
Abstract
Besides operative procedures (e.g., necrosectomies, skin grafting), conservative treatments of thermal injuries are increasingly important. wIRA as an additional therapy for burns, scalds, and chemically induced injuries and for treating severe skin reactions (e.g., toxic epidermal necrolysis) is used in our clinic on a daily basis. The most successful therapy involves 3–4 irradiations/30 min/day. Therefore, patients with superficial partial-thickness burns are treated with topical polyhexanide ointment and wIRA 2–4 days after the accident. In these cases, we see a quick wound-drying and a rapid re-epithelialization of the skin. The approach in deep partial-thickness burns depends on whether surgical procedures must be postponed due to poor general conditions. In these patients, preservation of the wound perfusion in regions that are not fully damaged is intended, avoiding extensive necrosectomies.
Although third-degree burns are dry and do not require wIRA irradiation, it can be used for adjacent regions with minor degree burns. Preliminary in vitro data suggest a wIRA-induced migration of adipose-derived stem cells.
Postoperatively, wIRA is used on areas transplanted with split-thickness skin grafts. After removal of the tie-over bolsters, wIRA is applied 3–4 times/20–30 min/day. The grafts exhibit a faster epithelialization of the fenestrated spots, and postoperative infections seem to be less frequent.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The treatment of thermal injuries is challenging and is an area of significant, clinical need. Early operative interventions which reduce the burden of skin necrosis and the related morbidity are favored by most patients [1]. In some patients, early necrosectomy is not possible due to compromised general condition, whereas in others, burn wounds need more postoperative care. For these cases, conservative treatment options are on the rise to provide an ideal environment for wound healing, preoperatively as well as postoperatively.
In this context, the therapeutic potential of water-filtrated infrared-A irradiation (wIRA irradiation) in different surgical disciplines is well known [2, 3]. We use wIRA irradiation as additional therapy for burns, scalds, and chemically induced injuries as well as for treating patients with severe skin reactions such as toxic epidermal necrolysis (TEN) on a daily basis. This chapter provides an overview of our experience treating various thermal wound types with wIRA irradiation.
2 Pathophysiology of Thermal Injuries
Thermal injuries can derive from heat, hot fluids or steam, chemical irritants, electrical trauma, or cold. Severe skin reactions such as toxic epidermal necrolysis (TEN) can also be included in this framework. The skin, which consists of the epidermis and dermis, is affected by heat. An increased skin temperature of up to 52 °C can be tolerated for a short period due to evaporation. However, if the temperature exceeds 69 °C for more than 1 s, cells of the skin are irreversibly damaged, with necrosis, with epidermolysis being the consequence [4]. A concept originally presented by Jackson in 1953 is still valid for the explanation of burn wound stages [5]. The center of a thermal wound shows a coagulation-related necrosis, whereas encircled areas present stasis with a mixture of vital and dead cells, constricted vessels, and ischemia. This area can be affected both positively and negatively and is at high risk of becoming necrotic if not treated meticulously. The outer, third zone shows a red appearance due to vasodilatation and is primarily not in danger of necrosis.
2.1 First-Degree Burns
First-degree burns appear as an erythema and are painful. There is no blistering, and the redness is caused by vasodilatation. A common trigger is a prolonged exposure to sunlight which damages the epidermis.
2.2 Second-Degree Burns
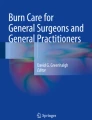
Second-degree burns are divided into superficial partial-thickness and deep partial-thickness burns, both associated with blistering of the skin due to epidermolysis and damage of several areas of the dermis. Whereas superficial partial-thickness burns primarily comprise vital dermis and are very painful, deep partial-thickness burns are characterized by a more injured dermis with a prolonged re-capillarization and less pain (Fig. 15.1).

Hand with both superficial and deep partial-thickness burn wounds
2.3 Third-Degree Burns
In third-degree burns, all skin layers are harmed and necrosis can extend to the muscles. There is no blistering, and wounds have a yellowish leather-like appearance (Fig. 15.2) which have to be treated surgically.

