
Abstract
Aims/hypothesis
Obesity is characterised by increased triacylglycerol storage in adipose tissue. There is in vitro evidence for a blunted beta-adrenergically mediated lipolytic response in abdominal subcutaneous adipose tissue (SAT) of obese individuals and evidence for this at the whole-body level in vivo. We hypothesised that the beta-adrenergically mediated effect on lipolysis in abdominal SAT is also impaired in vivo in obese humans.
Methods
We investigated whole-body and abdominal SAT glycerol metabolism in vivo during 3 h and 6 h [2H5]glycerol infusions. Arterio–venous concentration differences were measured in 13 lean and ten obese men after an overnight fast and during intravenous infusion of the non-selective beta-adrenergic agonist isoprenaline [20 ng (kg fat free mass)−1 min−1].
Results
Lean and obese participants showed comparable fasting glycerol uptake by SAT (9.7 ± 3.4 vs 9.3 ± 2.5% of total release, p = 0.92). Furthermore, obese participants showed an increased whole-body beta-adrenergically mediated lipolytic response versus lean participants. However, their fasting lipolysis was blunted [glycerol rate of appearance: 7.3 ± 0.6 vs 13.1 ± 0.9 μmol (kg fat mass)−1 min−1, p < 0.01], as was the beta-adrenergically mediated lipolytic response per unit SAT [Δ total glycerol release: 140 ± 71 vs 394 ± 112 nmol (100 g tissue)−1 min−1, p < 0.05] compared with lean participants. Net triacylglycerol flux tended to increase in obese compared with lean participants during beta-adrenergic stimulation [Δ net triacylglycerol flux: 75 ± 32 vs 16 ± 11 nmol (100 g tissue)−1 min−1, p = 0.06].
Conclusions/interpretation
We demonstrated in vivo that beta-adrenergically mediated lipolytic response is impaired systematically and in abdominal SAT of obese versus lean men. This may be important in the development or maintenance of increased triacylglycerol stores and obesity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Obesity is characterised by excess fat storage in adipose tissue, in the form of triacylglycerol (TAG). A blunted fat mobilisation, due to decreased adipose tissue lipolysis, might be an important factor contributing to the development or maintenance of the expanded adipose tissue mass in obesity. Fasting lipolysis per unit of lean body mass has been reported to be increased in obesity, whereas a decrease is reported when expressed per unit of fat mass (FM) [1]. The hormonal regulation of lipolysis is still under debate. There is strong evidence from in vitro and in vivo studies for the existence of lipolytic resistance to catecholamines in obese individuals. Blunted whole-body catecholamine-induced lipolysis has been shown in vivo in obese persons [2, 3]. This impaired lipolysis did not improve after weight reduction [4]. Furthermore, a decreased lipolytic response to catecholamines is a feature of childhood-onset obesity [5, 6] and is also present in adipocytes from first-degree relatives of obese persons [7]. These observations suggest that catecholamine resistance of lipolysis may be an important early, and perhaps primary factor, in the development of obesity. In vitro catecholamine resistance of lipolysis was reported in subcutaneous adipocytes of men and women with upper-body obesity, in relation with a decreased cell surface density of β2-adrenoceptors [8]. We hypothesised that beta-adrenergically mediated lipolytic response at the whole-body and abdominal subcutaneous adipose tissue (SAT) level is impaired in vivo in obese persons. If so, this might contribute to the increased fat storage in this adipose tissue depot.
To obtain an accurate estimation of lipolysis, state-of-the-art [2H5]glycerol tracer methodology in combination with the measurement of arterio–venous concentration differences across abdominal SAT was used. Obese and lean male control participants were investigated after an overnight fast and during catecholamine stimulation using the non-selective beta-adrenergic agonist isoprenaline. The primary outcome measures of the present study were glycerol rate of appearance (R a) and glycerol exchange across abdominal SAT. A methodological issue that arises when determining local adipose tissue glycerol release is the possibility that adipose tissue may also take up small amounts of glycerol [9]. A pilot study was performed to determine the time period required to obtain a steady-state in glycerol enrichment in both arterialised and venous blood draining from adipose tissue, since a lack of isotopic equilibration may explain previous discrepant findings on glycerol uptake [10].
