
Abstract
This chapter provides structured summaries of all 25 currently published national EQ-5D-5L value sets. The summaries were developed by extracting information from the published manuscripts of each value set and conducting secondary data analyses of the original valuation data generated in each country/region. The summaries include the mathematical formula for the preferred model for each national value set; information on the representativeness of the samples that were used to generate the value set; the mean values observed for each health state valued using composite time trade-off, the distribution of responses in the discrete choice experiment; information on the number of interviewers and whether any interviewer effects were present in the valuation data; key characteristics of the predicted values and relative importance of the EQ-5D-5L dimensions; and information on the uptake of the value set by local decision makers and health technology assessment bodies. This chapter serves as a compendium of EQ-5D-5L value sets, which may inform users of these value sets about the characteristics of all published EQ-5D-5L value sets.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others
4.1 Introduction
This chapter provides summary-level information on the currently published EQ-5D-5L value sets. The countries/regions are reported alphabetically, by study wave. This means that the oldest studies are reported first, and the newest studies are reported last. Figure 4.1 provides an overview of the 25 studies which are included, by wave and protocol version.

Overview of EQ-VT studies by study wave and protocol version
Most of the information reported in this chapter was extracted from the manuscripts in which these value sets were published. However, in some cases, some of the relevant information was not included in the published papers. In these cases, we have undertaken secondary analyses of the data sets, with permissions from the study authors, using the methods reported below.
From each value set, we have extracted the mathematical formula for the preferred model for the value set, presented as V(x) and present the relative weights for each of the different dimension levels (20 parameters). The parameter therefore represents the decrement from level 1 to the respective level. We also present some other key characteristics of the value sets, such as the order of importance of each of the 5 dimensions of the EQ-5D-5L, the value for the worst and best health states, as well as the value for the best suboptimal health state. Lastly, we report key aspects of the study, such as the time frame in which the valuation data was collected, the sample size, sampling frame and sample characteristics.
4.2 Methods
As each study has valued the same 86 health states using cTTO using the study design discussed in Chap. 3,Footnote 1 we report the arithmetic means and standard errors for each of these 86 health states in each country/region. The means are calculated for the same sample used in modelling the value set in each case i.e., following any exclusions which may have been made, which we describe. For studies in which the feedback module was used, as discussed in Chap. 2, the arithmetic means are calculated after the exclusion of any flagged responses.
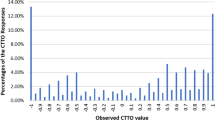
For the DCE data, we report the proportion of respondents choosing EQ-5D-5L state A by the difference in level sum score between the two states included in the pair. Here, the level sum score is merely the sum of the levels of an EQ-5D-5L health state to give a broad indication of the severity of the state. For example, for state 12312, the level sum score would be 1+2+3+1+2=9. For example, the difference in level sum scores within a DCE choice pair with alternative A being 12341 and alternative B being 22335 is then 11 − 15= −4. We then report the percentage of responses choosing A when the difference in level sum scores equals −4. This will be a mix of choice pairs, as various choice pairs will have a level sum score difference of −4.
The modelling and other data analysis strategies used by the value set research team in each country/region differ somewhat. Therefore, we report the following for each study: (1) data exclusion criteria and the number of excluded responses/respondents; (2) interviewer effects; and (3) a description of modelling choices. To determine whether there are any interviewer effects, we partition the variance in the valuation data into variance related to interviewers i, respondents j and responses k, and determine the relative share of variance attributed to differences between interviewers. This is done by employing a mixed model in the form of equation 4.1 to each of the valuation datasets:
This model assumes there is a mean value β0 for all health states, which varies by interviewer (γi), respondent (μij) and health state valued (εijk). Here, β0 is a fixed effects parameter, while all others are random effects parameters. We then assume that \( {\gamma}_i\sim N\left(0,{\sigma}_{\gamma}^2\right) \), \( {\mu}_{ij}\sim N\left(0,{\sigma}_{\mu}^2\right) \) and \( {\varepsilon}_{ij}\sim N\left(0,{\sigma}_{\varepsilon}^2\right) \).Footnote 2
To determine the share of variance attributed to differences between interviewers, we then calculate the Intra Class Correlation (ICC) coefficient as in Eq. 4.2Footnote 3:
The relative importance of the EQ-5D-5L dimensions was determined by taking the sum of the coefficients for one dimension, and dividing this by the sum of the coefficients for all coefficients. This measure can be seen as the size of the share of the total weight assigned to all dimension levels, and takes into account the relative importance for each dimension at all levels.
Finally, depending on the availability of the relevant information, we report the uptake of the value set by local HTA agencies, as reported in the manuscript or drawing on information provided by the principal investigators of the valuation studies to the authors of this book.
For each value set, we include full reference details and any other relevant literature directly related to the value set. Permission to reproduce these value sets and related information have been granted by the journals in which they are published, and access to the data to facilitate secondary analyses reported in this chapter was granted by the principal investigators, on behalf of the study teams in each case.
4.3 Country-by-Country Overview of Value Sets
4.3.1 Wave 1
4.3.1.1 Country/Region: Canada (Table 4.1)
The mathematical representation of the model for health state X isFootnote 4:
-
(i)
Date/wave of study
Data were collected in the first wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 1.0. Additionally, traditional TTO was used as elicitation technique to supplement the EQ-VT. Interviews were conducted in 2012.
-
(ii)
Sample size; sample frame
1209 interviews with the general population were conducted in three English speaking metropolitan areas: Vancouver, Hamilton and Edmonton, and French speaking respondents were recruited in Montreal. Quota sampling with respect to age, gender, and education was applied. Of the 1073 respondents included in the final value set, 55.5% were female and 44.5% were male. The age distribution of the respondents was:
18–24 years | 12.5% |
25–29 years | 8.0% |
30–39 years | 14.6% |
40–49 years | 14.8% |
50–64 years | 31.6% |
65–74 years | 13.1% |
75+ years | 5.4% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the Canadian population in terms of age (over 18 years), gender, marital status, born in Canada and language spoken at home. The sample was more educated, but had lower incomes compared to the general population in Canada (Table 4.2).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.3)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.2)

Proportions choosing A based on relative severities of A and B. (DCE data were collected during the study, but not used in the modelling stage)
-
(vi)
Exclusion criteria
A share of respondents with inconsistent responses were excluded. Inconsistencies were defined as strict dominance (e.g., assigning a higher value to state 11411 compared to state 11311). For each respondent, the number of dominated states by the very mild health states (with just one deviation from full health, e.g., 11121) was counted. Respondents were excluded if they assigned (a) the same or a lower value to at least half of the states that were dominated or (b) the same or a lower value for the very mild health state compared with the pits state (55555). 136 respondents met these exclusion criteria.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1209 interviews were conducted by 8 interviewers. The variance of the responses included in the final value set can be partitioned into variance related to differences between interviewers (2.6%), respondents (35.8%) and responses (61.6%).
-
(viii)
Description of modelling choices
The Canadian EQ-5D-5L value set was based on a combination of cTTO and conventional TTO data. The authors chose a final model that included a linear parameter for each dimension, with each dimension variables having levels 1, 2, 3, 4 and 5. Furthermore, the authors added dummy variables for each of the 5 dimensions, that equal 1 if that dimension reports level 4 or 5 problems, and 0 otherwise. Lastly, a term was added that represents the square of the number of dimensions reporting level 4 or 5 problems, beyond the first. The estimated model used a Tobit link function, assuming censoring at 0 for negative values and values equal to 0 in the cTTO, and assumed a random intercept for each respondent.
- (ix)

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
Canadian Agency for Drugs and Technologies in Health (CADTH) is the national HTA body that reviews and makes reimbursement recommendations to the public insurance programs across Canada. Cost-utility analysis (CUA) is a recommended type of economic evaluation for reimbursement applications. Validated generic health state classification systems with Canadian-specific value sets are recommended for the estimation of QALYs. Although there is no preference for any specific instrument, the EQ-5D-5L has become one of the commonly used instruments in clinical trials and economic evaluations.
-
(xi)
Reference(s) of value set
Xie F, Pullenayegum E, Gaebel K, Bansback N, Bryan S, Ohinmaa A, Poissant L, Johnson JA (2016) A time trade-off-derived value set of the EQ-5D-5L for Canada. Med Care 54(1):98–105
Further Literature
-
Statistics Canada (2006) 2006 Census of Canada. https://www.statcan.gc.ca/. Accessed 14 July 2021
-
Statistics Canada (2011) https://www12.statcan.gc.ca/census-recensement/2011/dp-pd/tbt-tt/Index-eng.cfm. Accessed 28 July 2021
4.3.1.2 Country/Region: China (Table 4.5)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the first wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 1.0. Interviews were conducted in 2012.
-
(ii)
Sample size; sample frame
1332 interviews with the general population were conducted in five urban areas in different parts of China: Beijing, Chengdu, Guiyang, Nanjing and Shenyang. Within these cities, respondents were sampled to represent these cities with respect to age, gender and educational level using a nonprobability sampling strategy. Of the 1271 respondents included in the final value set, 49.9% were female and 50.1% were male. The age distribution of the respondents was:
18–24 years | 16.5% |
25–29 years | 8.1% |
30–39 years | 19.2% |
40–49 years | 21.4% |
50–64 years | 25.9% |
65–74 years | 6.2% |
75+ years | 2.7% |
-
(iii)
Representativeness of achieved sample (Table 4.6)
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.7)
-
(v)
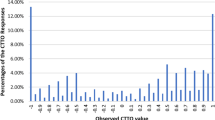
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.4)

Proportions choosing A based on relative severities of A and B

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(vi)
Exclusion criteria
Respondents that were younger than 18 years old were excluded (n=25). Another 36 respondents were excluded as they did not finish the interview.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1332 interviews were conducted by 20 interviewers. The variance of the responses included in the final value set can be partitioned into variance related to differences between interviewers (2.4%), respondents (28.8%) and responses (68.8%).
-
(viii)
Description of modelling choices
The Chinese EQ-5D-5L value set was based on cTTO data only. The selected model was an 8-parameter multiplicative model with a random intercept, in which 5 coefficients are estimated for the EQ-5D-5L’s 5 dimensions, and 3 coefficients are estimated for the 3 intermediate levels of the EQ-5D-5L (2,3 and 4), representing level weights. For levels 1 and 5, these are assumed to be 0 and 1, respectively. The predicted coefficients were rescaled by (1-intercept). The eight-parameter model can be converted to 20 parameters, as presented in Table 4.8 for consistency purposes in this chapter.
- (ix)
-
(x)
Uptake by local HTA/health care decision makers
There is currently no HTA agency in China. There are only academic methodology Pharmacoeconomic/Health Technology Assessment guidelines, (China Guidelines for Pharmacoeconomic Evaluations Writing Group, 2019) but there are no recommendations about which specific health related quality of life instruments are preferred for use.
-
(xi)
Reference(s) of value set
Luo N, Liu G, Li M, Guan H, Jin X, Rand-Hendriksen K (2017) Estimating an EQ-5D-5L value set for China. Value Health 20(4):662–669
Further Literature
-
Guidelines for Evaluation of Chinese Pharmacoeconomics (2019) China Guidelines for Pharmacoeconomic Evaluations Writing Group http://proa28198.pic40.websiteonline.cn/upload/0ikw.pdf. Accessed 14 July 2021
-
China Statistical Yearbook (2011) Population statistics. http://www.stats.gov.cn/tjsj/ndsj/2012/indexeh.htm. Accessed 15 July 21
4.3.1.3 Country/Region: England (Table 4.9)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the first wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 1.0. Interviews were conducted between November 2012 and May 2013.
-
(ii)
Sample size; sample frame
1004 interviews were conducted (996 respondents completing the valuation tasks in full) with the general population. A sample of 2020 addresses from 66 primary sampling units (based on postcode sectors) across England was randomly selected, using the Post Office small user Postcode Address File as the sampling frame. The sample was intended to be representative of adults aged 18 years and over living in private residential accommodation in England.
Of the 912 respondents included in the analysis, 59.3% were female and 40.7% were male. The age distribution of the 912 respondents was:
18–24 years | 5.37% |
25–29 years | 6.14% |
30–39 years | 18.75% |
40–49 years | 20.61% |
50–64 years | 23.14% |
65–74 years | 12.94% |
75+ years | 13.05% |
-
(iii)
Representativeness of achieved sample
The study sample was broadly representative for the English population in terms of age (over 18 years), sex and employment status. However, compared to the general population, the sample included a larger proportion of those aged over 75 and retired and a smaller proportion of younger individuals and males (Office for National Statistics 2011) (Table 4.10).
-
(iv)
Mean observed cTTO values by EQ-5D-5L state (Table 4.11)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.6)

