
Abstract
Background
For 10 consecutive years, the ESPN/ERA-EDTA Registry has included data on children with stage 5 chronic kidney disease (CKD 5) receiving kidney replacement therapy (KRT) in Europe. We examined trends in incidence and prevalence of KRT and patient survival.
Methods
We included all children aged <15 years starting KRT 2007–2016 in 22 European countries participating in the ESPN/ERA-EDTA Registry since 2007. General population statistics were derived from Eurostat. Incidence and prevalence were expressed per million age-related population (pmarp) and time trends studied with JoinPoint regression. We analyzed survival trends using Cox regression.
Results
Incidence of children commencing KRT <15 years remained stable over the study period, varying between 5.5 and 6.6 pmarp. Incidence by treatment modality was unchanged over time: 2.0 for hemodialysis (HD) and peritoneal dialysis (PD) and 1.0 for transplantation. Prevalence increased in all age categories and overall rose 2% annually from 26.4 pmarp in 2007 to 32.1 pmarp in 2016. Kidney transplantation prevalence increased 5.1% annually 2007–2009, followed by 1.5% increase/year until 2016. Prevalence of PD steadily increased 1.4% per year over the entire period, and HD prevalence started increasing 6.1% per year from 2011 onwards. Five-year unadjusted patient survival on KRT was around 94% and similar for those initiating KRT 2007–2009 or 2010–2012 (adjusted HR: 0.98, 95% CI:0.71–1.35).
Conclusions
We found a stable incidence and increasing prevalence of European children on KRT 2007–2016. Five-year patient survival was good and was unchanged over time. These data can inform patients and healthcare providers and aid health policy makers on future resource planning of pediatric KRT in Europe.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
After decades of continuous growth, the incidence of kidney replacement therapy (KRT) for stage 5 chronic kidney disease (CKD 5) in European adult patients has slightly declined during the last decade, whereas the increase in prevalence has started to slow down and patient survival has improved [1].
CKD 5 etiologies in children are notably different from those in adults, as kidney failure at pediatric age is mostly caused by congenital or hereditary disorders rather than by diabetes or hypertension which are the most common causes in adults [2, 3]. Despite major improvements in pediatric nephrology care over the past 30–40 years, mortality on KRT remains 30 times higher compared to healthy peers [4, 5]. Moreover, improved patient care has resulted in the acceptance of more challenging patients into pediatric KRT programs, including very young patients and patients with more comorbidities [4].
For pediatric patients from the USA, the incidence of KRT decreased by 21% since 2004 after a long period of increasing incidence rates, whereas the prevalence was stable over the last decade [6]. Furthermore, in Australia and New Zealand, the incidence rate varied widely from year to year, but remained overall stable over the past 20 years. On the other hand, the prevalence of pediatric KRT in Australia increased, whereas there was no trend in New Zealand [7]. Data on trends in pediatric KRT are important to inform patients and healthcare providers and to aid healthy policy makers on future resource planning of pediatric KRT in Europe. Earlier European data showed a rise in KRT incidence in the 1980s which remained stable thereafter, while the prevalence of KRT among patients aged less than 20 years tripled from 1980 to 2000 [8]. However, more recent data on the incidence and prevalence of pediatric KRT in Europe have only been reported over a short time frame [4], and trends were not studied.
With 10 consecutive years of data collection on European pediatric KRT patients within the ESPN/ERA-EDTA Registry, we are now able to report on trends in the incidence, prevalence, treatment modality, and patient survival from 2007 to 2016.
Methods
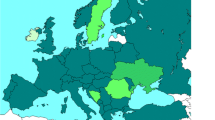
Patient data were extracted from the ESPN/ERA-EDTA Registry, a population-based registry that collects data on individual pediatric patients on KRT in Europe on an annual basis [9, 10]. Currently, 36 countries participate in the Registry. Most countries report information from pediatric centers only. As older children (15–19 years of age) may be treated in adult centers, they might not be included in the ESPN/ERA-EDTA Registry, possibly leading to an underestimation of incidence and prevalence figures. Therefore, for this study, we included data of patients initiating KRT < 15 years of age from the 22 countries contributing with data on all treatment modalities for the entire period from January 1, 2007, to December 31, 2016 (Fig. 1). For comparison reasons, we also report incidence and prevalence rates for the other countries, but these numbers are not included in the trend analyses.