Methods
Participants
Three lean (two women and one man; BMI < 25 kg/m2) participants took part in a pilot experiment, during which [2H5]glycerol enrichment was measured for 6 h to determine the time required for obtaining an isotopic steady-state. Thirteen lean (BMI < 25 kg/m2) and ten obese (BMI ≥ 30 kg/m2) non-smoking normotensive men participated in the actual SAT lipolysis study, during which [2H5]glycerol was infused for a 3 h period. Clinical characteristics of the participants are summarised in Table 1. Body weight and body density were determined after an overnight fast, as previously described [11]. All participants were in good health as assessed by their medical history, free of any medication and spent no more than 3 h/week in organised sports activities. The Medical Ethical Committee of Maastricht University approved the study protocol and all participants gave their written informed consent before participating in the study.
Experimental protocol
Pilot study
The time course in [2H5]glycerol enrichment was determined in order to identify when steady-state levels were achieved (n = 3). Glycerol enrichment was measured in arterialised blood and blood draining the abdominal SAT (adipose vein) during primed (3 μmol/kg) constant infusion for 6 h of [2H5]glycerol (0.20 μmol kg−1 min−1). Blood samples were taken simultaneously from the two sites, both at baseline before the start of the tracer infusion (t0 min), and at ten time points during glycerol infusion (t60, t90, t120, t150, t180, t210, t240, t330, t345, t360 min).
Whole-body and SAT lipolysis study
Glycerol enrichment and exchange across abdominal SAT were investigated during primed (3 μmol/kg) constant infusion of [2H5]glycerol for 3 h (0.20 μmol kg−1 min−1). Following a 120 min baseline period, isoprenaline was infused at a rate of 20 ng [kg fat free mass (FFM)]−1 min−1 for 60 min. During the experiment, heart rate was recorded continuously by means of a three-lead ECG. When heart rate increased by more than 40 beats per min or in the event of ECG irregularities, isoprenaline infusion was stopped (n = 2, one lean and one obese participant). Before the start of the tracer infusion an arterialised blood sample was taken for background enrichment. Blood samples were also taken simultaneously from the arterialised and adipose vein at three baseline time points (t90, t105 and t120 min) and at three time points during the last 30 min of isoprenaline infusion (t150, t165 and t180 min). Adipose tissue blood flow (ATBF) was monitored continuously using the 133Xe washout technique [12]. ATBF results have been published previously in another context [13].
Clinical methods
All participants were asked to refrain from drinking alcohol and to perform no strenuous exercise for 24 h before the study. Participants came to the laboratory by car or bus at 08:00 hours after an overnight fast. Three cannulas were inserted before the start of the experiment. Arterialised venous blood was obtained through a 20-gauge cannula inserted retrogradely into a superficial dorsal hand vein. The hand was warmed in a hotbox, which was maintained at 60°C to achieve adequate arterialisation [14]. In the same arm, a second cannula was inserted in a forearm antecubital vein for the infusion of [2H5]glycerol tracer and the non-selective beta-adrenergic agonist isoprenaline at a rate of 20 ng (kg FFM)−1 min−1. At this infusion rate, plasma isoprenaline concentrations are comparable in lean and obese participants [3]. Finally, the veins on the anterior abdominal wall were identified by means of a fibre-optic light source. In order to obtain adipose tissue venous blood, a 10 cm 22-gauge catheter (Central venous catheter kit Seldinger technique; Becton Dickinson, Alphen aan den Rijn, the Netherlands) was introduced anterogradely over a guide wire into one of the superficial veins and threaded towards the groin, so that its tip lay just superior to the inguinal ligament [15]. This method provides the drainage from the adipose tissue of the abdomen, uncontaminated by muscle drainage and with only a minor contribution from skin [15]. The adipose vein was kept patent by continuous saline (9 g/l NaCl) infusion at a rate of 80 ml/h. The participants rested in a supine position for the duration of the study.
