
Abstract
There are several non-invasive methods to study endothelial function, but their interrelation and association to cardiovascular risk have not been well evaluated. We studied macrovascular and microvascular endothelial function simultaneously in different vascular beds in relation to cardiovascular mortality risk (Systematic Coronary Risk Evaluation, SCORE) and hypertension induced cardiac organ damage, and their interrelationship. The study investigated 71 hypertensive patients by forearm post-ischemic flow-mediated vasodilation, pulse wave analysis (applanation tonometry) and beta 2-adrenoceptor agonist stimulation for changes in reflection index, skin microvascular reactivity by laser Doppler fluxmetry with iontophoresis and heat-induced hyperaemia, and coronary microvascular function by subendocardial viability ratio (derived from pulse wave analysis). Flow mediated vasodilation related inversely to SCORE (r = 0.34, P = 0.011). Adding microalbuminuria and pulse wave velocity strengthened the associations. Pulse wave reflection changes did not relate to SCORE. Skin microvascular reactivity related inversely to SCORE (peak flux change to sodium nitroprusside r = 0.29, P = 0.033, and to heating r = 0.31, P = 0.018). Subendocardial viability ratio did not relate to SCORE. Endothelial function indices showed no consistent relation to cardiac target organ damage. The agreement between the different methods for evaluating indices of macrovascular and microvascular endothelial function was weak. In conclusion, indices of macrovascular and microvascular endothelial function relate to cardiovascular mortality risk. Their use may improve cardiovascular risk prediction in hypertension. However, methods representing different vascular beds show little interrelationship and are not interchangeable, which may depend on different pathogenetic mechanisms representing different aspects of future cardiovascular risk.
Trial registry: NCT02901977
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Impaired endothelial function can detect early disturbances in vascular function that precede symptomatic atherosclerotic disease. Changes in forearm blood flow during intra-arterial infusion of acetylcholine (Ach) and sodium nitroprusside (SNP) to induce endothelium dependent and endothelium independent vasodilatation, respectively, have been used to assess endothelial function representing mainly resistance arteries, and reveal that endothelial dysfunction is associated with risk of future atherosclerotic cardiovascular events in the general population and in hypertension [1, 2]. Endothelial function can also be evaluated by non-invasive techniques. Forearm post-ischemic hyperaemia induced flow mediated vasodilatation (FMD) is often used to assess endothelial function representing conduit arteries. FMD is also related to invasively assessed coronary artery endothelial function and coronary flow reserve [3, 4]. Impaired FMD predicts risk of future cardiovascular events in the general population, and in patients with hypertension or with atherosclerotic disease in some [5,6,7], but not all [8, 9] studies. Beta 2-adrenoceptor agonist stimulation induces endothelial dependent vasodilation and changes pulse wave reflection, which can be expressed as the change in augmentation index derived from the first reflected wave, or from the relative height of the first diastolic reflective wave [2, 10]. This non-invasive technique assesses endothelial function representing resistance arteries. A blunted response is associated with coronary artery disease, hypercholesterolemia, and diabetes [10, 11].
Non-invasive methods are also available to assess microvascular function in man. Skin microvascular reactivity can be evaluated by laser Doppler fluxmetry (LDF) and transdermal iontophoretic application of Ach and SNP to represent endothelium dependent and endothelium independent vasodilatation, respectively, or by the maximum hyperaemic response to local heating or following arterial occlusion [12, 13]. Hypertensive patients show impaired forearm skin microvascular reactivity with signs of endothelial dysfunction together with structural and functional capillary rarefaction [12, 14]. In addition, disturbed skin microvascular reactivity is associated with coronary heart disease and incident type 2 diabetes [15, 16]. Microvascular function in the coronary circulation can be assessed by the subendocardial viability ratio (SEVR), which can be calculated from pulse wave analysis and tonometry, to reflect an index of myocardial oxygen supply and demand. A lower SEVR, representing impaired subendocardial perfusion, is associated with a reduced coronary flow reserve [17, 18] and can predict cardiovascular mortality and end stage renal disease in patients with type 1 diabetes and in chronic kidney disease [19, 20].
A simple way to assess cardiovascular risk is important to identify people at high risk, and to offer them appropriate prevention strategies. Hypertension-induced target organ damage such as left ventricular (LV) hypertrophy and its geometric pattern is a strong independent risk factor for future cardiovascular morbidity and mortality, and for all cause mortality [21, 22]. Another means of risk prediction is to use risk algorithms, such as the European Systematic coronary risk evaluation (SCORE) algorithm [23] or the US Framingham risk score [24]. SCORE is based on cardiovascular risk factors, stratified for different regions and countries in Europe, and estimates a 10-year risk for a fatal cardiovascular event [23]. Evidence suggests that SCORE provides better cardiovascular risk prediction in European populations than the Framingham risk score [25].
Endothelial structure and function in microvascular and macrovascular beds differ, as well as the response to stimulation due to differences in the endothelial surface [26]. However, the interrelation between non-invasive methods to assess macrovascular and microvascular endothelial function in different vascular beds, and specifically skin microvascular reactivity and coronary microvascular function, has not been well studied in hypertension. Simultaneous assessment by different methods may be particularly important as microvascular dysfunction may be a prognostic biomarker while macrovascular endothelial dysfunction may reflect existing atherosclerosis, thus representing different mechanisms and aspects of future cardiovascular risk [27, 28]. Moreover, simultaneous association of macrovascular and microvascular function in different vascular beds to cardiovascular risk has not been well studied in hypertension. Thus, this study aimed to investigate the interrelationship of four methods to evaluate macrovascular and microvascular endothelial function in different vascular regions. Second, we wanted to relate indices of endothelial and microvascular function to cardiovascular risk, as assessed by SCORE and by signs of hypertensive heart disease.