European countries included in the study
Data were categorized as follows: age at initiation of KRT (for incidence) or at the 31st of December of each year (for prevalence) (0 < 5 years, 5 < 10 years, 10 < 15 years), sex (male or female), treatment modality (hemodialysis (HD), peritoneal dialysis (PD), or kidney transplantation), cause of CKD 5 (categorized according to the ERA-EDTA coding system adapted for children) [3], calendar year (2007 to 2016).
Incidence rates per million age-related population (pmarp) were calculated as the number of new cases on KRT in each calendar year divided by the mid-year age-related general population. General population characteristics were extracted from the Eurostat database [11].
Prevalence was calculated as the number of cases being alive and treated with KRT on the 31st of December of each calendar year and expressed as pmarp using the mid-year general population.
To evaluate time trends in the observed incidence and prevalence, the JoinPoint regression program provided by the Surveillance Research Program of the US National Cancer Institute was used. The annual percentage change (APC) was computed using Poisson regression provided by the JoinPoint regression program, as described previously by Kramer et al. [12]. In short, the program fits a series of joint straight lines on a log scale to the trends in observed rates. Line segments are joined at points called joinpoints, and each joinpoint denotes a statistically significant change in trend. The APC (i.e., the slope of the line segment) was calculated with the observed rate as outcome variable and year as explanatory variable, in order to describe and test the significance of the trends.
Patient survival probabilities were defined as the probability that a person has survived up to a specific time point, e.g., 1, 2, or 5 years after commencing KRT or after receiving a first kidney transplant, and causes of death were classified according to the ERA-EDTA Registry coding system, whereas cardiac failure, cardiac arrest/sudden death, myocardial ischemia and infarction, and cerebro-vascular accidents were combined as cardiovascular mortality [3]. Patients were followed from the first day of KRT (patient survival on KRT) or from the day of first kidney transplant (patient survival after transplantation) until death, lost to follow-up or end of study, whichever occurred first.
The annual number of kidney transplants performed (pmarp) between 2007 and 2016 was calculated, as well as the 1-, 2 -, and 5-year graft survival, defined as being alive with a functioning kidney transplant at 1, 2, or 5 years after transplantation, respectively.
The Cox proportional hazard regression model was used to calculate patient and graft survival probabilities, while accounting for confounders. To compare adjusted 5-year survival between two periods of initiating KRT (2007–2009 and 2010–2012), adjusted hazard ratios were calculated using Cox proportional hazard regression models. Adjustments were made for the confounding effects of country, sex, cause of CKD 5, and age and treatment modality at start of KRT.
Analyses were performed using SAS 9.4 statistical software package (SAS Institute, Cary, NC, USA) and JoinPoint version 4.7.0.0.
Two-sided P values of 0.05 were considered statistically significant.
Results
Trends in incidence
A total of 4459 patients aged 0–14 years from 22 European countries initiated KRT between 2007 and 2016. The yearly incidence of patients under 15 years commencing KRT by country fluctuated considerably from year to year (Table 1). The overall KRT incidence in Europe ranged between 5.5 pmarp and 6.6 pmarp, corresponding to 401 and 482 patients initiating KRT annually. There was no trend in the overall incidence in Europe from 2007 to 2016 (APC: − 0.8, 95% CI: − 2.5 to 1.0).
The incidence of HD tended to decrease from 2.6 pmarp in 2007 to 2.0 pmarp in 2011 and to gradually increase back to 2.6 pmarp in 2014 and 2015, but these changes were not statistically significant (Fig. 2a). The incidence of PD fluctuated between 2.0 pmarp and 3.0 pmarp, but there was no significant trend between 2007 and 2016 (APC: − 1.5, 95% CI: − 4.0 to 1.1). The pre-emptive transplantation rate showed a more stable pattern and was around 1.0 pmarp over the entire period (Fig. 2a). The distribution of first treatment modality was stable, with 80% of patients commencing KRT on dialysis (HD and PD both 40%), while 20% received a pre-emptive kidney transplant (Fig. 2b).

