
Abstract
Background
Cardiovascular morbidity and mortality are closely linked to chronic kidney disease (CKD). Sex-specific long-term outcome data of patients with coronary artery disease (CAD) and CKD are scarce.
Methods
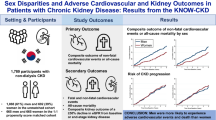
In the prospective observational multicenter Coronary Artery Disease and REnal Failure (CAD-REF) Registry, 773 (23.1%) women and 2,579 (76.9%) men with angiographically documented CAD and different stages of CKD were consecutively enrolled and followed for up to 8 years. Long-term outcome was evaluated using survival analysis and multivariable Cox-regression models.
Results
At enrollment, women were significantly older than men, and suffered from more comorbidities like CKD, hypertension, diabetes mellitus, and multivessel coronary disease. Regarding long-term mortality, no sex-specific differences were observed (Kaplan–Meier survival estimates: 69% in women vs. 69% in men, plog-rank = 0.7). Survival rates decreased from 89% for patients without CKD at enrollment to 72% for patients with CKD stages 1–2 at enrollment and 49% for patients with CKD stages 3–5 at enrollment (plog-rank < 0.001). Cox-regression analysis revealed that sex or multivessel coronary disease were no independent predictors of long-term mortality, while age, CKD stages 3–5, albumin/creatinine ratio, diabetes, valvular heart disease, peripheral artery disease, and left-ventricular ejection fraction were predictors of long-term mortality.
Conclusions
Sex differences in CAD patients mainly exist in the cardiovascular risk profile and the extent of CAD. Long-term mortality was not depended on sex or multivessel disease. More attention should be given to treatment of comorbidities such as CKD and peripheral artery disease being independent predictors of death.
Clinical Trail Registration ClinicalTrials.gov Identifier: NCT00679419
Graphic abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Coronary artery disease (CAD) and chronic kidney disease (CKD) are frequently associated. The prevalence of CAD as well as of CKD differs in men and women. Women have a higher prevalence of CKD than men [1], whereas the prevalence of CAD is higher in men than in women [2]. Both morbidities share some risk factors, e.g., higher age, male sex, smoking, hypertension, and diabetes mellitus [2, 3], and patients with CKD are more likely to die from cardiovascular disease than to progress to end-stage renal disease [4]. The long-term outcome of women and men with CAD is still a matter of debate: some studies and registries reported higher mortality for women with CAD, others reported no difference [5,6,7,8]. Data on patients suffering from both, CAD and CKD, are rarely presented, because patients with CKD are often excluded from studies. Therefore, the influence of renal function on long-term outcome of women and men with CAD is not well studied and needs clarification.
In 2008, the prospective, observational multicenter German Coronary Artery Disease and REnal Failure (CAD-REF) Registry was established to evaluate the impact of CKD on the manifestation, progression, and general outcome of patients with CAD [9]. Patients with angiographically documented CAD ≥ 50% stenosis in at least one coronary artery were registered, classified by their estimated glomerular filtration rate (eGFR) and followed for up to 96 months. The main objective of this report was to analyze sex-specific differences in baseline characteristics, medical treatment, and long-term mortality of CAD patients with varying degrees of renal disease.
Materials and methods
The German CAD-REF Registry (ClinicalTrials.gov identifier number NCT00679419, http://clinicaltrials.gov), a multicenter, prospective, observational registry, included patients with an angiographically documented ≥ 50% stenosis in at least one coronary artery. The patients were classified according to their eGFR and proteinuria into either a control group with normal renal function or one of two CKD categories (CKD stages 1–2 or CKD stages 3–5, determination see below). A detailed description of the trial design [9] and baseline characteristics [10] has been published elsewhere. In brief, 3,352 patients of European/white descent aged ≥ 18 years were enrolled at 32 cardiological recruiting centers distributed all over Germany. All patients gave written informed consent prior to their inclusion. Urine, serum, and EDTA-blood samples of each patient were collected prior to coronary angiography. Patients with organ transplantations other than kidney transplantation, with immunosuppressive therapy apart from immunosuppressive therapy after kidney transplantation, with polycystic renal disease, with known malignant tumors as well as pregnant or breastfeeding patients were excluded from the registry.
Data collection
Before coronary angiography, demographic characteristics, anthropometric data, cardiovascular risk factors, medical history, standard laboratory parameters of serum and urine samples, and medication were recorded. Data on the degree and localization of stenoses were collected from coronary angiograms according to the Cardiology Audit and Registration Data Standards (CARDS) [11]. At hospital discharge, data on medication were recorded. Follow-up data were collected by questionnaire and telephone calls.