Methods
Study design and subjects
The Doxazosin–ramipril study included women and men 18 years or older with untreated mild-to-moderate primary hypertension (office systolic blood pressure 141–180 mmHg and/or diastolic blood pressure 91–110 mmHg) to evaluate the effects of treatment with ramipril or doxazosin during 12 weeks on vascular function, as described in detail elsewhere [29]. Patients with ischemic heart disease, congestive heart failure, arrhythmias, or diabetes mellitus were excluded. The current study reports on investigations performed with no previous antihypertensive drug treatment for at least 4 weeks (63 were previously never treated for hypertension). Patients arrived for the investigations in the morning after overnight fasting, and were asked to refrain from caffeine containing beverages, fruit juices or vitamin C, and any other medication influencing endothelial function. The studies were performed in the supine position following a 20 min period of rest in a quiet room kept at a constant temperature of 21–24 °C. To avoid pharmacological interference on the vascular function protocols the examinations were performed on two consecutive days.
Body mass index (in kg/m2) was calculated as weight/height2. Routine biochemistry was analysed by standard procedures in fasting blood samples. Estimated glomerular filtration rate was calculated by the CDK-EPI formula [30]. Low density lipoprotein cholesterol was calculated according to Friedewald’s formula. The urine albumin-to-creatinine ratio was calculated by urine albumin (mg/L)/urine creatinine (mmol/L), and microalbuminuria was defined as > 2.5 mg/mmol for men and > 3.5 mg/mmol for women.
Assessment of global cardiovascular risk
The SCORE algorithm was used for global cardiovascular risk prediction [23]. SCORE uses information on age, sex, smoking, systolic blood pressure, and total cholesterol to predict the 10-year risk for cardiovascular mortality in patients 40–65 years of age. We used the electronic version for low-risk countries (where Sweden belongs), which also includes high-density lipoprotein cholesterol for improved risk prediction [31]. There were 11 patients below the age of 40 years, and 15 patients above the age of 65 years, whom we considered being 40 and 65 years of age, respectively, for the purpose of this risk calculation, as generally recommended.
Echocardiography
Echocardiography was performed to detect signs of cardiac hypertension-induced organ damage, as an additional estimate of future cardiovascular risk [21, 22]. Investigations were made in the supine position by standard procedures by use of a Vivid 7 Dimension device and a phased array 3,5 MHz transducer (Doppler frequency 5.0–3.5 MHz) (GE Medical System, Horten, Norway), as we have previously described [32]. Measurements of LV end systolic and end diastolic dimensions, interventricular septum, and posterior wall thickness were made with M-mode recordings. The Penn convention was used for calculation of LV mass [33], which was corrected for body surface area (i.e. LV mass index), and an LV mass index > 95 g/m2 for women and > 115 g/m2 for men was considered LV hypertrophy [34]. To assess LV geometric pattern, relative wall thickness was calculated as (interventricular septum thickness + posterior wall thickness)/LV end diastolic diameter, and considered increased if > 0.42. Left arterial volume indexed for body surface area (ml/m2) was calculated as a mean of the four- and two-chamber view measurements. Evaluation of diastolic function was made by pulsed Doppler registrations. The mitral peak flow velocities of the early (E) and late (A) waves were used for the E/A ratio calculations. Tissue Doppler echocardiography was performed in the apical four-chamber view, and by pulsed wave Doppler the mitral annular systolic (s) and early diastolic (e′) velocities were registered. Calculation of the e′ mean (mean of the e′ septal and e′ lateral registrations) was used to assess LV diastolic filling pressures, E/e′.
Blood pressures measurements and pulse wave analysis
Brachial blood pressure for the vascular function examinations was obtained in the supine position by an oscillometric device (OMRON 705IT, OMRON Healthcare Co, Ltd, Kyoto Japan) on the right arm with an appropriately sized cuff, as a mean of three readings 1 min apart. Pulse pressure was calculated as systolic minus diastolic blood pressure.
PWA was assessed by applanation tonometry (Millar Instruments, Houston, TX, US) and the SpygmoCor device (AtCor Pty Ltd, West Ryde, NSW, Australia), as described previously [29]. From radial applanation tonometry, the central aortic waveform was calculated using a general transfer function by the device software, and central blood pressure was derived. The carotid-femoral pulse wave velocity (PWV) was calculated as the carotid-to-femoral distance divided by the transit time difference of the carotid and femoral pulse wave propagation. Also the carotid-radial PWV was calculated similarly, to obtain the carotid-femoral/carotid-radial PWV ratio. This has been suggested to illustrate the cross-talk between macrocirculation and microcirculation, where a mismatch in aortic–brachial stiffness results in increased forward wave transmission pressure into the microcirculation and end organ damage [35]. Increased central aortic to peripheral brachial stiffness is a prognostic marker in patients with established atheosclerotic disease and high cardiovascular risk [36].
Methods to evaluate endothelial function
FMD was measured by post-ischemic hyperaemia in the non-dominant arm, as previously described [29]. Resting basal diameter of the brachial artery was measured for 1 min by a Vivid 7 Dimension ultrasound device with a 9 MHz linear transducer (GE Medical System, Horten, Norway). Thereafter, an inflated pneumatic tourniquet placed around the forearm to a pressure of 250 mmHg for 5 min induced occlusion of the brachial artery. After cuff deflation, maximum change in diameter was achieved by repeated measurements (30, 60 and 90 s). The relative change from baseline diameter was taken as a measure of FMD. After 10 min of additional rest, endothelium independent vasodilation was induced by 0.4 mg sublingual glyceryl trinitrate (GTN; Nitrolingual, G Pohl-Boskamp GmbH & Co KG, Hohenlockstedt, Germany). Relative changes in artery diameter were calculated from rest to 4 min following GTN administration. The endothelial functional index was calculated as the ratio of the FMD/GTN ratio and was used as a measure of the endothelial vasodilation capacity (37). The inter-assay coefficient of variation for FMD in our laboratory is 15% (n = 20).