Incidence of KRT by treatment modality and year. a Trends in the incidence rate of pediatric KRT by treatment modality (pmarp). Trends were calculated by the APC and its 95% confidence interval. b Distribution of first KRT modality by year. Abbreviations: KRT, kidney replacement therapy; pmarp, per million age-related population; APC, annual percentage change; HD, hemodialysis; PD, peritoneal dialysis; Tx, pre-emptive kidney transplantation
Figure 3 shows the incidence rate by age group for all countries combined. The incidence rate was the highest among 10–14-year-old patients (ranging from 7.1 to 8.5 pmarp) and the lowest among patients aged 5–9 years (ranging from 4.1 to 5.4 pmarp), while it ranged from 5.5 to 6.4 pmarp in the youngest patients (< 5 years). Although the incidence rate by age group fluctuated, there were no clear trends in incidence rate according to age group.

Incidence of KRT (pmarp) by age group and year. Trends were calculated by the APC and its 95% confidence interval. Abbreviations: KRT, kidney replacement therapy; pmarp, per million age-related population; APC, annual percentage change
A statistically significant decrease in incidence rate was observed for patients with congenital anomalies of the kidney and urinary tract (CAKUT) (APC: − 3.3, 95% CI: − 5.5 to − 1.0) and metabolic disorders (APC: − 8.1, 95% CI: − 14.3 to − 1.5) leading to CKD 5, whereas the incidence rate of unknown or missing causes of CKD 5 increased significantly by 5.2% annually (95% CI: 1.1 to 9.4) between 2007 and 2016. Although not statistically significant, we observed a tendency towards decreasing numbers of patients commencing KRT due to vasculitis and hemolytic uremic syndrome (HUS). The incidence of KRT due to other causes remained stable over the study period (Table 2).
Trends in prevalence
The prevalence by country and year is shown in Table 3. There were large country differences, but the overall prevalence increased by 1.9% annually (95% CI: 1.5–2.3) from 2120 children (29.5 pmarp) on KRT on December 31st, 2007, to 2675 children on KRT (35.6 pmarp) on December 31st, 2016.
The prevalence of patients on all three treatment modalities increased during the study period (Fig. 4). For transplantation, the increase was the strongest in the first 3 years, with an annual change of 5.1% (95% CI: 1.8–8.6), whereas the annual increase was 1.5% (95% CI: 1.1–1.9) for the following years. The HD prevalence started to increase from 2011 onwards with 6.1% annually (95% CI: 2.2–10.0), while PD prevalence steadily increased by 1.4% annually (95% CI: 0.1–2.7) between 2007 and 2016.

Prevalence of KRT (pmarp) by treatment modality and year. Trends were calculated by the APC and its 95% confidence interval. Abbreviations: KRT, kidney replacement therapy; pmarp, per million age-related population; APC, annual percentage change, HD, hemodialysis; PD, peritoneal dialysis; Tx, kidney transplantation
For all age groups, the prevalence increased (Fig. 5). The smallest increase was observed for the youngest patients (APC: 1.6%, 95% CI: 0.5–2.7), while the strongest increase was observed for patients aged 10–14 years between the years 2007 and 2009, with an annual increase of 4.6% (95% CI: 1.5–7.8%). In the period thereafter, the prevalence for 10–14-year-old patients increased by 1.3% annually.

Prevalence of KRT (pmarp) by age group and year. Trends were calculated by the APC and its 95% confidence interval. Abbreviations: KRT, kidney replacement therapy; pmarp, per million age-related population; APC, annual percentage change
Patient survival on KRT and causes of death
During follow-up, 225 patients died after a median follow-up of 4.1 years (IQR: 1.9–6.4). Overall 1-, 2-, and 5-year patient survival were 97.6% (95% CI: 97.1–98.1), 96.4% (95% CI: 95.8–96.9), and 94.4% (95% CI: 93.6–95.2), respectively. Similar adjusted survival probabilities were found (Table 4). Most patients died from cardiovascular disease (28.9%), followed by infections (22.7%), and for 23.1% of patients, the cause of death was missing or unknown.
