
Abstract
Tuberculosis (TB) is an important zoonotic disease caused by infection with Mycobacterium tuberculosis (Mtb) complex and has a significant impact on public health. Animal models are suitable tools to mimic the clinical symptoms observed in human TB and provide an opportunity to understand immune responses to infection and the pathophysiology and pathogenesis of TB. In this chapter, we summarize the animal models that are used in Mtb research, including common models such as the mouse, rat, guinea pig, non-human primates, rabbit, cattle and zebrafish, as well as discuss some newly established animal models.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
In 2020, an estimated ten million people fell ill with tuberculosis (TB) worldwide, and approximately 1.5 million people died from TB. TB is the second leading infectious killer after COVID-19 (above HIV/AIDS) [1]. In recent years, the global incidence of TB has increased further due to antibiotic abuse and the prevalence of HIV, both of which aggravate TB control [2]. Therefore, the development of anti-TB drugs and vaccines has become urgent, to control TB spread. With the development of modern molecular sequencing technology, more information about the biological characteristics of Mycobacterium tuberculosis (Mtb) complex has been determined and promoted further research on the pathogenesis of TB. In general, acquiring enough disease information is impossible simply by observing clinical symptoms, and the development of animal models has provided complementary tools for human disease research.
In recent years, the pathogenesis of Mtb infection and the host immune response mechanisms have been widely researched and elucidated by immunological techniques and animal models (Fig. 7.1). Since Robert Koch in 1882 first used guinea pigs to prove that Mtb caused TB, various animal models—including the mouse, rat, rabbit, guinea pig, zebrafish, non-human primate, cattle, etc.—have been used to study various aspects of TB [3] (Fig. 7.2). Indeed, animal models have contributed to the development of infection technologies such as aerosol instillation and bacterial growth control following infection through innate and adaptive immune responses, which have provided invaluable contributions to our understanding of TB (Fig. 7.1). Each animal model cannot mimic completely the symptoms of human TB, so in practical application, the characteristics of different animals are often complementary to each other to fulfill research aims. For example, studies with the mouse, which lacks some immunological features, often require using guinea pigs as the complementary animal model to test vaccine effectiveness [4, 5]. At present, the main problem for every experimental animal model is that they cannot fully reflect human symptomatic TB.

(a) The intracellular transport process of Mtb. After Mtb infects the host, macrophages engulf the pathogen with the assistance of a variety of receptors, including complement receptor, mannose receptor and scavenger receptors. Then, common signaling pathways are activated leading to cell activation and cytokine production. Mtb is a classical intracellular pathogen and can persist in the early phagolysosome. After phagosomes mature, intracellular bactericidal substances such as reactive oxygen species (ROS) and reactive nitrogen species (RNS) will kill some Mtb. Surviving Mtb then begin to replicate and multiply within the macrophage, until the cell ruptures and disseminates bacteria to the surrounding cells. (b) T cell-dependent regulation of anti-TB immune response in vivo. There are several ways that cellular and humoral immunity may cooperate to protect the host from TB infection. CD4+ T cells can activate B cells to secrete antibody by major histocompatibility complex; CD4+ T cells can produce cytokines, e.g. IL-2 that can activate Natural Killer (NK) cells and promote cytotoxic immune responses associated with antibodies. Conversely, specialized phagocytes process and present TB antigens to CD4+ T cells, which results in increased proliferation of cytotoxic CD8+ T cells and enhanced Mtb killing. Meanwhile, the different T cells produce interferon γ (IFN-γ) that synergizes with tumour necrosis factor α (TNF-α) to activate macrophages

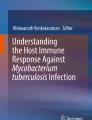
Pie chart showing the different animal models used for TB research. A PubMed search was done using the following keywords: “mouse AND tuberculosis”, “rat AND tuberculosis”, “guinea pig AND tuberculosis”, “non-human tuberculosis AND tuberculosis”, “zebrafish AND tuberculosis”, “cattle AND tuberculosis” and other animal models, including “cat tuberculosis”, “deer tuberculosis”, “minipig tuberculosis”, “fruit fly tuberculosis” and “dog tuberculosis”. The pie chart percentages were calculated as the proportion of each animal model to all the animal models
A clear understanding of the advantages and disadvantages of each animal model is necessary for experimental Mtb research. Mouse models are currently the most widely used laboratory animals, but they lack some characteristics of human TB including the formation of mature granulomas, central necrosis and cavities [6]. Guinea pigs are highly susceptible to Mtb and often need only a few bacilli to establish an infection in vivo [4]. Traditionally, rabbits were thought to be resistant to TB infection: however, recent reports suggest that rabbits can be used to establish models of chronic progressive granulomatous disease [7]. Although the rabbit model has been widely used, because some of the histopathological features in this animal closely resemble human TB, the lack of available commercial reagents has limited its use [7, 8]. By contrast, non-human primate cynomolgus monkeys are known to mimic TB symptoms in humans, including the formation of solid masses, necrosis and cavities [9]. The major advantage of this model is that it can establish latent TB infection and provide an opportunity to understand latency mechanisms. However, the high cost and hard management of this model limit its wide use in TB research. The use of animal models has greatly boosted TB research in recent years, but animals are not humans, and even Homo sapiens, who are highly similar at the genetic level, cannot fully mimic every aspect of human TB [8]. Therefore, key to successful experimental research is to consider the characteristics of the various animal models available and make reasoned choices. In this review, the characteristics of various animal models are summarized, pointing out their advantages and disadvantages and the research progress that each one has made. Such information informs selection of the most appropriate models to be used for TB research.
2 Mouse (Order Rodentia, Family Muridae, Mus musculus)
Mouse models are very popular in TB research, and they have been used extensively in developing diagnostics and experimental drugs and vaccines. The first scientist to use mice was Robert Koch [10]. The mouse is often chosen as the research animal model because the genetic and immunological background of humans and mice shares many similarities. Some important discoveries on the pathogenesis of TB, e.g. the roles of adaptive immunity and the process of granulomatous formation, have been discovered with mouse models. In addition, many preclinical trials of new TB drugs and vaccines must first be done in a mouse model before moving into human clinical trials.
In animal experiments, Mtb (usually the reference strain H37Rv) first invade and multiply in the lungs before spreading to other tissues. When establishing the mouse animal models, different infection routes are used, including aerosol exposure, intranasal, intratracheal and intravenous (Table 7.1). The evaluation standards are usually determined by observing the bacterial load in the lungs, histopathological changes and the immune index of the mice. A low-dose infection mouse model, e.g. with the C57BL strain, was established by inoculating ~100–200 bacilli via aerosol exposure. In this chronic infection mouse model, Mtb infection produced a well-tolerated infection dominated by a Th1-type immune response. In contrast, a high-dose infection BALB/c mouse model was established by intratracheal injection and resulted in a persistent pathological process characterized by progressive lung consolidation, extensive lung fibrosis and the presence of many T cells and anti-inflammatory cytokines. This high infection dose led to a persistent high bacterial load and host mortality. In addition, the phenotype of the mouse infection model was also influenced by various factors including environment, nutrition, immune status, gut microbiota and Mycobacteria species. In addition, host genetic factors may have different effects on establishing the mouse TB model. For example, if the mouse models were deficient in superoxide genes, this may affect host killing of Mtb in vivo. Expression of the host sst1 gene has been reported to exacerbate disease progression [28].
The Mtb genetic background may also play an essential role in infection. For example, the (3 R)-hydroxyacyl-ACP dehydratases—HadAB and HadBC—which can affect Mtb growth, colony morphology and biofilm formation, can also significantly influence the virulence of Mtb in a mouse model [29]. Mtb genes also exert a major influence on disease outcome by regulating innate and adaptive immunity [30]. Inducing low-level IL-1β production promotes macrophage phagocytosis, making it easier to establish infection in mice [31]. The total immunoglobulin isolated from the exposed healthcare workers in a TB-specialized hospital was reported to inhibit Mtb growth in vivo in an aerosol infection mouse model [20]. Of course, the nutrition and feeding environment of the mouse could likely affect experimental data. It has been shown that a high-fat diet provided to C3HeB/FeJ strain made TB infection in this mouse more likely to develop into a progressive tuberculosis and also impaired the protective effect of BCG vaccination, which may be related to dysbiosis of the gut microbiota [32].
Humans have different susceptibilities to Mtb infection because of heterogeneous immune responses. Only about 5% of infected humans would eliminate all pathogens, 5%–10% would develop active TB, and 90% become latent TB infection (LTBI) [33]. Thanks to advances in genetics technologies, many mouse models can be used in TB research. Currently, genetic approaches also provide a powerful tool to develop different species with special genetic backgrounds, including inbred Mtb-susceptible strains of CBA, DBA/2, C3HeB/FeJ and 129/SvJ mice and Mtb-resistant strains of BALB/c and C57BL/6J mice, which would provide strong support for TB research [34]. For example, in the DBA/2 mouse infection model, expression of the Trl1–4 gene can significantly affect DBA/2 mouse susceptibility to Mtb infection, which could allow further study of the regulatory network and immune cells involved and promote the development of new drugs and vaccines [34, 35]. The BALB/c mouse is the most widely used mouse for Mtb infection studies, particularly for identification of virulence factors and in the evaluation of vaccines [36,37,38,39]. The recent studies have established mouse models that are contributing significantly to TB research [40]. For example, humanized mice have been used to investigate post-chemotherapy relapse TB [40], and a new outbred mouse model named Diversity Outbred (DO) can provide potentially a novel vaccination model that can better reflect the TB outcomes observed in humans [41].
Mouse models have several advantages, including low cost, the availability of abundant commercial reagents and mature immunological evaluating indices. Mouse models also have important disadvantages: (1) the mouse is not a natural reservoir for Mtb, and the pathways and immune cells involved during infection maybe different; (2) the current common mouse model(s) cannot fully mimic the symptoms of human TB; (3) humanized mice can mimic aspects of human infection, but are expensive; (4) some TB symptoms cannot be fully replicated in mouse models. Despite these disadvantages, there is still an urgent need to develop novel mouse models.
3 Rat (Order Rodentia, Family Muridae, Rattus norvegicus)
The use of rats in TB research was first reported in 1923 by Gloyne and Page, but it was not until 1950 that the characteristics of the rat model were elaborated by Gray et al. [42, 43]. Earlier reports showed that rats are resistant to infection with human, bovine and avian strains of tubercle bacilli [16, 44]. However, later research has shown that if the bacteria can directly infect some target organs of the host, such as the lungs, liver or spleen, the result will be significant pathological changes in the rats. The rat model is very similar to the mouse model, and infection can be established through a variety of inoculation methods, including oral, subcutaneous, intraperitoneal, intranasal and aerosol [42]. Currently, several rat breeds, such as Wistar [45], nude [46], American cotton [47] and Lewis [48], have been used in TB research. The pathology following infection is influenced by the breed and route of infection: for example, pulmonary infection of American cotton rats produced necrotic granulomas, whilst the granulomas observed in Wistar and Lewis rats did not have necrotic lesions [49]. Previous studies have shown that all pathological changes and disease processes are dose-dependent in rat models. Even different subspecies of the same rat can have different immune responses: for example, the American cotton rat has two subspecies S. fulviventer and S. hispidus, and the infection mortality rate in S. fulviventer was significantly higher than that observed in S. hispidus [47]. Although there have not been many reports on the use of the rat model in TB research in recent years, the rat has some specific characteristics that make it still a promising TB research animal model (Table 7.2).