Endothelial dependent vasodilation was also evaluated by applanation tonometry and PWA with beta 2-adrenoceptor agonist stimulation (29). PWA was performed before and 15 and 20 min after 0.25 mg sc terbutaline (Bricanyl, AstraZeneca, Mölndal, Sweden) to evaluate the maximum effect of beta 2-adrenoceptor agonist stimulation. Aortic waveforms were generated by the SphygmoCor software from radial artery applanation tonometry. The change in reflection index (RI) was a measure of endothelial nitric oxide availability, and hence endothelium dependant vasodilatation [2].
SEVR, an index of myocardial oxygen supply and demand, is an indirect measure of subendocardial perfusion capacity [17]. Applanation tonometry and PWA (see above) was used to calculate SEVR, expressed as the ratio of diastolic/systolic pressure integral of the derived aortic pulse wave (18). Coronary flow reserve is often used to express coronary microvascular function, and SEVR is closely related to direct invasive measurements of coronary flow reserve in response to intracoronary adenosine in hypertension [18]. Thus, SEVR may provide a useful assessment of the coronary microcirculation [18].
Forearm skin microvascular reactivity (vasodilatation) was assessed by LDF and 60 s transcutaneous iontophoretic administration (Periflux system 5000, PF 5010 LDPM Unit, PF5010 Temp Unit, and 481-1 Single Probe, Perimed, Järfälla, Sweden) of small amounts of Ach (Sigma-Aldrich AB, Stockholm, Sweden) and SNP (Hospira, Inc., Lake Forest, IL, USA) to represent endothelium dependent and independent vasodilatation, respectively, as described previously [29]. Skin microvascular peak flux was recorded continuously up to 16 min after iontophoresis, and is expressed in arbitrary units. To determine maximum skin microvascular hyperaemia, peak flux was evaluated after local heating of forearm skin to 44°C for 6 min [29].
Statistics
Data are presented as mean values ± SD or median values and interquartile ranges, as appropriate. Associations were assessed by linear regression and Pearson’s correlation coefficients (r). Associations to cardiovascular risk by SCORE (always log transformed) was also assessed in a multivariable logistic regression model including PWV and microalbuminuria, which have been suggested to improve cardiovascular risk prediction, as compared to SCORE alone [38, 39]. All statistical tests were 2-sided and carried out to a significance level (P) of < 0.05. The statistical program used was JMP version 13.0 (SAS Institute Inc., Cary, NC, USA).
The size of the current study population originates from the co-primary outcomes in the Doxazosin–ramipril study, which were changes in endothelial function assessed by FMD, and in haemostatic function measured by the generation of thrombin–antithrombin complex, as presented elsewhere [29, 40].
Results
General
Baseline characteristics of the 71 participants are presented in Table 1. About one-third were women. Most women were postmenopausal and no one used systemic hormone replacement therapy. There were few smokers, and lipid levels and glucose metabolism were within normal limits. Most patients had normal renal function (chronic kidney disease stage 1, with an estimated glomerular filtration rate ≥ 90 ml/min/1.72 m2), while 29 were in stage 2 (60–89 ml/min/1.72 m2) and 2 were in stage 3 (30–59 ml/min/1.72 m2).
Values for indices of endothelial function and LV structure and function are presented in Table 2. There were 19 patients (5 women and 14 men) out of the 61 with available echocardiographic data with LV hypertrophy. The distribution of LV geometric pattern is shown in Table 2. No patient had reduced (< 40%) LV ejection fraction.
Relations between methods to evaluate endothelial function
Measurements of endothelial function in various vascular beds and their interrelations are presented in Table 3. The relations between indices of endothelial function in the forearm, the coronary microcirculation assessed by SEVR, and the skin microcirculation were, at most, weak. However, there was a trend for SEVR to relate to endothelial function index, and the RI change tended to relate to GTN induced vasodilatation and to skin microcirculatory responses to Ach peak flux.
Endothelial function in different vascular beds in relation to cardiovascular risk
Endothelium dependent vasodilation (FMD) was inversely related to cardiovascular risk, as assessed by SCORE, while endothelium independent vasodilation (GTN) did not relate to SCORE (Fig. 1a, b). Accordingly, endothelial functional index was inversely related to SCORE (Fig. 1c). There was a trend for a relation between the RI change and SCORE (Fig. 1d).

The relations between a flow mediated vasodilatation (FMD), b glyceryl trinitrate (GTN) mediated vasodilation, c endothelial functional index (EFI), and d relative change in reflection index (RI) before and after beta 2-adrenoceptor agonist stimulation, and a 10-year-risk for a fatal cardiovascular event, as assessed by the systematic coronary risk evaluation (SCORE)
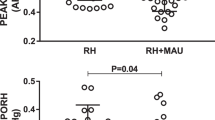
Coronary microcirculatory function (SEVR) did not relate to SCORE (Fig. 2a). Concerning the skin microcirculation, relative peak flux changes induced by Ach did not relate to SCORE (Fig. 2b). However, relative peak flux changes induced by SNP, and peak flux change after heat induced maximal hyperaemia, all showed inverse relations to SCORE (Fig. 2c, d). Peak LDF (in absolute values) induced by Ach or by SNP were not related to SCORE, and peak flux ratio Ach/SNP did not relate to SCORE (data not shown).