Proportions choosing A based on relative severities of A and B
-
(vi)
Exclusion criteria
Twenty-three participants (2.3%) gave all 10 health states the same value, and 61 participants (6.1%) valued 55555 no lower than the value they gave to the mildest health state. Excluding these participants gave a core modelling dataset of 912 participants (9120 cTTO observations). No DCE data were excluded.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1004 interviews were conducted by 48 interviewers. Primary data collection was carried out in England by the market research company Ipsos MORI. The valuation data were collected via face-to-face interviews in respondents' homes.
The variance of the responses (following exclusions) can be partitioned into variance related to differences between interviewers (5.39%), respondents (32.46%), and responses (62.15%).
-
(viii)
Description of modelling choices
The England EQ-5D-5L value set was based on 20-parameter hybrid model, combining both cTTO and DCE data. cTTO data were treated as being censored at −1 and at 1 (to account for asymmetry in the error distributions) and, for specific responses, at 0 (e.g., for respondents who gave a value of 0 for more than one health state, including 55555). Heterogeneity was addressed via three latent classes, accounting for different groups of respondents differing in their use of the scale. The latent class coefficients act to apply an adjustment across all dimensions/level coefficients; the value set reported in Table 4.12 above simplifies the presentation of the value set by reporting the coefficients for dimensions/levels after the application of the latent class coefficients.
- (ix)

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
The value set was subject to a ‘quality assurance’ commissioned by the Department of Health for England from the Economic Evaluation Policy Research Unit (EEPRU). EEPRU’s critique is summarised in Hernandez-Alava et al. (2020) and a response from the authors is provided in van Hout et al. (2020). In response to concerns about data quality raised by EEPRU, NICE (2019) issued a position statement indicating it did not recommend use of the value set for England, recommending instead that EQ-5D-5L data be mapped to the EQ-5D-3L using the crosswalk published by van Hout et al. (2012) and the Dolan (1997) UK value set for the EQ-5D-3L be used. A new value set – for the UK, rather than for England – has been commissioned and NICE will review its policy once that study is complete (expected in 2022).
-
(xi)
Reference(s) for this value set
Feng Y, Devlin N, Shah K, Mulhern B, van Hout B (2018) New methods for modelling EQ-5D-5L value sets: an application to English data. Health Econ 27(1):23–38
Devlin N, Shah K, Mulhern B, Feng Y, van Hout B (2018) Valuing health related quality of life: an EQ-5D-5L value set for England. Health Econ 27(1): 7–22.
Further Literature
-
Dolan P (1997) Modeling valuations for EuroQol health states. Med Care 35(11):1095–1108
-
Hernandez-Alava M, Pudney S, Wailoo A (2020) The EQ-5D-5L value set for England: findings of a quality assurance program. Value Health 23(5):642–648
-
National Institute for Health and Care Excellence (2019) Position statement on the use of the EQ-5D-5L valuation set for England. www.nice.org.uk/about/what- we-do/our-programmes/nice-guidance/technology-appraisal-guidance/eq-5 d-5l. Accessed 14 June 2021
-
Office for National Statistics (2011) Census: Digitised boundary data (England and Wales) [computer file]. UK Data Service Census Support. http://edina.ac.uk/ukborders. Accessed 15 June 2021
-
van Hout B, Janssen M, Feng Y, Kohlmann T, Busschbach J, Golicki D, Lloyd A, Scalone L, Kind P, Pickard AS (2012) Interim Scoring for the EQ-5D-5L: Mapping the EQ-5D-5L to EQ-5D-3L Value Sets. Value Health 15(5):708–715.
-
van Hout B, Mulhern B, Feng Y, Shah K, Devlin N (2020) The EQ-5D-5L Value Set for England: Response to the “Quality Assurance”. Value Health 23(5):649–655
4.3.1.4 Country/Region: Netherlands (Table 4.13)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the first wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 1.0. Interviews were conducted in the fall of 2012.
-
(ii)
Sample size; sample frame
1003 interviews with the general population were conducted in five cities and surrounds located in different parts of Netherlands: Utrecht, Rotterdam, Maastricht, Enschede and Groningen. Strata-based sampling with respect to age, gender and educational level as recorded by the by Statistics Netherlands (Centraal Bureau voor de Statistiek 2012). Of the 979 respondents included in the final value set, 50.85% were female and 49.15% were male. The age distribution of the respondents was:
18–24 years | 11.91% |
25–29 years | 6.71% |
30–39 years | 13.71% |
40–49 years | 20.62% |
50–64 years | 28.53% |
65–74 years | 13.91% |
75+ years | 4.60% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the Dutch population in terms of age (except for the age group 80 and older), gender, education, and employment status (Table 4.14).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.15)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.8)

Proportions choosing A based on relative severities of A and B
-
(vi)
Exclusion criteria
cTTO data were excluded when the task was not finished or when interviewers had indicated that the respondent had clearly not understood the task. Furthermore, respondents that gave the same value to all health states in the cTTO tasks were excluded. In total, 13 respondents were excluded from analysis of the cTTO data. In addition, no data were obtained from another 11 respondents, due to a loss of data caused by technical issues, respondents being unable to start the valuation tasks due to technical problems, the absence of an interviewer, unwillingness to participate after being informed about the topic of research and other and unknown reasons.
-
(vii)
Number of interviewers; Interviewer effects Footnote 5
In total, 1003 interviews were conducted by 21 interviewers.
-
(viii)
Description of modelling choices
The Dutch EQ-5D-5L value set was based on the cTTO data only. The selected model was a Tobit model, that accounts for censoring at −1. Levels 4 and 5 were collapsed for the self-care and usual activities dimensions, as they were ordered inconsistently in other models.
- (ix)

Value decrements across dimensions. (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
Cost-utility analysis (CUA) is required by the Dutch regulatory body, Zorg Instituut Nederland (2016). For QALYs, the use of the EQ-5D-5L and the accompanying Dutch value set is recommended.
-
(xi)
Reference(s) of value set
Versteegh MM, Vermeulen KM, Evers SMAA, De Wit GA, Prenger R, Stolk EA (2016) Dutch tariff for the five-level version of EQ-5D. Value Health 19(4):343–352
Further Literature
-
Versteegh M, Knies S, Brouwer W (2016) From good to better: new Dutch guidelines for economic evaluations in healthcare. Pharmacoeconomics 34(11):1071–1074
-
Zorginstituut Nederland (2016) Guideline for economic evaluations in healthcare. https://english.zorginstituutnederland.nl/publications/reports/2016/06/16/guideline-for-economic-evaluations-in-healthcare. Accessed 12 May 2021
-
Statistics Netherlands (Centraal Bureau voor de Statistiek) (2012) Dutch Population data. https://www.cbs.nl. Accessed 14 July 2021
4.3.1.5 Country/Region: Spain (Table 4.17)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the first wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 1.0. Interviews were conducted in June and July 2012.
-
(ii)
Sample size; sample frame
1000 interviews with the general population were conducted, stratified over all provinces of Spain. Within these provinces, respondents were sampled to represent the age and gender distribution of that province. Of the 973 respondents included in the final value set, 52.4% were female and 47.6% were male. The age distribution of the respondents was:
18–24 years | 11.7% |
25–29 years | 15.1% |
30–39 years | 22.9% |
40–49 years | 14.8% |
50–64 years | 19.0% |
65–74 years | 11.1% |
75+ years | 5.3% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the Spanish population in terms of age (over 18 years) and gender (Table 4.18).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.19)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.10)

Proportions choosing A based on relative severities of A and B
-
(vi)
Exclusion criteria
Respondents that valued all health states in the cTTO tasks as equal to dead were excluded. Furthermore, respondents that had a positive slope on the regression between respondent’s cTTO values and level sum score were excluded. 27 out of 1000 respondents were excluded. No DCE data were excluded from the analysis.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1000 interviews were conducted by 33 interviewers. The variance of the responses included in the final value set can be partitioned into variance related to differences between interviewers (7.3%), respondents (31.9%), and responses (60.8%).
-
(viii)
Description of modelling choices
The Spanish EQ-5D-5L value set was based on a hybrid model combining a conditional logit model for the DCE data and a censored at −1 Tobit model for the cTTO data, correcting for heteroskedasticity. Furthermore, cTTO responses were treated as intervals rather than point responses. For respondents that were not shown the WTD task in the explanations (see Chap. 2 for more details), the data were considered to be censored at 0. The intercept was constrained in the final model, as it was not statistically significant.
- (ix)

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
Cost-utility analysis (CUA) is currently not mandatory in pharmacoeconomics and health technology assessment reports either by AEMPS (Agencia Española de Medicamentos y Productos Sanitarios), or RedETS (Red Española de Agencias de Evaluación de Tecnologías Sanitarias y Prestaciones del Sistema Nacional de Salud); the agencies that provide evidence for reimbursement decisions on drugs and technical devices, respectively, in Spain. However, use of CUA is demanded by the State Health Authority in the assessment process of national Public Health programs such as Population Screening or Vaccination programs.
-
(xi)
Reference(s) of value set
Ramos-Goñi JM, Craig BM, Oppe M, Ramallo-Fariña Y, Pinto-Prades JL, Luo N, Rivero-Arias O (2018) Handling data quality issues to estimate the Spanish EQ-5D-5L value set using a hybrid interval regression approach. Value Health 21(5):596–604
Further Literature
-
Ramos-Goñi JM, Pinto-Prades JL, Oppe M, Cabasés JM, Serrano-Aguilar P, Rivero-Arias O (2017) Valuation and modeling of EQ-5D-5L health states using a hybrid approach. Med Care 55(7):e51–e58
-
Spanish Ministry of Health (2012) Spanish national health survey 2011/2012.
-
https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2011.htm. Accessed 13 July 2021
4.3.2 Wave 2
4.3.2.1 Country/Region: Japan (Table 4.21)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the second wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 1.1. Interviews were conducted between March and June 2014.
-
(ii)
Sample size; sample frame
1098 interviews with the adult general population > 20 years of age were conducted in five cities in Japan: Tokyo, Okayama, Nagoya, Osaka, and Niigata. Respondents were recruited by a research company (ANTE-RIO Inc.) that sampled approximately 200 respondents at each location. The sample number was not determined on the basis of statistical considerations; respondents were stratified by sex and age group in each location to collect the same number in each cell.
Following the application of quality control, data from respondents interviewed by three interviewers were excluded from analysis. Of the 1026 respondents included in the analysis, 49.8% were female and 50.2% were male. The age distribution of the respondents was:
18–24 years | 10.33% |
25–29 years | 9.65% |
30–39 years | 19.98% |
40–49 years | 19.88% |
50–64 years | 29.24% |
65–74 years | 9.75% |
75+ years | 1.17% |
-
(iii)
Representativeness of achieved sample
The study sample was indicated to be broadly representative of the adult general public of Japan – however the paper does not report descriptive statistics for the general population to enable direct comparison with the characteristics of the analysis sample. The sample characteristics are provided in Table 4.22.
-
(iv)
Mean observed cTTO values by EQ-5D-5L state (Table 4.23)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.12)

Proportions choosing A based on relative severities of A and B
-
(vi)
Exclusion criteria
Quality control flagged three interviewers as failing to comply with the protocol; some or all of the data from the 72 respondents who were interviewed were excluded from the analysis data set.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1098 interviews were conducted by 31 interviewers. The variance of the responses can be partitioned into variance related to differences between interviewers (0.95%), respondents (38.77%), and responses (60.28%).
-
(viii)
Description of modelling choices
The preferred value set is modelled using only cTTO data. The data were analysed by a linear mixed model with “1 - QOL score” as the dependent variable. To account for the intra-respondent correlation, a constant term and dummy variables representing the levels of the five dimensions were treated as fixed effects and the respondents were treated as random effects.