Analytical methods
A small portion of blood was used to measure oxygen saturation (%HbO2) and ensure adequate arterialisation (ABL510; Radiometer, Copenhagen, Denmark). Blood was collected in tubes containing EDTA and immediately centrifuged for 10 min at 1,000g, 4°C. The plasma was removed for enzymatic colorimetric quantification of NEFA (NEFA C kit; Wako, Neuss, Germany), glycerol (Boehringer, Mannheim, Germany) and TAG (Sigma, St Louis, MO, USA) on a centrifugal spectrophotometer (Cobas Fara; Roche Diagnostica, Basel, Switzerland). Plasma glucose concentration (ABX Diagnostics, Montpellier, France) was measured on an automated spectrophotometer (Cobas Mira; Roche Diagnostica). Plasma insulin was measured with a double antibody radioimmunoassay (Linco Research, St Charles, MO, USA). Insulin sensitivity was assessed by the homeostasis model assessment index for insulin resistance, calculated from fasting glucose and insulin [16]. Packed cell volume was measured using a microcapillary system (Hirschmann Laborgeräte, Eberstadt, Germany).
Isotope enrichment
To determine isotopic enrichment of glycerol, samples first were derivatised. Acetone (1 ml) was added to 150 μl plasma and each tube was vortexed for 2 min and centrifuged for 20 min at 17,500g, 4°C. The supernatant fraction was transferred to a clean tube and dried under nitrogen at 37°C and derivatised by adding 80 μl ethyl acetate (cat. no. 45765; Sigma-Aldrich, Seelze, Germany) and 80 μl heptafluorobutyric acid anhydride (cat. no. 63164; Pierce Biotechnology, Rockford, IL, USA). The tubes were vortexed for 2 min and incubated for 1 h at 70°C. Samples were than rotated end over end for 5 min at 25°C and evaporated under nitrogen at room temperature. Ethyl acetate (70 μl) was added before injection into the GC-MS (Finnigan MAT 252, Bremen, Germany) for measurement of glycerol enrichment. Stable isotope enrichment was analysed by selectively monitoring the mass to charge ratio (m/z) of molecular ions 253 and 257 for glycerol [17].
Calculations
The net exchange (flux) of metabolites across abdominal SAT was calculated by multiplying the arterio–venous concentration difference of metabolites by adipose tissue plasma flow. Plasma flow was calculated as ATBF×(1–packed cell volume), with packed cell volume expressed as a fraction. A positive net flux indicates net uptake from plasma, whereas a negative net flux indicates net tissue release.
The expected adipose vein enrichment, in case of no glycerol uptake, was calculated as arterialised enrichment multiplied by arterialised glycerol concentration divided by the measured adipose vein enrichment.
The R a of glycerol was calculated according to the following steady-state equation:
where TTR is tracer/tracee ratio and F is the isotope infusion rate (μmol kg−1 min−1).
The fractional extraction (fract) of glycerol across abdominal SAT was calculated by dividing the arterio–venous concentration difference of [2H5]glycerol by the arterialised [2H5]glycerol concentration. Abdominal SAT total glycerol uptake was calculated as follows:
where the units are nmol (100 g tissue)−1 min−1; (glycerolart) is arterialised glycerol concentration (μmol/l); and ATBF is in ml (100 g tissue)−1 min−1. Abdominal SAT total glycerol release was calculated from the formula:
Statistical analysis
Baseline fasting values and changes (Δbeta-adrenergic stimulation to baseline) were compared between groups (obese vs lean) using Student’s unpaired t test. Statistical calculations were performed with SPSS for Macintosh (version 11.0; SPSS, Chicago, IL, USA). Data are presented as mean ± SEM. A value of p < 0.05 was considered statistically significant.