The relations between a subendocardial viability ratio (SEVR), b relative change in endothelial dependent peak flux (Δ% Peak flux Ach), c relative change in endothelial independent peak flux (Δ% Peak flux SNP), and d relative change peak flux after maximal hyperaemia (Δ% Peak flux heat), and a 10-year risk for a fatal cardiovascular event, as assessed by the systematic coronary risk evaluation (SCORE)
Endothelial function in relation to signs of hypertensive heart disease
FMD did not relate to LV mass index (data not shown). Accordingly, there were no differences in responses to FMD or GTN when comparing patients without or with LV hypertrophy (6.2 ± 4.5 and 5.4 ± 3.2%, P = 0.41 for FMD %, and 15.2 ± 7.7 and 13.5 ± 5.8%, P = 0.35, for GTN %, respectively; mean values ± SD). Furthermore, FMD did not relate to relative wall thickness or to indices of diastolic function (i.e. E/A, E/e′, or left atrial volume; data not shown). However, endothelial functional index tended to be inversely related to left atrial volume (r = 0.23, P = 0.087) but not to relative wall thickness, E/A, or E/e′ (data not shown). There was a trend for improvement of SEVR to the reduction of E/é ratio (r = 0.21, P = 0.101). However, there were no relations between indices of skin microvascular function (i.e. Ach and SNP peak flux, relative peak flux changes by Ach and SNP, or relative peak flux change after maximal hyperaemia) and LV mass index or with indices of diastolic function (data not shown).
Endothelial function in relation to indices of arterial stiffness
FMD was inversely related to carotid-femoral PWV (Fig. 3a), while GTN induced vasodilatation did not relate to PWV (r = 0.11, P = 0.42). However, endothelial functional index (r = 0.05, P = 0.74) and the RI change (r = 0.10, P = 0.47) failed to relate to PWV. SEVR was inversely related to PWV (Fig. 3b). FMD tended to relate inversely to central aortic pulse pressure (Fig. 3c) but did not relate to brachial pulse pressure (r = 0.11, P = 0.37). However, endothelial functional index (r = 0.14, P = 0.27) and the RI change (r = 0.12, P = 0.33) did not relate to aortic pulse pressure. SEVR was related to aortic pulse pressure (Fig. 3d) and to brachial pulse pressure (r = 0.38, P = 0.002).

The relations between a flow-mediated vasodilatation (FMD), b subendocardial viability ratio (SEVR), and carotid-femoral pulse wave velocity, and c flow mediated vasodilatation (FMD), and d subendocardial viability ratio (SEVR), and aortic pulse pressure
In the skin microcirculation, Ach and SNP peak flux did not significantly relate to PWV (r = 0.22, P = 0.101, and r = 0.06, P = 0.66, respectively). However, SNP peak flux related to aortic pulse pressure (r = 0.26, P = 0.035), and tended to relate to brachial pulse pressure (r = 0.23, P = 0.061). Ach peak flux tended to relate to aortic pulse pressure (r = 0.21, P = 0.094) but not to brachial pulse pressure (r = 0.18, P = 0.13). The relative peak flux changes by Ach and SNP, heat-induced peak flux, and the peak flux change after heat-induced maximal hyperaemia were not related to indices of arterial stiffness (i.e. PWV, aortic pulse pressure, or brachial pulse pressure) (data not shown).
Indices of skin microcirculation (Ach peak flux and maximum peak flux after local heating) were related to the carotid-femoral PWV/carotid-radial PWV ratio (Fig. 4a, b), while SNP peak flux did not relate (r = 0.06, P > 0.5). There were no relations between indices of skin microcirculation and the aortic pulse pressure/brachial pulse pressure ratio (data not shown).

The relations between a acetylcholine induced peak flux and b peak flux after heat-induced maximum hyperaemia (heat peak flux), and the carotid-femoral to carotid-radial pulse wave velocity ratio (car-fem PWV/car-rad PWV)
PWV (P = 0.014), but not microalbuminuria (P > 0.5), was independently related to SCORE. In a multivariable model, PWW and microalbuminuria were added to SCORE in an attempt to provide a better prediction of future cardiovascular risk. This improved the relations between indices of endothelial function and future cardiovascular risk for FMD (R = 0.44, P = 0.021) and for SEVR (R = 0.44, P = 0.022), but not for the RI change or for indices for skin microvascular function (data not shown). Adding LV mass index did not improve the multivariable model (data not shown).
Discussion
Main findings
This is the first study comparing simultaneous measurements of macrovascular endothelial function by brachial artery vasodilatation induced by post-ischemic flow mediated hyperaemia (by FMD) and pulse wave reflection (by PWA), skin microvascular function (by LDF and iontophoresis), and coronary microvascular function (using SEVR) in hypertensive patients. Of note, SEVR has not previously been well evaluated in relation to peripheral endothelial vascular function. We show that endothelial dysfunction in macrocirculation and microcirculation is both related to cardiovascular mortality risk (by SCORE). However, the applied methods for investigating macrovascular and microvascular function were poorly interrelated, suggesting that endothelial function and microvascular function assessed in different vascular beds represent different aspects of future cardiovascular risk.
Comparison of endothelial function in different vascular beds
The simultaneous measurements of indices of endothelial function representing conduit arteries (FMD), resistance arteries (PWA), skin microvascular reactivity (LDF and iontophoresis), and coronary microcirculation (SEVR), all previously reported to be associated with cardiovascular risk [6, 9, 15, 18], showed that these markers of macrovascular and microvascular function were poorly interrelated. We found no relation between FMD and skin microvascular function, also when the potential confounding effects of non-specific vasodilation were taken into account. This is in agreement with observations in healthy subjects, and in patients with diabetes or chronic inflammatory disease [41,42,43]. A relation between conduit artery endothelial function and skin microvascular reactivity has, however, also been reported [44, 45].
The change in pulse wave reflection assessed by the digital volume pulse has been reported to relate to FMD [46]. However, we found no association between change in RI (here assessed by PWA) and FMD, in support of other findings [2]. Thus, our results in hypertensive patients suggest that endothelial function in conduit arteries, as compared to smaller resistance arteries, might not be equivalent. Furthermore, we observed no consistent relations between RI and skin microvascular function, in consort with findings by others [47]. These mixed findings may, at least in part, be related to differences in methodology and study subjects characteristics. More important, however, the lack of relations between macrovascular and microvascular function could be explained by the fact that endothelial dysfunction in conduit vessels and impaired skin microvascular reactivity might develop independently, due to differences in their pathogenesis [48, 49]. Thus, nitric oxide is the major mediator of endothelium dependent vasodilation in conduit arteries, whereas endothelium derived hyperpolarization factor, prostanoids, and other factors are predominant mediators of this in the skin microcirculation [50].