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
According to Sect. 8.2.1 of the Japanese HTA Guidelines, “If Japanese quality of life scores are newly collected for a cost-effectiveness analysis, the use of preference-based measures with a value set developed in Japan using TTO (or mapped onto a TTO score) is recommended as the first choice." (C2H. 2019) The characteristics of the Japanese EQ-5D-5L reported here therefore meets the stated requirements of Japan’s HTA body, although it is unclear how often it has been used in evidence submitted to it.
-
(xi)
Reference(s) for this value set
Shiroiwa T, Ikeda S, Noto S, Igarashi A, Fukuda T, Saito S, Shimozuma K (2016) Comparison of value set based on DCE and/or TTO data: scoring for EQ-5D-5L health states in Japan. Value Health 19(5): 648–655
Further Literature
-
Center for Outcomes Research and Economic Evaluation for Health, National Institute of Public Health (C2H) (2019) Guideline for Preparing Cost-Effectiveness Evaluation to the Central Social Insurance Medical Council. https://c2h.niph.go.jp/tools/guideline/guideline_en.pdf. Accessed 16 June 2021
-
Ministry of Health, Labour and Welfare (2018) Vital Statistics. https://www.mhlw.go.jp. Accessed 29 July 2021
-
Statistics of Japan (2010) 2010 Population Census. https://e-stat.go.jp. Accessed 29 July 2021
4.3.2.2 Country/Region: Korea (Table 4.25)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the second wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 1.1. Interviews were performed between August 9 and November 13, 2013.
-
(ii)
Sample size; sample frame
Sampling was performed using a multistage stratified quota method. A sample quota was assigned to each of the 15 regions according to population structure (population in region, sex, age, and education level), as defined in the June 2013 resident registration data available through the Ministry of Administration and Security, South Korea.
Of the 1080 respondents included in the analysis, 50.6% were female and 49.4% were male.
The age distribution of the respondents was:
18–24 years | 8.98% |
25–34 years | 9.35% |
35–44 years | 19.35% |
45–54 years | 21.30% |
55–64 years | 33.33% |
65–74 years | 6.94% |
75+ years | 0.74% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the Korean population in terms of age (over 18 years), sex, education and employment status (Table 4.26).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.27)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.14)

Proportions choosing A based on relative severities of A and B
-
(vi)
Exclusion criteria
Five respondents who responded with the same answer for all 10 health states of cTTO were excluded from the modelling dataset.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1080 interviews were conducted by 27 interviewers. The variance of the responses can be partitioned into variance related to differences between interviewers (12.54%), respondents (20.69%), and responses (66.77%).
-
(viii)
Description of modelling choice
The value set was based on cTTO data only, using 20 dummy variables (4 levels for each of 5 dimensions). Three criteria were used to select the final model (1) the model must demonstrate logically consistent predictions; (2) goodness of fit of the model, judged using mean absolute error (MAE), generalized R2 and the number of health states with absolute error <0.05 or 0.1; and (3) where models with similar MAEs were consistent, the simplest model was selected to maintain parsimony. The final model includes a constant, and a term that picked up whether any dimension in the state was at a level 4 or 5.
- (ix)

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
CUA is currently the preferred form of economic evaluation in the 3rd version of Pharmacoeconomic Guideline revised by HIRA (Health Insurance Review Agency), the institute that assesses the cost-effectiveness of healthcare services to determine whether to include the service into the benefit package and decides the reimbursement price of the service (HIRA 2021), in 2021. There is no preference for a specific multi-attribute utility instrument but the recommended source of values is a representative sample of the general population, preferably Korean (Bae et al. 2013). For EQ-5D, value sets for both 3-level version and 5-level version were developed from the general population in Korea (Jo et al. 2008; Lee et al. 2009; Kim et al., 2016) and those instruments have been applied for economic evaluations informing the reimbursement decision making regarding new drugs.
-
(xi)
Reference(s) for this value set
Kim SH, Ahn J, Ock M, Shin S, Park J, Luo N, Jo MW (2016) The EQ-5D-5L valuation study in Korea. Qual Life Res 25(7):1845–1852
Further Literature
-
Health Insurance review agency (2021) http://www.hira.or.kr/dummy.do?pgmid=HIRAJ010000009001 (Korean) Accessed 28 July 2021
-
Bae S, Lee S, Bae EY, Jang S (2013) Korean guidelines for pharmacoeconomic evaluation (second and updated version): consensus and compromise. Pharmacoeconomics 31(4):257–267
-
Jo MW, Yun SC, Lee SI (2008) Estimating quality weights for EQ-5D health states with the time trade-off method in South Korea. Value Health 11(7):1186–1189
-
Lee YK, Nam HS, Chuang LH, Kim KY, Yang HK, Kwon IS, Kind P, Kweon SS, Kim YT (2009) South Korean time trade-off values for EQ-5D health states: modeling with observed values for 101 health states. Value Health 12(8):1187–1893
4.3.2.3 Country/Region: Thailand (Table 4.29)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the second wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 1.1. Interviews were conducted between August 2013 and January 2014.
-
(ii)
Sample size; sample frame
1207 interviews with the general population were conducted in the capital Bangkok and the following 11 provinces: Sing Buri, Trat, Suphan Buri, Chiang Mai, Chiang Rai, Sukhothai, Surin, Nong Bua Lam Phu, Roi Et, Krabi, and Nakhon Si Thammarat. Within these provinces, probability-based sampling was used to select geographical subunits, from each of which 10 respondents were selected using quota sampling with respect to age and gender. Of the 1207 respondents included in the final value set, 51.6% were female and 48.4% were male. The age distribution of the respondents was:
18–24 years | 12.8% |
25–29 years | 8.0% |
30–39 years | 21.7% |
40–49 years | 22.6% |
50–64 years | 25.4% |
65–74 years | 8.0% |
75+ years | 1.4% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the Thai population in terms of age (over 18 years), gender, residential area, and number of children (Table 4.30).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.31)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.16)

Proportions choosing A based on relative severities of A and B
-
(vi)
Exclusion criteria
cTTO responses were excluded if (1) a respondent assigned the same value to all 10 states valued, (2) a respondent had a positive slope on the regression between respondent’s cTTO values and level sum score and (3) there were severe irrational responses, defined as major inconsistent responses (e.g. severe dominance violations). Two respondents were excluded from analysis. No DCE data were excluded from the analysis.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1207 interviews were conducted by 6 interviewers. The variance of the responses included in the final analysis can be partitioned into variance related to differences between interviewers (1.8%), respondents (17.1%) and responses (81.1%).
-
(viii)
Description of modelling choices
The Thai EQ-5D-5L value set was based on a hybrid model combining a conditional logit model for the DCE data and a censored at −1 Tobit model for the cTTO data, correcting for heteroskedasticity. The intercept was constrained in the final model.
- (ix)

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
Economic evidence is one type of evidence to be considered during the decision-making process for both pharmaceutical and non-pharmaceutical interventions in Thailand (Leelahavarong et al. 2019). Cost-utility analysis (CUA) using QALYs is required for economic evidence (such as when considering high-cost medicines for public funding). EQ-5D-5L and its value set are recommended in the National Health Technology Assessment (HTA) guideline as a method to estimate health utility and subsequently QALYs. Health Intervention and Technology Assessment Program (HITAP) has been offering an annual economic evaluation training to policymakers and researchers which includes how to interpret and use EQ-5D-5L values in health technology assessment (HTA). Currently, EQ-5D-5L is being widely adopted in health economic evaluations in Thailand.
-
(xi)
Reference(s) of value set
Pattanaphesaj J, Thavorncharoensap M, Ramos-Goñi JM, Tongsiri S, Ingsrisawang L, Teerawattananon Y (2018) The EQ-5D-5L valuation study in Thailand. Expert Rev Pharmacoecon Outcomes Res 18(5): 551–558
Further Literature
-
Chaikledkaew U, Kittrongsiri K (2014) Guidelines for Health Technology Assessment in Thailand (Second Edition)-The Development Process. J Med Assoc Thai 97: 4–9
-
Leelahavarong P, Doungthipsirikul S, Kumluang S, Poonchai A, Kittiratchakool N, Chinnacom D, Suchonwanich N, Tantivess S (2019) Health technology assessment in Thailand: institutionalization and contribution to healthcare decision making: review of literature. Int J Tech Assess Health Care 35(6): 467–473
-
Teerawattananon Y, Luz AC, Culyer A, Chalkidou K (2020) Charging for the use of survey instruments on population health: the case of quality-adjusted life years. Bull World Health Organ 98(1):59–65
-
National Statistics Office (2012) The 2010 Population and Housing Census. National Statistics Office, Bangkok
-
National Statistics Office (2013). The Labor Force Survey 2012. National Statistics Office, Bangkok
4.3.2.4 Country/Region: Uruguay (Table 4.33)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the second wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 1.1. Interviews were conducted between October 2013 and June 2014.
-
(ii)
Sample size; sample frame
805 interviews with the general population were conducted. Respondents were recruited from 3 Uruguayan regions: Montevideo and the departments of Maldonado and Paysandú, using a stratified approach. Respondents were recruited using quotas for location, age, gender and socio-economic status. Of the 794 respondents included in the final value set, 55.3% were female and 44.7% were male. The age distribution of the respondents was:
18–24 years | 12.1% |
25–29 years | 11.7% |
30–39 years | 24.8% |
40–49 years | 16.3% |
50–64 years | 23.6% |
65–74 years | 9.8% |
75+ years | 1.8% |
-
(iii)
Representativeness of achieved sample
The study sample was broadly representative for the Uruguayan population. However, younger and higher educated respondents were slightly over-represented (Table 4.34).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.35)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.18)

Proportions choosing A based on relative severities of A and B
-
(vi)
Exclusion criteria
Respondents were excluded (1) if they had a positive slope on the regression between respondent’s cTTO values and level sum score, or (2) if they assigned the same value to all health states (except if all states were assigned the value 1, i.e., non-traders). 11 respondents were excluded from analysis.
-
(vii)
Number of interviewers; Interviewer effects
In total, 805 interviews were conducted by 11 interviewers. The variance of the responses included in the final value set can be partitioned into variance related to differences between interviewers (5.5%), respondents (26.9%) and responses (67.6%).
-
(viii)
Description of modelling choices
The Uruguayan EQ-5D-5L value set was based on cTTO data only. The selected model was based on a robust regression. A tuning variable was used, which was set to equal 8.5.
- (ix)

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
The Uruguayan EQ-5D-5L value set has been disseminated in scientific meetings in Uruguay and Latin America and used in several scientific projects. Research is currently ongoing to collect population health data using EQ-5D-5L in relevant health conditions, in order to use the Uruguayan weights. There are two HTA bodies in Uruguay; División de Evaluación Sanitaria/Ministerio de Salud Publica and Fondo Nacional de Recursos (FNR). Neither of these HTA bodies currently makes a specific recommendation to use the Uruguayan EQ-5D-5L value set in economic evaluations.
-
(xi)
Reference(s) of value set
Augustovski F, Rey-Ares L, Irazola V, Garay OU, Gianneo O, Fernández G, Morales M, Gibbons L, Ramos-Goñi JM (2016) An EQ-5D-5L value set based on Uruguayan population preferences. Qual Life Res 25(2):323–333
Further Literature
-
National Institute of Statistics Uruguay (Instituto Nacional de Estadística) (2011) Census http://www.ine.gub.uy/censos2011/index.html. Accessed 18 July 2021
4.3.2.5 Country/Region: Hong Kong (Table 4.37)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the second wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 1.1. Interviews were conducted between June 2014 and October 2015.
-
(ii)
Sample size; sample frame
A total of 1014 Hong Kong residents aged 18 and above participated in this study. Stratified quota sampling was applied based on age, sex and educational attainment over three geographical areas of Hong Kong: Hong Kong Island, Kowloon, and New Territories. Of the 999 respondents included in the final value set, 59.2% were female, and 40.8% were male. Furthermore, 29.8% of the respondents had at least 1 chronic health condition. The age distribution of the respondents was:
18–24 years | 16.52% |
|---|---|
25–29 years | 8.71% |
30–39 years | 17.62% |
40–49 years | 12.61% |
50–64 years | 29.43% |
65–74 years | 10.01% |
75+ years | 5.11% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the Hong Kong general population in terms of age, sex and highest education attainment. The distribution of the study sample in terms of marital status, employment status, and area of residence approximated that of the general population (Table 4.38).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.39)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.20)

Proportions choosing A based on relative severities of A and B
-
(vi)
Exclusion criteria
Three respondents with a positive slope on a regression between their cTTO values and the severity of the states were excluded from analysis. In addition, one respondent who valued all states at zero and 11 respondents who valued all states as −1 were removed from analysis. All DCE data were included in the analysis. A further 515 out of 9990 (5.16%) cTTO responses were removed following issues flagged in the feedback module.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1014 interviews were conducted by 6 interviewers. The variance of the responses included in the final value set can be partitioned into variance related to differences between interviewers (2.2%), respondents (33.1%), and responses (64.7%).
-
(viii)
Description of modelling choices
The Hong Kong EQ-5D-5L value set was based on a hybrid model combining a conditional logit model for the DCE data and a censored at −1 Tobit model for the cTTO data. The intercept was constrained in the final model as it was not statistically significant.
- (ix)