Data collection was performed by the IKKF Institute GmbH, Munich, Germany, and the University Hospital Muenster, Muenster, Germany. Primary route of data entry was done through a web-based interface.
Renal function and proteinuria
Serum creatinine was used to estimate the GFR according to the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula [12, 13].
Proteinuria was determined using a dipstick test. Proteinuria could not be determined in ten patients because of no residual urine.
For analysis, patients were classified into three categories of CKD: patients without CKD had eGFR ≥ 90 ml/min/1.73 m2 and no proteinuria, patients with CKD stages 1–2 had eGFR ≥ 90 ml/min/1.73 m2 and proteinuria or eGFR 60–89 ml/min/1.73 m2, and patients with CKD stages 3–5 had eGFR < 60 ml/min/1.73 m2 or were on dialysis.
Definition of cardiovascular risk factors
The cardiovascular risk factors were documented based on questionnaires and patients’ records. Definitions of the cardiovascular risk factors are found in the Supplemental Material.
Data and statistical analyses
All statistical analyses were done using SPSS version 25 and 27 (IBM Corporation, Armonk, NY, USA). Right-skewed continuous variables (creatinine, albumin/creatinine ratio, and protein/creatinine ratio) were log10-transformed prior to further analyses. Baseline characteristics of patients were described by presenting means and 95% confidence intervals of continuous variables, after back-transformation if applicable, as well as absolute and percentage frequency distributions of categorical variables. For continuous dependent variables, comparisons of sex and CKD stages within sex were done based on F tests and associated p values, using the procedure UNIANOVA. For dichotomous dependent variables, comparisons were made based on logistic regression analyses [14], using procedure LOGISTIC REGRESSION. For ordinal dependent variables, procedure GENLIN was used with multinomial distribution and cumlogit link. For nominal variables, procedure NOMREG was used. The p values associated with the respective analyses are reported. These analyses were unadjusted as well as adjusted for age where applicable. Survival of female and male patients was analyzed for the whole cohort and by CKD category (no CKD, CKD stages 1–2, CKD stages 3–5) using the Kaplan–Meier method, comparing sexes by log-rank tests [15]. Survival was further analyzed by multivariable Cox-regression analysis, forcing the independent variables sex, CKD, and all potential confounders into the regression equation and also testing the interactions between sex and all other variables. However, none of the interactions was found to be statistically significant. Missing values occurred when a patient failed to answer a question or when a laboratory value was not obtained. While univariable analyses such as those comparing baseline variables by sex were based on the available non-missing data, multivariable Cox-regression analyses were done on five multiply imputed data sets (imputed by the fully conditional specification method). Hazard ratios with 95% confidence intervals and p values of the pooled results are reported. A two-sided p ≤ 0.05 was considered statistically significant.
Results
Baseline characteristics
Between January 2008 and May 2011, 773 (23.1%) women and 2,579 (76.9%) men with a ≥ 50% stenosis in at least one coronary artery were consecutively enrolled without preselection (Table 1). Compared to men, women were significantly older at time of enrollment (69.9 vs. 66.3 years, p < 0.001), had a lower eGFR (65.7 vs. 73.3 ml/min/1.73 m2, p < 0.001) and more often presented with severe CKD (39.1% vs. 26.9%), had a higher prevalence of hypertension (87.5% vs. 82.2%, p = 0.001), diabetes mellitus (28.8% vs. 24.6%, p = 0.02), and valvular heart disease (16.2% vs. 12.8%, p = 0.02), and a lower prevalence of prior myocardial infarction (26.5% vs. 34.3%, p < 0.001), previous coronary artery bypass grafting (CABG; 16.3% vs. 21.6%, p = 0.001) and percutaneous coronary intervention (PCI; 39.8% vs. 46.0%, p = 0.002). Women were significantly less often smokers (32.2% vs. 60.9%, p < 0.001), drank less alcohol (43.1% vs. 63.7%, p < 0.001), and were more often physically inactive (79.7% vs. 75.2%, p = 0.02) compared to men (Table 1).
Some of the differences in risk factor distribution could be caused by the fact that women were on average 4 years older than men. After age adjustment, the risk factors diabetes mellitus, physical inactivity, and valvular heart disease were no longer significantly different between men and women (Supplementary Table 1).