FMD relates to invasive evaluation of coronary artery endothelial function [3] and to coronary flow reserve [4]. However, the present study appears to be the first evaluation of FMD in relation to SEVR. Circumstantial support to our findings that SEVR and FMD did not relate is the observation that SEVR did not relate to dimethylarginines (circulating markers of endothelial dysfunction) [51]. Furthermore, FMD and coronary microvascular reactivity did not relate in healthy subjects or in patients with atherosclerotic coronary artery disease or microvascular angina pectoris [52]. In addition, SEVR was not related to skin microvascular reactivity in the current study. This is in agreement with results suggesting that skin microvascular reactivity and coronary microvascular reactivity are poorly interrelated [53]. Thus, similar to skin microvascular reactivity, coronary microvascular function assessed by SEVR does not seem to relate to macrovascular endothelial function. Accordingly, microvascular dysfunction may be a prognostic biomarker while macrovascular endothelial dysfunction may reflect existing atherosclerosis, representing different mechanisms and aspects of future cardiovascular risk [27, 28].
Vascular function in relation to cardiovascular mortality risk
FMD was inversely related to SCORE. Our findings were consistent when adjusted for the potential confounding of endothelium independent non-specific vasodilatation assessed by GTN These results support previous observations that reduced endothelium dependent vasodilatation by FMD is inversely related to cardiovascular risk, as reviewed elsewhere [54]. Our findings also confirm an association between FMD and PWV [55]. Furthermore, we confirm that including PWV and microalbuminuria with SCORE in a multivariable linear regression model can improve the prediction of cardiovascular mortality risk [38, 39]. Thus, our results in hypertensive patients extend previous findings [54] to suggest that conduit artery endothelial function is associated to future cardiovascular mortality.
This study also measured endothelial function by PWA and applanation tonometry, where the RI change after beta 2-adrenoceptor agonist stimulation was taken as a measure of global endothelial function, mainly reflecting resistance arteries [2]. The RI change tended to relate to SCORE, in support of our findings on brachial artery endothelial function. Our results are in agreement with those showing that the RI change was related to cardiovascular risk (by Framingham Risk Score), although those authors did not establish a relation to future cardiovascular events [2, 9]. Whereas FMD may be considered to reflect endothelial function in conduit arteries, the RI change is likely to reflect resistance arteries. Conduit arteries may better reflect atherosclerotic vascular changes with a stronger association to cardiovascular risk than resistance arteries reflecting arteriosclerotic vascular disease more closely, and thus being more closely related to blood pressure per se. This could, at least in part, explain the stronger relation observed for FMD than for the RI change to cardiovascular risk in our study.
Coronary microvascular function estimated by SEVR did not relate to SCORE. SEVR is a validated measure of cardiovascular health in subjects with rheumatoid arthritis, a population with a high prevalence of hypertension [56]. Accordingly, SEVR predicts cardiovascular mortality in patients at high risk [19, 20, 57]. However, compared to invasive methods, SEVR is an indirect measure of coronary microcirculation, and might be influenced by other confounding factors. This could have contributed to our findings. In contrast, we showed that total skin microvascular dilatory capacity (assessed as peak flux change to SNP and peak flux change after heat induced maximal hyperaemia) was related to SCORE, in agreement with other results [13, 15]. This suggests that global microvascular vasodilator capacity may be more important than Ach induced skin microvascular reactivity to predict cardiovascular risk. Accordingly, impaired heat-induced maximal hyperaemia in the skin microcirculation has been suggested to discriminate patients with coronary artery disease better than the response to Ach by iontophoresis [58]. These findings indicate that total skin microvascular reactivity is a marker of cardiovascular risk in hypertension.
Endothelial function in relation to LV mass and function
Impaired macrovascular endothelial function (assessed by FMD, endothelial function index, or RI change) did not relate to LV mass index or indices of LV diastolic dysfunction. Our results are in agreement with some studies [6, 59]; but weak relations between FMD and LV mass index have also been reported [15]. SEVR and LV mass index were not related, and furthermore skin microvascular reactivity was not related to LV mass index or indices of LV diastolic function. Thus, in contrast to our observed associations between vascular reactivity and SCORE, endothelial function measurements did not relate to LV hypertrophy. This suggests that different risk factors are associated to endothelial dysfunction and to hypertensive heart disease. While LV wall tension (i.e. blood pressure) and neurohormonal activation of the renin–angiotensin–aldosterone system and the sympathetic nervous system may be more important for the development of hypertensive heart disease, glucose and lipid metabolism, sex, and smoking may play a greater role for endothelial dysfunction.
Vascular function in relation to indices of arterial stiffness
Our results show that FMD related to PWV are in agreement with findings that FMD is related to indices of large arterial stiffness [55, 61]. In the skin microcirculation, SNP peak flux related (and Ach peak flux tended to relate) to aortic pulse pressure. Neither Ach peak flux nor SNP associated to PWV but Ach peak flux and maximum peak flux after local heating related to the carotid-femoral PWV/carotid-radial PWV ratio. A mismatch in aortic–brachial stiffness with higher carotid-femoral PWV than carotid-radial PWV has been shown to predict cardiovascular mortality in patients at very high risk (end stage kidney disease) [36]. Our results extend these findings to patients with uncomplicated hypertension (i.e. at a lower risk) to suggest that the carotid-femoral PWV/carotid-radial PWV ratio might be a sensitive measure to detect aortic–brachial stiffness mismatch. An increased PWV mismatch results in an increased forward wave transmission pressure into the microcirculation causing compensating mechanisms like rarefaction and vasodilatation in skin microcirculation where total skin microvascular dilatory capacity is of importance [35].