Results
Characteristics
Obese participants had significantly higher BMI, FM, waist to hip ratio, fasting circulating TAG and insulin concentrations than their lean counterparts (Tables 1 and 2).
Tracer/tracee ratio
In the pilot experiment, the tracer/tracee ratios (TTR) obtained during a 6 h [2H5]glycerol infusion after an overnight fast were examined (n = 3). Arterialised and adipose vein TTR reached a steady-state after 1 h of infusion (Fig. 1). Mean values are presented, as all participants (n = 3) showed the same pattern. The measured adipose vein enrichment was consistently lower than the expected enrichment, implying uptake of glycerol by adipose tissue. In the actual SAT lipolysis experiment (3 h [2H5]glycerol infusion), TTR also reached a steady-state after 1 h and remained stable during isoprenaline infusion. Data in lean and obese men were comparable (data not shown).

Plasma glycerol TTR during 6 h primed constant infusion of [2H5]glycerol (n = 3) in arterialised blood (squares) and blood draining from abdominal SAT (adipose vein; black circles). White circles, expected adipose vein enrichment. The measured adipose vein enrichment was consistently lower than the expected enrichment
Circulating metabolites
Beta-adrenergic stimulation with isoprenaline increased arterialised TAG concentrations in obese participants, while in lean participants TAG concentrations decreased during isoprenaline infusion (Table 2). Thus, the change in arterialised TAG concentrations from baseline to isoprenaline was different between obese and lean participants (ΔTAG obese vs lean, 100 ± 37 vs −45 ± 22 μmol/l, p < 0.05; Table 2).
Furthermore, beta-adrenergic stimulation increased arterialised NEFA and glycerol concentrations in lean and obese participants. The beta-adrenergic mediated increase in arterialised NEFA (ΔNEFA 454 ± 68 vs 271 ± 46 μmol/l, p < 0.05) and glycerol concentration (Δglycerol 40 ± 8 vs 15 ± 5 μmol/l, p < 0.05) was more pronounced in obese than in lean participants (Table 2), suggesting a higher whole-body lipolytic response in the former. Indeed, beta-adrenergic stimulation increased whole-body glycerol R a in lean and obese participants (Table 2), this increase tending to be higher in the obese group (Δglycerol R a obese vs lean: 172 ± 19 vs 109 ± 13 μmol/min, p = 0.07; Table 2). Expressed per unit of FM, fasting glycerol R a was significantly reduced in obese compared with lean participants (p < 0.05; Table 2). Interestingly, the beta-adrenergically mediated increase in glycerol R a per unit of FM was significantly blunted in obese participants [Δglycerol R a per unit FM: 5.4 ± 0.9 vs 7.7 ± 1.5 μmol (kg FM)−1 min−1, p < 0.05] (Table 2), suggesting a blunted lipolytic response per unit of FM in obese participants.
Finally, beta-adrenergic stimulation increased arterialised insulin concentrations in lean and obese participants (Table 2). This increase in circulating insulin levels was significantly higher in obese than in lean participants (Δinsulin 62 ± 13 vs 25 ± 4 pmol/l, p < 0.05; Table 2).
Abdominal SAT lipolysis
Glycerol uptake by abdominal SAT was observed in lean and obese participants after an overnight fast (Fig. 2a). Fractional extraction of [2H5]glycerol from the circulation (lean vs obese, 16.6 ± 4.5 vs 13.9 ± 6.7%) and total glycerol uptake expressed relative to total glycerol release were very small (lean vs obese, 9.7 ± 3.4 vs 9.3 ± 2.5% of total release) with no significant difference between lean and obese participants (p = 0.74 and p = 0.92, respectively). Adipose tissue total glycerol uptake increased during beta-adrenergic stimulation in lean and obese participants, but this increase was not significantly different between groups [Δ total glycerol uptake obese vs lean, 4 ± 9 vs 21 ± 5 nmol (100 g tissue)−1 min−1, p = 0.15] (Fig. 2a). The increased total glycerol uptake during beta-adrenergic stimulation appeared to be partly explained by the increase in ATBF (r = 0.633, p < 0.05).

