
Abstract
Minimally Invasive Surgery (MIS) instruments are patterned after conventional hand instruments to perform similar specific functions; they are designed to pass and perform through small diameter ports and at a distance to the target tissues. The development of instruments has evolved since the early period of MIS, starting from the use of rudimentary gynecologic instruments; at that time. Gynecology was the only specialty widely performing laparoscopic procedures. The evolution in design, ergonomics, and variety has been pivotal for advancing endo-laparoscopic surgery to perform more complex surgical procedures with safety and better outcome. Various evolving concepts of MIS like Single-site or reduced Surgery, Natural Orifice Transluminal Endoscopic Surgery (NOTES), Needlescopic Surgery, and Robotic-assisted Surgery have also pushed the development of features such as articulation control, pre-bent configuration, smaller diameter, and robotic instruments to meet specific needs.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Introduction
Minimally Invasive Surgery (MIS) instruments are patterned after conventional hand instruments to perform similar specific functions; they are designed to pass and perform through small diameter ports and at a distance to the target tissues. The development of instruments has evolved since the early period of MIS, starting from the use of rudimentary gynecologic instruments; at that time. Gynecology was the only specialty widely performing laparoscopic procedures. The evolution in design, ergonomics, and variety has been pivotal for advancing endo-laparoscopic surgery to perform more complex surgical procedures with safety and better outcome. Various evolving concepts of MIS like Single-site or reduced Surgery, Natural Orifice Transluminal Endoscopic Surgery (NOTES), Needlescopic Surgery, and Robotic-assisted Surgery have also pushed the development of features such as articulation control, pre-bent configuration, smaller diameter, and robotic instruments to meet specific needs.
A better understanding of the features, ergonomics, characteristics, and different instrumentations is crucial for any surgeon before embarking on basic or advanced laparoscopic surgery.
We can divide the instrumentations into three categories: access the cavity or workspace, maintain the working space, and perform the surgical procedures. Let us analyze the role of these groups.
The development of these devices has also evolved to respond to the requirements of new MIS concepts.
In the first two groups: access devices are meant to gain entry into the workspace (i.e., abdominal cavity, chest, pre-peritoneal space, etc.) while other devices are needed to maintain the space by the insufflated CO2 while allowing insertion of instruments necessary in the performance of surgery.
Access Devices: Role and Characteristic
Access devices’ primary purpose is to gain entry to the workspace, the insufflation of CO2, maintain a pressurized workspace, and serve as a conduit for instruments to pass through.
-
1.
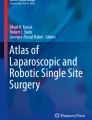
Veress needle. A specially designed instrument to enter the abdominal or thoracic cavity using the closed technique (Fig. 1). It consists of an outer sharp cutting needle and an inner blunt spring-loaded stylet. During insertion, the needle encounters resistance; the blunt stylet retracts, exposing the sharp outer sheath which facilitates penetration of the structure; when it enters a cavity, the blunt stylet springs forward beyond the outer sheath to protect the viscera within. Once proper intraperitoneal placement has been ascertained using accepted maneuvers, insufflation of the peritoneal cavity may be initiated and followed by the insertion of working ports.
-
2.
Hasson trocar. Composed of a cannula with an adjustable sliding cone and a blunt-tip trocar (Fig. 2). Intended to be inserted into the abdominal cavity after access is achieved with the open technique; the cone serves as a stopper preventing air leaks while the blunt trocar prevents visceral injury as it is inserted.
-
3.
Optical trocar. It is a specially designed trocar that is utilized to access the abdominal cavity (Fig. 3). It is beneficial in certain situations like obesity or when the access with Veress or open technique is at risk of injury. The trocar has a transparent tip that allows a view through. The trocar accommodates an endo-laparoscope (0° scope preferred), allowing visualization of each layer of the abdominal wall as it is inserted into the abdominal cavity. The trocar may have either a cutting or a dilating tip, with the latter preferred.
-
4.
Hand-assist port. Ports are designed to accommodate the passage of a hand (for assisting) while maintaining intraperitoneal pressure (Fig. 4).
-
5.
Single or Reduced Ports. These ports are specifically designed for the single or reduced port technique. They are introduced through a single access point and allow multiple instruments and camera endoscope to be inserted. There are reusable and disposable devices, with different diameters and sizes. Also, the type and number of instrumentations that can be inserted may vary. Fig. 5 shows Olympus Tri-port, a form of Single/Reduced port.