Hand with third-degree burn wounds
3 wIRA Irradiation in Thermal Injuries
3.1 Effects of wIRA Irradiation on the Skin
Several effects of wIRA irradiation on the skin have been reported [3]. These include the following reactions:
-
increase in tissue temperature;
-
improvement of tissue perfusion (blood flow); and
-
increase in tissue oxygen partial pressure.
Blood flow and oxygen partial pressure in wounds are key features for a successful healing process. Cell proliferation and synthesis of proteins require energy that greatly depends to a major extent on the presence of oxygen [6]. Hypoxic conditions additionally decrease the capability of leukocytes to kill bacteria [7]. These problems are mostly linked to a compromised microcirculation [8]. Microcirculatory disturbances negatively affect wound healing because all above-mentioned key factors are decisively dependent on adequate tissue perfusion.
Reduced inflammatory reactions via modulation of the immune system have also been described. A reduced bacterial colonization in infectious wounds is noticeable in the clinical setting and evidence suggests that wIRA irradiation impairs bacterial colonization [9, 10].
3.2 wIRA Application in Thermal Wounds
Although first-degree burns can be treated with wIRA irradiation, such patients are most likely outpatients and are not necessarily hospitalized. wIRA irradiation therefore is primarily used for treating hospitalized patients with second- and third-degree thermal injuries, patients with frostbites, and in particular patients with infectious thermal wounds.
Patients with superficial partial-thickness burns are treated with topical polyhexanide ointment and wIRA irradiation 2–4 days after injuries. In these cases, we see quick-drying wounds with a fast-progressing re-epithelialization of the skin. After the onset of epithelialization, dexpanthenol-containing fatty ointments are applied to the skin after wIRA irradiation to further support wound healing [11].
The approach in deep partial-thickness burns is slightly different but can have an impact on the dimension of surgical procedures. In patients with poor general condition or multiorgan failure, it is sometimes necessary to postpone surgical procedures in order to stabilize patients with complex treatments on intensive care burn units. In these patients, we intend to preserve the perfusion of wound regions, not fully damaged according to Zone II [5], so that less extensive necrosectomies are necessary, and the risk for bacterial infections is reduced.
If patients are in good clinical condition and surgery can be performed safely, wIRA irradiation is applied preoperatively with the same intention as mentioned above. Postoperatively, wIRA is used for re-epithelialization of split-thickness skin graft donor sites [12].
Due to the capability of the wIRA irradiation to penetrate skin (and other materials), we also started to irradiate tie-over-bolsters in order to support the healing process of split-thickness grafts in the first 5 days after transplantation.
Although third-degree burns are usually dry and do not require wIRA irradiation, it can be used for the adjacent regions with minor degree burns.
The protocol used in this study administers 3–4 irradiation sessions for 30 min/day each, with the distance between the wIRA-radiator exit and targeted body region being set at 30 to 40 cm. Postoperatively, radiators are used for areas that were transplanted with split-thickness skin grafts. After removal of tie-over bolsters, irradiation is applied 3–4 times per day for 20–30 min each session. Treated grafts show a faster epithelialization of the fenestrated spots.
Frostbites are rare and primarily seen in homeless persons in regions with cold winters or in extreme athletes. Cell damage arises due to protein denaturation, dehydration, or formation of ice crystals. Endothelial damage might still continue even if the impact of cold can be stopped due to reperfusion injury (Fig. 15.3). Late ischemia with vasoconstriction and thrombosis impairs microcirculation with consecutive necrosis. Among other therapies, we also apply wIRA irradiation in these patients, albeit with mixed results.

Right: severe frostbites of the fingers. Left: Documentation with FLIR ONE thermography showing the colder parts
In this context, other severe skin diseases such as toxic epidermal necrolysis are also treated. Here, large wound areas often require extended logistics and medical armamentarium of a specialized burn unit. Initial results appear promising; however, the rarity of these skin diseases impedes systemic analyses.