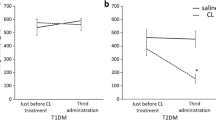
Total glycerol uptake (a) and release (b) across abdominal SAT after an overnight fast (black bars) and during beta-adrenergic stimulation (white bars) in obese vs lean participants during 3 h [2H5]glycerol infusion. Values are mean ± SEM. *p < 0.05 for change (Δ) from baseline obese vs lean
Fasting net glycerol and NEFA release across abdominal SAT were comparable between lean and obese participants (Table 3). Beta-adrenergic stimulation increased net NEFA and glycerol release across abdominal SAT to a greater extent in lean than in obese participants, although changes were not significantly different between groups (Table 3). In line with these findings, the beta-adrenergically mediated increase in total glycerol release across abdominal SAT was blunted in the obese group [Δ total glycerol release obese vs lean, 140 ± 71 vs 394 ± 112 nmol (100 g tissue)−1 min−1, p < 0.05] (Fig. 2b), suggesting a blunted lipolytic response per unit of abdominal SAT in obese participants. Finally, obese men tended to show an increased net TAG flux across abdominal SAT during beta-adrenergic stimulation [Δ net TAG flux obese vs lean, 75 ± 32 vs 16 ± 11 nmol (100 g tissue)−1 min−1, p = 0.06] (Table 3).
Discussion
The present study was designed to investigate in vivo whole-body and abdominal SAT lipolysis in obese and lean men. To our knowledge, this is the first study to show in vivo that obese participants have a blunted beta-adrenergically mediated lipolytic response per unit of adipose tissue.
Methodological considerations
A point of discussion with studies on glycerol uptake and release using tracer methodology is the infusion time of the labelled glycerol. In previous studies, the infusion time was relatively short (1–3 h), raising the question of whether equilibration between labelled glycerol and the adipose tissue glycerol pool is complete or not [9, 10]. We investigated glycerol enrichment during a 3 h and 6 h period of [2H5]glycerol infusion. Steady-state levels in labelled [2H5]glycerol were achieved in arterialised and adipose vein enrichment after 1 h and remained constant for the subsequent 5 h. Thus, our data support the use of a relatively short infusion time (1 h) for study of glycerol metabolism.
Glycerol uptake
The present data show a slight glycerol uptake by abdominal SAT of lean and obese participants. Glycerol uptake was not significantly different between lean and obese participants. Uptake and dilution of [2H5]glycerol across abdominal SAT has been shown previously during 1 h [9] of tracer infusion. In this study, the dilution of the labelled glycerol was consistently greater than expected from the measured net release of glycerol, indicating significant uptake of glycerol by adipose tissue. In line with this study, we observed a two- to fivefold higher glycerol enrichment in arterialised than in venous blood draining adipose tissue. The observed enrichment in venous blood was universally lower than that predicted from the net addition of glycerol to venous blood. This indicates that an exchange must occur between enriched glycerol in the blood and the unenriched non-esterified glycerol pool in adipose tissue. In contrast, some studies were unable to detect significant uptake of glycerol by adipose tissue after 1 h of tracer infusion [10]. The reason for this apparent discrepancy remains to be elucidated. It should be mentioned that glycerol uptake is low in human adipose tissue as is the activity of the enzyme glycerol kinase [18]. This enzyme is responsible for the phosphorylation of glycerol into glycerol 3-phosphate, making it available for re-esterification.