4 Rabbit (Order Lagomorpha, Family Leporidae, Oryctolagus cuniculus)
In nature, there are very few reported cases of Mtb infection in rabbits, and they mainly involve non-tuberculous mycobacteria (NTM) such as Mycobacterium avium [53]. There is only one reported case of a rabbit on a New Zealand farm infected with M. bovis [54]. Therefore, it seems plausible that rabbits might be resistant to TB or have some sort of self-protection mechanisms against Mtb infection [55]. Interestingly, the rabbit was the first laboratory animal to be used for TB research, recorded in 1867 [56]. Generally, rabbits have been widely and successfully used as animal models for many years, both in the production of immunological reagents and as infection models [57, 58]. In recent years, the New Zealand white rabbit has become common in laboratory research [53], and because rabbit animal models closely reflect the symptoms of some human diseases, they are often used to explore the pathogenesis of diseases and to develop new vaccines and therapies [58].
Rabbits are relatively resistant to Mtb infection when compared with mice and guinea pigs. Furthermore, different infection routes, mycobacterial strains and doses may lead to different disease outcomes (Table 7.3). Rabbits infected with HN878, a hyper-virulent Mtb strain, can develop progressive cavitation that is similar to cavitation seen in humans with active TB [64]. However, rabbits infected with CDC1551, a hyper-immunogenic clinical Mtb isolate, became latently infected [59]. In terms of infection route, rabbits infected with Mtb HN878 by aerosol inoculation developed granulomas and lung cavitation [65, 66]. In addition, the rabbit model was resistant to mimicking natural infection with M. bovis but showed significant susceptibility through inhalation or bronchial inoculation [67]. Interestingly, different subspecies are also susceptible to different Mtb strains; thus, inbred strains of New Zealand white rabbits have higher susceptibility to Mtb than outbred strains [68].
Rabbits have several advantages in TB research: (1) due to their relative resistance to Mtb infection, latent TB infection can be studied in this model [59, 69]; (2) rabbits can develop similar pulmonary cavitation as seen in humans, so they can be used to study the factors of disease formation and the pathogenesis of bronchial infection [67]; (3) rabbits are large animals to allow facile collection of sufficient blood and tissue samples from a single animal without sample enrichment [53]; (4) rabbits are also suitable for pharmacological experiments with anti-TB drugs, including drug penetration, distribution and cell accumulation [70]; (5) rabbits have been used to study bovine para-TB infection [71]. However, there are some disadvantages principally that they require higher biocontainment, there is a lack of immunological reagents and often the clinical signs are not obvious. Regardless, rabbit models for TB research will become increasingly popular in the future as new reagents are developed and biosafety conditions are established.
5 Zebrafish (Order Cypriniformes, Family Cyprinidae, Subfamily Danioninae, Danio rerio)
The zebrafish was first used in TB research by the group of Ramakrishnan in 2002 [72]. It is a useful tool to demonstrate Mtb virulence and pathogen-vertebrate host interactions (Table 7.4). Their use has become common in recent years and has benefited from the development of genetic approaches and improved imaging techniques [78]. Zebrafish are vertebrate, but they do not have lungs and are not a natural Mtb reservoir, so they cannot present some symptoms of mammalian TB. Mycobacterium marinum, which shares 85% genome homology with Mtb, can establish an infection in zebrafish that shares some similarities to human and mouse infections. There are two established zebrafish infection models with their own characteristics: an embryonic-larval model and an adult model [49, 78]. The immune markers during TB infection in adult zebrafish are similar to those of mammals, such as humans and mice. However, the embryonic-larval model is preferred for studying the effects of innate immunity on Mtb infection, due to its lack of an adaptive immune system.
In nature, zebrafish infection by M. marinum via the gastrointestinal tract has been reported [79]. However, zebrafish can be infected in the laboratory with M. marinum via various routes, including intraperitoneal and intramuscular and via the caudal vein. Local injections via the notochord, muscle, hindbrain ventricle, otic vesicle and yolk have been developed in zebrafish to study macrophage and neutrophil chemotaxis. Latent, chronic and active TB states can be established in zebrafish and depend on the inoculation doses and the different M. marinum strains. Latent infection model can be established by low-dose inoculation, and chronic progressive disease and acute infection by high-dose inoculation [80]. Early injection of M. marinum into the yolk of zebrafish embryos can provide a method to achieve a systemic Mycobacteria infection [75]. In addition, the M. marinum yolk infection model can be useful for high-throughput applications since it can be automated using an injection robot [75, 81, 82].
Active TB in zebrafish is characterized by rapid lethal inflammation, whilst chronic disease shows swelling of the abdomen and haemorrhages and skin ulceration typical of TB [83]. Following infection, bacteria invading zebrafish are phagocytized by macrophages and form caseating granulomas similar to human TB [72, 84]. Most granulomas also contain a necrotic centre where bacteria settle and form a cuff of cells, separate from the surrounding tissue [76, 77].
Zebrafish have been used extensively to evaluate new drugs and vaccines and are a useful model for gene editing and real-time imaging techniques. Embryonic-larval and adult zebrafish have been used to investigate each life stage of TB infection. Only the innate immune system exists in embryonic-larval zebrafish, and the main functional immune cells in this life stage are macrophages and neutrophils (the most suitable cells for studying zebrafish innate immune responses) [85,86,87]. In addition, the embryonic-larval model can develop externally and remain transparent, thus proving to be useful for studying host-pathogen interactions with real-time imaging systems [78, 88]. The use of fluorescent reporter systems has enabled more molecular details to be discovered, such as immune cell types, subcellular structures, intra-cytoplasmic trafficking and immune-modulatory mechanisms [89]. The development of gene editing techniques has enabled researchers to artificially design models on the genetic level, such as gene knockouts, to better meet research needs [90,91,92,93,94]. The larval model has been used to evaluate the efficacy of TB drugs such as rifampicin, isoniazid, ethambutol and moxifloxacin [95]. In addition, the embryonic infection model has been used to investigate early pathogenesis mechanisms, e.g. p62, a ubiquitin-mediated receptor protein contributed to host resistance to Mtb infection [96], and to elucidate the underlying mechanisms of the isoniazid-induced hepatotoxicity [97].
The adult zebrafish is more suitable for studying the pathogenic mechanisms of TB based on the mature innate and adaptive immunity system. The most common route for injecting bacteria into adult zebrafish is intraperitoneal, which results in progressive or chronic infection symptoms. At 1-week post-infection, form within many tissues and organs, including fatty tissue, pancreas, liver, spleen, adipose tissue and gonads. The histology of zebrafish granulomas is similar to human TB with a caseating and necrotic core surrounded by leukocytes and epithelial cells [98]. Like human control of TB, zebrafish control Mtb infection with their adaptive immune system. However, since zebrafish lack lymph nodes, immune cells can only develop and function in tissues or organs such as the spleen, kidney and thymus. The adaptive immune system begins to function at 4 weeks post-infection [76, 84].
The main advantage of zebrafish models is that granuloma formation can be reproduced, which is difficult in other animal models [99]. Other advantages include their small size, easy of breeding and their use for real-time imaging. However, zebrafish do have some disadvantages: for example, (1) they do not have lungs and cannot systematically reflect the symptoms of TB in mammals, limiting their use for studying underlying mechanisms of TB, and (2) blood samples for detecting immunological markers are difficult to collect [100].
6 Cattle (Order Artiodactyla, Family Bovidae, Subfamily Bovinae, Bos taurus)
A century has passed since Mycobacterium bovis was identified as the etiological agent of bovine TB [101]. Despite extensive research on the pathogenesis of M. bovis infection, the prevention, control and treatment of bovine TB still face great challenges. At present, BCG vaccination is the most effective way to prevent bovine TB. However, immune protection in cattle begins to decline 2 years after BCG vaccination, and this can be solved by repeating BCG vaccination [102,103,104]. Studies have shown also that BCG vaccine does not protect 6-month-old calves from bovine TB infection after pre-sensitization to environmental TB. This suggests that sensitivity to TB in the environment in human clinical trials is one of the main reasons for the wide variation in immune efficiency with BCG vaccination [105, 106]. Since calves are immune from birth, this model can be used to mimic vaccine immunity of human newborns in many developing countries. Despite decades of research and numerous new vaccines being tested, nothing superior to BCG has yet emerged. Cattle are a suitable model for simulating human diseases because of the similarity in disease type (Table 7.5). In addition, the outcrossing of almost all experimental cattle can serve as a link between vaccine testing in small animal models and subsequent human experiments.
Cattle with bovine TB show significant pathological changes and immune responses in various target organs that are comparably observed in human and mainly in the lungs, respiratory tracts and lymph nodes [101, 112]. Generally, cattle in-the-field become infected when they inhale or ingest pasture, water or fomites contaminated with M. bovis [113]. In experimental research, there are many routes by which TB can spread to cattle other than via the respiratory tract and include the intravenous [114], subcutaneous [115], oral [116], intranasal [117], intratracheal [118], intratonsillar [119] and aerosol routes [120]. More recently, some researchers have tried to establish the infection model upon exposure to infectious sources in laboratory animals, in order to mimic natural infection conditions [105, 107, 121]. In cattle, as in other animal models, the doses and routes of inoculation can significantly affect the outcome of infection. Unlike other animals, cattle rarely shed M. bovis, and establishing infection in other cattle usually requires large doses of bacteria [122]. Neill et al. fully elucidated, experimentally, the relationship between challenge doses and pathological changes in cattle [123].
Calmette and Guerin created the first attenuated TB vaccine in 1906—BCG vaccine—that can protect against artificial or natural TB infection. Since then, new anti-TB vaccines have been developed that inactivate some of BCG’s own genes, such as auxotrophic mutants, to reduce skin test responses and develop more safe vaccines for immuno-deficient individuals [108]. A gene deletion vaccine based on M. bovis is also an option, whereby some virulence or metabolism-related genes were deleted and the vaccine showed a significantly increased IFN-γ response in a calf infection model [105]. Relatively safe inactivated vaccines and DNA vaccines have also been developed, but trials in calf models did not show superior immune performance over BCG [107, 109]. Thus, safer and effective vaccines need to be developed, and both neonatal and adult bovine models are important for validating vaccine efficacy.
The main advantage of using cattle is that they are the natural host for M. bovis and thus display the most complete pathogenic mechanisms and pathological changes. Promising vaccine candidates can be tested on natural hosts prior to clinical trials. Other advantages are that the pathology and immunology of bovine TB are very similar to human TB, and related commercial immunological reagents are readily available. In addition, cattle are suitable for screening anti-TB vaccines and drugs, and it is relatively easy to collect large numbers and volumes of blood samples. Conversely, the disadvantages of using cattle are high cost of the animals and the larger facilities required for experimental work.
7 Guinea Pigs (Order Rodentia, Family Caviidae, Cavia, C. porcellus)
Guinea pigs have been used for more than a century for studying TB [4]. This animal model has played a key role in elucidating the pathogenesis of TB. Guinea pigs are highly susceptible to Mtb and can be infected by aerosol inoculation with ultra-low doses of bacteria [124]. At present, the guinea pig strain most used in the laboratory is the outbred Dunkin-Hartley strain, although inbred strains do exist [125, 126] (Table 7.6). Several well-characterized inoculation routes have been used to establish TB infection in guinea pigs, including the aerosol route and intratracheal and intranasal instillation [131]. The aerosol route is the most used. After infection with Mtb, symptoms similar to those of human TB appear at the lesion, such as central necrotic granuloma surrounded by lymphocytes, macrophages, multinucleated giant cells and fibrotic capsules [4]. However, cavitation is rarely observed in guinea pigs, which is a shortcoming of the model that may affect the testing of some anti-TB compounds [131, 132].
In order to clearly establish and characterize the symptoms of guinea pig infection with Mtb, the aerosol method was used initially to inoculate very low doses of bacteria [4]. The process of bacterial replication in the lungs and spleen of guinea pigs after infection was comprehensively described by Alsaadi and Smith in 1973 [133]. In the lungs, the logarithmic growth phase was reached after 16 days of infection, and after a few weeks of replication, the bacterial load reached its maximum and remained stable [133]. TB infection in guinea pigs shows dose-dependent characteristics, e.g. aerosol infection with 20–50 bacilli enables animals to reach humane end points more quickly than low-dose infection in non-sensitive animal models, and high-dose infection leads to earlier humane end points [134,135,136,137]. Importantly, high doses of infection are not consistent with the nature of natural transmission and are not particularly relevant to clinical trials.