Although we have not yet been able to determine any significant reduction in the requirement for pain medication, as postulated earlier [13, 14], most patients report an enjoyable and comfortable warmth and a pleasant sense of relaxation during the application of wIRA.
4 Outlook to Further Research
Our preliminary in vitro data also show that wIRA irradiation induces the migration of adipose-derived stromal cells (ASCs). In scratch assays simulating wounds in a cell monolayer, ASCs lead to a faster wound closure after wIRA application compared to untreated or heat-treated controls. Further research is needed to understand the molecular mechanisms that are induced or mitigated/inhibited by wIRA irradiation.
References
Ong YS, Samuel M, Song C. Meta-analysis of early excision of burns. Burns. 2006;32(2):145–50.
Winkel R, Hoffmann G, Hoffmann R. Water-filtered infrared-A (wIRA) promotes wound healing. Chirurg. 2014;85(11):980–92.
Hoffmann G, Hartel M, Mercer JB. Heat for wounds - water-filtered infrared-A (wIRA) for wound healing - a review. Ger Med Sci. 2016;14:Doc08.
Herndon DN. Total burn care. 5th ed. Amsterdam: Elsevier; 2017.
Jackson DM. The diagnosis of the depth of burning. Br J Surg. 1953;40(164):588–96.
Schreml S, Szeimies RM, Prantl L, et al. Oxygen in acute and chronic wound healing. Br J Dermatol. 2010;163(2):257–68.
Allen DB, Maguire JJ, Mahdavian M, et al. Wound hypoxia and acidosis limit neutrophil bacterial killing mechanisms. Arch Surg. 1997;132(9):991–6.
Sorg H, Tilkorn DJ, Mirastschijski U, et al. Panta rhei: neovascularization, angiogenesis and nutritive perfusion in wound healing. Eur Surg Res. 2018;59(3–4):232–41.
Daeschlein G, Alborova J, Patzelt A, et al. Kinetics of physiological skin flora in a suction blister wound model on healthy subjects after treatment with water-filtered infrared-A radiation. Skin Pharmacol Physiol. 2012;25(2):73–7.
Kuratli J, Borel N. Perspective: water-filtered infrared-A-radiation (wIRA) - novel treatment options for chlamydial infections? Front Microbiol. 2019;10:1053.
Gorski J, Proksch E, Baron JM, et al. Dexpanthenol in wound healing after medical and cosmetic interventions (Postprocedure wound healing). Pharmaceuticals (Basel). 2020;13:7.
Aljasir A, Pierson T, Hoffmann G, Menke H. Management of donor site infections in split-thickness skin graft with water-filtered infrared-A (wIRA). GMS Interdiscip Plast Reconstr Surg DGPW. 2018;7:Doc03.
von Felbert V, Schumann H, Mercer JB, et al. Therapy of chronic wounds with water-filtered infrared-A (wIRA). GMS Krankenhhyg Interdiszip. 2008;2(2):Doc52.
Hartel M, Hoffmann G, Wente MN, et al. Randomized clinical trial of the influence of local water-filtered infrared A irradiation on wound healing after abdominal surgery. Br J Surg. 2006;93(8):952–60.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2022 The Author(s)
About this chapter

Cite this chapter
Bingoel, A.S., Strauss, S., Vogt, P.M. (2022). Clinical Application of wIRA Irradiation in Burn Wounds. In: Vaupel, P. (eds) Water-filtered Infrared A (wIRA) Irradiation. Springer, Cham. https://doi.org/10.1007/978-3-030-92880-3_15
Download citation
DOI: https://doi.org/10.1007/978-3-030-92880-3_15
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-92879-7
Online ISBN: 978-3-030-92880-3
eBook Packages: MedicineMedicine (R0)