Abdominal SAT lipolytic response to beta-adrenergic stimulation
A blunted isoprenaline-induced increase in total glycerol release per unit abdominal SAT was observed in obese men, indicating that in vivo beta-adrenergic mediated lipolytic response in abdominal SAT of obese participants is blunted. Our data are consistent with evidence of catecholamine resistance in vitro and in situ in obese individuals [2–4], in children with obesity [5, 6] and also in relatives of obese individuals [7]. Defects in catecholamine signal transduction have been observed at the β2-adrenoceptor level and further downstream or directly involving hormone-sensitive lipase [8, 19–22]. However, from our experiments it is not possible to determine at which level the observed defect is located. Interestingly, catecholamine resistance has been observed in adipose tissue of first-degree relatives of obese participants [7] and persists after weight reduction [4], suggesting that catecholamine resistance may be a primary defect in obesity. Furthermore, plasma insulin concentrations may play an important role in regulating lipolysis [23]. Therefore, we cannot fully rule out the possibility that the blunted lipolytic response per unit adipose tissue mass that we observed is a secondary phenomenon, due to the higher degree of hyperinsulinaemia during beta-adrenergic stimulation in obese compared with lean participants. However, this explanation seems unlikely, since a blunted in situ lipolytic response in abdominal SAT of obese women was still observed when the confounding influence of hyperinsulinaemia had been excluded using a pancreatic hormonal clamp [2].
In contrast to the present study, two in situ microdialysis studies performed in men found that the increase in interstitial glycerol during isoprenaline administration did not differ between lean and obese individuals [24, 25]. A possible explanation for this is that in microdialysis studies interstitial glycerol is used as a measure of lipolysis. Since glycerol is taken up by adipose tissue, interstitial glycerol concentration may not reflect the overall rate of lipolysis. Rather, it may be the net result of TAG and glycerol metabolism, thus reflecting net glycerol turnover [26].
Whole-body beta-adrenergically mediated lipolytic response
Whole-body lipolytic response during isoprenaline infusion tended to be higher in obese participants. This was reflected by a higher increase in circulating NEFA and glycerol concentrations during beta-adrenergic stimulation in obese than in lean participants. Expressed per unit of FM, beta-adrenergically mediated lipolysis (glycerol R a) was significantly lower in obese than in lean men. This suggests that the increased whole-body beta-adrenergically mediated lipolytic response in obese individuals is directly linked to the increased adipose tissue mass, as has been shown before in upper body obese women [2]. Increased release of NEFA into the circulation increases NEFA delivery to the liver, resulting in increased hepatic VLDL-TAG output and hence increased circulating TAG levels during beta-adrenergic stimulation, as was observed in our obese participants. The control of whole-body lipid metabolism is, to a large extent, dependent on the efficient regulation of lipid metabolism in adipose tissue and the liver. Moreover, hepatic VLDL-TAG is a precursor of TAG stored in adipose tissue [27, 28]. Consequently, a greater VLDL-TAG delivery to adipose tissue and greater lipoprotein lipase-mediated hydrolysis might explain the tendency towards increased positive TAG flux across abdominal SAT of obese participants during beta-adrenergic stimulation. Our observation is in agreement with a study by Samra et al. [29] showing an increased rate of action of lipoprotein lipase during epinephrine infusion. These in vivo findings are in contrast with in vitro studies showing that lipoprotein lipase expression and activity are suppressed by epinephrine [30, 31]. Future studies are needed to elucidate whether an increased TAG flux across SAT might contribute to the increased TAG storage in adipose tissue of obese participants.
Conclusion
The present study demonstrates in vivo that obese men have a blunted beta-adrenergically mediated lipolytic response in abdominal SAT. Therefore, a blunted lipolysis during beta-adrenergic stimulation may be an important factor in the development or maintenance of increased TAG stores and obesity.