Coronary angiography, treatment, and outcome after angiography
Multivessel CAD was found in 67.5% of women and in 76.5% of men (p < 0.001; Table 2). About half of all patients with multivessel CAD had CKD stages 1–2 regardless of sex, whereas CKD stages 3–5 were more prominent in women than in men (40.2% vs. 28.1%). Women had more often normal left-ventricular ejection fraction (> 50%) than men (72.6% vs. 59.9%), whereas men had more than twice as often a severely reduced left-ventricular ejection fraction (≤ 30%) than women (4.2% in women vs. 9.4% in men, p < 0.004; Table 2).
Data regarding treatment during and after index angiography revealed no differences between women and men (Table 2). A PCI was performed in 69.6% of all women and 67.6% of all men (p = 0.3). A CABG was performed at almost equal rates in both sexes (10.4% vs. 10.2%, p = 0.9). With advanced CKD (regarding the categories no CKD, CKD stages 1–2, CKD stages 3–5), patients received less PCIs, but more CABGs (Supplemental Fig. 1a, 1b).

Kaplan–Meier survival analyses. a Kaplan–Meier curve for the cumulative survival of women (red line) and men (blue line) during 8-year follow-up. There was no difference in survival between women and men. b Kaplan–Meier curve for the cumulative survival of patients according to their renal status at enrollment. Cumulative hazard was significantly different between the three groups. (plog-rank < 0.001). Green line displays patients without CKD, blue line displays patients with CKD stages 1–2, and red line displays patients with CKD stages 3–5. c Kaplan–Meier curve for the cumulative survival of women and men according to their renal status at enrollment. There was no difference in the hazards for women and men within the same CKD group. Light green line displays women without CKD, dark green line displays men without CKD, light blue line displays women with CKD stages 1–2, dark blue line displays men with CKD stages 1–2, light red line displays women with CKD stages 3–5, and dark red line displays men with CKD stages 3–5
In-hospital complications and outcome after in-hospital treatment also showed no differences between women and men (Table 2). Stroke or myocardial infarction after index intervention were very low (5 and 7 patients, respectively, Table 2). Only 8 patients died during their in-hospital stay (Table 2).
After age adjustment (Supplementary Table 2), a significant difference between women and men existed also for performed PCI during index angiography (p = 0.04).
Medication at enrollment and at hospital discharge
Prescription rates of antihypertensive, antithrombotic, antihyperlipidemic, and diuretic drugs were significantly higher after hospital discharge than at enrollment (for all p value (visit) < 0.05, except for angiotensin II receptor blocker, Table 3). Regarding antihypertensive drug types, angiotensin-converting enzyme-inhibitors were less often prescribed to women than men (p < 0.001), whereas beta-blockers were significantly more often applied in women than men (p = 0.03). Diuretics were taken more often by women (p = 0.03) and statins were prescribed significantly less often to women than to men (p = 0.03).
Of the three guideline-recommended drug classes for treatment of CAD, only statins with an overall prescription rate of 84.0% were insufficiently prescribed after hospital discharge; more than 95% of all patients were discharged with a prescription for a platelet aggregation inhibitor and/or anticoagulant and an antihypertensive drug (Table 3).
Long-term overall survival
Follow-up data were available for 3,350 (99.9%) patients. Mean follow-up time was 83.2 months (95% confidence interval 82.3–84.1 months). In total, 663 (19.8%) patients deceased, thereof 144 (18.6%) women and 519 (20.1%) men. Kaplan–Meier estimated 8-year survival rate was 69.3% in women and 68.8% in men (plog-rank = 0.7, Fig. 1a). Regarding renal function at enrollment, survival rates decreased from 89.2% for patients without CKD to 71.9% for patients with CKD stages 1–2 and 49.0% for patients with CKD stages 3–5 (plog-rank < 0.001, Fig. 1b). There was no difference in survival rates between women and men without CKD (93.8% vs. 88.5%, plog-rank = 0.4), with CKD stages 1–2 (82.7% vs. 69.6%, plog-rank = 0.5) and with CKD stages 3–5 (41.3% vs. 49.8%, plog-rank = 0.1, Fig. 1c).
Cox-regression analysis of long-term mortality showed no significant difference between sexes (hazard ratio 0.913, 95% confidence interval 0.744–1.120; p = 0.4, Table 4). Increased mortality was associated with higher age, CKD stages 3–5, albumin/creatinine ratio, diabetes mellitus, active smoking, prior MI, valvular heart disease, peripheral artery disease, and slightly as well as severely reduced left-ventricular ejection fraction. Physical activity and a family history of CAD reduced the risk for mortality (Table 4). A power calculation for a two-sided log-rank test on the actual data indicated that a hazard ratio ≤ 0.78 or ≥ 1.26 for female sex (i.e., if the mortality risk of women was ≤ 22% or ≥ 26%, respectively, compared to men) would be detectable within our study with at least 80% power (power = probability of rejecting the null hypothesis when it is false).