Value decrements across dimensions (MO mobility, SC self-care, UA usual activities, PD pain/discomfort, AD anxiety/depression)
-
(x)
Uptake by local HTA/health care decision makers
The EQ-5D-5L has been adopted in healthcare management for individual patients, education in healthcare delivery and health policy to promote patient-centred care in hospital settings in Hong Kong. The association between health-related quality of life and shared decision-making among patients was explored using the EQ-5D-5L in enhancing health professional-patient communications. The tool was incorporated into the local validated patient-reported experience measures (PREMs) among patients as a measure of health outcomes together with patient experience in different healthcare settings including inpatient, specialist outpatient, and accident and emergency department under the Hospital Authority (HA) in Hong Kong. It was also applied in health-related population surveys and routine measurement among patients with chronic conditions such as musculoskeletal problems, diabetes mellitus and elderly with hypertension in both clinical and non-clinical settings.
-
(xi)
Reference(s) for this value set
Wong EL, Ramos-Goni JM, Cheung AW, Wong AY, Rivero-Arias O (2018) Assessing the use of a feedback module to model EQ-5D-5L health states values in Hong Kong. Patient 11(2):235–247
Further Literature
-
Coulter A, Cheung AWL, Yam CHK, Yeoh EK, Griffiths S (2013) Validation of inpatient experience questionnaire. Int J Qual Health Care 25(4):443–451.
-
Lam CLK, Chao DVK, Cheung JPY, Fong D, Kind P, Ko WWK, Or CKL, Wong CKH, Wong ELY (2020) Effectiveness of routine measurement of health-related quality of life in improving the outcomes of patients with Musculoskeletal problems – A randomized controlled trial. 2019/2020 Research Grants Council Funded Study
-
Wong ELY, Xu RH, Cheung AWL (2020) Health-related quality of life in elderly people with hypertension and the estimation of minimally important difference using EQ-5D-5L in Hong Kong SAR, China. Eur J Health Econ 21(6):869–879
-
Wong ELY, Xu RH, Cheung AWL (2020) Measurement of health-related quality of life in patients with diabetes mellitus using EQ-5D-5L in Hong Kong, China. Qual Life Res 29(7):1913–921.
-
Wong ELY, Ho KF, Wong SYS, Cheung AWL, Yau PSY, Dong D, Yeoh EK (2020) Views on workplace policies and its impact on health-related quality of life during Coronavirus Disease (COVID-19) pandemic: Cross-sectional survey of employees. Int J Health Policy Manag. https://doi.org/10.34172/ijhpm.2020.127
-
Wong ELY, Xu RH, Cheung AWL. (2019) Health-related quality of life among patients with hypertension: population-based survey using EQ-5D-5L in Hong Kong SAR, China. BMJ Open 9(9):e032544. https://doi.org/10.1136/bmjopen-2019-032544
-
Wong ELY, Cheung AWL, Xu RH, Yam CHK, Lui SF, Yeoh EK (2019) Development and validation of a generic patient experience instrument for measuring specialist outpatient service in Hong Kong. Int J Qual Health Care 31(10):G158-G164
-
Wong ELY, Cheung AWL, Wong AYK, Xu RH, Ramos-Goni JM, Rivero-Arias O (2019) Normative profile of health-related quality of life for Hong Kong general population using preference-based instrument EQ-5D-5L. Value Health 22(8):916–924
-
Wong ELY, Shah K, Cheung AWL, Wong AYK, Visser M, Stolk E (2018) Evaluation of split version and feedback module on the improvement of Time Trade-Off Data. Value Health 21(6):732–741
-
Wong ELY, Coulter A, Hewitson P, Cheung AWL, Yam CHK, Lui SF, Tam WWS, Yeoh EK (2015) Patient experience and satisfaction with inpatient service: Development of short form survey instrument measuring the core aspect of inpatient experience. PLoS One 10(4):e0122299.https://doi.org/10.1371/journal.pone.0122299
-
Wong ELY, Xu RH, Cheung AWL, Wong ELY (2017) The relationship between shared decision-making and health-related quality of life among patients in Hong Kong SAR, China. Int J Qual Health Care. 29(4), 534–540. 11.
-
Census and Statistics Department (2012) 2011 Population census main report: Volume I. Census and Statistics Department, Hong Kong. http://www.statistics.gov.hk/pub/B11200592012XXXXB0100.pdf. Accessed 28 July 2021
4.3.3 Wave 3
4.3.3.1 Country/Region: France (Table 4.41)
The mathematical representation of the model for health state X is:
-
$$ {\displaystyle \begin{array}{l}V(X)=1-0.038\ M{O}_2-0.048\ M{O}_3-0.179\ M{O}_4-0.325\ M{O}_5-0.037\\ {}S{C}_2-0.051\ S{C}_3-0.172\ S{C}_4-0.258\ S{C}_5-0.033\ U{A}_2-0.040\ U{A}_3-0.157\\ {}U{A}_4-0.240\ U{A}_5-0.022\ P{D}_2-0.047\ P{D}_3-0.264\ P{D}_4-0.444\ P{D}_5-0.020\\ {}A{D}_2-0.047\ A{D}_3-0.200\ A{D}_4-0.258\ A{D}_5\end{array}} $$
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 2.0. Interviews were conducted from March until November 2018.
-
(ii)
Sample size; sample frame
1143 interviews with the general population were conducted. Quota-based sampling with respect to age, sex, and socioeconomic status was applied (National Institute for Statistics and Economic Studies [INSEE] 2018). Interviewers were selected to provide reasonable coverage of the territory and population size of the respondents’ residence. Of the 1048 respondents included in the final value set, 55.4% were female and 44.6% were male. The age distribution of the respondents was:
18–24 years | 9.6% |
25–29 years | 9.6% |
30–39 years | 15.4% |
40–49 years | 15.6% |
50–64 years | 26.0% |
65–74 years | 14.5% |
75+ years | 9.4% |
-
(iii)
Representativeness of achieved sample
The study sample was broadly representative for the French population aged over 18. However, the composition of the final sample used in modelling (following exclusions – see (vi) below) differed from the French general population in terms of age and gender. An overrepresentation of female respondents was observed. Respondents aged 25–34 years were overrepresented for both sexes. Moreover, women aged 75 and older were underrepresented in the sample, whereas woman in the age group 55–64 years were overrepresented (Table 4.42).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.43)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.22)

Proportions choosing A based on relative severities of A and B

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(vi)
Exclusion criteria
95 interviews were excluded from data analysis due to poor data quality. Interviews were excluded if the interviewer did not show the WTD task in the wheelchair example or if the respondent gave state 55555 a value that was higher than the value given to the mildest health state presented in the cTTO tasks. Moreover, a total of 6.5% of cTTO responses (n = 677) were removed following the feedback module. No DCE data were excluded from the analysis.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1143 interviews were conducted by 11 interviewers. The variance of the responses included in the final value set can be partitioned into variance related to differences between interviewers (3.3%), respondents (11.1%), and responses (85.6%).
-
(viii)
Description of modelling choices
The French EQ-5D-5L value set was based on a hybrid model combining a conditional logit model for the DCE data and a censored at −1 tobit model for the cTTO data, correcting for heteroskedasticity. The model was additionally adjusted to correct for imbalance in the sample in terms of age and gender distribution compared to the general population in France. The intercept was constrained in the final model because it was marginal and non-significant.
- (ix)
-
(x)
Uptake by local HTA/health care decision makers
The French National Authority for Health (Haute Autorité de Santé [HAS]) recommends in its updated official methodological guide for economic evaluation that the EQ-5D-5L questionnaire and the French EQ-5D-5L value set should be the preferred measure used to derive utility values for use in HTA (HAS 2020).
-
(xi)
Reference(s) for this value set
Andrade LF, Ludwig K, Ramos-Goñi JM, Oppe M, de Pouvourville G (2020) A French Value Set for the EQ-5D-5L. Pharmacoeconomics 38(4):413–425
Further Literature
-
National Institute for Statistics and Economic Studies (INSSE) (2018) Total population age and sex, January 1st, 2018. https://www.insee.fr/fr/statistiques/1892086?sommaire=1912926. Accessed 1 Jan 2018
-
Haute Autorité de Santé (HAS) (2020) The Choix méthodologiques pour l'évaluation économique à la HAS guideline. https://www.has-sante.fr/upload/docs/application/pdf/2020-07/guide_methodologique_evaluation_economique_has_2020_vf.pdf. Accessed 25 June 2021
4.3.3.2 Country/Region: Germany (Table 4.45)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 2.0. Interviews were conducted between December 2014 and March 2015.
-
(ii)
Sample size; sample frame
1158 interviews with the general population were conducted in six cities and surrounds located in different parts of Germany: Berlin, Leipzig, Hamburg, Bielefeld, Munich, and Frankfurt. Quota-based sampling with respect to age, sex, educational level, and employment status was applied (Federal Statistical Office 2015). Of the 1158 respondents included in the final value set, 53.4% were female and 46.6% were male. The age distribution of the respondents was:
18–24 years | 8.1% |
25–29 years | 6.3% |
30–39 years | 13.4% |
40–49 years | 19.5% |
50–64 years | 27.6% |
65–74 years | 14.2% |
75+ years | 10.9% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the German population in terms of age, sex, education, and employment status (Table 4.46).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.47)

Proportions choosing A based on relative severities of A and B
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.24)
-
(vi)
Exclusion criteria
A total of 6.2% of cTTO responses (n = 713) were removed following the feedback module; but no respondent’s entire cTTO responses were excluded. No DCE data were excluded from the analysis.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1158 interviews were conducted by 19 interviewers. The variance of the responses can be partitioned into variance related to differences between interviewers (2.7%), respondents (16.0%), and responses (81.3%).
-
(viii)
Description of modelling choices
The German EQ-5D-5L value set was based on a hybrid model combining a conditional logit model for the DCE data and a censored at −1 tobit model for the cTTO data, correcting for heteroskedasticity. The intercept was constrained in the final model because it was marginal and non-significant.
- (ix)

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
Cost-utility analysis (CUA) is currently not required and is not the preferred form of economic evaluation in pharmacoeconomics and health technology assessment guidelines provided by the Institute for Quality and Efficiency in Health Care (IQWiG), the official agency for providing evidence for reimbursement decisions of drugs in Germany (IQWiG 2020; Kennedy-Martin et al. 2020; Rowen et al. 2017). Use of CUA is common in the assessment process for the development of vaccination recommendations by the Standing Committee on Vaccination (STIKO) but no preference for a specific multi-attribute utility instrument is recorded (STIKO 2016).
-
(xi)
Reference(s) for this value set
Ludwig K, Graf von der Schulenburg JM, Greiner W (2018) German Value Set for the EQ-5D-5L. Pharmacoeconomics 36(6):663–674
Further Literature
-
Federal Statistical Office (2015) Mikrozensus. Bevölkerung und Erwerbstätigkeit. Stand und Entwicklung der Erwerbstätigkeit in Deutschland 2014. Federal Statistical Office, Wiesbaden
-
Thematisch/Arbeitsmarkt/Erwerbstaetige/StandEntwicklungErwerbstaetigkeit.html. Accessed 10 Aug 2017
-
Institute for Quality and Efficiency in Health Care (IQWiG) (2020) Allgemeine Methoden 6.0. IQWiG, Cologne. https://www.iqwig.de/ueber-uns/methoden/methodenpapier/. Accessed 25 June 2021
-
Standing Committee on Vaccination (STIKO) (2016) Methoden zur Durchführung und Berücksichtigung von Modellierungen zur Vorhersage epidemiologischer und gesundheitsökonomischer Effekte von Impfungen für die Ständige Impfkommission. STIKO, Berlin. https://www.rki.de/DE/Content/Kommissionen/STIKO/Aufgaben_Methoden/methoden_node.html;jsessionid=54B83BAC57F91FF652D8A285C014CD53.internet112. Accessed 25 June 2021
-
Kennedy-Martin M, Slaap B, Herdman M, van Reenen M, Kennedy-Martin T, Greiner W, Busschbach J, Boye K (2020) Which multi-attribute utility instruments are recommended for use in cost-utility analysis? A review of national health technology assessment (HTA) guidelines. Eur J Health Econ 21(8):1245–1257
-
Rowen D, Azzabi ZI, Chevrou-Severac H, van Hout B (2017) International Regulations and Recommendations for Utility Data for Health Technology Assessment. Pharmacoeconomics 35(Suppl 1):11–19
4.3.3.3 Country/Region: Indonesia (Table 4.49)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 2.0. Interviews were conducted between March 2015 and January 2016.
-
(ii)
Sample size; sample frame
1056 interviews with the general population were conducted in six cities and surrounds located in different parts of Indonesia: Jakarta, Bandung, Jogjakarta, Surabaya, Medan, and Makassar. A multi-stage stratified quota sampling with respect to residence, gender, age, and level of education (stage 1) and with respect to religion and ethnicity (stage 2) was applied (Indonesian Bureau of Statistics (BPS) 2015). Of the 1054 respondents included in the final value set, 49.9% were female and 50.1% were male. The age distribution of the respondents was:
17–24 years | 26.28% |
25–29 years | 11.20% |
30–39 years | 25.05% |
40–49 years | 17.08% |
50–64 years | 18.22% |
65–74 years | 2.09% |
75+ years | 0.09% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the Indonesian general population (over 17 years). The distribution of the study sample in terms of residence, gender, and religion was similar to that of the general population. There were some small differences between the Indonesian general population and some of the age groups, education levels, and ethnicities in the study sample (Table 4.50).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.51)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.26)

