
Abstract
Purpose
Quality registers give unique possibilities to achieve information from large groups of patients, but outcome must be interpreted carefully due to less stringent data collection and lower follow-up rates than in research projects. We tried to quantify any outcome differences between a national spine quality register and a prospective observational study.
Methods
Adult patients treated with lumbar discectomy between 2004 and 2010 were retrieved from the Swedish Spine register (Swespine) (n = 7791) and from the single center lumbar disc herniation study (LDHS) in Stockholm (n = 177). The mean follow-up rates at 1 and 2 years were 73 and 62%, compared to 98 and 99%, respectively. Patient-reported outcome measurements included VAS for back and leg pain, ODI, EQ-5D, patient satisfaction, and global assessment.
Results
When comparing the two cohorts at baseline, there were minor differences in the patient-reported outcome measurements, all within reported minimal clinical important differences (MCID). Mean outcome improved significantly in both groups after surgery. All outcomes at 1 and 2 years were similar and within the reported MCID in both groups. Complications and reoperations were similar, except for more surgical site infections in the LDHS group.
Conclusions
Higher response rates than seen in Swespine are not needed to achieve reasonably representative data on patient-reported outcome for large cohorts. Two-year data do not seem to add additional information.
Graphical abstract
These slides can be retrieved under Electronic Supplementary Material.

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Multicenter gathering of data in quality registries gives unique possibilities to achieve information from large groups of patients [1]. Data collection in registers is usually less stringent than in research projects. For example, data are not collected by the researchers, diagnoses may be uncertain, the quality of data is unknown, data may be missing, and the study design is often retrospective, even if data are collected prospectively [2].
Another major limitation of register studies involving questionnaires is often the relatively high proportion of non-responders. In two recent studies based on the Swedish National Spine register ‘Swespine’, the non-responders consisted of a higher proportion of men, were slightly younger, more frequent smokers, and had a longer preoperative leg and back-pain duration [3, 4]. Therefore, the responders may not be completely representative of the surgically treated population.
In individuals treated for lumbar degenerative disorders, others have compared follow-up data from the initial questionnaire responders to non-responders and did not find any major discrepancies between the two groups [5, 6]. However, the proportions of initial non-responders were low, 22% and 12%, respectively, and these studies were done at single hospitals. Thus, these results still leave uncertainty regarding the interpretation of data from a nation-wide register like Swespine.
We choose another way to elucidate the validity of Swespine, by comparing register data with a locally performed prospective observational study, the lumbar disc herniation study ‘LDHS’, which has an unusually high follow-up rate.
We hypothesized that patients treated with surgery for lumbar disc herniation in Swespine and LDHS have (1) similar preoperative characteristics, (2) similar outcome at 1 and 2 years, and (3) similar relation between patient satisfaction and ODI/VAS leg pain, despite a large variation in data collection between the two cohorts.
Materials and methods
Swespine
Swespine [1] was introduced in 1993 to obtain prospective data on outcome following spine surgery in Sweden and has since the start been developed continually. The coverage (the number of clinics performing spine surgery, using the register) is approximately 90%. The completeness (the number of patients reported to Swespine at the time of surgery) is approximately 75%. ‘Opt-out’ is used, which means that unless the patient actively declines participation, the surgeon registers diagnosis, type of surgical procedure, length of hospitalization, and any complications occurring during the in-patient stay.
The patient is asked to fill out a questionnaire without the assistance of health care personnel, including data on anthropometrics, co-morbidities, smoking status, medication, work, sick leave, and patient-reported outcome measurements (PROMs) before surgery, 1, 2, 5, and 10 years postoperatively. At the 1-year follow-up, the patients are also asked whether any complications occurred during the first 3 months after surgery. All questionnaires are mailed to the patient and answered without the assistance of personnel involved in the care. One reminder is sent.
Lumbar disc herniation study
The prospective observational study, LDHS, included patients admitted for lumbar disc herniation surgery at Södersjukhuset, Stockholm, Sweden. Details of the study have been presented earlier [7]. Inclusion criteria were: one-level paramedian or central lumbar disc herniation, radiculopathy with corresponding MRI finding, a duration of more than 2 months, or earlier if requiring hospitalization, a need for 25% or more of sick leave or similar disability, and an age of 18 years or older. Exclusion criteria were ‘cauda equina impaction’, previous lumbar spine surgery, intra- or extraforaminal localization of the disc herniation and conditions that could affect follow-up or outcome interpretation, such as difficulties to understand Swedish, severe psychiatric illness, drug abuse, or co-morbidity. The LDHS used the same questionnaires and management of these, as in Swespine, but with additional follow-ups at 6 weeks and 6 months. Research nurses ensured the data quality and frequent reminders for follow-ups were sent to reach a high response rate.