Discussion
This analysis of CAD-REF Registry long-term data provides insight into sex-specific disease characteristics, treatment, and mortality of patients with normal and impaired renal function and angiographically proven CAD. Few studies [16, 17] and registries [18] have evaluated patients with CAD and CKD, but sex-specific data and analyses were not reported. Other publications have focused only on sex differences in CAD but lack data on renal function [6, 19, 20]. The inclusion of predominantly male patients, up to 77% as in our registry, is a common feature of these studies and registries. The under-representation of women has long been criticized [21], especially since cardiovascular disease is the number one cause of mortality in both women and men. However, the proportion of women in CAD studies is still at a low, ~ 25%, and thus lower than the female proportion of about 46% in the CAD population [22]. The unequal distribution between men and women in these studies may reflect a lack of awareness of how to identify women eligible for coronary angiography, but it seems to reflect the current reality in this health sector.
Baseline characteristics, extent of coronary artery disease, and interventions
The German multicenter, prospective, observational CAD-REF Registry confirms the well-known different risk profiles in cardiovascular disease of women in comparison to men: women are usually older, show a higher prevalence of risk factors and comorbidities such as CKD, diabetes mellitus, hypertension, or positive family history of CAD, and had less prior MI and fewer revascularization procedures, higher incidence of preserved LVEF, and lesser extent of CAD (6, 18,19,20, 23,24,25,26,27,28,29). In the CAD-REF Registry, the prevalence of CKD stages 1–2 (51%) or CKD stages 3–5 (30%) in patients with CAD was higher than the prevalence in the general population, e.g., 5.9% prevalence of CKD stages 3–5 in Germany [30]. In particular, CKD stages 3–5 affect women with multivessel disease more frequently than men with multivessel disease. This underlines the urgent need to examine and treat renal comorbidity especially in female patients with CAD.
Conflicting data exit on outcome of women after PCI and CABG. While some researchers found higher in-hospital mortality and worse outcome for women after PCI [31, 32], others reported no sex-specific difference for PCI and CABG [33]. In our registry, in-hospital outcome revealed no sex-specific difference. Many factors contribute to the outcome after interventions: e.g., age, acute or stable CAD, medical treatment, concomitant diseases, experience of the physician, and number of PCIs performed annually at the treatment center. Furthermore, studies, especially randomized-controlled trials, include only highly selected patients, whereas registries include patients from routine clinical practice. All these aspects might explain the different outcomes in diverse registries and studies.
Drug treatment
Control of blood pressure and atherosclerotic risk factors are the key aspects for cardiovascular disease management, especially in patients with reduced renal function. Our data on drug treatment showed high prescription rates of antihypertensive drugs (> 98%) and acetylsalicylic acid (> 91%) both for women and men after hospital discharge, but insufficient prescription rates of statins which were even lower in females (82%) compared to males (85%). Importantly, our registry showed that prescription patterns according to guidelines [34] are realized to a higher degree than about to 20 years ago [17]. Similarly, the CLARIFY registry which started in 2009 reported better secondary prevention in patients with CKD and CAD with more than 75% of all patients taking ACE inhibitors or angiotensin-receptor blockers, 95% taking antiplatelet medication, and—comparable to our findings—84% taking statins [18]. Consistently, lower treatment with statins in women was reported from researchers of the CLARIFY registry [6] and from the Dyslipidemia International Study (DYSIS) [35].