Proportions choosing A based on relative severities of A and B

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(vi)
Exclusion criteria
Due to data quality issues, after the first 102 interviews all interviewers were retrained and the interviews collected to that point were excluded from data analysis and regarded as pilot interviews (not included in the above-mentioned study sample, details are reported in Purba et al. 2017b).
A total of 9.8% of cTTO responses (n = 1033) were removed following the feedback module. Moreover, further 45 cTTO responses were excluded where the respondent preferred living in an impaired health state over full health. In addition, two respondents with a positive slope on the regression between his cTTO values and the level sum score were also excluded. No DCE data were excluded from the analysis.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1056 interviews were conducted by 15 interviewers. The variance of the responses included in the final value set can be partitioned into variance related to differences between interviewers (2.7%), respondents (12.1%), and responses (85.2%).
-
(viii)
Description of modelling choices
The Indonesian EQ-5D-5L value set was based on a hybrid model combining a conditional logit model for the DCE data and a censored at −1 tobit model for the cTTO data, correcting for heteroskedasticity. The intercept was constrained in the final model.
- (ix)
-
(x)
Uptake by local HTA/health care decision makers
The Indonesian Health Technology Assessment Committee (InaHTAC) produced an HTA guideline in 2017 that suggests use of cost-utility analysis (CUA) and cost-effectiveness analysis (CEA) for economic evaluations in Indonesia. The guideline also recommends EQ-5D as the preferred instrument for use in estimating QALYs (InaHTAC 2017). The availability of EQ-5D-5L value set from a societal, Indonesian perspective supported various HTA and non-HTA studies in Indonesia.
-
(xi)
Reference(s) for this value set
Purba FD, Hunfeld JAM, Iskandarsyah A, Fitriana TS, Sadarjoen SS, Ramos-Goñi JM, Passchier J, Busschbach JJV (2017a) The Indonesian EQ-5D-5L Value Set. Pharmacoeconomics 35(11):1153–1165
Further Literature
-
Badan Pusat Statistik (BPS) (2015) Statistik 70 Tahun Indonesia Merdeka. Badan Pusat Statistik, Jakarta
-
Indonesian Health Technology Assessment Committee (InaHTAC) (2017) Health Technology Assessment (HTA) Guideline. Pusat Pembiayaan dan Jaminan Kesehatan Kementerian Kesehatan RI, Jakarta
-
Purba FD, Hunfeld JAM, Iskandarsyah A, Fitriana TS, Sadarjoen SS, Passchier J, Busschbach JJV (2017b) Employing quality control and feedback to the EQ-5D-5L valuation protocol to improve the quality of data collection. Qual Life Res 26(5):1197–1208
4.3.3.4 Country/Region: Ireland (Table 4.53)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 2.0. Interviews were conducted between March 2015 and September 2016.
-
(ii)
Sample size; sample frame
1160 interviews with the general population were conducted. A representative sample of Irish residents was obtained using a two-stage stratified clustering process. In the first stage, a sample of 54 small areas stratified by income and urban/rural classifications were drawn at random from across the country. In the second stage, within each small area, a sample of approximately 20 households were selected at random. Random selection was achieved by using a random starting point and inviting a resident from every third household to participate in the survey. The recruited sample was then compared with Central Statistics Office for Ireland (CSO) national population estimates for age and sex. Purposive sampling was used to augment the number of younger individuals and males in the sample. Of the 1160 completed surveys, 102 were purposive; 37% were male and 63% female.
The age distribution of the respondents was:
18–24 years | 7.84% |
|---|---|
25–29 years | 5.60% |
30–39 years | 18.02% |
40–49 years | 20.69% |
50–64 years | 25.95% |
65–74 years | 14.05% |
75+ years | 7.84% |
-
(iii)
Representativeness of achieved sample
Including the purposive sample, the sample broadly reflects the Irish population, with some over-representation of those aged > 45 years and of females. Those with tertiary-level education were over-represented and those with only primary- level education were under-represented compared with the population at large (Table 4.54).
-
(iv)
Mean values of cTTO states (Table 4.55)
-
(v)
Proportions choosing A and B in DCE based on relative severities of A and B (Fig. 4.28)

Proportions choosing A and B based on relative severities of A and B
-
(vi)
Exclusion criteria
No data were excluded from analysis.
-
(vii)
Number of interviewers; Interviewer effects
In total 1160 interviews were conducted by 7 interviewers. The variance of the responses can be partitioned into variance related to differences between interviewers (1.39%) respondents (30.98%) and responses (67.63%).
-
(viii)
Description of modelling choices
The observed cTTO values for the non-flagged health states after the feedback module were used i.e., the respondent’s flagged cTTO observations – which accounted for 2% values) were excluded (details on the feedback module and its use are provided in Chap. 2). For the DCE data, the dependent variable was the binary stated choice (i.e., 0/1 indicated the choice for each health state pair). No DCE data were excluded.
The Irish EQ-5D-5L value set was based on a main effects hybrid model combining DCE data and cTTO data, addressing the censoring of cTTO data at −1 and correcting for heteroskedasticity.

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
There are two principal public entities involved in cost-utility analysis (CUA) in Ireland: the Health Information and Quality Authority (HIQA) for non-pharmaceutical technologies and the National Centre for Pharmacoeconomics (NCPE) for pharmaceutical technologies. The former can undertake CUAs; the latter can request evidence from CUAs by pharmaceutical companies. While HIQA has used the Irish EQ-5D-5L value set (HIQA 2018) as have a number of academic studies (for example, see Murphy et al. 2019; Cardwell et al. 2020), NCPE have not yet adopted it for use.
-
(xi)
Reference for this value set
Hobbins A, Barry L, Kelleher D, Shah K, Devlin N, Ramos Goni JM, O'Neill C (2018) Utility Values for Health States in Ireland: A Value Set for the EQ-5D-5L. Pharmacoeconomics 36(11):1345–1353
Further Literature
-
Central Statistics Office for Ireland (2011) Census 2011 reports. https://www.cso.ie/en/census/census2011reports/. Accessed 29 July 2021
-
HIQA (2018) HTA of extending the HPV vaccination to boys. https://www.hiqa.ie/reports-and-publications/health-technology-assessment/hta-extending-hpv-vaccination-boys. Accessed 21 July 2021
-
Cardwell K, Smith S M, Clyne B, McCullagh L, Wallace E, Kirke C, Fahey T, Moriarty F (2020) Evaluation of the General Practice Pharmacist (GPP) intervention to optimise prescribing in Irish primary care: a non-randomised pilot study. BMJ Open 10(6):e035087. https://doi.org/10.1136/bmjopen-2019-035087
-
Murphy A, Bourke J, Flynn D, Kells M, Joyce M (2019) A cost-effectiveness analysis of dialectical behaviour therapy for treating individuals with borderline personality disorder in the community. Ir J Med Sci 189(2):415–423
4.3.3.5 Country/Region: Malaysia (Table 4.57)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 2.0. Interviews were conducted between August and September 2016.
-
(ii)
Sample size; sample frame
1137 interviews with the general population were conducted in four Malaysian states: Penang (Northern), Selangor (Central), Kelantan (Eastern), and Malacca (Southern). A quota-based sampling with respect to urbanicity, gender, age (over 18 years) and ethnicity based on the Malaysian National Census (Department of Statistics Malaysia 2010). Of the 1125 respondents included in the final value set, 48.8% were female and 51.2% were male. The age distribution of the respondents was:
18–24 years | 26.8% |
25–29 years | 13.7% |
30–39 years | 15.6% |
40–49 years | 14.6% |
50–64 years | 21.4% |
65–74 years | 6.3% |
75+ years | 1.5% |
-
(iii)
Representativeness of achieved sample
The study sample was largely representative for the Malaysian general population in terms of gender, age, ethnicity, and residential area. Employed (full time)/self-employed respondents were slightly underrepresented in the study sample (Table 4.58).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.59)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.30)

Proportions choosing A based on relative severities of A and B

Value decrements across dimensions. (Please note that the lines of MO and PD are virtually identical. The line for MO is obscured by the yellow line for PD; AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(vi)
Exclusion criteria
Respondents whose cTTO value increased with health state severity and those who valued all health states at −1 were excluded from data analysis (n=12). No DCE data were excluded from the analysis.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1137 interviews were conducted by 18 interviewers. The variance of the responses included in the final value set can be partitioned into variance related to differences between interviewers (1.1%), respondents (21.8%), and responses (77.1%).
-
(viii)
Description of modelling choices
The Malaysian EQ-5D-5L value set was based on a non-linear constrained hybrid model combining a conditional logit model for the DCE data and an additive model assuming a normal distribution for the cTTO data. A constrained eight-parameter model was selected that fits a single parameter per dimension, taking a value representing level 5; and one parameter for each of levels 2, 3, and 4 that are multiplied by the respective dimension parameters. The eight-parameter model can be converted to 20 parameters, as presented in Table 4.57 for consistency purposes in this chapter. The intercept was constrained in the final model because it was non-significant.
- (ix)
-
(x)
Uptake by local HTA/health care decision makers
According to the current Malaysia Pharmacoeconomic Guidelines, the preferred economic evaluation techniques to inform health technology assessment decisions are cost-effectiveness analysis (CEA) and cost-utility analysis (CUA) (Ministry of Health Malaysia 2019). CUA is the recommended technique when HRQOL is an important outcome and when the intervention affects both morbidity and mortality. The guideline also states that EQ-5D is the preferred patient-reported outcomes measure and that a locally derived value set is strongly recommended for use, with the Malaysian EQ-5D-5L value set study being cited in the document.
-
(xi)
Reference(s) for this value set
Shafie AA, Vasan Thakumar A, Lim CJ, Luo N, Rand-Hendriksen K, Yusof FAM (2019) EQ-5D-5L Valuation for the Malaysian Population. Pharmacoeconomics 37(5):715–725
Further Literature
-
Department of Statistics Malaysia (2010) Population distribution and basic demographic characteristic report 2010. Department of Statistics Malaysia, Putrajaya
-
Department of Statistics Malaysia (2016) Labour Force Survey Report Malaysia 2016. Department of Statistics Malaysia, Putrajaya. https://www.dosm.gov.my/v1/index.php?r=column/cthemeByCat&cat=126&bul_id=SGZCNnMrWW9ZTEdpYys4YW0yRlhoQT09&menu_id=U3VPMldoYUxzVzFaYmNkWXZteGduZz09. Accessed 14 July 2021
-
Ministry of Health Malaysia (2019) Pharmacoeconomic guidelines for Malaysia. Ministry of Health Malaysia, Petaling Jaya. https://www.pharmacy.gov.my/v2/sites/default/files/document-upload/pharmacoeconomic-guidelines-malaysia-malaysia-second-edition-2019-final-page-adjustment.pdf. Accessed 25 June 2021
4.3.3.6 Country/Region: Poland (Table 4.61)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 2.0. Interviews were conducted from June until October 2016.
-
(ii)
Sample size; sample frame
1281 interviews with the general population were conducted. Quota-based sampling was applied using Polish census data from November 2014, based on personal identification number registry and Central Statistical Office data on education (Central Statistical Office 2015). Of the 1252 respondents included in the final value set, 52.5% were female and 47.5% were male. The age distribution of the respondents was:
18–24 years | 14.8% |
25–29 years | 7.0% |
30–39 years | 17.5% |
40–49 years | 15.9% |
50–64 years | 26.5% |
65–74 years | 13.9% |
75+ years | 4.5% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the Polish general population in terms of age, sex, education, employment status, as well as size and geographical location of the place of residence (Table 4.62).
Table 4.62 Representativeness of the sample in the Polish valuation study
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.63)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.32)

Proportions choosing A based on relative severities of A and B
-
(vi)
Exclusion criteria
29 interviews with data quality issues in the cTTO part were excluded from the data analysis (i.e. flagged interviews in QC tool; see Chap. 2 for more details). A total of 8.3% of cTTO responses (n = 1040) were removed following the feedback module. No DCE data were excluded from the analysis.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1281 interviews were conducted by 15 interviewers. The variance of the responses included in the final value set can be partitioned into variance related to differences between interviewers (3.5%), respondents (13.7%), and responses (82.8%).
-
(viii)
Description of modelling choices
The Polish EQ-5D-5L value set was based on a hybrid model that accounted for random parameters, error scaling with fat tails, censoring at −1, unwillingness to trade life years in cTTO by the religious people and Cauchy distribution in DCE. The intercept was constrained in the final model.
- (ix)