We applied the same inclusion and exclusion criteria to Swespine as used in the LDHS, except for those not available in Swespine; ‘corresponding MRI finding’, ‘duration of more than 2 months, or earlier if requiring hospitalization’, and a ‘need for 25% or more of sick leave or similar disability’ and information about ‘conditions that could affect follow-up’. At least 1 of the 7 outcome variables at 1 and 2 years postoperatively were needed for inclusion.
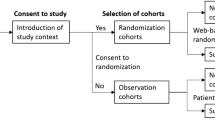
Flowcharts of the patients in the two cohorts are shown in Figs. 1 and 2.

Flow charts of patients in Swespine

Flow charts of patients in the Lumbar Disc Herniation Study
Patient-reported outcome measures
The following PROMs were used; back- and leg pain, measured from 0 (no pain) to 100 (maximum pain) on a ‘Visual Analog Scale’ (VAS) [8]; the ‘Oswestry Disability Index’ (ODI), a questionnaire for rating disability and function related to back problems [9] giving a score from 0 (best) to 100 (worst); ‘EuroQol 5-dimensions’ (EQ-5D), a form measuring quality of life, translated to an index between − 0.59 (worst) and 1.00 (best) [10] and preoperatively, ‘Short Form 36’ (SF-36) that for each of the eight sections range from 0 (worst) to 100 (best) [11]. SF-36 was in this study only used at baseline.
At the 1- and 2-year follow-ups, identical questionnaires were mailed to the patient, also including questions on ‘Satisfaction’ and ‘Global Assessment’ (GA) of back- and leg pain [12]. The Satisfaction question is formulated: ‘Are you satisfied with the result of the surgery?’ The three alternative answers were dichotomized into ‘Satisfied’, vs ‘Uncertain’ and ‘Dissatisfied’. The GA of back-pain question was formulated ‘How is your back pain today, when compared to before surgery?’ The five alternative choices were dichotomized into ‘Pain free’ and ‘Much better’ vs ‘Somewhat better’, ‘Unchanged’, or ‘Worse’. The GA question for leg pain was treated in the same way.
Reoperations and complications
Reoperations on the same spinal segment and side were reported by the surgeon performing the reoperation and counted if within 2 years. Complications occurring during the in-patient stay were reported by the surgeon and complications occurring during the first 3 months were reported by the patient at the 1-year follow-up.
Statistics
Descriptive data are presented as mean (SD), or number (%). The study groups are compared with the Student’s t test (if equal variances) or the Welch–Satterthwaite’s t test (if unequal variances) for continuous variables and with Chi-square test for categorical variables after dichotomization.
Outcome analysis was conducted with analysis of covariance for continuous variables and with logistic regression for categorical. Adjustments were made for variables with significant differences between the groups at baseline.
VAS leg pain and ODI may be considered the most important variables for outcome after lumbar disc herniation. Satisfaction with the surgical result and its relation to these two variables were compared between the cohorts. We used ‘Receiver Operating Characteristics’ (ROC) curves to define the optimal cut-off value for VAS leg pain and ODI at 1 year using Youden’s index (maximum = sensitivity + specificity − 1) [13]. The ‘Area Under the Curve’ (AUC) is the area under the curve to the bottom right corner, representing the accuracy of the test variable, to correctly classify the external criterion. We used the DeLong test for group comparisons of AUC:s [14].
SPSS version 23 was used for the statistical analysis. Missing data were excluded analysis by analysis. The level of significance was set to P < 0.05.
Ethical approval
The study was approved by the Ethics Committee at the Karolinska University Hospital Huddinge, Stockholm (number 310/98) and the Stockholm Regional Ethical Review Board (number 2012/206-31/1).
Results
When comparing the Swespine and the LDHS cohorts at baseline, there were statistically significant differences in age, co-morbidities, belief in return to work, retirement and disability pension, duration of back pain > 3 months, preoperative VAS back pain, SF-36 Role Physical and SF-36 Role Emotional (Table 1).