For patients commencing KRT in the period 2007–2009, the 5-year unadjusted survival probability was 93.9% (95% CI: 92.6–95.2), whereas it was 93.3% (95% CI: 91.8–94.7) for patients commencing KRT between 2010 and 2012. After adjustment for age, sex, cause of CKD 5, and treatment modality at start, the patient survival at 1, 2 (data not shown), and 5 years did not differ between the periods (adjusted HR 2010–2012 vs. 2007–2009: 0.98, 95% CI: 0.71–1.35). The causes of death differed by period (Table 5). Patients who commenced KRT between 2007 and 2009 died more often from infections (31.3%), whereas cardiovascular disease was more often the cause of death (41.3%) for patients who commenced KRT between 2010 and 2012 (P < 0.001).
Kidney transplantation and graft survival
The overall number of kidney transplants (pre-emptive and non-pre-emptive, deceased and living donor) performed annually was stable and varied between from 3.1 to 3.9 pmarp (APC: − 1.4%, 95% CI: − 2.8–0.1).
Overall unadjusted graft survival was 94.4% (95% CI: 93.5–95.3) at 1 year and 89.1% (95% CI: 87.8–90.5) at 5 years post-transplantation. Graft survival varied by year between 90.8% (95% CI: 87.3–94.4) and 97.0% (95% CI: 94.8–99.2) at 1 year and between 87.1% (95% CI: 83.2–91.2) and 94.1% (95% CI: 91.2–97.0) at 5 years after transplantation, but did not change over time (Table 6).
Overall unadjusted patient survival after transplantation was 98.8% (95% CI: 98.4–99.3), 98.5% (95% CI: 97.9–99.0), and 97.2% (95% CI: 96.3–98.1) at 1, 2, and 5 years post-transplantation, respectively.
Discussion
In this ESPN/ERA-EDTA Registry study, we found a stable incidence and an increasing prevalence of nearly 2% per year in European pediatric KRT over the last decade. The first mode of KRT was stable over time, with the majority of patients initiating KRT on dialysis (both HD and PD 40%), and 20% of patients received a pre-emptive kidney transplant. Patient survival was good and did not change over time, but we found a shift in causes of death. Patients who commenced KRT before 2010 died more often from infectious causes, whereas patients commencing KRT later were more likely to die from cardiovascular disease.
Incidence
A previous ERA-EDTA Registry study reported a stable incidence for patients initiating KRT at an age below 19 years of age between 1997 and 2006 [12]. Similarly, we found a stable overall incidence of European patients commencing KRT before the age of 15 years over the last decade. Also, in Australia and New Zealand, the overall trend in the incidence of treated CKD 5 patients <18 years was stable for the past 20 years [7]. A more recent ERA-EDTA Registry study, studying the years 2001 to 2011, reported a small decrease of 2.5% per year in the incidence of European patients below 19 years [1]. Although the incidence increased prior to 2004, also in the USA, the incidence of children (0–21 years of age) requiring KRT has steadily declined between 2004 and 2016 [6]. Differences between our study and the other cohorts might in part be caused by different age limits of included patients, as well as by differences in the years studied. However, none of the recent studies reported an increase in incident pediatric patients requiring KRT for CKD 5, suggesting that pediatric nephrologists are succeeding in their efforts to prevent progression to stage 5 CKD.
In adults, lifestyle-related diseases such as hypertension, diabetes, and obesity are important risk factors for CKD [13]. Although there are some studies reporting similar associations for the pediatric population [14, 15], causes of CKD 5 in children are mostly of congenital and hereditary origin [2]. We did, however, observe changes in the causes of kidney disease over time. The number of children who needed KRT due to CAKUT decreased on average by 3.3% per year over the 10-year study period. According to the European network of congenital anomaly registries, there were more live births of children with congenital urinary anomalies in the same period [16], which might further strengthen the hypothesis of successful pre-CKD 5 treatment in this category of European children with CKD. We also found a decrease in the number of children initiating KRT due to rare diseases, such as metabolic disorders, HUS, and vasculitis, which might be the result of advances in timely and more accurate diagnosis, as well as the emergence of new therapeutics (i.e., biologics and monoclonal antibodies). At the same time, we found an increase in the number of children initiating KRT because of an unknown or missing cause of CKD 5. Although this might be due to a registration issue, it could also suggest that the number of complex cases, in which it is difficult to identify a single or clear diagnosis, accepted into KRT programs is increasing. Furthermore, it might also be the result of late referral, which might imply that fewer biopsies were performed. Indeed, in a UK study, patients with an uncertain etiology were more likely to be referred late [17].