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
A pharmacoeconomic analysis is required in Polish HTA submissions, and cost-utility analysis is the preferred form of economic evaluation in HTA reports and reimbursement dossiers of drugs, according to Reimbursement Act (2011) and Polish HTA agency (Agencja Oceny Technologii Medycznych i Taryfikacji, AOTMiT) guidelines (AOTMiT 2016). The preferred way of obtaining health state values is based on secondary sources – published data collected using questionnaires accompanied by values. The first choice is EQ-5D (EQ-5D-5L or EQ-5D-3L). If EQ-5D-based data are not available, the second choice is SF-6D- or HUI-based utilities. The third choice covers health state values based on other instruments. In the case of primary collection of health states valuation data, the use of EQ-5D (EQ-5D-3L or EQ-5D-5L) and Polish values sets are recommended.
-
(xi)
Reference(s) for this value set
Golicki D, Jakubczyk M, Graczyk K, Niewada M (2019) Valuation of EQ-5D-5L Health States in Poland: the First EQ-VT-Based Study in Central and Eastern Europe. Pharmacoeconomics 37(9):1165–1176
Further Literature
-
Agencja Oceny Technologii Medycznych i Taryfikacji (AOTMiT) (2016) Health Technology Assessment Guidelines (Version 3.0). AOTMiT, Warsaw.
https://www.aotm.gov.pl/media/2020/07/20160913_Wytyczne_AOTMiT.pdf [Polish version];
-
https://www2.aotm.gov.pl/wp-content/uploads/wytyczne_hta/2016/20161104_HTA_Guidelines_AOTMiT.pdf [English version]. Accessed 13 July 2021
-
Central Statistical Office (2015) Demographic yearbook of Poland. Zakład Wydawnictw Statystycznych, Warsaw
4.3.3.7 Country/Region: Portugal (Table 4.65)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 2.0. Interviews were conducted between October 2015 and July 2016.
-
(ii)
Sample size; sample frame
1451 interviews with the general population were conducted over the country. Random sampling stratified by gender and age group, based on the Portuguese census (Portuguese Statistical Office 2012), was applied that was originally designed based on the random route sampling method. Of the 1450 respondents included in the final value set, 56.9% were female and 43.1% were male.The age distribution of the respondents was:
18–24 years | 10.6% |
25–29 years | 5.9% |
30–39 years | 16.3% |
40–49 years | 13.8% |
50–64 years | 21.2% |
65–74 years | 19.0% |
75+ years | 13.2% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the Portuguese population in terms of age (over 18 years), and gender of the general population of mainland Portugal and the islands (Table 4.66).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.67)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.34)

Proportions choosing A based on relative severities of A and B

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(vi)
Exclusion criteria
A total of 7.7% of cTTO responses (n = 1119) were removed following the feedback module. In addition, one participant with a positive slope on the regression between his cTTO values and the level sum score was also excluded. No DCE data were excluded from the analysis.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1451 interviews were conducted by 28 interviewers. The variance of the responses included in the final value set can be partitioned into variance related to differences between interviewers (5.7%), respondents (20.0%), and responses (74.3%).
-
(viii)
Description of modelling choices
The Portuguese EQ-5D-5L value set was based on a hybrid model combining a conditional logit model for the DCE data and a censored at -1 tobit model for the cTTO data, correcting for heteroskedasticity. The intercept was constrained in the final model.
- (ix)
-
(x)
Uptake by local HTA/health care decision makers
The National Authority of Medicines and Health Products (Infarmed) recommends in its official methodological guidelines for economic evaluation studies of health technologies that the EQ-5D-5L questionnaire and the Portuguese EQ-5D-5L value set should be the preferred measure used to assess HRQoL in cost-utility analyses (CUA) (Perelman et al. 2019).
-
(xi)
Reference(s) for this value set
Ferreira PL, Antunes P, Ferreira LN, Pereira LN, Ramos-Goñi JM (2019) A hybrid modelling approach for eliciting health states preferences: the Portuguese EQ-5D-5L value set. Qual Life Res 28(12):3163–3175
Further Literature
-
Perelman J, Soares M, Mateus C, Duarte A, Faria R, Ferreira L, Saramago P, Veiga P, Furtado C, Caldeira S, Teixeira MC, Sculpher M (2019) Methodological Guidelines for Economic Evaluation Studies of Health Technologies. INFARMED – National Authority of Medicines and Health Products, I.P., Lisbon. https://www.infarmed.pt/web/infarmed-en/human-medicines. Accessed 25 June 2021
-
Portuguese Statistical Office (2012) Census 2011. Portuguese Statistical Office, Lisbon
4.3.3.8 Country/Region: Taiwan (Table 4.69)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 2.0. Interviews were conducted between January and July 2017.
-
(ii)
Sample size; sample frame
1000 interviews with the general population were conducted in nine randomly selected cities located in six geographic regions in Taiwan: Taipei, New Taipei, Tauyuan, Chinju, Hualien, Taichung, Chiayi, Tainan, and Kaohsiung. Multi-stage stratified quota sampling with respect to region (stage 1) and age (over 20), gender, and education (stage 2) was applied (Department of household registration, Ministry of the Interior, Taiwan 2016). Of the 1000 respondents included in the final value set, 50.5% were female and 49.5% were male. The age distribution of the respondents was:
20–24 years | 7.9% |
25–29 years | 9.4% |
30–39 years | 20.8% |
40–49 years | 19.0% |
50–64 years | 28.8% |
65–74 years | 11.5% |
75+ years | 2.6% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the Taiwanese population in terms of age, gender, and living area. Respondents with higher education were overrepresented while respondents with primary school education were underrepresented in the study sample (Table 4.70).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.71)

Proportions choosing A based on relative severities of A and B
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.36)
-
(vi)
Exclusion criteria
No data were excluded from the analysis.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1000 interviews were conducted by 10 interviewers. The variance of the responses can be partitioned into variance related to differences between interviewers (1.3%), respondents (15.5%), and responses (83.2%).
-
(viii)
Description of modelling choices
The Taiwanese EQ-5D-5L value set was based on a hybrid model combining a conditional logit model for the DCE data and a censored at -1 tobit GLS model for the cTTO data. The intercept was constrained in the final model because it was non-significant.
- (ix)

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
Conducting local cost-effectiveness analyses for new technologies is encouraged in the official guideline of the Center for Drug Evaluation (CDE) in Taiwan (CDE 2021a, 2021b; Taiwan Society for Pharmacoeconomics and Outcomes Research [TaSPOR] 2014). The EQ-5D is listed as one of three recommended tools for multi-attribute utility system in this HTA guideline (TaSPOR 2014). A local value set was recommended, although no local value sets were available at the time of publishing this HTA guideline. Under the implementation of NHI in Taiwan, it was announced that “new drug applications with local pharmacoeconomic studies are more likely to get reimbursement (…) [and the] additional markup of up to 10% of pricing decision (…) [can be added once the] applicants conduct a local pharmacoeconomic study” after quality review of the HTA/CDE (Chen et al. 2018). As a result, the EQ-5D-5L value set for Taiwan reported here was endorsed by CDE and TaSPOR in a joint conference (“Workshop of health utility applications - How to use Taiwan EQ-5D-5L value set to promote the impacts of pharmacoeconomics and outcomes research?” November 29, 2019). Given that the large value range of the Taiwanese value set might influence the future calculation of quality-adjusted life years (QALYs) in cost-utility analyses, it was also agreed that there was a need for further research and discussions to facilitate more reasonable decision-making about adopting a national set of EQ-5D-5L weights for QALYs calculations in that aforementioned conference. This was also endorsed by HTA/CDE. In addition to its use in HTA, the EQ-5D-5L is also included in the National Health Interview Survey.
-
(xi)
Reference(s) for this value set
Lin HW, Li CI, Lin FJ, Chang JY, Gau CS, Luo N, Pickard AS, Ramos Goñi JM, Tang CH, Hsu CN (2018) Valuation of the EQ-5D-5L in Taiwan. PLoS ONE 13(12). https://doi.org/10.1371/journal.pone.0209344
Further Literature
-
Center for Drug Evaluation (CDE) (2021a) Health Technology Assessment. Introduction. https://www.cde.org.tw/eng/HTA/. Accessed 21 June 2021
-
CDE (2021b) HTA Consultation Services. The Process of HTA Assessment for Applications of NHI New Drug Listing. http://www.cde.org.tw/eng/HTA/business. Accessed 21 June 2021
-
Chen GT, Chang SC, Chang CJ (2018) New Drug Reimbursement and Pricing Policy in Taiwan. Value Health Reg Issues 15:127–132
-
Department of household registration, Ministry of the Interior, Taiwan (2016) Household registration statistic data analysis 2016. http://www.ris.gov.tw/en/web/ris3-english/home. Accessed 12 Jan 2021
-
Taiwan Society for Pharmacoeconomics and Outcomes Research (TaSPOR) (2014) HTA guidelines in Taiwan 2014. Taiwan PE guideline, Pharmacoeconomic Guidelines Around the World. https://tools.ispor.org/PEguidelines/countrydet.asp?c=31&t=1. Accessed 15 June 2021
4.3.3.9 Country/Region: Denmark (Table 4.73)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 2.1. Interviews were conducted between October 2018 and November 2019.
-
(ii)
Sample size; sample frame
1052 interviews with the general population were conducted. Randomly selected representative samples with respect to age, gender, education, and geographical region were provided by Statistics Denmark and a panel from a Danish market research company, to be invited to the study. Of the 1014 respondents included in the final value set, 51.6% were female and 48.4% were male. The age distribution of the respondents was:
18–24 years | 3.9% |
25–29 years | 7.3% |
30–39 years | 12.0% |
40–49 years | 15.7% |
50–64 years | 29.7% |
65–74 years | 21.6% |
75+ years | 9.8% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the Danish population in terms of age (over 18 years), gender, education, and geographical region. However, higher educated respondents were slightly overrepresented compared to the general population (Table 4.74).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.75)

Proportions choosing A based on relative severities of A and B
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.38)
-
(vi)
Exclusion criteria
5 interviews were dropped because the two interviewers that conducted these interviews were not sufficiently available to do more interviews. Additionally, 12 interviews were dropped due to technical issues, respondents having cognitive or emotional issues, or withdrawing consent. Lastly, 21 respondents were excluded as they did not provide both cTTO and DCE data. A total of 7.0% of cTTO responses (n = 712) were removed following the feedback module.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1014 interviews were conducted by 13 interviewers. 11 interviewers were included in the final interviewer team (see section vi). The variance of the responses included in the final value set can be partitioned into variance related to differences between interviewers (1.9%), respondents (23.8%), and responses (74.3%).
-
(viii)
Description of modelling choices
The Danish EQ−5D-5L value set was based on a hybrid model combining a conditional logit model for the DCE data and a censored at −1 Tobit model for the cTTO data, correcting for heteroskedasticity. The intercept was constrained in the final model.
- (ix)

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
As of 1st January 2021, the Danish Medicines Council started using quality-adjusted life years (QALYs) for the evaluation of new hospital-dispensed pharmaceuticals and change of indication. QALY estimates are expected to be based on EQ-5D-5L and the new Danish value set (Danish Medical Council 2021). Voluntary submissions of cost-utility analyses to the Reimbursement Committee (for prescription medicines prescribed by GPs) are also expected to make use of EQ-5D-5L with the Danish value set (Danish Medicines Agency). Furthermore, a new priority-setting council for new technology (excluding medicines) was established on 1st January 2021—the Danish Health Technology Council. Submissions to the council with cost-utility analysis are requested to use QALYs based on EQ-5D-5L and the Danish value set.
-
(xi)
Reference(s) of value set
Jensen CE, Sørensen SS, Gudex C, Jensen MB, Pedersen KM, Ehlers, LH (2021) The Danish EQ-5D-5L Value set A Hybrid Model Using cTTO and DCE Data. Appl Health Econ Health Policy 19(4):579–591
Further Literature
-
Danmarks Statistik (2019) Befolkningens udvikling 2019 (Vital Statistics 2019). https://www.dst.dk/Site/Dst/Udgivelser/GetPubFile.aspx?id=29444&sid=befudv2019 Accessed 28 July 2021
-
Danish Medicines Agency (2018) Health economic analyses in reimbursement applications https://laegemiddelstyrelsen.dk/en/reimbursement/general-reimbursement/application/health-economic-analyses-in-reimbursement-applications/. Accessed 15 July 2021
-
Danish HTA Agency (2021) Behandlingsrådet. https://behandlingsraadet.dk/proces-og-metode/. Accessed 15 July 2021
-
Danish Medicines Council (Medicinrådet) (2021) Medicinrådets metodevejledning for vurdering af nye lægemidler. Version 1.0. Published 3rd February 2021. https://medicinraadet.dk/media/5nvplk03/efter-1-januar-2021_medicinrådets-metodevejledning-for-vurdering-af-nye-lægemidler-vers-1-0_adlegacy.pdf. Accessed 15 July 2021
4.3.3.10 Country/Region: Ethiopia (Table 4.77)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using the EQ-VT protocol 2.1 and the EQ-PVT software. Interviews were conducted between March and May 2018.
-
(ii)
Sample size; sample frame
1050 interviews with the general population were conducted, recruited from the capital Addis Ababa city, and Butajira, which is a rural region. Multistage stratified quota sampling with respect to geographic area/residence, age, gender, and religion was applied. Of the 1048 respondents included in the final value set, 47.9% were female and 52.1% were male. The age distribution of the respondents was:
18–24 years | 37.2% |
25–29 years | 23.7% |
30–39 years | 21.1% |
40–49 years | 7.1% |
50–64 years | 7.6% |
65–74 years | 3.2% |
75+ years | 0.1% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the Ethiopian population in terms of age (over 18 years), gender, residence and religion (Table 4.78).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.79)