Outcome and mortality
The strength of the present analysis is the long-term observation of mortality, since patients are rarely followed up for more than 5 years. During the 8-year follow-up period, we found no difference in mortality between women and men neither overall nor when they were grouped by renal function (no CKD, CKD stages 1–2, CKD stages 3–5). Sex was not an independent predictor for mortality, in contrast to age and comorbidities such as diabetes mellitus, CKD, reduced left-ventricular ejection fraction, valvular heart disease, and peripheral artery disease. Our results show no clear advantage regarding either revascularization technique in CAD patients with CKD in terms of long-term mortality. Not surprisingly, overall-mortality was higher in patients with more advanced CKD than in patients without CKD. Several studies with follow-up periods of 1–5 years support this observation: a very recent international, multicenter registry evaluation on the outcome after contemporary PCI in patients with CAD and renal insufficiency reported that one of the most powerful parameters for adverse outcome, namely major adverse cardiovascular events including cardiac death as well as a patient-oriented composite endpoint including all-cause death, was the presence of CKD and dialysis-dependent CKD [36]. Other predictors were age, diabetes mellitus, previous MI, and smoking, all in good accordance with our findings. The CLARIFY registry [6], evaluating patients with CAD, reported a comparable 1-year outcome for men and women. The 5-year outcome of the same registry also showed no sex-specific difference in all-cause mortality [8]. Similar to our registry, main independent predictors for cardiovascular mortality or non-fatal myocardial infarction were age, diabetes, smoking, prior MI, peripheral artery disease, but also prior stroke, atrial fibrillation, and history of hospitalization for heart failure. A pooled analysis of individual patient data regarding outcome after PCI [37], a subgroup analysis of the GLOBAL LEADERS trial [38], and a sex-related study on patients with acute myocardial infarction [39] also found no association of sex with long-term mortality. In contrast, 10 years ago Ezekowitz et al. [17] reported on a higher 1-year mortality in women with CAD compared to men, but prescription rates for guideline-recommended medication were lower in that study than in our registry. Improved medical treatment strategies might have lowered the mortality risk for women in the last years. Additionally, as mentioned above, other factors such as comorbidities and lifestyle factors have an impact on mortality. Therefore, prevention and treatment of comorbidities such as chronic kidney disease, atherosclerotic disease in general, and diabetes mellitus are essential for lowering mortality. Furthermore, it should be taken into account that personal circumstances might have an influence on outcome: recently, the GENESIS-PRAXY study brought into focus that behavior and characteristics which are traditionally ascribed women influence the outcome of male and female patients with acute coronary syndrome. The researchers showed that young patients with more typical to feminine roles ascribed traits and social roles had worse outcome than patients with a personality traditionally ascribed to men, regardless of their biological sex [40].
Limitation
In our registry, patients who received a coronary angiogram were consecutively enrolled, resulting in an over-representation of men and an under-representation of women. This unequal sex distribution has been reported earlier for diverse populations undergoing coronary angiography [6, 19, 23, 27, 28] and has been criticized [21]. Therefore, the evidence base for treatment of CAD is more limited for women than for men.
Most characteristics of the patients were only collected at baseline and cardiovascular risk factors were evaluated using questionnaires, not by physical examination. Therefore, the prevalence and incidence of some cardiovascular risk factors, e.g., peripheral artery disease, may be actually higher than recorded. Also, we collected only one serum sample for estimation of GFR. Since serum creatinine concentration depends also on other factors (e.g., muscle mass and nutritional status) than kidney function, some patients may be misclassified. Similarly, proteinuria was detected by dipstick test before angiography which is a semiquantitative estimation of proteinuria and may also lead to misclassification. Blood pressure values were collected with a single measurement at patient hospitalization. The results on the impact of low or high blood pressure levels on mortality are therefore limited.
In long-term outpatient registries, it is difficult to stay in contact with patients over a very long period of time. Therefore, the number of patients for whom follow-up data could be collected decreased over time and cause of death was often unknown. This is the reason why only data on all-cause mortality are presented.
Finally, data were collected in Germany only, an industrialized country with a very sophisticated health care system. The results cannot be extrapolated to other countries or regions with limited medical care.
Conclusions
Sex differences in patients with CKD and CAD mainly exist in cardiovascular risk profile determined before diagnosis of CAD. Treatment differences between men and women were not observed, which may be the reason for similar in-hospital and long-term outcome. Therefore, sex differences may start to diminish possibly due to the broader use of effective secondary prevention. Nevertheless, further research on sex-specific strategies is warranted to optimize pharmacological and interventional treatment concepts for women and men especially with decreased renal function, since mortality rates in this high-risk group remain high.