Prevalence
In accordance with findings in European adults [1] and in Australian children [7], this study found that the overall prevalence of European children on KRT has increased by nearly 2% per year over the 10-year study period. In contrast, the prevalence of KRT for pediatric patients from the USA and from New Zealand remained stable for the most recent decade [6, 7]. In the US, the incidence rate decreased and the survival improved resulting in a stable prevalence rate [6].
We observed an increasing trend in prevalence for all age groups and for all treatment modalities. Throughout the study period, the prevalence for both dialysis modalities was similar, whereas the number of patients living with a functioning transplant was about 4 to 5 times larger than the number of patients treated with dialysis. We did not find any further improvement in patient survival, but as long as the number of new CKD 5 cases is higher than the numbers of deaths, the prevalence rate will continue to grow.
Mortality
Overall, 1- and 5-year patient survival on KRT were 98% and 94%, respectively, and are similar to or slightly higher than rates reported in other high-income countries [18]. We found a stable patient survival throughout the decade. Although the 1-year patient mortality has decreased by 20% over the last decade in US pediatric patients, the 5-year survival probability for those starting KRT from 2002 to 2006 was 89% [19], whereas it was 91% for those starting KRT between 2007 and 2011 [6] and therefore patient survival in the US was lower than that in Europe.
The improvement in patient survival of pediatric KRT has possibly reached its ceiling, but mortality remains at least 30 times higher than in the general pediatric population [18].
Patients initiating KRT between 2007 and 2009 died more often from infections, whereas cardiovascular disease was the leading cause of death for patients initiating KRT between 2010 and 2012. Although others also reported cardiovascular disease and infections to be the leading causes of death in pediatric KRT patients [6, 20,21,22], a decrease in cardiovascular mortality due to vigorous cardioprotective management has been reported. However, these findings were mainly based on data from patients treated during the last decades of the twentieth century or from adult patients who commenced KRT during childhood [20, 22,23,24]. Due to a high number of cases for whom the cause of death was reported as unknown or missing, as well as the relatively short period of time, we cannot draw any conclusions about trends in causes of death over time. Future studies with longer periods of follow-up are needed to determine whether a trend towards higher cardiovascular mortality exists in the European pediatric KRT population, and which specific factors are involved.
Kidney transplantation
We did not find an overall trend in the number of kidney transplants performed. Also the graft survival remained stable over time. The prevalence of kidney transplantation increased over the decade as the incidence of kidney transplantation continues to outweigh the number of patients whose kidney graft fails. One-year graft survival remained stable over the study period ranging from 91.5 to 97.3%. Overall graft survival was 94% at 1 year and 89% at 5 years and thereby slightly higher than in registry studies from Australia and New Zealand (83%) and the USA (86% for living donor kidneys and 79% for deceased donor kidneys) [7, 25].
As with every KRT registry, a limitation of our study is that only CKD 5 patients treated with KRT are included, and the numbers presented in this study do not reflect pediatric patients with CKD 5 not (yet) on KRT. Furthermore, only countries that participated in the ESPN/ERA-EDTA Registry for the entire study period of 2007 to 2016 are included in the current study, and our study might not be fully representative for the whole of Europe. However, our study is the first one to provide data on trends in incidence, prevalence, and rates of kidney transplantation and patient survival for European pediatric KRT patients over a 10-year period.
In conclusion, we found a stable incidence and an increasing prevalence of European children on KRT over the past decade. Five-year patient survival was good and did not change over time. Also, the annual number of kidney transplantations performed did not change. These data can be used for future resource planning of pediatric KRT in Europe.