Proportions choosing A based on relative severities of A and B

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.40)
-
(vi)
Exclusion criteria
Respondents that valued all states as equal in the cTTO were excluded. Furthermore, respondents that valued the worst health state (55555) as higher than the mildest health state in their block were excluded. This amounts to 9 respondents excluded by the characteristics of their cTTO responses. Furthermore, 2 respondents’ DCE data were excluded due to technical problems.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1050 interviews were conducted by 10 interviewers. The variance of the responses included in the final value set can be partitioned into variance related to differences between interviewers (0.1%), respondents (10.5%) and responses (89.4%).
-
(viii)
Description of modelling choices
The Ethiopian EQ-5D-5L value set was based on a hybrid model combining a conditional logit model for the DCE data and a censored at −1 Tobit model for the cTTO data, correcting for heteroskedasticity. The intercept was constrained in the final model.
- (ix)
-
(x)
Uptake by local HTA/health care decision makers
The Ethiopian Federal Ministry of Health (FMOH) has set up an HTA agency in Ethiopia. However, HTA is not yet used for reimbursement decisions in Ethiopia.
-
(xi)
Reference(s) of value set
Welie AG, Gebretekle GB, Stolk E, Mukuria C, Krahn MD, Enquoselassie F, Fenta TG (2020) Valuing health state: an EQ-5D-5L value set for Ethiopians. Value Health Reg Issues 22:7–14
Further Literature
-
Central Statistical Agency (2017) Demographic and Health Survey 2016. https://dhsprogram.com/pubs/pdf/FR328/FR328.pdf. Accessed 28 July 2021
4.3.3.11 Country/Region: Hungary (Table 4.81)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 2.1. Interviews were conducted from May 2018 until March 2019.
-
(ii)
Sample size; sample frame
1000 interviews with the general population were conducted. A non-probability quota sampling was used, and quotas were set for age and sex according to the latest data reported by the Hungarian Central Statistical Office (2016). Of the 1000 respondents included in the final value set, 53.3% were female and 46.7% were male. The age distribution of the respondents was:
18–24 years | 10.0% |
25–29 years | 11.4% |
30–39 years | 14.4% |
40–49 years | 17.6% |
50–64 years | 24.0% |
65–74 years | 13.0% |
75+ years | 9.6% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the Hungarian general population in terms of age and sex. The distribution of the study sample in terms of marital status, employment status, and area of residence approximated that of the general population. Higher-educated respondents and inhabitants of Central Hungary were slightly overrepresented in the Hungarian valuation study (Table 4.82).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.83)

Proportions choosing A based on relative severities of A and B
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.42)
-
(vi)
Exclusion criteria
A total of 6.3% of cTTO responses (n = 634) were removed following the feedback module, but no respondent’s entire cTTO responses were excluded.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1000 interviews were conducted by 13 interviewers. The variance of the responses can be partitioned into variance related to differences between interviewers (1.7%), respondents (10.7%), and responses (87.6%).
-
(viii)
Description of modelling choices
The Hungarian EQ-5D-5L value set was based on the cTTO data only. The selected model was a pooled heteroskedastic tobit model, left-censored at -1. The intercept was constrained in the final model because it was non-significant.
- (ix)

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
In Hungary, guidelines on methods for economic evaluations in healthcare are developed by the Ministry of Human Capacities (EMMI 2017), and submissions are critically appraised at the Division for HTA at the National Institute for Pharmacy and Nutrition (OGYÉI 2019). Cost-utility analysis is the preferred form of economic evaluation of new health technologies. EQ-5D-5L is the preferred measure to calculate QALY’s (EMMI 2017). From 2020, the availability of the Hungarian value sets for both EQ-5D-5L and EQ-5D-3L are expected to increase the use and diffusion of the EQ-5D in Hungary.
-
(xi)
Reference(s) for this value set
Rencz F, Brodszky V, Gulácsi L, Golicki D, Ruzsa G, Pickard AS, Law EH, Péntek M (2020) Parallel Valuation of the EQ-5D-3L and EQ-5D-5L by Time Trade-Off in Hungary. Value Health 23(9):1235–1245
Further Literature
-
Hungarian Central Statistical Office (2016) Microcensus 2016. http://www.ksh.hu/docs/eng/xftp/idoszaki/microcensus2016/microcensus_2016_3.pdf. Accessed 24 Feb 2019
-
Ministry of Human Capacities of Hungary (Az Emberi Erőforrások Minisztériuma, EMMI) (2017) Szakmai irányelve az egészségügyi technológia értékelés módszertanáról és ennek keretében költséghatékonysági elemzések készítéséről. Egészségügyi Közlöny 3(10):821–842
-
Ministry of Human Capacities of Hungary (Az Emberi Erőforrások Minisztériuma, EMMI) (2021) Egészségügyi szakmai irányelve az egészség-gazdaságtani elemzések készítéséhez és értékeléséhez. Egészségügyi Közlöny 71(21): 2178-2200
-
National Institute of Pharmacy and Nutrition (Országos Gyógyszerészeti és Élelmezés-egészségügyi Intézet, OGYÉI) (2019) A gyógyszer befogadási kérelmek értékelésének OGYÉI Technológia-értékelő Főosztálya által figyelembe vett szempontjai. https://www.ogyei.gov.hu/ajanlasok. Accessed 8 Nov 2020
-
Rencz F, Gulacsi L, Drummond M, Golicki D, Prevolnik Rupel V, Simon J, Stolk EA, Brodszky V, Baji P, Závada J, Petrova G, Rotar A, Péntek M (2016) EQ-5D in Central and Eastern Europe: 2000–2015. Qual Life Res 25(11):2693–2710
4.3.3.12 Country/Region: Mexico (Table 4.85)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 2.1. Interviews were conducted from June until August 2019.
-
(ii)
Sample size; sample frame
A nationally representative sample of Mexican adults > 18 years stratified by sex, age and socioeconomic level were obtained using sample frames developed by CONAPO, the Mexican Office of Statistics and Geography and the socioeconomic classification of households by the Mexican Association of Marketing Research and Public Opinion Agencies (AMAI). Of the 1000 respondents included in the analysis, 48.6% were female and 51.4% were male. The age distribution of the respondents was:
18–24 years | 22.3% |
25–34 years | 15.4% |
35–44 years | 19.9% |
45–54 years | 16.5% |
55–64 years | 17.1% |
65–74 years | 5.9% |
75+ years | 2.9% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the adult Mexican population in terms of age, sex, geographical region and socioeconomic group (Table 4.86).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.87)

Proportions choosing A based on relative severities of A and B
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.44)
-
(vi)
Exclusion criteria
Using the feedback module, 2.1% of the cTTO responses were deemed problematic and were excluded from analysis. No DCE data were excluded from the analysis.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1000 interviews were conducted by 15 interviewers. The variance of the responses can be partitioned into variance related to differences between interviewers (0.99%), respondents (7.61%), and responses (91.40%).
-
(viii)
Description of modelling choices
The observed cTTO values for the non-flagged health states after the feedback module were used (i.e. the respondent’s flagged cTTO observations were excluded) (details on the feedback module and its use are provided in Chap. 2).
The Mexican EQ-5D-5L value set was based on a 20-parameter model estimated using only cTTO data. The value set is based on a heteroscedastic Bayesian model with censoring at −1.
- (ix)

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
Mexico’s General Health Council (GHC) is the collegiate body responsible for updating the National Compendium of Healthcare Supplies of the public health care institutions. The Compendium aims to strengthen the evaluation of health care technologies, to optimize public resources directed at addressing health problems and to notify and update health professionals. The GHC periodically updates the health technology assessment (HTA) processes used to determine inclusion in the Compendium. The most recent update of the HTA process includes cost-utility analysis (CUA) as a complementary evaluation that can be presented to strengthen the cost-effectiveness and budget impact analyses of health technologies seeking inclusion in the Compendium. It can be foreseen that the Mexican value set will encourage the development of CUA in the near future.
-
(xi)
Reference(s) for this value set
Gutierrez-Delgado C, Galindo-Suárez RM, Cruz-Santiago C, Shah K, Papadimitropoulos M, Zamora B, Feng Y, Devlin N (2021) EQ-5D-5L Health-State Values for the Mexican Population. Appl Health Econ Health Policy. https://doi.org/10.1007/s40258-021-00658-0
Further Literature
-
Consejo de Salubridad General (2017) Guía para la Conducción de Estudios de Evaluación Económica para la Actualización del Cuadro Básico y Catálogo de Insumos del Sector Salud en México. Comisión Interinstitucional del Cuadro Básico y Catálogo de Insumos del Sector Salud. http://www.csg.gob.mx/descargas/pdf/priorizacion/cuadro-basico/guias/insumos_salud/GEI_2017_Diciembre.pdf. Accessed 28 July 2021
-
Consejo de Salubridad General (2017) Guía de Evaluación de Insumos para la Salud. Comisión Interinstitucional del Cuadro Básico y Catálogo de Insumos del Sector Salud. http://www.csg.gob.mx/descargas/pdf/priorizacion/cuadro-basico/guias/insumos_salud/GEI_2017_Diciembre.pdf. Accessed 28 July 2021
-
Consejo Nacional de Población (CONAPO) (2018) Proyecciones de la población de México y de las entidades federativas, 2016–2050 y conciliación demográfica de México 1950–2015. https://www.gob.mx/conapo/acciones-y-programas/conciliacion-demografica-de-mexico-1950-2015-y-proyecciones-de-la-poblacion-de-mexico-y-de-las-entidades-federativas-2016-2050. Accessed 28 July 2021
-
Instituto Nacional de Estadística y Geografía (INEGI) (2015) Regiones Socioeconómicas de México. http://sc.inegi.gob.mx/niveles/datosnbi/reg_soc_mexico.pdf. Accessed 28 July 2021
-
Asociación Mexicana de Agencias de Investigación de Mercado (AMAI) (2016) Niveles socioeconómicos. http://nse.amai.org/niveles-socio-economicos-amai/. Accessed 28 July 2021
4.3.3.13 Country/Region: Peru (Table 4.89)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using a “Lite” version of the EQ-5D-5L valuation protocol 2.1 (see also Chap. 3 for more details). Interviews were conducted between April 2018 and February 2019.
-
(ii)
Sample size; sample frame
1000 interviews with the general population were conducted in three cities located in different parts of Peru: Lima, Arequipa and Iquitos. 300 of these respondents completed a full cTTO + DCE interview, while 700 completed DCE tasks only. Sampling was stratified by region, age and gender. Of the 300 respondents included in the final value set, 49.7% were female and 50.3% were male. The age distribution of the respondents was:
18–24 years | 11.4% |
25–29 years | 16.2% |
30–39 years | 20.9% |
40–49 years | 19.1% |
50–64 years | 17.3% |
65–74 years | 14.1% |
75+ years | 1.0% |
-
(iii)
Representativeness of achieved sample (Table 4.90)
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.91)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.46)
-
(vi)
Exclusion criteria
Respondents were excluded if they did not belong to the age range that was intended to be sampled (18–75 years old). Furthermore, respondents were excluded if they did not live in a household selected through the sampling strategy. A total of 30 respondents were excluded for these reasons.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1000 interviews were conducted by 12 interviewers. 5 interviewers performed cTTO + DCE interviews, while the other 7 interviewers conducted DCE interviews only. The variance of the responses included in the final value set can be partitioned into variance related to differences between interviewers (0.7%), respondents (27.5%) and responses (71.8%).
-
(viii)
Description of modelling choices
The Peruvian EQ-5D-5L value set was based on the cTTO data only. The selected model was a Tobit model, that accounts for censoring at −1, with a correction for heteroskedasticity. The model was additionally adjusted by differential weights to improve the representativeness of the sample compared to the general population in Peru. The intercept was constrained in the final model.
- (ix)