Study strengths and limitations
A strength of this study is the evaluation of macrovascular and microvascular function in different vascular beds and by several established non-invasive techniques simultaneously. We compared skin microvascular reactivity and SEVR to large artery endothelial function in hypertensive subjects, which had not been well studied. In addition, SEVR had not been validated to skin microvascular reactivity in hypertensive patients. Second, we studied hypertensive patients with no concomitant confounding cardiovascular disease, ongoing medication, or hormone replacement therapy. However, the study must be interpreted in the context of its limitations. The study population was small and we did not include invasive assessment of endothelial function, which might be considered more reliable. Second, this cross-sectional study evaluated vascular function in relation to predicted future cardiovascular risk and did not prospectively evaluate cardiovascular events. Finally, the results from this small study do not allow us to elucidate in more detail why these methods to assess vascular function were poorly interrelated. However, endothelial function and microvascular function assessed in different vascular beds might develop independently, at least in part due to several differences in their pathogenesis, and thus represent different aspects of future cardiovascular risk [27, 28].
In conclusion, indices of macrovascular and microvascular endothelial function representing different vascular beds were poorly interrelated and are not interchangeable. However, they were all were related to cardiovascular mortality risk, as estimated by SCORE (but not to signs of hypertension-induced cardiac organ damage). These findings suggest that indices of macrovascular and microvascular endothelial function may depend on different mechanisms and thus represent different aspects of future cardiovascular risk. Different techniques to evaluate endothelial function are poorly interrelated. Thus, a global approach to assess vascular endothelial function is required in the risk assessment of hypertensive patients.
References
Perticone F, Ceravolo R, Pujia A, Ventura G, Iacopino S, Scozzafava A, Ferraro A, Chello M, Mastroroberto P, Verdecchia P, Schillaci G (2001) Prognostic significance of endothelial dysfunction in hypertensive patients. Circulation 104:191–196
Lind L, Fors N, Hall J, Marttala K, Stenborg A (2005) A comparison of three different methods to evaluate endothelium-dependent vasodilation in the elderly: the Prospective Investigation of the Vasculature in Uppsala Seniors (PIVUS) study. Arterioscler Thromb Vasc Biol 25:2368–2375
Anderson TJ, Uehata A, Gerhard MD, Meredith IT, Knab S, Delagrange D, Lieberman EH, Ganz P, Creager MA, Yeung AC, Selwyn AP (1995) Close relation of endothelial function in the human coronary and peripheral circulations. J Am Coll Cardiol 26:1235–1241
Campuzano R, Moya JL, García-Lledó A, Tomas JP, Ruiz S, Megías A, Balaguer J, Asín E (2006) Endothelial dysfunction, intima-media thickness and coronary reserve in relation to risk factors and Framingham score in patients without clinical atherosclerosis. J Hypertens 24:1581–1588
Yeboah J, Folsom AR, Burke GL, Johnson C, Polak JF, Post W, Lima JA, Crouse JR, Herrington DM (2009) Predictive value of brachial flow-mediated dilation for incident cardiovascular events in a population-based study: the multi-ethnic study of atherosclerosis. Circulation 120:502–509
Muiesan ML, Salvetti M, Paini A, Monteduro C, Galbassini G, Poisa P, Porteri E, Agabiti-Rosei C, Paderno V, Belotti E, Rizzoni D, Castellano M, Agabiti-Rosei E (2008) Prognostic role of flow-mediated dilatation of the brachial artery in hypertensive patients. J Hypertens 26:1612–1618
Gokce N, Keaney JF Jr, Hunter LM, Watkins MT, Nedeljkovic ZS, Menzoian JO, Vita JA (2003) Predictive value of noninvasively determined endothelial dysfunction for long-term cardiovascular events in patients with peripheral vascular disease. J Am Coll Cardiol 41:1769–1775
Frick M, Suessenbacher A, Alber HF, Dichtl W, Ulmer H, Pachinger O, Weidinger F (2005) Prognostic value of brachial artery endothelial function and wall thickness. J Am Coll Cardiol 46:1006–1010
Lind L, Berglund L, Larsson A, Sundström J (2011) Endothelial function in resistance and conduit arteries and 5-year risk of cardiovascular disease. Circulation 123:1545–1551
Wilkinson IB, Hall IR, MacCallum H, Mackenzie IS, McEniery CM, van der Arend BJ, Shu YE, MacKay LS, Webb DJ, Cockcroft JR (2002) Pulse-wave analysis: clinical evaluation of a noninvasive, widely applicable method for assessing endothelial function. Arterioscler Thromb Vasc Biol 22:147–152
Chowienczyk PJ, Kelly RP, MacCallum H, Millasseau SC, Andersson TL, Gosling RG, Ritter JM, Anggård EE (1999) Photoplethysmographic assessment of pulse wave reflection: blunted response to endothelium-dependent beta2-adrenergic vasodilation in type II diabetes mellitus. J Am Coll Cardiol 34:2007–2014
Farkas K, Kolossvary E, Jarai Z, Nemcsik J, Farsang C (2004) Non-invasive assessment of microvascular endothelial function by laser Doppler flowmetry in patients with essential hypertension. Atherosclerosis 173:97–102
Östlund Papadogeorgos N, Jörneskog G, Bengtsson M, Kahan T, Kalani M (2016) Severely impaired microvascular reactivity in diabetic patients with an acute coronary syndrome. Cardiovasc Diabetol 15:66. https://doi.org/10.1186/s12933-016-0385-6