Abbreviations
- ATBF:
-
adipose tissue blood flow
- FFM:
-
fat free mass
- FM:
-
fat mass
- R a :
-
glycerol rate of appearance
- SAT:
-
abdominal subcutaneous adipose tissue
- TAG:
-
triacylglycerol
- TTR:
-
tracer/tracee ratio
References
Campbell PJ, Carlson MG, Nurjhan N (1994) Fat metabolism in human obesity. Am J Physiol 266:E600–E605
Horowitz JF, Klein S (2000) Whole body and abdominal lipolytic sensitivity to epinephrine is suppressed in upper body obese women. Am J Physiol Endocrinol Metab 278:E1144–E1152
Blaak EE, Van Baak MA, Kemerink GJ, Pakbiers MT, Heidendal GA, Saris WH (1994) beta-Adrenergic stimulation of energy expenditure and forearm skeletal muscle metabolism in lean and obese men. Am J Physiol 267:E306–E315
Blaak EE, Van Baak MA, Kemerink GJ, Pakbiers MT, Heidendal GA, Saris WH (1994) beta-Adrenergic stimulation of skeletal muscle metabolism in relation to weight reduction in obese men. Am J Physiol 267:E316–E322
Bougneres P, Stunff CL, Pecqueur C, Pinglier E, Adnot P, Ricquier D (1997) In vivo resistance of lipolysis to epinephrine. A new feature of childhood onset obesity. J Clin Invest 99:2568–2573
Enoksson S, Talbot M, Rife F, Tamborlane WV, Sherwin RS, Caprio S (2000) Impaired in vivo stimulation of lipolysis in adipose tissue by selective beta2-adrenergic agonist in obese adolescent girls. Diabetes 49:2149–2153
Hellstrom L, Langin D, Reynisdottir S, Dauzats M, Arner P (1996) Adipocyte lipolysis in normal weight subjects with obesity among first-degree relatives. Diabetologia 39:921–928
Reynisdottir S, Wahrenberg H, Carlstrom K, Rossner S, Arner P (1994) Catecholamine resistance in fat cells of women with upper-body obesity due to decreased expression of beta 2-adrenoceptors. Diabetologia 37:428–435
Kurpad A, Khan K, Calder AG et al (1994) Effect of noradrenaline on glycerol turnover and lipolysis in the whole body and subcutaneous adipose tissue in humans in vivo. Clin Sci (Lond) 86:177–184
Coppack SW, Persson M, Judd RL, Miles JM (1999) Glycerol and nonesterified fatty acid metabolism in human muscle and adipose tissue in vivo. Am J Physiol 276:E233–E240
Goossens GH, Blaak EE, Saris WH, van Baak MA (2004) Angiotensin II-induced effects on adipose and skeletal muscle tissue blood flow and lipolysis in normal-weight and obese subjects. J Clin Endocrinol Metab 89:2690–2696
Larsen OA, Lassen NA, Quaade F (1966) Blood flow through human adipose tissue determined with radioactive xenon. Acta Physiol Scand 66:337–345
Goossens GH, Jocken JW, Blaak EE, Schiffers PM, Saris WH, van Baak MA (2007) Endocrine role of the renin–angiotensin system in human adipose tissue and muscle: effect of beta-adrenergic stimulation. Hypertension 49:542–547
Abumrad NN, Rabin D, Diamond MP, Lacy WW (1981) Use of a heated superficial hand vein as an alternative site for the measurement of amino acid concentrations and for the study of glucose and alanine kinetics in man. Metabolism 30:936–940
Frayn KN, Coppack SW, Humphreys SM, Whyte PL (1989) Metabolic characteristics of human adipose tissue in vivo. Clin Sci (Lond) 76:509–516
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC (1985) Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28:412–419
Blaak EE, Wagenmakers AJ, Glatz JF et al (2000) Plasma FFA utilization and fatty acid-binding protein content are diminished in type 2 diabetic muscle. Am J Physiol Endocrinol Metab 279:E146–E154
Tan GD, Debard C, Tiraby C et al (2003) A “futile cycle” induced by thiazolidinediones in human adipose tissue? Nat Med 9:811–812; author reply 812