After surgery, the mean outcome improvement, satisfaction, and global assessment of leg and back pain were similar in both groups except from VAS back pain (unadjusted analysis) at 1 and 2 years (Table 2). After adjustment for baseline differences in analyses of covariance, VAS back-pain lost significance, but ODI and EQ-5D reached significance, although showing very small differences in absolute values (data not shown). Looking at absolute values of the outcome (Table 3) at 1 year, there were no statistically significant differences, except at 2 years, when ODI and EQ-5D were more favourable in Swespine. Adjustment for baseline differences in analyses of covariance increased the significance, but the absolute differences were still small (data not shown). There were no evident trends of outcome change between 1 and 2 years within the two cohorts, despite a larger loss to follow-up in the Swespine cohort (Table 3).
Reoperations and other complications did not differ between the groups, except for surgical site infection, being more common in the LDHS cohort (Table 4).
The ROC curves for LDHS and Swespine are shown in Fig. 3. The cutoff for being ‘Satisfied’ with the surgical result at the 1-year follow-up was 24 for VAS leg pain and 22 for ODI in Swespine, and 26 and 27 in the LDHS cohort, respectively (Table 5). The ‘Area Under the Curve’ (AUC) shows ‘Good’ and ‘Excellent’ accuracy for Swespine and LDHS, at 1 year, respectively, with no significant differences between the groups (Table 5) [15].

‘ROC’ curves show the sensitivity and one specificity at all values of VAS leg pain and ODI at 1 year, corresponding to the variable Satisfaction dichotomized into satisfied vs uncertain or dissatisfied
Non-response analysis
The baseline variables of the patients missing at 1 and 2 years in Swespine were compared to the responders at the same time. The largest differences were: non-responders compared to the responders, more often males (60 vs 54%), younger (41.6 vs 44.8 years), smokers (28 vs 19%), unemployed (16 vs 11%), had heavy physical work strain (32 vs 24%), non-elective admission (20 vs 17%), and less retirement pension (5 vs 9%). At 2 years, similar differences between non-responders and responders were seen.
Discussion
Results from studies with a high follow-up rate, for example, randomized controlled trials, or cohort studies take long time and much effort to achieve. Gathering data from national quality or other multicenter registers often result in vast amounts of data during relatively few years. As discussed, the problem on hand is frequently a lower quality of data and non-responders. If these shortcomings could be handled properly, much would be gained in terms of earlier knowledge and clinical improvements and at lower cost and less spend of scientific resources.
A direct comparison between Swespine register data and a much smaller cohort study with a high degree of follow-up after surgery for lumbar disc herniation showed some differences in baseline variables, but similar clinical outcome.
Any differences in VAS leg pain, ODI, VAS back pain, and EQ-5D at baseline, as well as change from baseline to 1- and 2-year postoperative, were non-significant or small and below the reported minimal clinical important differences (MCID) [16,17,18]. Despite a loss to follow-up in the Swespine cohort between 1 and 2 years, no change in the relation to the data in the LDHS cohort was found.
The LDHS group was in mean 3 years younger than the Swespine group. The reason for this is unknown, but may explain some of the difference in the variables concerning co-morbidity, retirement, and belief in working ability. More co-morbidity, a higher proportion of retired and a higher age, could lead to a less favorable outcome in Swespine, but was not reflected in the outcome data comparisons at 1 and 2 years [19, 20].
The concept of PASS (Patient Acceptable Symptom State), i.e., the level of pain or discomfort a patient regards as acceptable, has recently been suggested to be 22 for ODI based on the ‘Core Outcome Measures Index score’ (COMI) as external criterion [21]. The absolute values of the outcome in our study are almost identical in the two cohorts at 1 and 2 years. In both cohorts, the mean ODI values are lower (18–21) than the proposed PASS value of 22. As these values are means of the whole study populations, they include also the patients not satisfied, implying that the means of the satisfied study groups are even lower. Patients in our two cohorts had similar relationships between the external criterion, ‘Satisfaction’, and the level of ODI and VAS leg pain. The LDHS group had slightly higher cut-off points than the Swespine group, possibly a result of the also slightly higher initial back-pain value, enabling a little higher pain tolerance. The differences were though clearly lower than the suggested MCID values [16,17,18].
The outcomes of ‘Satisfaction’ and ‘GA back- and leg pain’ were also very similar in the two groups, showing around 75% of acceptable results, which is a result that seems to be rather reproducible in degenerative low back surgery through the decades [19, 22, 23]. As the aim of this study is to show if there is any real difference between the groups, the unadjusted outcome values are presented, but even adjusted for variables showing differences in baseline values, this did not alter the results essentially.