Serne EH, Gans RO, ter Maaten JC, Tangelder GJ, Donker AJ, Stehouwer CD (2001) Impaired skin capillary recruitment in essential hypertension is caused by both functional and structural capillary rarefaction. Hypertension 38:238–242
Ijzerman RG, de Jongh RT, Beijk MA, van Weissenbruch MM, Delemarre-van de Waal HA, Serné EH, Stehouwer CD (2003) Individuals at increased coronary heart disease risk are characterized by an impaired microvascular function in skin. Eur J Clin Invest 33:536–542
Jörneskog G, Kalani M, Kuhl J, Båvenholm P, Katz A, Allerstrand G, Alvarsson M, Efendic S, Östenson CG, Pernow J, Wahren J, Brismar K (2005) Early microvascular dysfunction in healthy normal-weight males with heredity for type 2 diabetes. Diabetes Care 28:1495–1497
Hoffman JI, Buckberg GD (1978) The myocardial supply:demand ratio–a critical review. Am J Cardiol 41:327–332
Tsiachris D, Tsioufis C, Syrseloudis D, Roussos D, Tatsis I, Dimitriadis K, Toutouzas K, Tsiamis E, Stefanadis C (2012) Subendocardial viability ratio as an index of impaired coronary flow reserve in hypertensives without significant coronary artery stenoses. J Hum Hypertens 26:64–70
Theilade S, Hansen TW, Rossing P (2014) Central hemodynamics are associated with cardiovascular disease and albuminuria in type 1 diabetes. Am J Hypertens 27:1152–1159
Di Micco L, Salvi P, Bellasi A, Sirico ML, Di Iorio B (2013) Subendocardial viability ratio predicts cardiovascular mortality in chronic kidney disease patients. Blood Purif 36:26–28
Krumholz HM, Larson M, Levy D (1995) Prognosis of left ventricular geometric patterns in the Framingham Heart Study. J Am Coll Cardiol 25:879–884
de Simone G, Izzo R, Aurigemma GP, De Marco M, Rozza F, Trimarco V, Stabile E, De Luca N, Trimarco B (2015) Cardiovascular risk in relation to a new classification of hypertensive left ventricular geometric abnormalities. J Hypertens 33:745–754
Conroy RM, Pyörälä K, Fitzgerald AP, Sans S, Menotti A, De Backer G, De Bacquer D, Ducimetière P, Jousilahti P, Keil U, Njølstad I, Oganov RG, Thomsen T, Tunstall-Pedoe H, Tverdal A, Wedel H, Whincup P, Wilhelmsen L, Graham IM, SCORE project group (2003) Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. Eur Heart J 24:987–1003
D'Agostino RB Sr, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, Kannel WB (2008) General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation 117:743–753
Brindle P, Emberson J, Lampe F, Walker M, Whincup P, Fahey T, Ebrahim SP (2003) Predictive accuracy of the Framingham coronary risk score in British men: prospective cohort study. BMJ 327:1267
Ghitescu L, Robert M (2002) Diversity in unity: the biochemical composition of the endothelial cell surface varies between the vascular beds. Microsc Res Tech 57:381–389
Flammer AJ, Anderson T, Celermajer DS, Creager MA, Deanfield J, Ganz P, Hamburg NM, Lüscher TF, Shechter M, Taddei S, Vita JA, Lerman A (2012) The assessment of endothelial function: from research into clinical practice. Circulation 126:753–767
Hellmann M, Roustit M, Cracowski JL (2015) Pharmacol Rep 67:803–810
Jekell A, Kalani M, Kahan T (2017) The effects of alpha 1-adrenoceptor blockade and angiotensin converting enzyme inhibition on central and brachial blood pressure and vascular reactivity: the doxazosin-ramipril study. Heart Vessels 32:674–684
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, Coresh J, CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) (2009) A new equation to estimate glomerular filtration rate. Ann Intern Med 150:604–612
HeartScore. Available from https://heartscore.escardio.org/2012/calc.aspx?model=europelow. Accessed 1 July 2017.
Iacobaeus C, Kahan T, Jörneskog G, Bremme K, Thorsell M, Andolf E (2016) Fetal growth is associated with first-trimester maternal vascular function. Ultrasound Obstet Gynecol 48:483–490
Devereux RB, Reichek N (1977) Echocardiographic determination of left ventricular mass in man. Anatomic validation of the method. Circulation 55:613–618
Marwick TH, Gillebert TC, Aurigemma G, Chirinos J, Derumeaux G, Galderisi M, Gottdiener J, Haluska B, Ofili E, Segers P, Senior R, Tapp RJ, Zamorano JL (2015) Recommendations on the use of echocardiography in adult hypertension: a report from the European Association of Cardiovascular Imaging (EACVI) and the American Society of Echocardiography (ASE). J Am Soc Echocardiogr 28:727–754
Safar ME, Struijker-Boudier HA (2010) Cross-talk between macro- and microcirculation. Acta Physiol (Oxf) 198:417–430
Fortier C, Mac-Way F, Desmeules S, Marquis K, De Serres SA, Lebel M, Boutouyrie P, Agharazii M (2015) Aortic-brachial stiffness mismatch and mortality in dialysis population. Hypertension 65:378–384
Millgård J, Hägg A, Sarabi M, Lind L (2002) Endothelium-dependent vasodilation in normotensive subjects with a familial history of essential hypertension and in young subjects with borderline hypertension. Blood Press 11:279–284
Sehestedt T, Jeppesen J, Hansen TW, Wachtell K, Ibsen H, Torp-Pedersen C, Hildebrandt P, Olsen MH (2010) Risk prediction is improved by adding markers of subclinical organ damage to SCORE. Eur Heart J 31:883–891
Sehestedt T, Jeppesen J, Hansen TW, Rasmussen S, Wachtell K, Ibsen H, Torp-Pedersen C, Olsen MH (2012) Thresholds for pulse wave velocity, urine albumin creatinine ratio and left ventricular mass index using SCORE, Framingham and ESH/ESC risk charts. J Hypertens 30:1928–1936
Ekholm M, Jekell A, Wallén NH, Gigante B, Kahan T (2018) The effects of angiotensin converting enzyme inhibition and alpha 1-adrenoceptor blockade on inflammation and haemostasis in human hypertension. J Cardiovasc Pharmacol. 71:240–247