The guinea pig model has been used widely to test new anti-TB drugs such as Capreomycin [138], PA-824 [139] and vaccines, such as the subunit vaccine composed of proteins Ag85b and ESAT6-CFP10 [137, 140,141,142]. Guinea pigs have some immunological features, such as the substantial similarities between the guinea pig and human CD1 systems [143, 144], which can be an advantage in testing for more types of vaccines, including glycolipid vaccines [136, 145]. The guinea pig model is also useful for identifying antigen targets for vaccine development. Testing of live attenuated TB vaccines has also been done with guinea pig models to provide a full profile of biosafety and potency prior to use in humans [142, 146]. Guinea pigs are considered an ideal model for testing anti-TB drugs because they mimic the pathological lesion changes observed in humans [147]. A significant advantage of the guinea pig model compared to the mouse model is that it can mimic the symptoms of latent infection and thus provides an opportunity for surrogate studies of the latency of human TB [148]. Disadvantages of guinea pigs as a model are the paucity of immunological tools, reagents and guinea pig strains. Nevertheless, the development of tools for guinea pig research is likely to increase their use in the future.
8 Non-Human Primates
Non-human primates (NHPs) have become increasingly popular in TB research, largely because NHPs provide excellent cellular and immunological insights into TB [49, 149] (Table 7.7). NHPs were first used in TB research in 1956, when Leno et al. used rhesus macaques to develop anti-TB drugs [150, 151]. In the past few decades, the application of NHPs in TB research has made great progress. For any animal model, the first consideration is whether the model is susceptible to the target pathogen. Previous studies have shown that both Old World and New World NHPs are susceptible to all Mtb strains tested [161]. Initially, rhesus macaques were used as animal models to study the pathogenesis of TB and to test new drugs and vaccines. Interest in using NHPs has increased with the emergence of human immunodeficiency virus (HIV) [162]. NHPs commonly used in the laboratory include rhesus macaques (Order Primates, Family Cercopithecidae, Macaca mulatta), cynomolgus macaques (Macaca fascicularis) and the common marmoset (Callithrix jacchus), all of which can recapitulate the full spectrum of outcomes of TB infection seen in humans. Indeed, different Mtb strains can produce different outcomes, ranging from rapidly progressive TB to latent TB. Many Mtb strains have been used in NHPs, including Mtb 5159, CDC1551, H37Rv and the Erdman strain. The latter is most used to study TB in NHPs [9, 163,164,165,166,167]. In addition, the routes, locations and doses of Mtb inoculation can affect infection outcomes [149]. For example, intrabronchial instillation can mimic all the outcomes of TB infection seen in humans, but it does not reflect the natural course of infection and bypasses the immune defences of the host’s upper respiratory tract [9, 165]. The first reported infection route of Mtb in NHPs was intratracheal instillation [150, 151], and the most commonly used methods currently in the laboratory are intra-airway instillation and inhalation of aerosolized bacilli [168]. Furthermore, Capuano et al. refined the infection process by introducing the fibre-optic bronchoscope, which could precisely quantify bacterial inocula into targeted organs [9]. Regardless, the results of some infections can still vary, and individual genetic differences, sample preparation and delivery before challenge can all significantly influence outcomes [169]. Therefore, more specialized and advanced equipment are needed urgently to produce better data by NHP models.
NHPs infected with different doses of the Erdman strain Mtb by intratracheal instillation produce a range of symptoms from active TB to latent TB [158]. This was proved by the development of dose-dependent TB in Mtb-infected macaques. High doses of bacteria caused monkeys to die of TB between 7 and 13 weeks post-infection, with pathological findings of extensive bilateral tuberculous pneumonia, abundant necrosis and extrapulmonary disease at the lesion sites [149]. Infection with moderate doses of bacteria led to a slower progression of disease in macaques, with the host dying between 14 and 24 months post-infection, with pathological findings of extensive pulmonary changes such as necrosis and extrapulmonary disease. Interestingly, cell infiltration in moderately infected macaques showed a tendency to increase compared to pathological changes after a high dose of infection. At low doses, the macaques developed a slower progression of the disease, and the host animals lived up to 19 months post-infection; their pathology showed smaller, denser granulomas at the site of the lesion, which were very similar to human TB [9, 149]. These pathological observations are extremely advantageous for studying human TB, especially with a low-dose infection model, and should provide a clearer understanding of the pathogenesis and pathological changes of human TB.
NHPs are generally considered to be very similar to humans, both anatomically, and pathologically and symptomatically for TB [168, 170]. The rhesus monkey is the first animal model of NHP, and its significant advantage is that it can perfectly recapitulate a series of symptoms of human TB, and the relevant commercial reagents and procedures are well developed [9, 149, 165]. Earlier studies showed that very low doses of Mtb could cause fatal TB in macaques [152, 171]. In NHP, there were also differences in susceptibility between macaque species. In rhesus monkeys, cynomolgus macaques and vervets, 100 colony forming units (CFU) of Erdman strains were inoculated into the three models by intrathecal injection [149, 164]. The infection time in vervet monkeys was faster than in rhesus monkeys, and the cynomolgus monkeys even showed resistance to Mtb infection [153]. However, different strains infected the same model differently [7, 128, 163]. For example, rhesus monkeys infected with the H37Rv strain showed subclinical symptoms [154], the attenuated strain CDC1551 led to latent TB, and Erdman strain showed progressive TB symptoms [155, 159]. Interestingly, the susceptibility of the same species of macaques from different geographical regions to the Mycobacterium strains also varies [172]. For example, rhesus macaques from India and China were inoculated with the same dose of Mtb, and whereas macaques from India were asymptomatic, the macaques from China showed progressive TB symptoms [154,155,156]. In 2013, a new NHP model, the common marmoset, was developed, which not only has the advantages of traditional NHP models but also has more prominent advantages in individual size of the monkey, their conditions for breeding and differences in their individual genetic backgrounds [159].
TB in NHPs and humans share similar symptoms [149]. After infection with Mtb, the bacteria enter the lungs and are taken up by professional phagocytes such as alveolar macrophages or dendritic cells [167]. After overcoming host innate and adaptive immune responses, the bacteria begin to replicate and spread in vivo. Every bacterium that survives in the body can form granulomas in the lungs. There is no uniform structure of TB granulomas, and in vivo granulomas are structurally and histopathologically diverse [165]. Lin et al. tracked the lesions in Mtb-infected cynomolgus macaques with F-fluorodeoxyglucose positron emission tomography/computed tomography imaging [167, 173] and showed that there were significant differences in lesions within individuals, and the final infection outcome could be predicted by the lesions [167]. Traditionally, the host can either control bacterial replication in vivo resulting in latent TB, or the bacteria start replicating and spreading to form active TB [149]. Latent infection carries the risk of reactivation and is a potential active TB outbreak point, and more research is needed to establish effective protocols for diagnosing and treating latent infections. The well-characterized cynomolgus monkey is the most suitable model for research into diagnostics and vaccines [174, 175]. Latent infection can remain stable in cynomolgus monkeys and reactivated when the host is immunosuppressed and thus mimic the symptoms of human latent TB [165].
Thus, the main advantages of NHPS are as follows: (1) similarity to humans; (2) rhesus macaque, cynomolgus macaque and common marmosets can reflect a series of similar outcomes to human TB; (3) cynomolgus macaques in particular present symptoms like human TB, and rhesus macaques and common marmosets play an important role in simulating particular aspects of TB; (4) the common marmosets are small, easy to group and house and cost-effective.
9 Other Models
The biological characteristics of other animals used to study TB are shown in Table 7.8 and discussed below.
9.1 Cat (Order Carnivora, Family Felidae, Felis catus)
Recently, five Abyssinian cats from an Italian cat farm were diagnosed with TB interstitial pneumonia, drawing our attention to the possibility of using cats as experimental animal models for TB research [181]. One interesting finding was that infection of cats with Bartonella henselae, the etiological agent of cat scratch disease, showed TB-like symptoms such as caseous necrosis and Langhans giant cells [182, 183].
The main etiological agents of cat TB are M. bovis, M. microti and some non-TB Mycobacteria. The incidence of TB in cats has been low, thanks to specialized eradication programmes and the use of commercial feed for pets [184]. TB in cats is transmitted mainly through the digestive tract, skin and by inhalation, and surprisingly there are no specific clinical TB characteristics in cats [185]. Granulomatous inflammation, cell infiltration and numerous alveolar macrophages containing Mtb are present in lesions [186]. There are very few reports on the use of cats as a TB model animal, and further research is needed to determine if they have any advantages over the more commonly used animal models.
9.2 Dog (Order Carnivora, Family Canidae, Canis familiaris)
Dogs are typical ‘sniffer’ animals with a very sensitive olfactory system, and they are used widely for drug searches, search-and-rescue and detecting pathogens [187] and pathological signals and conditions, e.g. malaria [188]. Some microbial infections produce special volatile organic compounds that can be sensed by sniffer animals [189]. Companion animals are rarely infected with TB, although there has been a report of a dog infected after being bitten by a wild animal infected with Mtb [177]. This raises the possibility that the frequent close contact between pets and humans may provide an opportunity for TB to spread inter-species. In dogs, the main symptoms of TB affect the lungs and regional lymph nodes. The first reported case of TB in a dog was published in 2016 [190]. The main pathological changes of a dog with cardiac tuberculoma were diffuse pneumonia, fibrinous pericarditis and large, yellow, semi-solid masses of caseous necrosis in the left and right atrium. Importantly, Mtb was isolated from the faeces of infected dogs, suggesting that faecal matter can act as a potential source of Mtb infection for animals and humans. Mtb can also be found in dog nasal secretions and urine. Dogs should be considered as a model animal to demonstrate the source and incidence of TB infection in humans, during studies of TB induced by M. tuberculosis and M. bovis infection.
9.3 Deer (Order Artiodactyla, Family Cervidae, Genus cervus)
Deer are globally ubiquitous, and some subgroups feed in artificial facilities such as game parks, zoological parks and gardens, where they can come into close contact with humans [191]. Many deer farms have been established to provide antler, venison and deer by-products. The occurrence of TB has been detected early in deers, and both captive and wild deer herds are highly susceptible to M. bovis, which has stimulated research in TB in this animal [192]. This is a major advance in understanding the aetiology, pathogenesis and epidemiology of TB in natural hosts and has important implications for detecting and treating TB.
M. bovis is the primary Mycobacterium detected in deer, which can be infected through contact with animals that carry the pathogens, such as tubercule-infected cattle and brush-tailed possums [193]. Indeed, there is another explanation: farmed animals and wild populations may have been infected by inhaling or licking terminally ill possums [194, 195]! Farmed deer are valuable economically, and it is important to develop a suitable method to detect M. bovis. Initially, intradermal tests were used, but deer sensitivity to the presence of M. bovis in the environment produced false-positive data that severely compromised the accuracy of the tests [196]. Carter et al. established a comparative cervical test in 1985, which showed up to 90% sensitivity in experimentally infected herds [197]. Subsequently, in 1985, Griffin and Cross developed a more sophisticated and accurate laboratory test that involved all aspects of immunological indicators in animals infected with TB [198]. In 2002, a more accurate ELISA-based antibody test was developed to compensate for the false-positives of previous tests [196].
In terms of vaccines, BCG is currently the only commercially approved vaccine with very high protection efficacy in humans and animals. An effective vaccine can protect animal populations, but the problems that arise are also of concern. Vaccinating farmed animals with BCG, for example, may lead to a higher false-positive rate in skin reactions for later TB tests, affecting normal test results [199]. It has been reported that either continuous or booster doses of BCG greatly improved immunity to BCG for deer [200]. The development of a new TB vaccine may help prevent TB in domestic and farmed animals.