Regarding complications and reoperations, the only significant difference is an approximately 50% higher relative infection rate postoperatively in the LDHS cohort. This finding is probably an effect of more efficient reporting in the LDHS group after discharge, as there are both 6-week and 6-month follow-ups. Thromboembolic events may also appear after discharge from hospital, but are fewer and often more serious, thus probably better reported. Dural or neural damage is reported during hospitalization time irrespective of study group.
The study design has some limitations. The study cohorts are prospectively collected, but with probably less stringent inclusion criteria in Swespine. Attempts were made to imply similar inclusion and exclusion criteria retrospectively in the two cohorts. As some information is not included in Swespine, the cohorts can never be perfectly matched. Even though we had no MRI information in Swespine, we assume that MRI findings corresponded to symptoms also in the Swespine cohort. In addition, baseline data on duration of leg pain and sick leave were without significant differences between the groups, indicating that the cohorts were comparable.
In the non-response analysis, the missing groups at 1 and 2 years were compared to the responders at the same time. The absolute differences between these groups were mainly small, although the relative difference in smokers and unemployment, for instance, was about 50%. Altogether, this could result in a less favorable outcome for the non-responders, leaving the responders to a possibly better outcome. However, the results of this study do not show any difference in clinical importance in any outcome variable. Results from the previous studies in various areas have usually found that responders seem to be healthier, with a better outcome than non-responders [24,25,26]. However, this does not seem to be the case after surgical treatment for lumbar degenerative disorders [5, 6]. Our data further support this, even though we cannot be certain that our findings are valid in other lumbar disorders. In addition, we also note that the lack of a trend of change in outcome between the 1- and 2-year follow-ups in both cohorts indicate that a 1-year follow-up may be sufficient when studying outcome after lumbar discectomy.
Conclusion
Higher response rates than seen in Swespine are not needed to achieve reasonably representative data on patient-reported outcome for large cohorts. Two-year patient-reported outcome data do not seem to add additional information in the follow-up of lumbar disc hernia surgery.
References
Stromqvist B, Fritzell P, Hagg O, Jonsson B, Sanden B (2013) Swespine: the Swedish spine register: the 2012 report. Eur Spine J 22:953–974. https://doi.org/10.1007/s00586-013-2758-9
Thygesen LC, Ersboll AK (2014) When the entire population is the sample: strengths and limitations in register-based epidemiology. Eur J Epidemiol 29:551–558. https://doi.org/10.1007/s10654-013-9873-0
Elkan P, Sjovie Hasserius J, Gerdhem P (2016) Similar result after non-elective and elective surgery for lumbar disc herniation: an observational study based on the SweSpine register. Eur Spine J 25:1460–1466. https://doi.org/10.1007/s00586-016-4419-2
Lagerback T, Elkan P, Moller H, Grauers A, Diarbakerli E, Gerdhem P (2015) An observational study on the outcome after surgery for lumbar disc herniation in adolescents compared with adults based on the Swedish Spine Register. Spine J 15:1241–1247. https://doi.org/10.1016/j.spinee.2015.02.024
Hojmark K, Stottrup C, Carreon L, Andersen MO (2016) Patient-reported outcome measures unbiased by loss of follow-up. Single-center study based on DaneSpine, the Danish spine surgery registry. Eur Spine J 25:282–286. https://doi.org/10.1007/s00586-015-4127-3
Solberg TK, Sorlie A, Sjaavik K, Nygaard OP, Ingebrigtsen T (2011) Would loss to follow-up bias the outcome evaluation of patients operated for degenerative disorders of the lumbar spine? Acta Orthop 82:56–63. https://doi.org/10.3109/17453674.2010.548024
Elkan P, Sten-Linder M, Hedlund R, Willers U, Ponzer S, Gerdhem P (2016) Markers of inflammation and fibrinolysis in relation to outcome after surgery for lumbar disc herniation. A prospective study on 177 patients. Eur Spine J 1:186–191. https://doi.org/10.1007/s00586-015-3998-7