Gori T, Di Stolfo G, Sicuro S, Dragoni S, Lisi M, Parker JD, Forconi S (2006) Correlation analysis between different parameters of conduit artery and microvascular vasodilation. Clin Hemorheol Microcirc. 35:509–515
Meyer MF, Lieps D, Schatz H, Pfohl M (2008) Impaired flow-mediated vasodilation in type 2 diabetes: lack of relation to microvascular dysfunction. Microvasc Res. 76:61–65
Sandoo A, Carroll D, Metsios GS, Kitas GD, Veldhuijzen van Zanten JJ (2011) The association between microvascular and macrovascular endothelial function in patients with rheumatoid arthritis: a cross-sectional study. Arthritis Res Ther. 13:R99
Debbabi H, Bonnin P, Ducluzeau PH, Lefthériotis G, Levy BI (2010) Noninvasive assessment of endothelial function in the skin microcirculation. Am J Hypertens. 23:541–546
Hansell J, Henareh L, Agewall S, Norman M (2004) Non-invasive assessment of endothelial function—relation between vasodilatory responses in skin microcirculation and brachial artery. Clin Physiol Funct Imaging. 24:317–322
Rambaran C, Jiang B, Ritter JM, Shah A, Kalra L, Chowienczyk PJ (2008) Assessment of endothelial function: comparison of the pulse wave response to beta 2-adrenoceptor stimulation with flow mediated dilatation. Br J Clin Pharmacol. 65:238–243
Ibrahim NNIN, Rasool AHG (2017) Assessment of macrovascular endothelial function using pulse wave analysis and its association with microvascular reactivity in healthy subjects. Skin Res Technol. 23:321–325
Hill CE, Phillips JK, Sandow SL (2001) Heterogeneous control of blood flow amongst different vascular beds. Med Res Rev. 21:1–60
Konukoglu D, Uzun H (2017) Endothelial dysfunction and hypertension. Adv Exp Med Biol. 956:511–540
Holowatz LA, Thompson CS, Minson CT, Kenney WL (2005) Mechanisms of acetylcholine-mediated vasodilatation in young and aged human skin. J Physiol 563:965–973
Dimitroulas T, Sandoo A, Hodson J, Smith JP, Kitas GD (2016) In vivo microvascular and macrovascular endothelial function is not associated with circulating dimethylarginines in patients with rheumatoid arthritis: a prospective analysis of the DRACCO cohort. Scand J Clin Lab Invest. 76:331–337
Bøttcher M, Madsen MM, Refsgaard J, Buus NH, Dørup I, Nielsen TT, Sørensen K (2001) Peripheral flow response to transient arterial forearm occlusion does not reflect myocardial perfusion reserve. Circulation 103:1109–1114
Sütsch G, Hess OM, Franzeck UK, Dörffler T, Bollinger A, Krayenbühl HP (1992) Cutaneous and coronary flow reserve in patients with microvascular angina. J Am Coll Cardiol. 20:78–84
Ras RT, Streppel MT, Draijer R, Zock PL (2013) Flow-mediated dilation and cardiovascular risk prediction: a systematic review with meta-analysis. Int J Cardiol 168:344–351
McEniery CM, Wallace S, Mackenzie IS, McDonnell B, DE Yasmin Newby, Cockcroft JR, Wilkinson IB (2006) Endothelial function is associated with pulse pressure, pulse wave velocity, and augmentation index in healthy humans. Hypertension 48:602–608
Sandoo A, Protogerou AD, Hodson J, Smith JP, Zampeli E, Sfikakis PP, Kitas GD (2012) The role of inflammation, the autonomic nervous system and classical cardiovascular disease risk factors on subendocardial viability ratio in patients with RA: a cross-sectional and longitudinal study. Arthritis Res Ther 14:R258
Laugesen E, Høyem P, Fleischer J, Kumarathas I, Knudsen ST, Hansen KW, Christiansen JS, Hansen TK, Poulsen PL (2016) Reduced subendocardial viability ratio is associated with unfavorable cardiovascular risk profile in women with short duration of type 2 diabetes. Am J Hypertens 29:1165–1172
Agarwal SC, Allen J, Murray A, Purcell IF (2012) Laser Doppler assessment of dermal circulatory changes in people with coronary artery disease. Microvasc Res 84:55–59
Olsen MH, Wachtell K, Hermann KL, Bella JN, Dige-Petersen H, Rokkedal J, Ibsen H (2002) Left ventricular hypertrophy is associated with reduced vasodilatory capacity in the brachial artery in patients with longstanding hypertension. A LIFE substudy. Blood Press 11:285–292
Lind L (2008) Left ventricular mass is related to endothelium-dependent vasodilation in the forearm, but not in the brachial artery, in elderly subjects: the Prospective Investigation of the Vasculature in Uppsala Seniors study. J Hum Hypertens 22:767–773
Nigam A, Mitchell GF, Lambert J, Tardif JC (2003) Relation between conduit vessel stiffness (assessed by tonometry) and endothelial function (assessed by flow-mediated dilatation) in patients with and without coronary heart disease. Am J Cardiol 92:395–399
Acknowledgments
We thank Ms. E. Andersson, J. Rasck and E. Wallén Nielsen for expert technical assistance.
Funding
Funding was provided by Karolinska Institutet (Grant No. 2014FoBi41054) and Hjärt-Lungfonden (Grant No. 20130467).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
The Regional Ethics Committee in Stockholm approved of the study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Oral and written informed consent was obtained from all individual participants included in the study.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Jekell, A., Kalani, M. & Kahan, T. The interrelation of endothelial function and microvascular reactivity in different vascular beds, and risk assessment in hypertension: results from the Doxazosin–ramipril study. Heart Vessels 34, 484–495 (2019). https://doi.org/10.1007/s00380-018-1265-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00380-018-1265-7