(a) Veress needle. (b) Needle tip magnified showing inner blunt spring-loaded tip

Hasson trocar

Optical trocars

Hand-assist port

Olympus Tri-port
Device to Maintain the Working Space
Trocars or Conventional ports. The trocar or port is generally composed of two parts: the outer cannula and the inner trocar. The outer cannula usually has a valve that allows entry of hand instruments while maintaining the workspace, and a stopcock allows the insufflation and evacuation of the workspace. Like hand instruments, these can be reusable or single-use, have specific features to the outer sheath (flexible, ridges, or fixation balloon), and have varying trocar tip designs with different penetrating capabilities (cutting or non-cutting). Maneuver during insertion through the abdominal wall: with long axis 90° to the wall, back and forth clockwise-counterclockwise rotation while slowly pushing in. Port can be held either two-handed (one hand on the head applying pushing and rotational force, while the second hand holds the cannula to prevent sudden slippage when the tip enters a cavity), or one-handed (the head in the palm with a finger or two along the cannula to act as a stopper when the tip enters a cavity)
-
(a)
Bladed/Cutting—facilitated by a blade under a spring-loaded cover (Fig. 6) that springs forward, covering the cutting blade and locking in place once the device enters the abdominal cavity protecting the viscera within.
-
(b)
Pyramidal—pyramidal tip is meant to expedite passage through tough tissue easier than the cone-tip, but with less trauma than a cutting-tip (Fig. 7).
-
(c)
Dilating /non-cutting Tip—are usually pointed conical tip trocars intended to push aside the tissue fibers without cutting (Fig. 8).

Showing the extended cutting blade of a trocar

Trocar with a pyramidal tip

Trocar with a conical tip
We will now analyze the variety and characteristics of the instrumentations most frequently utilized to perform procedures. Instrumentations have different ergonomics, and they are mainly designed to accomplish a task or a determined action. Any surgeon must make proper and correct use of each one.
Endo-Laparoscopic Instruments: The Basic
The laparoscopic hand instruments (Fig. 9) are generally composed of three parts/sections:

Expanded view of the parts of a laparoscopic instrument
-
1.
Handle—this part controls the instrument tip and its function; it has features that contribute to the additional functions of the instrument and configuration that allows for the user’s ergonomic preference.
-
(a)
Configuration/Design—the primary interface with the user provides control of the instrument’s jaw action and has varying designs that allow for user preference that enhance comfort and ease of use (Fig. 10).
-
(b)
Locking mechanism—provides securing mechanism for the jaws to minimize hand strain when grasping tissues for extended periods.
-
(c)
Rotation knob—provides the means to rotate the instrument tip 360° around its long axis.
-
(d)
Electro-surgical post connects either monopolar or bipolar cable from the electro-surgical device to provide tissue coagulation or cutting capability.
-
(a)
-
2.
Shaft—is a metal sheath through which the insert runs and connects to the instrument handle. Together with the insert, determine the instrument’s length, based on the distance to the target tissue (dependent on varying factors: adult (33 cm) vs pediatric (23 cm), nonobese vs obese (43 cm), or preferred point of access). This part is usually covered by a nonconductive material (silicone or plastic) to isolate the current passing from the electro-surgical post to the instrument tip and prevent collateral injuries.
-
3.
Instrument Insert/Tip—the main part that determines the function with specifically designed jaws.

Various handle designs in laparoscopic instruments
Concepts of Hand Instrument Variations
-
1.
Jaw Action
-
(a)
Double-action—both jaws of the tip move; it is the preferred action for dissectors as it allows for greater tissue separation and access to varying tissue planes (Fig. 11b).
-
(b)
Single-action—one jaw moves while the other remains fixed; the mechanism allows for the force applied via the handle to be concentrated on the mobile jaw providing a firm grip. In instruments intended for delicate functions, this allows the user to focus on the mobile jaw (Fig. 11a).
-
(a)
-
2.
Tip Function
-
(a)
Dissectors—are meant to expose, isolate, or separate tissue structures. The jaws are usually of the double-action type, fine-tipped, and with the curved jaws preferred by most users to allow better tip visualization. The most popular of which is the Maryland dissector (Fig. 12).
-
(b)
Graspers—are meant to hold on to structures to allow exposure, manipulation, or retraction. The jaws may be of atraumatic design for delicate tissues (Fig. 13), double- or single-action, with or without fenestration (for a more secure grip, by allowing the tissue to mold into the gaps), with or without teeth (affords secure grip on tougher tissues).
-
(c)
Scissors/Shears—primarily meant for cutting or sharp dissection, has varying designs for specific functions.
-
i.
Straight scissors—mainly for cutting and dissection (Fig. 14).
-
ii.
Curved scissors—preferred by most users, the curvature of the blade allows a better view of the tip (Fig. 15).
-
iii.
Serrated scissors—ridges on the blade minimizes tissue or suture slippage (Fig. 16).
-
iv.
Hook scissors—encircles the structure before cutting, assuring firm and solid grip (Fig. 17).
-
v.
Micro scissors—facilitates partial cutting of structures (Fig. 18).
-
i.
-
(a)
-
3.
Insulation—In MIS, electro-surgical energy use plays a crucial part in dissection and hemostasis. The nonconducting material (usually plastic or silicone) covering the instrument shaft prevents the conduction of electrical current to surrounding tissues and isolates the flow toward the instrument’s tip, allowing use even when the instrument shaft is in contact with other structures.
-
4.
Reusability
-
(a)
“Reusable” instruments are meant to be used multiple times. They are constructed of durable materials, usually more rigid, and are expected to withstand repeated use and cleaning and sterilization processing cycles. They are also designed to be readily dismantled to allow thorough cleaning and have replaceable parts for easy maintenance.
-
(b)
“Disposable” instruments are also termed “single-use,” they came about in response to the perceived high acquisition and maintenance cost of reusable instruments. They are usually manufactured from less costly materials, generally less robust, relatively flexible, cannot be dismantled for cleaning, and quickly wears down.
-
(c)
“Reposable” instruments arose from the combination of terms “reusable” and “disposable”; meant to describe the category of instruments having the beneficial characteristic of both. Reusable part (usually the handle) and disposable part (the insert and shaft, commonly scissors) components; supposed to integrate features: a sturdy instrument with low acquisition cost and eliminate the need for maintenance.
-
(a)