References
Zhang QL, Rothenbacher D (2008) Prevalence of chronic kidney disease in population-based studies: Systematic review. BMC Public Health 8:117. https://doi.org/10.1186/1471-2458-8-117
Mozaffarian D, Benjamin EJ, Go AS et al (2015) Heart disease and stroke statistics–2015 update: a report from the American Heart Association. Circulation 131:e29–e322. https://doi.org/10.1161/CIR.0000000000000152
National Kidney Foundation (2002) K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification and stratification. Am J Kidney Dis 39:S1–S266
Reddan DN, Szczech LA, Tuttle RH (2003) Chronic kidney disease, mortality, and treatment strategies among patients with clinically significant coronary artery disease. J Am Soc Nephrol 14:2373–2380. https://doi.org/10.1097/01.asn.0000083900.92829.f5
Sederholm Lawesson S, Alfredsson J, Szummer K, Fredrikson M, Swahn E (2015) Prevalence and prognostic impact of chronic kidney disease in STEMI from a gender perspective: data from the SWEDEHEART register, a large Swedish prospective cohort. BMJ Open 5:e008188. https://doi.org/10.1136/bmjopen-2015-008188
Steg PG, Greenlaw N, Tardif JC et al (2012) Women and men with stable coronary artery disease have similar clinical outcomes: insights from the international prospective CLARIFY registry. Eur Heart J 33:2831–2840. https://doi.org/10.1093/eurheartj/ehs289
Lempereur M, Magne J, Cornelis K et al (2016) Impact of gender difference in hospital outcomes following percutaneous coronary intervention. Results of the Belgian Working Group on Interventional Cardiology (BWGIC) registry. EuroIntervention 12:e216–e223. https://doi.org/10.4244/EIJY14M12_11
Sorbets E, Fox KM, Elbez Y et al (2020) Long-term outcomes of chronic coronary syndrome worldwide: insights from the international CLARIFY registry. Eur Heart J 41:347–356. https://doi.org/10.1093/eurheartj/ehz660
Brand E, Pavenstädt H, Schmieder RE et al (2013) Coronary artery disease and renal failure (CAD-REF) Registry: design and methods. Am Heart J 166:449–456. https://doi.org/10.1016/j.ahj.2013.06.010
Reinecke H, Breithardt G, Engelbertz C et al (2016) Baseline characteristics and prescription patterns of standard drugs in patients with angiographically determined coronary artery disease and renal failure (CAD-REF Registry). PLoS ONE 11:e0148057. https://doi.org/10.1371/journal.pone.0148057
Flynn MR, Barrett C, Cosío FG et al (2005) The Cardiology Audit and Registration Data Standards (CARDS), European data standards for clinical cardiology practice. Eur Heart J 26:308–313. https://doi.org/10.1093/eurheartj/ehi079
Zamora E, Lupón J, Vila J et al (2012) Estimated glomerular filtration rate and prognosis in heart failure: value of the Modification of Diet in Renal Disease Study-4, chronic kidney disease epidemiology collaboration, and cockroft-gault formulas. J Am Coll Cardiol 59:1709–1715. https://doi.org/10.1016/j.jacc.2011.11.066
Levey AS, Stevens LA, Schmid CH et al (2009) A new equation to estimate glomerular filtration rate. Ann Intern Med 150:604–612. https://doi.org/10.7326/0003-4819-150-9-200905050-00006
Kleinbaum DG, Klein M (2010) Logistic regression: A self-learning text, 3rd edn. Springer, New York
Kleinbaum DG, Klein M (2012) Survival Analysis. A self-learning text, 3rd edn. Springer, New York
Pun PH, Smarz TR, Honeycutt EF, Shaw LK, Al-Khatib SM, Middleton JP (2009) Chronic kidney disease is associated with increased risk of sudden cardiac death among patients with coronary artery disease. Kidney Int 76:652–658. https://doi.org/10.1038/ki.2009.219
Ezekowitz J, McAlister FA, Humphries KH et al (2004) The association among renal insufficiency, pharmacotherapy, and outcomes in 6,427 patients with heart failure and coronary artery disease. J Am Coll Cardiol 44:1587–1592. https://doi.org/10.1016/j.jacc.2004.06.072
Kalra PR, García-Moll X, Zamorano J et al (2014) Impact of chronic kidney disease on use of evidence-based therapy in stable coronary artery disease: a prospective analysis of 22,272 patients. PLoS ONE 9:e102335. https://doi.org/10.1371/journal.pone.0102335
Ferrari R, Abergel H, Ford I et al (2013) Gender- and age-related differences in clinical presentation and management of outpatients with stable coronary artery disease. Int J Cardiol 167:2938–2943. https://doi.org/10.1016/j.ijcard.2012.08.013
Gudnadottir GS, Andersen K, Thrainsdottir IS, James SK, Lagerqvist B, Gudnason T (2017) Gender differences in coronary angiography, subsequent interventions, and outcomes among patients with acute coronary syndromes. Am Heart J 191:65–74. https://doi.org/10.1016/j.ahj.2017.06.014
Maas AH, van der Schouw YT, Regitz-Zagrosek V et al (2011) Red alert for women’s heart: the urgent need for more research and knowledge on cardiovascular disease in women: proceedings of the workshop held in Brussels on gender differences in cardiovascular disease, 29 September 2010. Eur Heart J 32:1362–1368. https://doi.org/10.1093/eurheartj/ehr048
