tao P, Scammell TE, Roth T, Lines C, Herring WJ (2018) Insight into reduction of wakefulness by suvorexant in patients with insomnia: analysis of wake bouts. Sleep 41(1):zsx178
Te Lindert BHW, Van Someren EJW (2018) Skin temperature, sleep, and vigilance. Handb Clin Neurol 156:353–365
Trachsel L, Dijk DJ, Brunner DP, Klene C, Borbély AA (1990) Effect of zopiclone and midazolam on sleep and EEG spectra in a phase-advanced sleep schedule. Neuropsychopharmacology 3(1):11–18
Urade Y (2017) Neurobiological basis of hypersomnia. Sleep Med Clin 12(3):265–277
Van Cauter E, Plat L, Scharf MB, Leproult R, Cespedes S, L’Hermite-Baleriaux M, Copinschi G (1997) Simultaneous stimulation of slow-wave sleep and growth hormone secretion by gamma-hydroxybutyrate in normal young men. J Clin Invest 100(3):745–753
Van der Maren S, Moderie C, Duclos C, Paquet J, Daneault V, Dumont M (2018) Daily profiles of light exposure and evening use of light-emitting devices in young adults complaining of a delayed sleep schedule. J Biol Rhythm 33(2):192–202
van Diepen HC, Lucassen EA, Yasenkov R, Groenen I, Ijzerman AP, Meijer JH, Deboer T (2014) Caffeine increases light responsiveness of the mouse circadian pacemaker. Eur J Neurosci 40(10):3504–3511
Van Dongen HP, Maislin G, Mullington JM, Dinges DF (2003) The cumulative cost of additional wakefulness: dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation. Sleep 26(2):117–126
Van Dongen HP, Baynard MD, Maislin G, Dinges DF (2004) Systematic interindividual differences in neurobehavioral impairment from sleep loss: evidence of trait-like differential vulnerability. Sleep 27(3):423–433
Vgontzas AN, Fernandez-Mendoza J, Liao D, Bixler EO (2013) Insomnia with objective short sleep duration: the most biologically severe phenotype of the disorder. Sleep Med Rev 17(4):241–254
Vienne J, Lecciso G, Constantinescu I, Schwartz S, Franken P, Heinzer R, Tafti M (2012) Differential effects of sodium oxybate and baclofen on EEG, sleep, neurobehavioral performance, and memory. Sleep 35(8):1071–1083
Viola AU, Archer SN, James LM, Groeger JA, Lo JC, Skene DJ, von Schantz M, Dijk DJ (2007) PER3 polymorphism predicts sleep structure and waking performance. Curr Biol 17(7):613–618
Viola AU, James LM, Archer SN, Dijk DJ (2008a) PER3 polymorphism and cardiac autonomic control: effects of sleep debt and circadian phase. Am J Physiol Heart Circ Physiol 295(5):H2156–H2163
Viola AU, James LM, Schlangen LJ, Dijk DJ (2008b) Blue-enriched white light in the workplace improves self-reported alertness, performance and sleep quality. Scand J Work Environ Health 34(4):297–306
Walch OJ, Cochran A, Forger DB (2016) A global quantification of “normal” sleep schedules using smartphone data. Sci Adv 2(5):e1501705
Walsh JK, Deacon S, Dijk DJ, Lundahl J (2007) The selective extrasynaptic GABAA agonist, gaboxadol, improves traditional hypnotic efficacy measures and enhances slow wave activity in a model of transient insomnia. Sleep 30(5):593–602
Walsh JK, Snyder E, Hall J, Randazzo AC, Griffin K, Groeger J, Eisenstein R, Feren SD, Dickey P, Schweitzer PK (2008) Slow wave sleep enhancement with gaboxadol reduces daytime sleepiness during sleep restriction. Sleep 31(5):659–672
Walsh JK, Hall-Porter JM, Griffin KS, Dodson ER, Forst EH, Curry DT, Eisenstein RD, Schweitzer PK (2010) Enhancing slow wave sleep with sodium oxybate reduces the behavioral and physiological impact of sleep loss. Sleep 33(9):1217–1225
Watson LA, Phillips AJK, Hosken IT, McGlashan EM, Anderson C, Lack LC, Lockley SW, Rajaratnam SMW, Cain SW (2018) Increased sensitivity of the circadian system to light in delayed sleep-wake phase disorder. J Physiol 596(24):6249–6261
Wei HG, Riel E, Czeisler CA, Dijk DJ (1999) Attenuated amplitude of circadian and sleep-dependent modulation of electroencephalographic sleep spindle characteristics in elderly human subjects. Neurosci Lett 260(1):29–32
Werth E, Dijk DJ, Achermann P, Borbély AA (1996) Dynamics of the sleep EEG after an early evening nap: experimental data and simulations. Am J Phys 271(3 Pt 2):R501–R510
Wilckens KA, Ferrarelli F, Walker MP, Buysse DJ (2018) Slow-wave activity enhancement to improve cognition. Trends Neurosci 41(7):470–482
Wild CJ, Nichols ES, Battista ME, Stojanoski B, Owen AM (2018) Dissociable effects of self-reported daily sleep duration on high-level cognitive abilities. Sleep 41(12):zsy182