Jaw action of laparoscopic instruments

Maryland dissector tip

Fenestrated atraumatic grasper tip

Straight scissors

Curved scissors

Curved scissors with serrated blades

Hook scissors

Micro scissors
Specialized Endo-Laparoscopic Instruments
-
1.
Irrigation and Suction instruments—meant to evacuate fluid by suction and dislodge adherent debris using pressurized water. The suction tip usually has multiple fenestrations that not only facilitate suctioning but decrease the chance of obstruction by surrounding tissue (Fig. 19). Some are designed with an electro-surgical attachment that allows for simultaneous suctioning of fluids and coagulation of tissue, advantageous when the target area is constantly flooded.
-
2.
Knot pushers—are usually long rods with specially designed tips used to perform extracorporeal knot tying (Fig. 20a, b). The knots are thrown outside, utilizing this instrument to push the knot through the cannula and secure it inside.
-
3.
Needle drivers/holders—are intended solely for executing intra-corporeal suturing and knot tying. These instruments have single-action, tough and robust jaws and, on occasion, may have tungsten inserts or diamond coating to ensure surface hardness and secure grip on the needle and suture, a rigid and sturdy shaft that can withstand applied rotational forces, and a ratchet mechanism. Various jaw configurations are available: straight, curved, and self-aligning (designed to orient the needle perpendicular to the jaws); the most versatile being the straight jaws which allow needle positioning in variable orientation (Fig. 21).
-
4.
Retractors—similar to those used in open surgery, provide exposure by moving aside mobile structures such as small intestines, solid organs, or stomach. They may be hand-held or fixed to a bracket attached to the operating table.
-
(a)
The Nathanson retractor is designed to retract the liver (Fig. 22); it is inserted through an epigastric puncture site, maneuvered into position under the liver, and fixed to a bracket.
-
(b)
The Hand-held retractors—meant to be operated by an assistant, allows for repositioning as the procedure progresses, a dynamic retractor. Once the desired retraction is achieved, it may also be fixed to a table-attached bracket and becomes a static retractor.
-
(a)

Irrigation-suction instrument

(a) Knot-pusher instrument, (b) Various tip-design of knot-pushers

Needle handler

Nathanson retractor

Fan-retractor

Snake-retractor
Further Reading
Ahmed HO. Color atlas of laparoscopy. Suleimani: University of Suleimani; 2008. p. 31–140.
Adrales G, Park A. Technological and instrumentation aspects of laparoscopic hernia surgery. In: LeBlanc K, editor. Laparoscopic hernia surgery: an operative guide. Oxford University Press, Inc; 2003. p. 7–15.
Carol EH, Scott-Conner. The SAGES manual. New York: Springer-Verlag; 1998.
Goel A. Laparoscopic hand instruments, accessories and ergonomics. In: Kriplani A, Bhatia P, Prasad A, Govil D, Garg HP, editors. Comprehensive laparoscopic surgery. New Delhi: Sagar Printers; 2007. p. 9–19.
Palanivelu C. CIGES atlas of laparoscopic surgery. New Delhi: Jaypee Brothers Medical Publishers, Ltd.; 2000.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2023 The Author(s)
About this chapter

Cite this chapter
Lee-Ong, A., Buenafe, A.A. (2023). Instrumentations and Access Devices. In: Lomanto, D., Chen, W.TL., Fuentes, M.B. (eds) Mastering Endo-Laparoscopic and Thoracoscopic Surgery. Springer, Singapore. https://doi.org/10.1007/978-981-19-3755-2_9
Download citation
DOI: https://doi.org/10.1007/978-981-19-3755-2_9
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-19-3754-5
Online ISBN: 978-981-19-3755-2
eBook Packages: MedicineMedicine (R0)