9.4 Minipig (Order Artiodactyla, Family Suidae, Sus domesticus)
Use of the minipig model in TB research was first reported in 2010 by Gil et al. [201]. Minipigs infected with Mtb show similar symptoms of latent TB infection (LTBI) to those seen in humans. A characteristic feature of this model is the ability to generate a very strong Th1-type immune response to control infection, as well as the ability to induce a strong local response during fibrosis. In terms of local pulmonary structure, minipigs are very similar to humans, which will greatly benefit our understanding of LTBI mechanisms and allow us to establish more rational treatment and prevention approaches in the future.
9.5 Fruit Fly (Order Diptera, Family Drosophilidae, Drosophila melanogaster)
D. melanogaster is an ideal model organism for studying innate immunity, and it has been widely used to elucidate the pathophysiological mechanisms of pathogen infections and associated immune responses. The Mycobacterium commonly used in fruit flies is M. marinum, which is usually injected into the abdomen under CO2 anaesthesia using specialized equipment. The pathology of Drosophila infected with Mtb is characterized by extensive tissue lesions and low bacterial load, which is useful for studying pathogen-host interaction mechanisms [202]. Drosophila have obvious advantages of easy feeding, handling, strong fertility, short passage time, low cost and mature technology, which is conducive to effective cost control [203, 204]. However, their lack of an adaptive immune system is a disadvantage and limits their use to studying only innate immune responses.
10 Conclusions and Perspectives
TB has been known for millennia, and it has been a century since the BCG vaccine was developed and given to people in 1921, but the infection is still not completely controlled. The main reasons are the complex mechanisms of tuberculosis initiation and progression and the difficulties in developing effective vaccines and drugs for absolutely preventing and treating TB. Using animal models is crucial in TB research, especially in simulating TB symptoms and elucidating mechanisms of pathogenesis and pathology. Although a variety of animal models have been used and described in detail above, none has been able to recapitulate all the symptoms of TB in humans. The development of LTBI animal models is still a challenge. An ideal animal model of LTBI needs to adequately mimic the state of persistent infections in TB patients. Although animal models like mouse, guinea pigs, rabbit and non-human primates can mimic human LTBI to a certain extent, they still cannot fully replicate human infection. Therefore, it is necessary to modify the available latent animal models or develop new models for LTBI research. Recently, the application of new techniques in genetics, immunology and molecular biology has led to new experimental animal models for TB research, such as humanized mice. Other experimental animal models, such as transgenic mice and knockout animal models, are also needed for developing and testing vaccines and drug treatments. However, many of the TB animal models are limited by their high cost and considerations of biosafety and ethics. To improve the efficacy of animal models to evaluate vaccines and drugs, new advanced imaging technologies are also needed. In addition, mathematical modelling plays an important role in collecting and analysing the data from TB animal models, and these models need to be developed further. In studies, it is important to choose the right TB animal models for different research aims and projects, and using complementary models is encouraged. Although there maybe disadvantages of different animal models, it is undeniable that all experimental animal models have made outstanding contributions to understanding the pathogenesis of TB, and they will continue to be used to develop new TB vaccines, drugs and therapies.
References
Harding E. WHO global progress report on tuberculosis elimination. Lancet Respir Med. 2020;8(1):19. https://doi.org/10.1016/S2213-2600(19)30418-7.
Weledji EP, Pokam BT. Abdominal tuberculosis: is there a role for surgery? World J Gastrointest Surg. 2017;9(8):174–81. https://doi.org/10.4240/wjgs.v9.i8.174.
Cambau E, Drancourt M. Steps towards the discovery of Mycobacterium tuberculosis by Robert Koch, 1882. Clin Microbiol Infect. 2014;20(3):196–201. https://doi.org/10.1111/1469-0691.12555.
Clark S, Hall Y, Williams A. Animal models of tuberculosis: Guinea pigs. Cold Spring Harb Perspect Med. 2014;5(5):a018572. https://doi.org/10.1101/cshperspect.a018572.
Orme IM, Ordway DJ. Mouse and Guinea pig models of tuberculosis. Microbiol Spectr. 2016;4:4. https://doi.org/10.1128/microbiolspec.TBTB2-0002-2015.
Orme IM. The mouse as a useful model of tuberculosis. Tuberculosis (Edinb). 2003;83(1–3):112–5. https://doi.org/10.1016/s1472-9792(02)00069-0.
Tsenova L, Ellison E, Harbacheuski R, Moreira AL, Kurepina N, Reed MB, et al. Virulence of selected Mycobacterium tuberculosis clinical isolates in the rabbit model of meningitis is dependent on phenolic glycolipid produced by the bacilli. J Infect Dis. 2005;192(1):98–106. https://doi.org/10.1086/430614.
Williams A, Orme IM. Animal models of tuberculosis: an overview. Microbiol Spectr. 2016;4:4. https://doi.org/10.1128/microbiolspec.TBTB2-0004-2015.
Capuano SV 3rd, Croix DA, Pawar S, Zinovik A, Myers A, Lin PL, et al. Experimental Mycobacterium tuberculosis infection of cynomolgus macaques closely resembles the various manifestations of human M. tuberculosis infection. Infect Immun. 2003;71(10):5831–44. https://doi.org/10.1128/IAI.71.10.5831-5844.2003.
Caceres-Assenco AM, Ferreira SCA, Santos AC, Befi-Lopes DM. Application of a Brazilian test of expressive vocabulary in European Portuguese children. Codas. 2018;30(2):e20170113. https://doi.org/10.1590/2317-1782/20182017113.
Major S, Turner J, Beamer G. Tuberculosis in CBA/J mice. Vet Pathol. 2013;50(6):1016–21. https://doi.org/10.1177/0300985813482952.
Boute M, Carreras F, Rossignol C, Doz E, Winter N, Epardaud M. The C3HeB/FeJ mouse model recapitulates the hallmark of bovine tuberculosis lung lesions following Mycobacterium bovis aerogenous infection. Vet Res. 2017;48(1):73. https://doi.org/10.1186/s13567-017-0477-7.
Lanoix JP, Lenaerts AJ, Nuermberger EL. Heterogeneous disease progression and treatment response in a C3HeB/FeJ mouse model of tuberculosis. Dis Model Mech. 2015;8(6):603–10. https://doi.org/10.1242/dmm.019513.
Driver ER, Ryan GJ, Hoff DR, Irwin SM, Basaraba RJ, Kramnik I, et al. Evaluation of a mouse model of necrotic granuloma formation using C3HeB/FeJ mice for testing of drugs against Mycobacterium tuberculosis. Antimicrob Agents Chemother. 2012;56(6):3181–95. https://doi.org/10.1128/AAC.00217-12.
Francisco-Cruz A, Mata-Espinosa D, Estrada-Parra S, Xing Z, Hernandez-Pando R. Immunotherapeutic effects of recombinant adenovirus encoding granulocyte-macrophage colony-stimulating factor in experimental pulmonary tuberculosis. Clin Exp Immunol. 2013;171(3):283–97. https://doi.org/10.1111/cei.12015.
Gray DF, Graham-Smith H, Noble JL. Variations in natural resistance to tuberculosis. J Hyg (Lond). 1960;58:215–27. https://doi.org/10.1017/s0022172400038304.
Andersen P, Askgaard D, Ljungqvist L, Bentzon MW, Heron I. T-cell proliferative response to antigens secreted by Mycobacterium tuberculosis. Infect Immun. 1991;59(4):1558–63. https://doi.org/10.1128/iai.59.4.1558-1563.1991.
Hoff DR, Ryan GJ, Driver ER, Ssemakulu CC, De Groote MA, Basaraba RJ, et al. Location of intra- and extracellular M. tuberculosis populations in lungs of mice and Guinea pigs during disease progression and after drug treatment. PLoS One. 2011;6(3):e17550. https://doi.org/10.1371/journal.pone.0017550.
Manca C, Tsenova L, Barry CE 3rd, Bergtold A, Freeman S, Haslett PA, et al. Mycobacterium tuberculosis CDC1551 induces a more vigorous host response in vivo and in vitro, but is not more virulent than other clinical isolates. J Immunol. 1999;162(11):6740–6.
Li H, Wang XX, Wang B, Fu L, Liu G, Lu Y, et al. Latently and uninfected healthcare workers exposed to TB make protective antibodies against Mycobacterium tuberculosis. Proc Natl Acad Sci U S A. 2017;114(19):5023–8. https://doi.org/10.1073/pnas.1611776114.
Flynn JL, Goldstein MM, Triebold KJ, Sypek J, Wolf S, Bloom BR. IL-12 increases resistance of BALB/c mice to Mycobacterium tuberculosis infection. J Immunol. 1995;155(5):2515–24.
Hernandez-Pando R, Orozcoe H, Sampieri A, Pavon L, Velasquillo C, Larriva-Sahd J, et al. Correlation between the kinetics of Th1, Th2 cells and pathology in a murine model of experimental pulmonary tuberculosis. Immunology. 1996;89(1):26–33.
Lopez B, Aguilar D, Orozco H, Burger M, Espitia C, Ritacco V, et al. A marked difference in pathogenesis and immune response induced by different Mycobacterium tuberculosis genotypes. Clin Exp Immunol. 2003;133(1):30–7. https://doi.org/10.1046/j.1365-2249.2003.02171.x.
Dormans J, Burger M, Aguilar D, Hernandez-Pando R, Kremer K, Roholl P, et al. Correlation of virulence, lung pathology, bacterial load and delayed type hypersensitivity responses after infection with different Mycobacterium tuberculosis genotypes in a BALB/c mouse model. Clin Exp Immunol. 2004;137(3):460–8. https://doi.org/10.1111/j.1365-2249.2004.02551.x.
Aguilar Leon D, Zumarraga MJ, Jimenez Oropeza R, Gioffre AK, Bernardelli A, Orozco Estevez H, et al. Mycobacterium bovis with different genotypes and from different hosts induce dissimilar immunopathological lesions in a mouse model of tuberculosis. Clin Exp Immunol. 2009;157(1):139–47. https://doi.org/10.1111/j.1365-2249.2009.03923.x.
Li H, Javid B. Antibodies and tuberculosis: finally coming of age? Nat Rev Immunol. 2018;18(9):591–6. https://doi.org/10.1038/s41577-018-0028-0.
Watson A, Li H, Ma B, Weiss R, Bendayan D, Abramovitz L, et al. Human antibodies targeting a Mycobacterium transporter protein mediate protection against tuberculosis. Nat Commun. 2021;12(1):602. https://doi.org/10.1038/s41467-021-20930-0.
Kramnik I. Genetic dissection of host resistance to Mycobacterium tuberculosis: the sst1 locus and the Ipr1 gene. Curr Top Microbiol Immunol. 2008;321:123–48. https://doi.org/10.1007/978-3-540-75203-5_6.
Lefebvre C, Frigui W, Slama N, Lauzeral-Vizcaino F, Constant P, Lemassu A, et al. Discovery of a novel dehydratase of the fatty acid synthase type II critical for ketomycolic acid biosynthesis and virulence of Mycobacterium tuberculosis. Sci Rep. 2020;10(1):2112. https://doi.org/10.1038/s41598-020-58967-8.
Namasivayam S, Sher A, Glickman MS, Wipperman MF. The microbiome and tuberculosis: early evidence for cross talk. MBio. 2018;9(5):e01420–18. https://doi.org/10.1128/mBio.01420-18.
Sousa J, Ca B, Maceiras AR, Simoes-Costa L, Fonseca KL, Fernandes AI, et al. Mycobacterium tuberculosis associated with severe tuberculosis evades cytosolic surveillance systems and modulates IL-1beta production. Nat Commun. 2020;11(1):1949. https://doi.org/10.1038/s41467-020-15832-6.