References
Pippias M, Jager KJ, Kramer A, Leivestad T, Sánchez MB, Caskey FJ, Collart F, Couchoud C, Dekker FW, Finne P, Fouque D, Heaf JG, Hemmelder MH, Kramar R, De Meester J, Noordzij M, Palsson R, Pascual J, Zurriaga O, Wanner C, Stel VS (2016) The changing trends and outcomes in renal replacement therapy: data from the ERA-EDTA Registry. Nephrol Dial Transplant 31:831–841
ESPN/ERA-EDTA Registry: ESPN/ERA-EDTA Registry Annual Report 2016. Amsterdam UMC, location AMC, Department of Medical Informatics, Amsterdam, the Netherlands, 2018
ERA-EDTA Registry: ERA-EDTA Registry Annual Report 2017. Amsterdam UMC, location AMC, Department of Medical Informatics, Amsterdam, the Netherlands, 2019
Chesnaye N, Bonthuis M, Schaefer F, Groothoff JW, Verrina E, Heaf JG, Jankauskiene A, Lukosiene V, Molchanova EA, Mota C, Peco-Antić A, Ratsch IM, Bjerre A, Roussinov DL, Sukalo A, Topaloglu R, van Hoeck K, Zagozdzon I, Jager KJ, van Stralen KJ, ESPN/ERA-EDTA Registry (2014) Demographics of paediatric renal replacement therapy in Europe: a report of the ESPN/ERA-EDTA Registry. Pediatr Nephrol 29:2403–2410
Chavers BM, Molony JT, Solid CA, Rheault MN, Collins AJ (2015) One-year mortality rates in US children with end-stage renal disease. Am J Nephrol 41:121–128
United States Renal Data System. 2018 USRDS annual data report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2018
ANZDATA Registry. 41st report, chapter 11: Paediatric patients with end stage kidney disease requiring renal replacement therapy, Australia and New Zealand Dialysis and Transplant Registry, Adelaide, 2018
van der Heijden BJ, van Dijk PCW, Verrier-Jones K, Jager KJ, Briggs JD (2004) Renal replacement therapy in children: data from 12 registries in Europe. Pediatr Nephrol 19:213–221
Tizard EJ, Verrina E, van Stralen KJ, Jager KJ (2009) Progress with the European Society for Paediatric Nephrology (ESPN)/ERA-EDTA Registry for children with established renal failure (ERF). Nephrol Dial Transplant 24:2615–2617
ESPN/ERA-EDTA Registry website. [Available from: https://espn-reg.org/index.jsp]. Accessed on 13 January 2020
Eurostat website. [Available from: https://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=demo_pjan&lang=en]. Accessed on 20 September 2019
Kramer A, Stel VS, Zoccali C, Heaf K, Ansell D, Grönhagen-Riska C, Leivestad T, Simpson K, Pálsson R, Postorino M, Jager KJ, ERA-EDTA Registry (2009) An update in renal replacement therapy in Europe: ERA-EDTA Registry data from 1997 to 2006. Nephrol Dial Transplant 24:3557–3566
Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJ, Mann JF, Matsuhita K, Wen CP (2013) Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms and prevention. Lancet 382:339–352
Staples AO, Greenbaum LA, Smith JM, Gipson DS, Filler G, Warady BA, Martz K, Wong CS (2010) Association between clinical risk factors and progression of chronic kidney disease in children. Clin J Am Soc Nephrol 5:2172–2179
Gunta SS, Mak RH (2013) Is obesity a risk factor for chronic kidney disease in children? Pediatr Nephrol 28:1949–1956
European network of population-based registries for the epidemiological surveillance of congenital anomalies (EUROCAT) website. [Available from: https://eu-rd-platform.jrc.ec.europa.eu/eurocat_en]. Accessed on 1 March 2020
Pruthi R, Casula A, Inward C, Roderick P, Sinha MD (2016) Early requirement for RRT in children at presentation in the United Kingdom: association with transplantation and survival. Clin J Am Soc Nephrol 11:795–802
Chesnaye NC, van Stralen KJ, Bonthuis M, Harambat J, Groothoff JW, Jager KJ (2018) Survival in children requiring chronic renal replacement therapy. Pediatr Nephrol 33:585–594
U.S. Renal Data System, USRDS 2013 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2013
Groothoff JW, Gruppen MP, Offringa M, Hutten J, Lilien MR, van de Kar NJ, Wolff ED, Davin JC, Heymans HS (2002) Mortality and causes of death of end-stage renal disease in children: a Dutch cohort study. Kidney Int 61:621–629