Melloni C, Berger JS, Wang TY et al (2010) Representation of women in randomized clinical trials of cardiovascular disease prevention. Circ Cardiovasc Qual Outcomes 3:135–142. https://doi.org/10.1161/CIRCOUTCOMES.110.868307
Ndrepepa G, Cassese S, Braun S et al (2013) A gender-specific analysis of association between hyperuricaemia and cardiovascular events in patients with coronary artery disease. Nutr Metab Cardiovasc Dis 23:1195–1201. https://doi.org/10.1016/j.numecd.2013.03.005
Gevaert SA, De Bacquer D, Evrard P et al (2013) Renal dysfunction in STEMI-patients undergoing primary angioplasty: higher prevalence but equal prognostic impact in female patients; an observational cohort study from the Belgian STEMI registry. BMC Nephrol 14:62. https://doi.org/10.1186/1471-2369-14-62
Diez C, Mohr P, Koch D, Silber RE, Schmid C, Hofmann HS (2009) Age- and gender-specific values of estimated glomerular filtration rate among 6232 patients undergoing cardiac surgery. Interact Cardiovasc Thorac Surg 9:593–597. https://doi.org/10.1510/icvts.2009.208033
Suessenbacher A, Wanitschek M, Dörler J et al (2014) Sex differences in independent factors associated with coronary artery disease. Wien Klin Wochenschr 126:718–726. https://doi.org/10.1007/s00508-014-0602-9
Claassen M, Sybrandy KC, Appelman YE, Asselbergs FW (2012) Gender gap in acute coronary heart disease: Myth or reality? World J Cardiol 4:36–47. https://doi.org/10.4330/wjc.v4.i2.36
Sakata Y, Miyata S, Nochioka K et al (2014) Gender differences in clinical characteristics, treatment and long-term outcome in patients with stage C/D heart failure in Japan. Report from the CHART-2 study. Circ J 78:428–435. https://doi.org/10.1253/circj.cj-13-1009
Reynolds HR, Shaw LJ, Min JK et al (2020) Association of sex with severity of coronary artery disease, ischemia, and symptom burden in patients with moderate or severe ischemia: secondary analysis of the ISCHEMIA Randomized Clinical Trial. JAMA Cardiol 5:773–786. https://doi.org/10.1001/jamacardio.2020.0822
Brück K, Stel VS, Gambaro G et al (2016) CKD prevalence varies across the European general population. J Am Soc Nephrol 27:2135–2147. https://doi.org/10.1681/ASN.2015050542
Ndrepepa G, Kufner S, Mayer K et al (2019) Sex differences in the outcome after percutaneous coronary intervention - a propensity matching analysis. Cardiovasc Revasc Med 20:101–107. https://doi.org/10.1016/j.carrev.2018.05.010
Benamer H, Tafflet M, Bataille S et al (2011) Female gender is an independent predictor of in-hospital mortality after STEMI in the era of primary PCI: insights from the greater Paris area PCI Registry. EuroIntervention 6:1073–1079. https://doi.org/10.4244/EIJV6I9A187
Kurlansky P, Herbert M, Prince S, Mack M (2017) Coronary bypass versus percutaneous intervention: sex matters. The impact of gender on long-term outcomes of coronary revascularization. Eur J Cardiothorac Surg 51:554–561. https://doi.org/10.1093/ejcts/ezw375
Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Working Group (2012) KDIGO clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int Suppl 2:337–414
Gitt AK, Lautsch D, Horack M et al (2017) P629 Undertreatment of female patients in lipid-lowering for secondary prevention in Europe, Canada, South Africa, Middle East and China: results of the Dyslipidemia International Study (DYSIS). Eur Heart J 38(suppl_1):ehx501.P629
Scholz SS, Lauder L, Ewen S et al (2020) One-year clinical outcomes in patients with renal insufficiency after contemporary PCI: data from a multicenter registry. Clin Res Cardiol 109:845–856. https://doi.org/10.1007/s00392-019-01575-y
Kosmidou I, Leon MB, Zhang Y et al (2020) Long-Term Outcomes in Women and Men Following Percutaneous Coronary Intervention. J Am Coll Cardiol 75:1631–1640. https://doi.org/10.1016/j.jacc.2020.01.056
Chichareon P, Modolo R, Kerkmeijer L et al (2020) Association of sex with outcomes in patients undergoing percutaneous coronary intervention: a subgroup analysis of the GLOBAL LEADERS Randomized Clinical Trial. JAMA Cardiol 5:21–29. https://doi.org/10.1001/jamacardio.2019.4296
Kanic V, Vollrath M, Tapajner A, Sinkovic A (2017) Sex-related 30-day and long-term mortality in acute myocardial infarction patients treated with percutaneous coronary intervention. J Womens Health (Larchmt) 26:374–379. https://doi.org/10.1089/jwh.2016.5957
Pelletier R, Khan NA, Cox J et al (2016) Sex versus gender-related characteristics: which predicts outcome after acute coronary syndrome in the young? J Am Coll Cardiol 67:127–135. https://doi.org/10.1016/j.jacc.2015.10.067
Acknowledgements
The authors gratefully acknowledge the willingness and patience of all patients for participating in the registry and the follow-ups. We are also indebted to the enthusiastic and unlimited support of all physicians and health care staff at the recruiting centers. Finally, we thank our local study nurses Ms. Jutta Beilker, Ms. Eva Michholz, and Ms. Anke Schneider-Schwinning and our local technician Ms. Mira Schiwek for their excellent contribution to this registry.