Arias L, Goig GA, Cardona P, Torres-Puente M, Diaz J, Rosales Y, et al. Influence of gut microbiota on progression to tuberculosis generated by high fat diet-induced obesity in C3HeB/FeJ mice. Front Immunol. 2019;10:2464. https://doi.org/10.3389/fimmu.2019.02464.
Yang J, He Y, Tang W, Wang F, Wang Y. Research progress of tuberculosis infection and immune response mechanism. Chin Med J (Engl). 2019;47:3.
Cooper AM. Mouse model of tuberculosis. Cold Spring Harb Perspect Med. 2014;5(2):a018556. https://doi.org/10.1101/cshperspect.a018556.
Marquis JF, Lacourse R, Ryan L, North RJ, Gros P. Genetic and functional characterization of the mouse Trl3 locus in defense against tuberculosis. J Immunol. 2009;182(6):3757–67. https://doi.org/10.4049/jimmunol.0802094.
Zatarain-Barron ZL, Ramos-Espinosa O, Marquina-Castillo B, Barrios-Payan J, Cornejo-Granados F, Maya-Lucas O, et al. Evidence for the effect of vaccination on host-pathogen interactions in a murine model of pulmonary tuberculosis by Mycobacterium tuberculosis. Front Immunol. 2020;11:930. https://doi.org/10.3389/fimmu.2020.00930.
Iantomasi R, Sali M, Cascioferro A, Palucci I, Zumbo A, Soldini S, et al. PE_PGRS30 is required for the full virulence of Mycobacterium tuberculosis. Cell Microbiol. 2012;14(3):356–67. https://doi.org/10.1111/j.1462-5822.2011.01721.x.
Arnold IC, Hutchings C, Kondova I, Hey A, Powrie F, Beverley P, et al. Helicobacter hepaticus infection in BALB/c mice abolishes subunit-vaccine-induced protection against M. tuberculosis. Vaccine. 2015;33(15):1808–14. https://doi.org/10.1016/j.vaccine.2015.02.041.
Khatri B, Keeble J, Dagg B, Kaveh DA, Hogarth PJ, Ho MM. Efficacy and immunogenicity of different BCG doses in BALB/c and CB6F1 mice when challenged with H37Rv or Beijing HN878. Sci Rep. 2021;11(1):23308. https://doi.org/10.1038/s41598-021-02442-5.
Huante MB, Saito TB, Nusbaum RJ, Naqvi KF, Chauhan S, Hunter RL, et al. Small animal model of post-chemotherapy tuberculosis relapse in the setting of HIV co-infection. Front Cell Infect Microbiol. 2020;10:150. https://doi.org/10.3389/fcimb.2020.00150.
Kurtz SL, Rossi AP, Beamer GL, Gatti DM, Kramnik I, Elkins KL. The diversity outbred mouse population is an improved animal model of vaccination against tuberculosis that reflects heterogeneity of protection. mSphere. 2020;5(2):e00097–20. https://doi.org/10.1128/mSphere.00097-20.
Gray DF, Noble JL, O’Hara M. Allergy in experimental rat tuberculosis. J Hyg (Lond). 1961;59:427–36. https://doi.org/10.1017/s0022172400039127.
Gloyne SR, Page DS. Reaction to B. tuberculosis in the albino rat. J Pathol Bacteriol. 1923;26:224.
Gray DF. The relative natural resistance of rats and mice to experimental pulmonary tuberculosis. J Hyg (Lond). 1961;59:471–7. https://doi.org/10.1017/s0022172400039164.
Gaonkar S, Bharath S, Kumar N, Balasubramanian V, Shandil RK. Aerosol infection model of tuberculosis in Wistar rats. Int J Microbiol. 2010;2010:426035. https://doi.org/10.1155/2010/426035.
Sugawara I, Yamada H, Mizuno S. Nude rat (F344/N-rnu) tuberculosis. Cell Microbiol. 2006;8(4):661–7. https://doi.org/10.1111/j.1462-5822.2005.00658.x.
Elwood RL, Wilson S, Blanco JC, Yim K, Pletneva L, Nikonenko B, et al. The American cotton rat: a novel model for pulmonary tuberculosis. Tuberculosis (Edinb). 2007;87(2):145–54. https://doi.org/10.1016/j.tube.2006.07.001.
Sugawara I, Yamada H, Mizuno S. Pulmonary tuberculosis in spontaneously diabetic goto kakizaki rats. Tohoku J Exp Med. 2004;204(2):135–45. https://doi.org/10.1620/tjem.204.135.
Singh P, Kolloli A, Subbian S. Animal models of tuberculosis. In: Understanding the host immune response against Mycobacterium tuberculosis infection; 2018. p. 67–97.
Lefford MJ, McGregor DD, Mackaness GB. Immune response to Mycobacterium tuberculosis in rats. Infect Immun. 1973;8(2):182–9. https://doi.org/10.1128/iai.8.2.182-189.1973.
Singhal A, Aliouat el M, Herve M, Mathys V, Kiass M, Creusy C, et al. Experimental tuberculosis in the Wistar rat: a model for protective immunity and control of infection. PLoS One. 2011;6(4):e18632. https://doi.org/10.1371/journal.pone.0018632.
Smith DT, Bethune N, Wilson JL. Etiology of spontaneous pulmonary disease in the albino rat. J Bacteriol. 1930;20(5):361–70. https://doi.org/10.1128/jb.20.5.361-370.1930.
Arrazuria R, Juste RA, Elguezabal N. Mycobacterial infections in rabbits: from the wild to the laboratory. Transbound Emerg Dis. 2017;64(4):1045–58. https://doi.org/10.1111/tbed.12474.
Gill JW, Jackson R. Tuberculosis in a rabbit: a case revisited. N Z Vet J. 1993;41(3):147. https://doi.org/10.1080/00480169.1993.35756.
Sevilla IA, Arnal MC, Fuertes M, Martin E, Comenge J, Elguezabal N, et al. Tuberculosis outbreak caused by Mycobacterium caprae in a rabbit farm in Spain. Transbound Emerg Dis. 2020;67(1):431–41. https://doi.org/10.1111/tbed.13366.
Villemin JA. 1867: Etudes sur la tuberculose. Paris: J- B Baillière et fils; 1867.
Dehnad A, Ravindran R, Subbian S, Khan IH. Development of immune-biomarkers of pulmonary tuberculosis in a rabbit model. Tuberculosis (Edinb). 2016;101:1–7. https://doi.org/10.1016/j.tube.2016.07.008.
Chen H, Liu X, Ma X, Wang Q, Yang G, Niu H, et al. A new rabbit-skin model to evaluate protective efficacy of tuberculosis vaccines. Front Microbiol. 2017;8:842. https://doi.org/10.3389/fmicb.2017.00842.
Subbian S, Tsenova L, O’Brien P, Yang G, Kushner NL, Parsons S, et al. Spontaneous latency in a rabbit model of pulmonary tuberculosis. Am J Pathol. 2012;181(5):1711–24. https://doi.org/10.1016/j.ajpath.2012.07.019.
Liu X, Jia W, Wang H, Wang Y, Ma J, Wang H, et al. Establishment of a rabbit model of spinal tuberculosis using Mycobacterium tuberculosis strain H37Rv. Jpn J Infect Dis. 2015;68(2):89–97. https://doi.org/10.7883/yoken.JJID.2014.147.
Mendez S, Hatem CL, Kesavan AK, Lopez-Molina J, Pitt ML, Dannenberg AM Jr, et al. Susceptibility to tuberculosis: composition of tuberculous granulomas in Thorbecke and outbred New Zealand white rabbits. Vet Immunol Immunopathol. 2008;122(1–2):167–74. https://doi.org/10.1016/j.vetimm.2007.11.006.
Zhang G, Zhu B, Shi W, Wang M, Da Z, Zhang Y. Evaluation of mycobacterial virulence using rabbit skin liquefaction model. Virulence. 2010;1(3):156–63. https://doi.org/10.4161/viru.1.3.11748.
Nedeltchev GG, Raghunand TR, Jassal MS, Lun S, Cheng QJ, Bishai WR. Extrapulmonary dissemination of Mycobacterium bovis but not Mycobacterium tuberculosis in a bronchoscopic rabbit model of cavitary tuberculosis. Infect Immun. 2009;77(2):598–603. https://doi.org/10.1128/IAI.01132-08.
Subbian S, Bandyopadhyay N, Tsenova L, O’Brien P, Khetani V, Kushner NL, et al. Early innate immunity determines outcome of Mycobacterium tuberculosis pulmonary infection in rabbits. Cell Commun Signal. 2013;11:60. https://doi.org/10.1186/1478-811X-11-60.
Singh AK, Gupta UD. Animal models of tuberculosis: lesson learnt. Indian J Med Res. 2018;147(5):456–63. https://doi.org/10.4103/ijmr.IJMR_554_18.
McMurray DN. Disease model: pulmonary tuberculosis. Trends Mol Med. 2001;7(3):135–7. https://doi.org/10.1016/s1471-4914(00)01901-8.
Peng X, Knouse JA, Hernon KM. Rabbit models for studying human infectious diseases. Comp Med. 2015;65(6):499–507.
Dorman SE, Hatem CL, Tyagi S, Aird K, Lopez-Molina J, Pitt ML, et al. Susceptibility to tuberculosis: clues from studies with inbred and outbred New Zealand white rabbits. Infect Immun. 2004;72(3):1700–5. https://doi.org/10.1128/IAI.72.3.1700-1705.2004.
Dharmadhikari AS, Nardell EA. What animal models teach humans about tuberculosis. Am J Respir Cell Mol Biol. 2008;39(5):503–8. https://doi.org/10.1165/rcmb.2008-0154TR.
Kjellsson MC, Via LE, Goh A, Weiner D, Low KM, Kern S, et al. Pharmacokinetic evaluation of the penetration of antituberculosis agents in rabbit pulmonary lesions. Antimicrob Agents Chemother. 2012;56(1):446–57. https://doi.org/10.1128/AAC.05208-11.
Shaughnessy LJ, Smith LA, Evans J, Anderson D, Caldow G, Marion G, et al. High prevalence of paratuberculosis in rabbits is associated with difficulties in controlling the disease in cattle. Vet J. 2013;198(1):267–70. https://doi.org/10.1016/j.tvjl.2013.08.030.
Davis JM, Clay H, Lewis JL, Ghori N, Herbomel P, Ramakrishnan L. Real-time visualization of Mycobacterium-macrophage interactions leading to initiation of granuloma formation in zebrafish embryos. Immunity. 2002;17(6):693–702. https://doi.org/10.1016/s1074-7613(02)00475-2.
Alibaud L, Rombouts Y, Trivelli X, Burguiere A, Cirillo SL, Cirillo JD, et al. A Mycobacterium marinum TesA mutant defective for major cell wall-associated lipids is highly attenuated in Dictyostelium discoideum and zebrafish embryos. Mol Microbiol. 2011;80(4):919–34. https://doi.org/10.1111/j.1365-2958.2011.07618.x.
Pozos TC, Ramakrishnan L. New models for the study of mycobacterium-host interactions. Curr Opin Immunol. 2004;16(4):499–505. https://doi.org/10.1016/j.coi.2004.05.011.
Benard EL, van der Sar AM, Ellett F, Lieschke GJ, Spaink HP, Meijer AH. Infection of zebrafish embryos with intracellular bacterial pathogens. J Vis Exp. 2012;61:3781. https://doi.org/10.3791/3781.
Parikka M, Hammaren MM, Harjula SK, Halfpenny NJ, Oksanen KE, Lahtinen MJ, et al. Mycobacterium marinum causes a latent infection that can be reactivated by gamma irradiation in adult zebrafish. PLoS Pathog. 2012;8(9):e1002944. https://doi.org/10.1371/journal.ppat.1002944.