Reynisdottir S, Ellerfeldt K, Wahrenberg H, Lithell H, Arner P (1994) Multiple lipolysis defects in the insulin resistance (metabolic) syndrome. J Clin Invest 93:2590–2599
Large V, Reynisdottir S, Langin D et al (1999) Decreased expression and function of adipocyte hormone-sensitive lipase in subcutaneous fat cells of obese subjects. J Lipid Res 40:2059–2066
Lofgren P, Hoffstedt J, Ryden M et al (2002) Major gender differences in the lipolytic capacity of abdominal subcutaneous fat cells in obesity observed before and after long-term weight reduction. J Clin Endocrinol Metab 87:764–771
Schiffelers SL, Saris WH, Boomsma F, van Baak MA (2001) beta(1)- and beta(2)-Adrenoceptor-mediated thermogenesis and lipid utilization in obese and lean men. J Clin Endocrinol Metab 86:2191–2199
Karpe F, Tan GD (2005) Adipose tissue function in the insulin-resistance syndrome. Biochem Soc Trans 33:1045–1048
Borsheim E, Lonnroth P, Knardahl S, Jansson PA (2000) No difference in the lipolytic response to beta-adrenoceptor stimulation in situ but a delayed increase in adipose tissue blood flow in moderately obese compared with lean men in the postexercise period. Metabolism 49:579–587
Schiffelers SL, Akkermans JA, Saris WH, Blaak EE (2003) Lipolytic and nutritive blood flow response to beta-adrenoceptor stimulation in situ in subcutaneous abdominal adipose tissue in obese men. Int J Obes Relat Metab Disord 27:227–231
Sjostrand M, Gudbjornsdottir S, Holmang A, Strindberg L, Ekberg K, Lonnroth P (2002) Measurements of interstitial muscle glycerol in normal and insulin-resistant subjects. J Clin Endocrinol Metab 87:2206–2211
Havel RJ, Kane JP, Balasse EO, Segel N, Basso LV (1970) Splanchnic metabolism of free fatty acids and production of triglycerides of very low density lipoproteins in normotriglyceridemic and hypertriglyceridemic humans. J Clin Invest 49:2017–2035
Bulow J, Simonsen L, Wiggins D et al (1999) Co-ordination of hepatic and adipose tissue lipid metabolism after oral glucose. J Lipid Res 40:2034–2043
Samra JS, Simpson EJ, Clark ML et al (1996) Effects of epinephrine infusion on adipose tissue: interactions between blood flow and lipid metabolism. Am J Physiol 271:E834–E839
Yukht A, Davis RC, Ong JM, Ranganathan G, Kern PA (1995) Regulation of lipoprotein lipase translation by epinephrine in 3T3-L1 cells. Importance of the 3′ untranslated region. J Clin Invest 96:2438–2444
Ong JM, Saffari B, Simsolo RB, Kern PA (1992) Epinephrine inhibits lipoprotein lipase gene expression in rat adipocytes through multiple steps in posttranscriptional processing. Mol Endocrinol 6:61–69
Acknowledgements
The authors greatly appreciate the technical support of P. van der Baan and the willingness of the volunteers to participate in this study. This research was supported by a grant from the Netherlands Organization for Scientific Research (NWO/ZonMw contract no. 015.01.095) to E. E. Blaak.
Duality of interest statement
The authors declare that there is no duality of interest associated with this manuscript.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Jocken, J.W.E., Goossens, G.H., van Hees, A.M.J. et al. Effect of beta-adrenergic stimulation on whole-body and abdominal subcutaneous adipose tissue lipolysis in lean and obese men. Diabetologia 51, 320–327 (2008). https://doi.org/10.1007/s00125-007-0866-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-007-0866-y