Funding
Open Access funding enabled and organized by Projekt DEAL. The CAD-REF Registry was mainly funded by grants from the German Federal Ministry of Education and Research (BMBF) (http://www.gesundheitsforschungbmbf. de/_media/NL_36.pdf; grant number 01GI0701) and the KfH Foundation for Preventive Medicine (http://www.kfhstiftungpraeventivmedizin.de/content/foerderprogramm). Research grants were given by Amgen GmbH, Munich (https://www.amgen.de/), AstraZeneca GmbH, Wedel (http://www.astrazeneca.de/willkommen), Boehringer Ingelheim Pharma GmbH & Co. KG, Ingelheim am Rhein (http://www.boehringer-ingelheim.de/), and Sanofi-Aventis Deutschland GmbH, Frankfurt (http://www.sanofi.de/l/de/de/index.jsp). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
All authors: analysis or interpretation of data and final approval; CE: drafting; HOP: statistical analysis of data, revision of the manuscript, providing intellectual content of critical importance; EF: revision of the manuscript, providing intellectual content of critical importance; HR: conception and design of the study, drafting, and revision of the manuscript, providing intellectual content of critical importance; BS: providing intellectual content of critical importance, revision of the manuscript; MF: analysis of human material; RES: conception and design of the study, and revision of the manuscript, providing intellectual content of critical importance; KW: statistical analysis of data, and revision of the manuscript, providing intellectual content of critical importance; GB: conception and design of the study, and revision of the manuscript, providing intellectual content of critical importance; HP: conception and design of the study, and revision of the manuscript, providing intellectual content of critical importance; EB: conception and design of the study, and revision of the manuscript, providing intellectual content of critical importance.
Corresponding author
Ethics declarations
Conflict of interest
CE has received travel support from Bayer Vital outside the submitted work. EF reports grants from Bayer outside the submitted work. HR reports personal fees from Daiichi-Sankyo, DiaPlan, MedUpdate, NeoVasc, NovoNordisk, Pfizer, and Pluristem, all outside the submitted work. He has received research grants from the German Federal Ministry for Education and Research (BMBF), Bard, Biotronik, BMS/Pfizer, and Pluristem, all outside the submitted work, KW has received consulting fees/honoraria from Biotronik, Boston Scientific, Novartis. GB has no direct interest to declare with regard to this specific topic. However, during the course of this register, he had received funds from Sanofi-Aventis as chairman of the German Atrial Fibrillation Network and in his position as Co-PI for running a clinical trial, and he had been on the advisory board of Boehringer-Ingelheim for a topic not related to this registry. EB declares no conflict of interest. She has received research grants from the German Federal Ministry for Education and Research (BMBF). EB was supported by a Heisenberg Professorship from the Deutsche Forschungsgemeinschaft (Br1589/8–2). All other authors declare no conflict of interest.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki and under the auspices of the German Cardiac Society (DGK) (http://dgk.org) and the German Society of Nephrology (DGfN) (http://www.dgfn.eu). The registry protocol was approved by the Ethics Committee of the Landesaerztekammer Westfalen-Lippe and the Medical Faculty of the University of Muenster (date August 16, 2007; No 2007–315-f-S).
Consent to participate
All patients gave written informed consent prior to their inclusion.
Data availability statement
The data that support the finding of this study are available from the corresponding author upon reasonable request.
Code availability
Not applicable.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Engelbertz, C., Pinnschmidt, H.O., Freisinger, E. et al. Sex-specific differences and long-term outcome of patients with coronary artery disease and chronic kidney disease: the Coronary Artery Disease and Renal Failure (CAD-REF) Registry. Clin Res Cardiol 110, 1625–1636 (2021). https://doi.org/10.1007/s00392-021-01864-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-021-01864-5