Ramakrishnan L. Revisiting the role of the granuloma in tuberculosis. Nat Rev Immunol. 2012;12(5):352–66. https://doi.org/10.1038/nri3211.
van Leeuwen LM, van der Sar AM, Bitter W. Animal models of tuberculosis: zebrafish. Cold Spring Harb Perspect Med. 2014;5(3):a018580. https://doi.org/10.1101/cshperspect.a018580.
Bouz G, Al Hasawi N. The zebrafish model of tuberculosis—no lungs needed. Crit Rev Microbiol. 2018;44(6):779–92. https://doi.org/10.1080/1040841X.2018.1523132.
Meijer AH. Protection and pathology in TB: learning from the zebrafish model. Semin Immunopathol. 2016;38(2):261–73. https://doi.org/10.1007/s00281-015-0522-4.
Carvalho R, de Sonneville J, Stockhammer OW, Savage ND, Veneman WJ, Ottenhoff TH, et al. A high-throughput screen for tuberculosis progression. PLoS One. 2011;6(2):e16779. https://doi.org/10.1371/journal.pone.0016779.
Meijer AH, Spaink HP. Host-pathogen interactions made transparent with the zebrafish model. Curr Drug Targets. 2011;12(7):1000–17. https://doi.org/10.2174/138945011795677809.
van der Sar AM, Abdallah AM, Sparrius M, Reinders E, Vandenbroucke-Grauls CM, Bitter W. Mycobacterium marinum strains can be divided into two distinct types based on genetic diversity and virulence. Infect Immun. 2004;72(11):6306–12. https://doi.org/10.1128/IAI.72.11.6306-6312.2004.
Swaim LE, Connolly LE, Volkman HE, Humbert O, Born DE, Ramakrishnan L. Mycobacterium marinum infection of adult zebrafish causes caseating granulomatous tuberculosis and is moderated by adaptive immunity. Infect Immun. 2006;74(11):6108–17. https://doi.org/10.1128/IAI.00887-06.
Ramakrishnan L. The zebrafish guide to tuberculosis immunity and treatment. Cold Spring Harb Symp Quant Biol. 2013;78:179–92. https://doi.org/10.1101/sqb.2013.78.023283.
Le Guyader D, Redd MJ, Colucci-Guyon E, Murayama E, Kissa K, Briolat V, et al. Origins and unconventional behavior of neutrophils in developing zebrafish. Blood. 2008;111(1):132–41. https://doi.org/10.1182/blood-2007-06-095398.
Stachura DL, Traver D. Cellular dissection of zebrafish hematopoiesis. Methods Cell Biol. 2016;133:11–53. https://doi.org/10.1016/bs.mcb.2016.03.022.
Basheer F, Liongue C, Ward AC. Zebrafish bacterial infection assay to study host-pathogen interactions. Bio Protoc. 2020;10(5):e3536. https://doi.org/10.21769/BioProtoc.3536.
Torraca V, Masud S, Spaink HP, Meijer AH. Macrophage-pathogen interactions in infectious diseases: new therapeutic insights from the zebrafish host model. Dis Model Mech. 2014;7(7):785–97. https://doi.org/10.1242/dmm.015594.
Pensado-Lopez A, Fernandez-Rey J, Reimunde P, Crecente-Campo J, Sanchez L, Torres AF. Zebrafish models for the safety and therapeutic testing of nanoparticles with a focus on macrophages. Nanomaterials (Basel). 2021;11(7):1784. https://doi.org/10.3390/nano11071784.
Bek JW, Shochat C, De Clercq A, De Saffel H, Boel A, Metz J, et al. Lrp5 mutant and crispant zebrafish faithfully model human osteoporosis, establishing the zebrafish as a platform for CRISPR-based functional screening of osteoporosis candidate genes. J Bone Miner Res. 2021;36(9):1749–64. https://doi.org/10.1002/jbmr.4327.
Shah AN, Davey CF, Whitebirch AC, Miller AC, Moens CB. Rapid reverse genetic screening using CRISPR in zebrafish. Zebrafish. 2016;13(2):152–3. https://doi.org/10.1089/zeb.2015.29000.sha.
Wu RS, Lam II, Clay H, Duong DN, Deo RC, Coughlin SR. A rapid method for directed gene knockout for screening in G0 zebrafish. Dev Cell. 2018;46(1):112–25 e4. https://doi.org/10.1016/j.devcel.2018.06.003.
Shankaran SS, Dahlem TJ, Bisgrove BW, Yost HJ, Tristani-Firouzi M. CRISPR/Cas9-directed gene editing for the generation of loss-of-function mutants in high-throughput zebrafish F0 screens. Curr Protoc Mol Biol. 2017;119:31.9.1–9.22. https://doi.org/10.1002/cpmb.42.
Takaki K, Cosma CL, Troll MA, Ramakrishnan L. An in vivo platform for rapid high-throughput antitubercular drug discovery. Cell Rep. 2012;2(1):175–84. https://doi.org/10.1016/j.celrep.2012.06.008.
Munoz-Sanchez S, van der Vaart M, Meijer AH. Autophagy and Lc3-associated phagocytosis in zebrafish models of bacterial infections. Cell. 2020;9(11):2372. https://doi.org/10.3390/cells9112372.
Jia ZL, Cen J, Wang JB, Zhang F, Xia Q, Wang X, et al. Mechanism of isoniazid-induced hepatotoxicity in zebrafish larvae: activation of ROS-mediated ERS, apoptosis and the Nrf2 pathway. Chemosphere. 2019;227:541–50. https://doi.org/10.1016/j.chemosphere.2019.04.026.
Volkman HE, Pozos TC, Zheng J, Davis JM, Rawls JF, Ramakrishnan L. Tuberculous granuloma induction via interaction of a bacterial secreted protein with host epithelium. Science. 2010;327(5964):466–9. https://doi.org/10.1126/science.1179663.
Myllymaki H, Niskanen M, Oksanen KE, Ramet M. Animal models in tuberculosis research—where is the beef? Expert Opin Drug Discovery. 2015;10(8):871–83. https://doi.org/10.1517/17460441.2015.1049529.
Tokunaga Y, Shirouzu M, Sugahara R, Yoshiura Y, Kiryu I, Ototake M, et al. Comprehensive validation of T- and B-cell deficiency in rag1-null zebrafish: implication for the robust innate defense mechanisms of teleosts. Sci Rep. 2017;7(1):7536. https://doi.org/10.1038/s41598-017-08000-2.
Pollock JM, Rodgers JD, Welsh MD, McNair J. Pathogenesis of bovine tuberculosis: the role of experimental models of infection. Vet Microbiol. 2006;112(2–4):141–50. https://doi.org/10.1016/j.vetmic.2005.11.032.
Gong W, Liang Y, Wu X. Animal models of tuberculosis vaccine research: an important component in the fight against tuberculosis. Biomed Res Int. 2020;2020:4263079. https://doi.org/10.1155/2020/4263079.
Thom ML, McAulay M, Vordermeier HM, Clifford D, Hewinson RG, Villarreal-Ramos B, et al. Duration of immunity against Mycobacterium bovis following neonatal vaccination with bacillus Calmette-Guerin Danish: significant protection against infection at 12, but not 24, months. Clin Vaccine Immunol. 2012;19(8):1254–60. https://doi.org/10.1128/CVI.00301-12.
Parlane NA, Shu D, Subharat S, Wedlock DN, Rehm BH, de Lisle GW, et al. Revaccination of cattle with bacille Calmette-Guerin two years after first vaccination when immunity has waned, boosted protection against challenge with Mycobacterium bovis. PLoS One. 2014;9(9):e106519. https://doi.org/10.1371/journal.pone.0106519.
Buddle BM, Wards BJ, Aldwell FE, Collins DM, de Lisle GW. Influence of sensitisation to environmental mycobacteria on subsequent vaccination against bovine tuberculosis. Vaccine. 2002;20(7–8):1126–33. https://doi.org/10.1016/s0264-410x(01)00436-4.
Fine PE. Variation in protection by BCG: implications of and for heterologous immunity. Lancet. 1995;346(8986):1339–45. https://doi.org/10.1016/s0140-6736(95)92348-9.
Wedlock DN, Keen DL, McCarthy AR, Andersen P, Buddle BM. Effect of different adjuvants on the immune responses of cattle vaccinated with Mycobacterium tuberculosis culture filtrate proteins. Vet Immunol Immunopathol. 2002;86(1–2):79–88. https://doi.org/10.1016/s0165-2427(02)00017-x.
Guleria I, Teitelbaum R, McAdam RA, Kalpana G, Jacobs WR Jr, Bloom BR. Auxotrophic vaccines for tuberculosis. Nat Med. 1996;2(3):334–7. https://doi.org/10.1038/nm0396-334.
Vordermeier HM, Cockle PJ, Whelan AO, Rhodes S, Chambers MA, Clifford D, et al. Effective DNA vaccination of cattle with the mycobacterial antigens MPB83 and MPB70 does not compromise the specificity of the comparative intradermal tuberculin skin test. Vaccine. 2000;19(9–10):1246–55. https://doi.org/10.1016/s0264-410x(00)00238-3.
Young JA, Paterson JS. Studies on the vaccination of cattle as a measure against infection with tuberculosis with the living vole acid-fast bacillus. J Hyg (Lond). 1949;47(1):39–78. https://doi.org/10.1017/s0022172400014303.
Buddle BM, Keen D, Thomson A, Jowett G, McCarthy AR, Heslop J, et al. Protection of cattle from bovine tuberculosis by vaccination with BCG by the respiratory or subcutaneous route, but not by vaccination with killed Mycobacterium vaccae. Res Vet Sci. 1995;59(1):10–6. https://doi.org/10.1016/0034-5288(95)90023-3.
Neill SD, O’Brien JJ, McCracken RM. Mycobacterium bovis in the anterior respiratory tracts in the heads of tuberculin-reacting cattle. Vet Rec. 1988;122(8):184–6. https://doi.org/10.1136/vr.122.8.184.
Neill SD, Pollock JM, Bryson DB, Hanna J. Pathogenesis of Mycobacterium bovis infection in cattle. Vet Microbiol. 1994;40(1–2):41–52. https://doi.org/10.1016/0378-1135(94)90045-0.
Morse GD. Tuberculosis from man to animals. J Lancet. 1958;78(4):138–41.
Waddington FG, Ellwood DC. An experiment to challenge the resistance to tuberculosis in B.C.G. vaccinated cattle in Malawi. Br Vet J. 1972;128(11):541–52. https://doi.org/10.1016/s0007-1935(17)36683-6.
Jones GJ, Steinbach S, Sevilla IA, Garrido JM, Juste R, Vordermeier HM. Oral vaccination of cattle with heat inactivated Mycobacterium bovis does not compromise bovine TB diagnostic tests. Vet Immunol Immunopathol. 2016;182:85–8. https://doi.org/10.1016/j.vetimm.2016.10.010.
Neill SD, Hanna J, O’Brien JJ, McCracken RM. Excretion of Mycobacterium bovis by experimentally infected cattle. Vet Rec. 1988;123(13):340–3. https://doi.org/10.1136/vr.123.13.340.
Buddle BM, Aldwell FE, Pfeffer A, de Lisle GW, Corner LA. Experimental Mycobacterium bovis infection of cattle: effect of dose of M. bovis and pregnancy on immune responses and distribution of lesions. N Z Vet J. 1994;42(5):167–72. https://doi.org/10.1080/00480169.1994.35814.
Palmer MV, Whipple DL, Rhyan JC, Bolin CA, Saari DA. Granuloma development in cattle after intratonsillar inoculation with Mycobacterium bovis. Am J Vet Res. 1999;60(3):310–5.