Wilson J t, Reid KJ, Braun RI, Abbott SM, Zee PC (2018) Habitual light exposure relative to circadian timing in delayed sleep-wake phase disorder. Sleep 41(11):zsy166
Winsky-Sommerer R, de Oliveira P, Loomis S, Wafford K, Dijk DJ, Gilmour G (2018) Disturbances of sleep quality, timing and structure and their relationship with other neuropsychiatric symptoms in Alzheimer’s disease and schizophrenia: insights from studies in patient populations and animal models. Neurosci Biobehav Rev 97:112–137
Wisden W, Yu X, Franks NP (2017) GABA receptors and the pharmacology of sleep. Handb Exp Pharmacol. https://doi.org/10.1007/164_2017_56
Wittenbrink N, Ananthasubramaniam B, Munch M, Koller B, Maier B, Weschke C, Bes F, de Zeeuw J, Nowozin C, Wahnschaffe A, Wisniewski S, Zaleska M, Bartok O, Ashwal-Fluss R, Lammert H, Herzel H, Hummel M, Kadener S, Kunz D, Kramer A (2018) High-accuracy determination of internal circadian time from a single blood sample. J Clin Invest 128(9):3826–3839
Woelders T, Beersma DGM, Gordijn MCM, Hut RA, Wams EJ (2017) Daily light exposure patterns reveal phase and period of the human circadian clock. J Biol Rhythm 32(3):274–286
Wright KP Jr, Hughes RJ, Kronauer RE, Dijk DJ, Czeisler CA (2001) Intrinsic near-24-h pacemaker period determines limits of circadian entrainment to a weak synchronizer in humans. Proc Natl Acad Sci U S A 98(24):14027–14032
Wright KP Jr, Gronfier C, Duffy JF, Czeisler CA (2005) Intrinsic period and light intensity determine the phase relationship between melatonin and sleep in humans. J Biol Rhythm 20(2):168–177
Wyatt JK, Ritz-De Cecco A, Czeisler CA, Dijk DJ (1999) Circadian temperature and melatonin rhythms, sleep, and neurobehavioral function in humans living on a 20-h day. Am J Phys 277(4 Pt 2):R1152–R1163
Wyatt JK, Cajochen C, Ritz-De Cecco A, Czeisler CA, Dijk DJ (2004) Low-dose repeated caffeine administration for circadian-phase-dependent performance degradation during extended wakefulness. Sleep 27(3):374–381
Wyatt JK, Dijk DJ, Ritz-de Cecco A, Ronda JM, Czeisler CA (2006) Sleep-facilitating effect of exogenous melatonin in healthy young men and women is circadian-phase dependent. Sleep 29(5):609–618
Yang H, Haack M, Dang R, Gautam S, Simpson NS, Mullington JM (2018) Heart rate variability rebound following exposure to persistent and repetitive sleep restriction. Sleep 42(2):zsy226
Yu X, Zecharia A, Zhang Z, Yang Q, Yustos R, Jager P, Vyssotski AL, Maywood ES, Chesham JE, Ma Y, Brickley SG, Hastings MH, Franks NP, Wisden W (2014) Circadian factor BMAL1 in histaminergic neurons regulates sleep architecture. Curr Biol 24(23):2838–2844
Yu X, Franks NP, Wisden W (2018) Sleep and sedative states induced by targeting the histamine and noradrenergic systems. Front Neural Circuits 12:4
Zant JC, Kim T, Prokai L, Szarka S, McNally J, McKenna JT, Shukla C, Yang C, Kalinchuk AV, McCarley RW, Brown RE, Basheer R (2016) Cholinergic neurons in the basal forebrain promote wakefulness by actions on neighboring non-cholinergic neurons: an opto-dialysis study. J Neurosci 36(6):2057–2067
Zeitzer JM, Dijk DJ, Kronauer R, Brown E, Czeisler C (2000) Sensitivity of the human circadian pacemaker to nocturnal light: melatonin phase resetting and suppression. J Physiol 526(Pt 3):695–702
Zerbini G, Kantermann T, Merrow M (2018) Strategies to decrease social jetlag: reducing evening blue light advances sleep and melatonin. Eur J Neurosci. https://doi.org/10.1111/ejn.14293
Zitting KM, Munch MY, Cain SW, Wang W, Wong A, Ronda JM, Aeschbach D, Czeisler CA, Duffy JF (2018) Young adults are more vulnerable to chronic sleep deficiency and recurrent circadian disruption than older adults. Sci Rep 8(1):11052
Acknowledgements
The authors thank Professors Alexander Borbély and Peter Achermann for comments on the manuscript.
Conflict of Interest
DJD has received research funding and acted as a consultant for various pharmaceutical companies.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2019 The Author(s)
About this chapter

Cite this chapter
Dijk, DJ., Landolt, HP. (2019). Sleep Physiology, Circadian Rhythms, Waking Performance and the Development of Sleep-Wake Therapeutics. In: Landolt, HP., Dijk, DJ. (eds) Sleep-Wake Neurobiology and Pharmacology . Handbook of Experimental Pharmacology, vol 253. Springer, Cham. https://doi.org/10.1007/164_2019_243
Download citation
DOI: https://doi.org/10.1007/164_2019_243
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-11270-7
Online ISBN: 978-3-030-11272-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)