Proportions choosing A based on relative severities of A and B

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
Cost-utility analysis (CUA) is currently not required by the Peruvian Ministry of Health, nor by national insurance agencies (Seguro Integral de Salud and Fondo Intangigle Solidario en Salud). However, previously CUAs have been used for decision making, especially on vaccination recommendations, using weights from other countries (Bolaños-Díaz et al. 2017; Bolaños-Días et al. 2016). Furthermore, researchers at CRONICAS institute for chronic diseases have been using the Peruvian EQ-5D-5L values in ongoing research. The National HTA Network, Red Nacional de Evaluación de Tecnologías Sanitarias (RENETSA), currently makes no specific recommendation on the use of EQ-5D-5L in economic evaluations in health care.
-
(xi)
Reference(s) of value set
Augustovski F, Belizán M, Gibbons L, Reyes N, Stolk E, Craig BM, Tejada RA (2020) Peruvian Valuation of the EQ-5D-5L: A Direct Comparison of Time Trade-Off and Discrete Choice Experiments. Value Health 23(7):880–888
Further Literature
-
Bolaños-Díaz R, Tejada RA, Sanabria C, Escobedo-Palza S (2017) Cost-Effectiveness of two antiviral therapies for chronic Hepatitis B in Peru: Entecavir and Tenofovir. Rev Peru Med Exp Salud Publica 34(3):377–385
-
Bolaños-Díaz R, Tejada RA, Beltrán J, Escobedo-Palza S (2016) Evaluation of the cost-effectiveness of two alternative human papillomavirus vaccines as prophylaxis against uterine cervical cancer. Rev Peru Med Exp Salud Publica 33(3):411–418.
-
Instituto Nacional de Estadística e Informática (2017) Censos Nacionales. https://www.inei.gob.pe/. Accessed 29 July 2021
4.3.3.14 Country/Region: United States (Table 4.93)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 2.1. Interviews were conducted between May and September 2017.
-
(ii)
Sample size; sample frame
1134 interviews with the general population were conducted in 6 US metropolitan areas: Chicago, Philadelphia, Seattle, Birmingham, Phoenix, and Denver. Quota sampling with respect to age, gender, ethnicity, and race was applied based on the US census (US Census Bureau 2015). Of the 1062 respondents included in the final value set, 51.0% were female and 48.5% were male. The age distribution of the respondents was:
18-24 years | 9.6% |
25–29 years | 13.8% |
30–39 years | 17.4% |
40–49 years | 17.0% |
50–64 years | 23.1% |
65–74 years | 10.9% |
75+ years | 8.1% |
-
(iii)
Representativeness of achieved sample
The study sample was representative for the US adult population in terms of age, gender, race, ethnicity, prevalence of chronic disease, and general health status (Table 4.94).
-
(iv)
Meactes (Table 4.95)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.48)

Proportions choosing A based on relative severities of A and B

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(vi)
Exclusion criteria
Respondents who did not understand the cTTO tasks (n = 72) were excluded from the analysis, based on interviewer assessment. Moreover, a total of 11.6% of cTTO responses (n = 1234) were removed following the feedback module from respondents who were deemed to have comprehended the task based on interviewer assessment.
-
(vii)
Number of interviewers; Interviewer effects
In total, 1134 interviews were conducted by 11 interviewers. The variance of the responses included in the final value set can be partitioned into variance related to differences between interviewers (0.04%), respondents (35.25%), and responses (64.71%).
-
(viii)
Description of modelling choices
The US EQ-5D-5L value set was based on the cTTO data only. The selected model was a tobit model, left-censored at −1, correcting for heteroskedasticity, and accounting for panel data (i.e., random intercept). Usual activities levels 4 and 5 were constrained to have the same value decrement. The intercept was constrained in the final model because it was non-significant.
- (ix)
-
(x)
Uptake by local HTA/health care decision makers
In the US, the Affordable Care Act prevents the denial of coverage of medical products or services in a manner that treats extending the life of an elderly, disabled, or terminally ill individual as of lower value than extending the life of healthy individuals. However, the absence of drug price regulation and instances of predatory business practices has led to the emergence of the non-profit Institute for Clinical Evaluation and Review as a highly influential organisation that assesses the fairness of drug prices using QALYs as one of the metrics. The EQ-5D-3L forms the basis for many utility inputs and this will likely extend to the EQ-5D-5L as greater use is seen in the literature. In the two years since the US value set was published, the EQ-5D-5L has been employed as an endpoint in clinical trials for pharmaceuticals as well as psychosocial interventions, with evidence that favorably supports its validity/responsiveness for a range of applications and health care interventions (Courtin et al. 2020; Hanmer et al. 2021; Reveille et al. 2021; Xiang et al. 2020).
-
(xi)
Reference(s) for this value set
Pickard AS, Law EH, Jiang R, Pullenayegum E, Shaw JW, Xie F, Oppe M, Boye KS, Chapman RH, Gong CL, Balch A, Busschbach JJV (2019) United States Valuation of EQ-5D-5L Health States Using an International Protocol. Value Health 2(8):931–941
Further Literature
-
Centers for Disease Control and Prevention (CDC) (2018) Data and Statistics. 2018. https://www.cdc.gov/datastatistics/index.html. Accessed 30 Jan 2018
-
Courtin E, Aloisi K, Miller C, Allen HL, Katz LF, Muennig P (2020) The Health Effects Of Expanding The Earned Income Tax Credit: Results From New York City. Health Aff 39(7):1149–1156
-
Li C, Balluz LS, Okoro CA, Strine TW, Lin JMS, Town M, Garvin W, Murphy W, Bartoli W, Valluru B, CDC (2011) Surveillance of certain health behaviors and conditions among states and selected local areas. Behavioral Risk Factor Surveillance System, United States, 2009. MMWR Surveill Summ 60(9):1–250
-
Hanmer J, DeWalt DA, Berkowitz SA (2021) Association between Food Insecurity and Health-Related Quality of Life: a Nationally Representative Survey. J Gen Intern Med 36(6):1638–1647
-
Reveille JD, Hwang MC, Danve A, Kafka S, Peterson S, Lo KH, Kim L, Hsia EC, Chan EK, Deodhar A (2021) The effect of intravenous golimumab on health-related quality of life and work productivity in adult patients with active ankylosing spondylitis: results of the phase 3 GO-ALIVE trial. Clin Rheumatol 40(4):1331–1341
-
US Census Bureau (2015) 2015 American Community Survey 1-Year Estimates. US Census Bureau: Washington, DC
-
Xiang X, Sun Y, Smith S, Lai PHL, Himle J (2020) Internet-Based Cognitive Behavioral Therapy for Depression: A Feasibility Study for Home Care Older Adults. Res Soc Work Prac 30(7):791–801
4.3.3.15 Country/Region: Vietnam (Table 4.97)
The mathematical representation of the model for health state X is:
-
(i)
Date/wave of study
Data were collected in the third wave of EQ-5D-5L valuation studies using the EQ-5D-5L valuation protocol 2.1. The following two adjustments were made to the EQ-VT: (1) the respondent was asked to answer the cTTO tasks for someone like them (“third person”) instead of themselves as per protocol, (2) additional use of printed coloured DCE cards as visual aid. Interviews were conducted between November and December 2017.
-
(ii)
Sample size; sample frame
1200 interviews with the general population were conducted in six provinces, representing different geographical regions: Northern mountains, the Red River delta, the Highlands, Central Coast, the South-East and the Mekong river delta. Multi-stage stratified cluster sampling with respect to region (stage 1) and residential area (stage 2), and a probabilistic quota-based method (stage 3) with respect to age (over 18 years) and gender was applied (Vietnam General Statistic Office 2017). Of the 1200 respondents included in the final value set, 51% were female and 49% were male. The age distribution of the respondents was:
18–24 years | 18.4% |
25–29 years | 15.8% |
30–39 years | 22.9% |
40–49 years | 17.1% |
50–64 years | 19.4% |
65–74 years | 4.8% |
75+ years | 1.7% |
-
(iii)
Representativeness of achieved sample
The study sample was largely representative for the Vietnamese general population in terms of age, gender, and residential area (Table 4.98).
-
(iv)
Mean observed cTTO values of EQ-5D-5L states (Table 4.99)
-
(v)
Proportions choosing A in the DCE based on relative severities of A and B (Fig. 4.50)

Proportions choosing A based on relative severities of A and B
-
(vi)
Exclusion criteria
A total of 8.9% of cTTO responses (n = 1068) were removed following the feedback module; but no respondent’s entire cTTO responses were excluded. The observations of the ten manually added DCE pairs were excluded from the data analysis (details on the DCE design are provided in Chap. 3).
-
(vii)
Number of interviewers; Interviewer effects
In total, 1200 interviews were conducted by 10 interviewers. The variance of the responses can be partitioned into variance related to differences between interviewers (4.0%), respondents (13.7%), and responses (82.3%).
-
(viii)
Description of modelling choices
The Vietnamese EQ-5D-5L value set was based on a hybrid model combining a conditional logit model for the DCE data and a censored at -1 tobit model for the cTTO data. The intercept was constrained in the final model.
- (ix)

Value decrements across dimensions (AD anxiety/depression, MO mobility, PD pain/discomfort, SC self-care, UA usual activities)
-
(x)
Uptake by local HTA/health care decision makers
Vietnam’s Ministry of Health (MOH) has taken a first step toward applying evidence-based medicine to health policy making process by enacting the national HTA guidelines and upgrading the health insurance package with cost-effective drugs based on HTA evidence (Ministry of Health 2017). The MOH has applied evidence-based HTA to produce well-informed healthcare decisions, initially in health insurance. According to the national guideline on HTA submissions, QALY is a required index. QALY estimates can either be sourced from related literature or measured directly using the suggested instrument, EQ-5D-5L. In Vietnam, the EQ-5D-5L is presently the only HRQoL instrument that can produce values which are based on the preferences of the Vietnamese general population (Mai et al. 2020).
-
(xi)
Reference(s) for this value set
Mai VQ, Sun S, Minh HV, Luo N, Giang KB, Lindholm L, Sahlen KG (2020) An EQ-5D-5L Value Set for Vietnam. Qual Life Res 29(7):1923–1933
Further Literature
-
Ministry of Health (2017) Decision 2701/QD-BYT on promulgating the working regulation of drafting committee, editing team and specialized teams, and rules and criteria for formulation of the circular promulgating the list, ratio and payment conditions for modern medicines covered by health insurance. Appendix 2: Rules and criteria for compilation of the list of modern medicines covered by health insurance. https://thuvienphapluat.vn/van-ban/Bao-hiem/Quyet-dinh-2701-QD-BYT-2017-Quy-che-lam-viec-xay-dung-Thong-tu-thuoc-tan-duoc-bao-hiem-y-te-353139.aspx. Accessed 13 July 2021
-
Vietnam General Statistic Office (2017) Statistic Yearbook of Vietnam 2017. GSO, Hanoi. https://www.gso.gov.vn/en/data-and-statistics/2019/10/7559/. Accessed 13 July 2021
Notes
- 1.
With the exception of Peru, where a different health state design for the cTTO was used, as this study was conducted using an EQ-VT ‘Lite’ protocol. A health state design including 31 unique health states was used instead of the 86-state design. For Peru, we therefore report the means of 31 health states.
- 2.
We did not consider correlation between the variance in responses between interviewers, respondents and responses, which is a limitation. However, accounting for correlation between variance in random slopes for interviewers and respondents may be challenging, as not every study may use a number of interviewers that is sufficiently large to be able to compute these correlations reliably.
- 3.
The ICC partitions variance into shares attributed to interviewers, respondents and responses. This is a way of operationalising interviewer effects, as it measures the share of variance caused by differences between interviewers. Small differences in distributions reflect good agreement between interviewers, and therefore small interviewer effects. However, they do not necessarily reflect good data quality only, as other factors, such as clustering of values and inconsistent responses are not captured by this measure.
- 4.
MO45, SC45, UA45, PD45 and AD45 are dummy variables that equal 1 when level 4 or 5 problems are reported in that dimension, and 0 otherwise. For example, SC45 will equal 1 in state 14111, but 0 in state 12111. Num45sq is a variable that represents the square of the number of level 4 or 5 problems in a health state, beyond the first.
- 5.
It was not possible to compute the variance attributed to differences between interviewers, as interviewers shared login information for the software used to conduct the interviews. Therefore, it is not possible to differentiate between interviewers.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2022 The Author(s)
About this chapter

Cite this chapter
Roudijk, B., Ludwig, K., Devlin, N. (2022). EQ-5D-5L Value Set Summaries. In: Devlin, N., Roudijk, B., Ludwig, K. (eds) Value Sets for EQ-5D-5L. Springer, Cham. https://doi.org/10.1007/978-3-030-89289-0_4
Download citation
DOI: https://doi.org/10.1007/978-3-030-89289-0_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-89288-3
Online ISBN: 978-3-030-89289-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)