Palmer MV, Waters WR, Whipple DL. Aerosol delivery of virulent Mycobacterium bovis to cattle. Tuberculosis (Edinb). 2002;82(6):275–82. https://doi.org/10.1054/tube.2002.0341.
Palmer MV, Wiarda J, Kanipe C, Thacker TC. Early pulmonary lesions in cattle infected via aerosolized Mycobacterium bovis. Vet Pathol. 2019;56(4):544–54. https://doi.org/10.1177/0300985819833454.
Neill SD, Bryson DG, Pollock JM. Pathogenesis of tuberculosis in cattle. Tuberculosis (Edinb). 2001;81(1–2):79–86. https://doi.org/10.1054/tube.2000.0279.
Neill SD, Hanna J, O’Brien JJ, McCracken RM. Transmission of tuberculosis from experimentally infected cattle to in-contact calves. Vet Rec. 1989;124(11):269–71. https://doi.org/10.1136/vr.124.11.269.
Smith DW, Harding GE. Animal model of human disease. Pulmonary tuberculosis. Animal model: experimental airborne tuberculosis in the Guinea pig. Am J Pathol. 1977;89(1):273–6.
Chan ED, Verma D, Ordway DJ. Animal models of Mycobacteria infection. Curr Protoc Immunol. 2020;129(1):e98. https://doi.org/10.1002/cpim.98.
Martinez L, Verma R, Croda J, Horsburgh CR Jr, Walter KS, Degner N, et al. Detection, survival and infectious potential of Mycobacterium tuberculosis in the environment: a review of the evidence and epidemiological implications. Eur Respir J. 2019;53(6):1802302. https://doi.org/10.1183/13993003.02302-2018.
Sugawara I, Udagawa T, Aoki T, Mizuno S. Establishment of a Guinea pig model of latent tuberculosis with GFP-introduced Mycobacterium tuberculosis. Tohoku J Exp Med. 2009;219(3):257–62. https://doi.org/10.1620/tjem.219.257.
Palanisamy GS, Smith EE, Shanley CA, Ordway DJ, Orme IM, Basaraba RJJT. Disseminated disease severity as a measure of virulence of Mycobacterium tuberculosis in the Guinea pig model. Tuberculosis (Edinb). 2008;88(4):295–306.
Padilla-Carlin DJ, McMurray DN, Hickey AJ. The Guinea pig as a model of infectious diseases. Comp Med. 2008;58(4):324–40.
Allen SS, Cassone L, Lasco TM, McMurray DN. Effect of neutralizing transforming growth factor beta1 on the immune response against Mycobacterium tuberculosis in Guinea pigs. Infect Immun. 2004;72(3):1358–63. https://doi.org/10.1128/IAI.72.3.1358-1363.2004.
Yang HJ, Wang D, Wen X, Weiner DM, Via LE. One size fits all? Not in in vivo modeling of tuberculosis chemotherapeutics. Front Cell Infect Microbiol. 2021;11:613149. https://doi.org/10.3389/fcimb.2021.613149.
Kato-Maeda M, Shanley CA, Ackart D, Jarlsberg LG, Shang S, Obregon-Henao A, et al. Beijing sublineages of Mycobacterium tuberculosis differ in pathogenicity in the Guinea pig. Clin Vaccine Immunol. 2012;19(8):1227–37. https://doi.org/10.1128/CVI.00250-12.
Alsaadi AI, Smith DW. The fate of virulent and attenuated Mycobacteria in Guinea pigs infected by the respiratory route. Am Rev Respir Dis. 1973;107(6):1041–6. https://doi.org/10.1164/arrd.1973.107.6.1041.
Wiegeshaus EH, McMurray DN, Grover AA, Harding GE, Smith DW. Host-parasite relationships in experimental airborne tuberculosis. 3. Relevance of microbial enumeration to acquired resistance in Guinea pigs. Am Rev Respir Dis. 1970;102(3):422–9. https://doi.org/10.1164/arrd.1970.102.3.422.
Brandt L, Skeiky YA, Alderson MR, Lobet Y, Dalemans W, Turner OC, et al. The protective effect of the Mycobacterium bovis BCG vaccine is increased by coadministration with the Mycobacterium tuberculosis 72-kilodalton fusion polyprotein Mtb72F in M. tuberculosis-infected Guinea pigs. Infect Immun. 2004;72(11):6622–32. https://doi.org/10.1128/IAI.72.11.6622-6632.2004.
Williams A, Hall Y, Orme IM. Evaluation of new vaccines for tuberculosis in the Guinea pig model. Tuberculosis (Edinb). 2009;89(6):389–97. https://doi.org/10.1016/j.tube.2009.08.004.
Grover A, Troudt J, Arnett K, Izzo L, Lucas M, Strain K, et al. Assessment of vaccine testing at three laboratories using the Guinea pig model of tuberculosis. Tuberculosis (Edinb). 2012;92(1):105–11. https://doi.org/10.1016/j.tube.2011.09.003.
Garcia-Contreras L, Fiegel J, Telko MJ, Elbert K, Hawi A, Thomas M, et al. Inhaled large porous particles of capreomycin for treatment of tuberculosis in a Guinea pig model. Antimicrob Agents Chemother. 2007;51(8):2830–6. https://doi.org/10.1128/AAC.01164-06.
Garcia-Contreras L, Sung JC, Muttil P, Padilla D, Telko M, Verberkmoes JL, et al. Dry powder PA-824 aerosols for treatment of tuberculosis in Guinea pigs. Antimicrob Agents Chemother. 2010;54(4):1436–42. https://doi.org/10.1128/AAC.01471-09.
Wang C, Lu J, Du W, Wang G, Li X, Shen X, et al. Ag85b/ESAT6-CFP10 adjuvanted with aluminum/poly-IC effectively protects Guinea pigs from latent Mycobacterium tuberculosis infection. Vaccine. 2019;37(32):4477–84. https://doi.org/10.1016/j.vaccine.2019.06.078.
Hanif SN, Garcia-Contreras L. Pharmaceutical aerosols for the treatment and prevention of tuberculosis. Front Cell Infect Microbiol. 2012;2:118. https://doi.org/10.3389/fcimb.2012.00118.
Grode L, Ganoza CA, Brohm C, Weiner J 3rd, Eisele B, Kaufmann SH. Safety and immunogenicity of the recombinant BCG vaccine VPM1002 in a phase 1 open-label randomized clinical trial. Vaccine. 2013;31(9):1340–8. https://doi.org/10.1016/j.vaccine.2012.12.053.
Eckhardt E, Bastian M. Animal models for human group 1 CD1 protein function. Mol Immunol. 2021;130:159–63. https://doi.org/10.1016/j.molimm.2020.12.018.
Hiromatsu K, Dascher CC, Sugita M, Gingrich-Baker C, Behar SM, LeClair KP, et al. Characterization of Guinea-pig group 1 CD1 proteins. Immunology. 2002;106(2):159–72. https://doi.org/10.1046/j.1365-2567.2002.01422.x.
Gupta UD, Katoch VM, McMurray DN. Current status of TB vaccines. Vaccine. 2007;25(19):3742–51. https://doi.org/10.1016/j.vaccine.2007.01.112.
Arbues A, Aguilo JI, Gonzalo-Asensio J, Marinova D, Uranga S, Puentes E, et al. Construction, characterization and preclinical evaluation of MTBVAC, the first live-attenuated M. tuberculosis-based vaccine to enter clinical trials. Vaccine. 2013;31(42):4867–73. https://doi.org/10.1016/j.vaccine.2013.07.051.
Basaraba RJ. Experimental tuberculosis: the role of comparative pathology in the discovery of improved tuberculosis treatment strategies. Tuberculosis (Edinb). 2008;88(Suppl 1):S35–47. https://doi.org/10.1016/S1472-9792(08)70035-0.
Li YL, Chen BW, Xu M, Luo YA, Wang GZ, Shen XB, et al. A Guinea pig model of latent Mycobacterium tuberculosis H(3)(7)Rv infection. Zhonghua Jie He He Hu Xi Za Zhi. 2010;33(9):684–7.
Scanga CA, Flynn JL. Modeling tuberculosis in nonhuman primates. Cold Spring Harb Perspect Med. 2014;4(12):a018564. https://doi.org/10.1101/cshperspect.a018564.
Schmidt LH. Some observations on the utility of simian pulmonary tuberculosis in defining the therapeutic potentialities of isoniazid. Am Rev Tuberc. 1956;74(2 Part 2):138–53; discussion, 53–9. https://doi.org/10.1164/artpd.1956.74.2-2.138.
Schmidt LH. Studies on the antituberculous activity of ethambutol in monkeys. Ann N Y Acad Sci. 1966;135(2):747–58. https://doi.org/10.1111/j.1749-6632.1966.tb45520.x.
Good RC. Biology of the mycobacterioses. Simian tuberculosis: immunologic aspects. Ann N Y Acad Sci. 1968;154(1):200–13. https://doi.org/10.1111/j.1749-6632.1968.tb16710.x.
Sharpe SA, Eschelbach E, Basaraba RJ, Gleeson F, Hall GA, McIntyre A, et al. Determination of lesion volume by MRI and stereology in a macaque model of tuberculosis. Tuberculosis (Edinb). 2009;89(6):405–16. https://doi.org/10.1016/j.tube.2009.09.002.
Zhang J, Ye YQ, Wang Y, Mo PZ, Xian QY, Rao Y, et al. M. Tuberculosis H37Rv infection of Chinese rhesus macaques. J Neuroimmune Pharmacol. 2011;6(3):362–70. https://doi.org/10.1007/s11481-010-9245-4.
Mehra S, Golden NA, Dutta NK, Midkiff CC, Alvarez X, Doyle LA, et al. Reactivation of latent tuberculosis in rhesus macaques by coinfection with simian immunodeficiency virus. J Med Primatol. 2011;40(4):233–43. https://doi.org/10.1111/j.1600-0684.2011.00485.x.
Gormus BJ, Blanchard JL, Alvarez XH, Didier PJ. Evidence for a rhesus monkey model of asymptomatic tuberculosis. J Med Primatol. 2004;33(3):134–45. https://doi.org/10.1111/j.1600-0684.2004.00062.x.
Barclay WR, Anacker RL, Brehmer W, Leif W, Ribi E. Aerosol-induced tuberculosis in subhuman primates and the course of the disease after intravenous BCG vaccination. Infect Immun. 1970;2(5):574–82. https://doi.org/10.1128/iai.2.5.574-582.1970.
Walsh GP, Tan EV, dela Cruz EC, Abalos RM, Villahermosa LG, Young LJ, et al. The Philippine cynomolgus monkey (Macaca fascicularis) provides a new nonhuman primate model of tuberculosis that resembles human disease. Nat Med. 1996;2(4):430–6. https://doi.org/10.1038/nm0496-430.
Via LE, Weiner DM, Schimel D, Lin PL, Dayao E, Tankersley SL, et al. Differential virulence and disease progression following Mycobacterium tuberculosis complex infection of the common marmoset (Callithrix jacchus). Infect Immun. 2013;81(8):2909–19. https://doi.org/10.1128/IAI.00632-13.
Via LE, England K, Weiner DM, Schimel D, Zimmerman MD, Dayao E, et al. A sterilizing tuberculosis treatment regimen is associated with faster clearance of bacteria in cavitary lesions in marmosets. Antimicrob Agents Chemother. 2015;59(7):4181–9. https://doi.org/10.1128/AAC.00115-15.
Montali RJ, Mikota SK, Cheng LI. Mycobacterium tuberculosis in zoo and wildlife species. Rev Sci Tech. 2001;20(1):291–303. https://doi.org/10.20506/rst.20.1.1268.
Corbett EL, Watt CJ, Walker N, Maher D, Williams BG, Raviglione MC, et al. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Intern Med. 2003;163(9):1009–21. https://doi.org/10.1001/archinte.163.9.1009.