McDonald SP, Graig JC, Australian and New Zealand Paediatric Nephrology Association (2004) Long-term survival of children with end-stage renal disease. N Engl J Med 350:2654–2662
Mitsnefes MM, Laskin BL, Dahhou M, Zhang X, Foster BJ (2013) Mortality risk among children initially treated with dialysis for end-stage kidney disease, 1990-2010. JAMA 309:1921–1929
Vogelzang JL, van Stralen KJ, Jager KJ, Groothoff JW (2013) Trend from non-cardiovascular late mortality in patients with renal replacement therapy since childhood. Nephrol Dial Transplant 28:2082–2089
Vogelzang JL, Heestermans LWAA, van Stralen KJ, Jager KJ, Groothoff JW (2013) Simultaneous reversal of risk factors for cardiac death and intensified therapy in long-term survivors of paediatric end-stage renal disease over the last 10 years. Nephrol Dial Transplant 28:2545–2542
North American Pediatric Renal Trials and Collaborative Studies. NAPRTCS 2014 Annu Rep, 2014
Acknowledgments
We would like to thank the patients, their parents, and the staff of all the dialysis and transplant units who have contributed data via their national registries and contact persons. We also would like to thank R Topaloglu, J Oh, Z Massy, and MD Sinha for being members of the ESPN/ERA-EDTA Registry Committee; D Shtiza, R Kramar, D Pokrajac, K van Hoeck, and the Centre contributors to the Belgian Registry Committee; A Sukalo, I Sheuchuk, O Liachovskaya, A Dudarevic, D Kavalenka, E Maurer, GF Laube, CE Kuehni, H Chehade, and the Swiss Paediatric Renal Registry; A Elia, T Seeman, K Vondrak, K Krupka, B Höcker, L Pape, B Tönshoff, L Weber, G von Gersdorff, J Dötsch, F Schaefer, K Hommel, Ü Toots, A Alonso Melgar, and the Spanish Paediatric Registry; J Helve, P Finne, P-H Groop, C Couchoud, M Lassalle, E Berard, T Davitaia, G Moustakas, A Kapogiannis, A Mitsioni, N Printza, D Milosevic, M Ban, J Slavicek, D Arapovic, S Abdovic, G Reusz, Cs Berecki, A Szabó, T Szabó, A Barczi, O Lakatos, E Kis, A Awan, T Raftery, C Sweeney, N Dolan, M Riordan, M Stack, M Waldron, R Palsson, V Edvardsson, B Gianoglio, E La Porta, F Paglialonga, M Parolin, C Pecoraro, A Jankauskiene, S Rudiatis, A Popova, V Kuzema, H Čerņevskis, S Gatcan, O Berbeca, N Zaikova, N Revenco, E Sahpazova, N Abazi, S Pavićević, V Said-Conti, L Heuveling, and MH Hemmelder on behalf of the Nefrovisie foundation; JW Groothoff and all centers participating in the RichQ-study; A Åsberg, AV Reisæter, A Zurowska, I Zagozdzon, C Mota, R Stone, C Simão, M Kostić, B Spasojević, M Cvetković, I Gojković, D Paripović, G Miloševski-Lomić, NA Tomilina, KG Prütz, M Stendahl, M Evans, S Schön, M Segelmark, T Lundgren, L Podracka, G Kolvek, N Battelino, G Novljan, J Buturovic-Ponikvar, S Bakkaloglu, DD Ivanov, SP Fomina, L Plumb, F Braddon, A Casula, and H Maxwell for contributing data to the ESPN/ERA-EDTA Registry.
Funding
The ESPN/ERA-EDTA Registry is funded by the European Society of Paediatric Nephrology (ESPN), and the European Renal Association–European Dialysis and Transplant Association (ERA-EDTA). Furthermore, Amgen has agreed to provide an unrestricted grant to assist the ERA-EDTA on the financial support of the ESPN/ERA-EDTA Registry. This article was written by M Bonthuis et al. on behalf of the ESPN/ERA-EDTA Registry and the ERA-EDTA Registry which is an official body of the ERA-EDTA (European Renal Association–European Dialysis and Transplant Association).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(DOCX 14 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bonthuis, M., Vidal, E., Bjerre, A. et al. Ten-year trends in epidemiology and outcomes of pediatric kidney replacement therapy in Europe: data from the ESPN/ERA-EDTA Registry. Pediatr Nephrol 36, 2337–2348 (2021). https://doi.org/10.1007/s00467-021-04928-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-021-04928-w