Chen CY, Huang D, Wang RC, Shen L, Zeng G, Yao S, et al. A critical role for CD8 T cells in a nonhuman primate model of tuberculosis. PLoS Pathog. 2009;5(4):e1000392. https://doi.org/10.1371/journal.ppat.1000392.
Langermans JA, Andersen P, van Soolingen D, Vervenne RA, Frost PA, van der Laan T, et al. Divergent effect of bacillus Calmette-Guerin (BCG) vaccination on Mycobacterium tuberculosis infection in highly related macaque species: implications for primate models in tuberculosis vaccine research. Proc Natl Acad Sci U S A. 2001;98(20):11497–502. https://doi.org/10.1073/pnas.201404898.
Lin PL, Rodgers M, Smith L, Bigbee M, Myers A, Bigbee C, et al. Quantitative comparison of active and latent tuberculosis in the cynomolgus macaque model. Infect Immun. 2009;77(10):4631–42. https://doi.org/10.1128/IAI.00592-09.
Lin PL, Rutledge T, Green AM, Bigbee M, Fuhrman C, Klein E, et al. CD4 T cell depletion exacerbates acute Mycobacterium tuberculosis while reactivation of latent infection is dependent on severity of tissue depletion in cynomolgus macaques. AIDS Res Hum Retroviruses. 2012;28(12):1693–702. https://doi.org/10.1089/AID.2012.0028.
Lin PL, Ford CB, Coleman MT, Myers AJ, Gawande R, Ioerger T, et al. Sterilization of granulomas is common in active and latent tuberculosis despite within-host variability in bacterial killing. Nat Med. 2014;20(1):75–9. https://doi.org/10.1038/nm.3412.
Pena JC, Ho WZ. Monkey models of tuberculosis: lessons learned. Infect Immun. 2015;83(3):852–62. https://doi.org/10.1128/IAI.02850-14.
Clark SO, Hall Y, Kelly DL, Hatch GJ, Williams A. Survival of Mycobacterium tuberculosis during experimental aerosolization and implications for aerosol challenge models. J Appl Microbiol. 2011;111(2):350–9. https://doi.org/10.1111/j.1365-2672.2011.05069.x.
Carlsson F, Kim J, Dumitru C, Barck KH, Carano RA, Sun M, et al. Host-detrimental role of Esx-1-mediated inflammasome activation in mycobacterial infection. PLoS Pathog. 2010;6(5):e1000895. https://doi.org/10.1371/journal.ppat.1000895.
Ribi E, Anacker RL, Barclay WR, Brehmer W, Harris SC, Leif WR, et al. Efficacy of mycobacterial cell walls as a vaccine against airborne tuberculosis in the rhesus monkey. J Infect Dis. 1971;123(5):527–38. https://doi.org/10.1093/infdis/123.5.527.
Yan G, Zhang G, Fang X, Zhang Y, Li C, Ling F, et al. Genome sequencing and comparison of two nonhuman primate animal models, the cynomolgus and Chinese rhesus macaques. Nat Biotechnol. 2011;29(11):1019–23. https://doi.org/10.1038/nbt.1992.
Lin PL, Coleman T, Carney JP, Lopresti BJ, Tomko J, Fillmore D, et al. Radiologic responses in Cynomolgus macaques for assessing tuberculosis chemotherapy regimens. Antimicrob Agents Chemother. 2013;57(9):4237–44. https://doi.org/10.1128/AAC.00277-13.
Lin PL, Flynn JL. Understanding latent tuberculosis: a moving target. J Immunol. 2010;185(1):15–22. https://doi.org/10.4049/jimmunol.0903856.
Gideon HP, Flynn JL. Latent tuberculosis: what the host "sees"? Immunol Res. 2011;50(2–3):202–12. https://doi.org/10.1007/s12026-011-8229-7.
Ramirez-Lapausa M, Menendez-Saldana A, Noguerado-Asensio A. Extrapulmonary tuberculosis. Rev Esp Sanid Penit. 2015;17(1):3–11. https://doi.org/10.4321/S1575-06202015000100002.
van der Burgt GM, Crawshaw T, Foster AP, Denny DJ, Schock A. Mycobacterium bovis infection in dogs. Vet Rec. 2009;165(21):634. https://doi.org/10.1136/vr.165.21.634.
Buddle BM, Mackintosh CG. Improving the diagnosis of bovine tuberculosis in farmed deer. Vet Rec. 2017;180(3):66–7. https://doi.org/10.1136/vr.j270.
Lopez Hernandez Y, Yero D, Pinos-Rodriguez JM, Gibert I. Animals devoid of pulmonary system as infection models in the study of lung bacterial pathogens. Front Microbiol. 2015;6:38. https://doi.org/10.3389/fmicb.2015.00038.
Ramos L, Obregon-Henao A, Henao-Tamayo M, Bowen R, Lunney JK, Gonzalez-Juarrero M. The minipig as an animal model to study Mycobacterium tuberculosis infection and natural transmission. Tuberculosis (Edinb). 2017;106:91–8. https://doi.org/10.1016/j.tube.2017.07.003.
Cerna P, O’Halloran C, Sjatkovska JO, Gunn-Moore DA. Outbreak of tuberculosis caused by Mycobacterium bovis in a cattery of Abyssinian cats in Italy. Transbound Emerg Dis. 2019;66(1):250–8. https://doi.org/10.1111/tbed.13010.
Machi T. Cat scratch disease showing clinical picture resembling tuberculous lymphadenitis: a case report. Kekkaku. 2001;76(7):545–8.
Atici S, Kadayifci EK, Karaaslan A, Toper MH, Celikel CA, Soysal A, et al. Atypical presentation of cat-scratch disease in an immunocompetent child with serological and pathological evidence. Case Rep Pediatr. 2014;2014:397437. https://doi.org/10.1155/2014/397437.
Pesciaroli M, Alvarez J, Boniotti MB, Cagiola M, Di Marco V, Marianelli C, et al. Tuberculosis in domestic animal species. Res Vet Sci. 2014;97(Suppl):S78–85. https://doi.org/10.1016/j.rvsc.2014.05.015.
Malik R, Wigney DI, Dawson D, Martin P, Hunt GB, Love DN. Infection of the subcutis and skin of cats with rapidly growing Mycobacteria: a review of microbiological and clinical findings. J Feline Med Surg. 2000;2(1):35–48. https://doi.org/10.1053/jfms.2000.0051.
Kaneene JB, Bruning-Fann CS, Dunn J, Mullaney TP, Berry D, Massey JP, et al. Epidemiologic investigation of Mycobacterium bovis in a population of cats. Am J Vet Res. 2002;63(11):1507–11. https://doi.org/10.2460/ajvr.2002.63.1507.
Eskandari E, Ahmadi Marzaleh M, Roudgari H, Hamidi Farahani R, Nezami-Asl A, Laripour R, et al. Sniffer dogs as a screening/diagnostic tool for COVID-19: a proof of concept study. BMC Infect Dis. 2021;21(1):243. https://doi.org/10.1186/s12879-021-05939-6.
Bijland LR, Bomers MK, Smulders YM. Smelling the diagnosis: a review on the use of scent in diagnosing disease. Neth J Med. 2013;71(6):300–7.
Barkham T, Taylor MB. Sniffing bacterial cultures on agar plates: a useful tool or a safety hazard? J Clin Microbiol. 2002;40(10):3877. https://doi.org/10.1128/JCM.40.10.3877.2002.
Szalus-Jordanow O, Augustynowicz-Kopec E, Czopowicz M, Olkowski A, Lobaczewski A, Rzewuska M, et al. Intracardiac tuberculomas caused by Mycobacterium tuberculosis in a dog. BMC Vet Res. 2016;12(1):109. https://doi.org/10.1186/s12917-016-0731-7.
Griffin JF, Mackintosh CG. Tuberculosis in deer: perceptions, problems and progress. Vet J. 2000;160(3):202–19. https://doi.org/10.1053/tvjl.2000.0514.
O’Reilly LM, Daborn CJ. The epidemiology of Mycobacterium bovis infections in animals and man: a review. Tuber Lung Dis. 1995;76(Suppl 1):1–46. https://doi.org/10.1016/0962-8479(95)90591-x.
Morris RS, Pfeiffer DU, Jackson R. The epidemiology of Mycobacterium bovis infections. Vet Microbiol. 1994;40(1–2):153–77. https://doi.org/10.1016/0378-1135(94)90053-1.
Paterson BM, Morris RS. Interactions between beef cattle and simulated tuberculous possums on pasture. N Z Vet J. 1995;43(7):289–93. https://doi.org/10.1080/00480169./1995.35908.
Sauter CM, Morris RS. Behavioural studies on the potential for direct transmission of tuberculosis from feral ferrets (Mustela furo) and possums (Trichosurus vulpecula) to farmed livestock. N Z Vet J. 1995;43(7):294–300. https://doi.org/10.1080/00480169./1995.35909.
Buddle BM, de Lisle GW, Griffin JF, Hutchings SA. Epidemiology, diagnostics, and management of tuberculosis in domestic cattle and deer in New Zealand in the face of a wildlife reservoir. N Z Vet J. 2015;63(Suppl 1):19–27. https://doi.org/10.1080/00480169.2014.929518.
Carter CE, Corrin KC, de Lisle GW, Kissling RC. Comparative cervical test in deer. In: Proceedings of New Zealand Veterinary Association Deer Branch; 1985. p. 80–87.
Griffin JF, Cross JP, Chinn DN, Rodgers CR, Buchan GS. Diagnosis of tuberculosis due to Mycobacterium bovis in New Zealand red deer (Cervus elaphus) using a composite blood test and antibody assays. N Z Vet J. 1994;42(5):173–9. https://doi.org/10.1080/00480169.1994.35815.
Whelan C, Shuralev E, O’Keeffe G, Hyland P, Kwok HF, Snoddy P, et al. Multiplex immunoassay for serological diagnosis of Mycobacterium bovis infection in cattle. Clin Vaccine Immunol. 2008;15(12):1834–8. https://doi.org/10.1128/CVI.00238-08.
Griffin JF, Mackintosh CG, Rodgers CR. Factors influencing the protective efficacy of a BCG homologous prime-boost vaccination regime against tuberculosis. Vaccine. 2006;24(6):835–45. https://doi.org/10.1016/j.vaccine.2005.07.033.
Gil O, Diaz I, Vilaplana C, Tapia G, Diaz J, Fort M, et al. Granuloma encapsulation is a key factor for containing tuberculosis infection in minipigs. PLoS One. 2010;5(4):e10030. https://doi.org/10.1371/journal.pone.0010030.
Dionne MS, Ghori N, Schneider DS. Drosophila melanogaster is a genetically tractable model host for Mycobacterium marinum. Infect Immun. 2003;71(6):3540–50. https://doi.org/10.1128/IAI.71.6.3540-3550.2003.
Igboin CO, Griffen AL, Leys EJ. The Drosophila melanogaster host model. J Oral Microbiol. 2012:4. https://doi.org/10.3402/jom.v4i0.10368.
Oh CT, Moon C, Choi TH, Kim BS, Jang J. Mycobacterium marinum infection in Drosophila melanogaster for antimycobacterial activity assessment. J Antimicrob Chemother. 2013;68(3):601–9. https://doi.org/10.1093/jac/dks425.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2023 The Author(s)
About this chapter

Cite this chapter
Li, H., Li, H. (2023). Animal Models of Tuberculosis. In: Christodoulides, M. (eds) Vaccines for Neglected Pathogens: Strategies, Achievements and Challenges . Springer, Cham. https://doi.org/10.1007/978-3-031-24355-4_7
Download citation
DOI: https://doi.org/10.1007/978-3-031-24355-4_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-24354-7
Online ISBN: 978-3-031-24355-4
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)