Zanoli G, Stromqvist B, Jonsson B (2001) Visual analog scales for interpretation of back and leg pain intensity in patients operated for degenerative lumbar spine disorders. Spine (Phila Pa 1976) 26:2375–2380
Fairbank JC, Pynsent PB (2000) The Oswestry Disability Index. Spine (Phila Pa 1976) 25:2940–2952 (discussion 2952)
Burstrom K, Johannesson M, Diderichsen F (2001) Swedish population health-related quality of life results using the EQ-5D. Qual Life Res 10:621–635
Sullivan M, Karlsson J, Ware JE Jr (1995) The Swedish SF-36 Health Survey–I. Evaluation of data quality, scaling assumptions, reliability and construct validity across general populations in Sweden. Soc Sci Med 41:1349–1358
Hagg O, Fritzell P, Oden A, Nordwall A (2002) Simplifying outcome measurement: evaluation of instruments for measuring outcome after fusion surgery for chronic low back pain. Spine (Phila Pa 1976) 27:1213–1222
Habibzadeh F, Habibzadeh P, Yadollahie M (2016) On determining the most appropriate test cut-off value: the case of tests with continuous results. Biochem Med 26:297–307. https://doi.org/10.11613/BM.2016.034
DeLong ER, DeLong DM, Clarke-Pearson DL (1988) Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 44:837–845
Tape TG (2017) Interpreting Diagnostic Tests; The area under a ROC curve. University of Nebraska Medical Center. http://gim.unmc.edu/dxtests/roc3.htm. Accessed 25 Feb
Hagg O, Fritzell P, Nordwall A (2003) The clinical importance of changes in outcome scores after treatment for chronic low back pain. Eur Spine J 12:12–20
Copay AG, Glassman SD, Subach BR, Berven S, Schuler TC, Carreon LY (2008) Minimum clinically important difference in lumbar spine surgery patients: a choice of methods using the Oswestry Disability Index, Medical Outcomes Study questionnaire Short Form 36, and pain scales. Spine J 8:968–974. https://doi.org/10.1016/j.spinee.2007.11.006
Asher AL, Kerezoudis P, Mummaneni PV, Bisson EF, Glassman SD, Foley KT, Slotkin J, Potts EA, Shaffrey ME, Shaffrey CI, Coric D, Knightly JJ, Park P, Fu KM, Devin CJ, Archer KR, Chotai S, Chan AK, Virk MS, Bydon M (2018) Defining the minimum clinically important difference for grade I degenerative lumbar spondylolisthesis: insights from the Quality Outcomes Database. Neurosurg Focus 44:E2. https://doi.org/10.3171/2017.10.focus17554
Vucetic N, Astrand P, Guntner P, Svensson O (1999) Diagnosis and prognosis in lumbar disc herniation. Clin Orthop Relat Res (361):116–122
Junge A, Dvorak J, Ahrens S (1995) Predictors of bad and good outcomes of lumbar disc surgery. A prospective clinical study with recommendations for screening to avoid bad outcomes. Spine (Phila Pa 1976) 20:460–468
van Hooff ML, Mannion AF, Staub LP, Ostelo RW, Fairbank JC (2016) Determination of the Oswestry Disability Index score equivalent to a “satisfactory symptom state” in patients undergoing surgery for degenerative disorders of the lumbar spine—a Spine Tango registry-based study. Spine J 16:1221–1230. https://doi.org/10.1016/j.spinee.2016.06.010
Spangfort EV (1972) The lumbar disc herniation. A computer-aided analysis of 2,504 operations. Acta Orthop Scand Suppl 142:1–95
van den Hout WB, Peul WC, Koes BW, Brand R, Kievit J, Thomeer RT (2008) Prolonged conservative care versus early surgery in patients with sciatica from lumbar disc herniation: cost utility analysis alongside a randomised controlled trial. BMJ 336:1351–1354. https://doi.org/10.1136/bmj.39583.709074.BE
Lechmann M, Peterson CK, Pfirrmann CW, Hodler J (2013) Lumbar nerve root injections: a prospective cohort outcomes study comparing age- and gender-matched patients who returned an outcomes-based postal questionnaire with patients who did not return the postal questionnaire. Skeletal Radiol 42:1429–1435. https://doi.org/10.1007/s00256-013-1673-9
Wihlborg A, Akesson K, Gerdhem P (2014) External validity of a population-based study on osteoporosis and fracture. Acta Orthop 85:433–437. https://doi.org/10.3109/17453674.2014.920987
Bisgard KM, Folsom AR, Hong CP, Sellers TA (1994) Mortality and cancer rates in nonrespondents to a prospective study of older women: 5-year follow-up. Am J Epidemiol 139:990–1000
Acknowledgements
We would like to acknowledge all the surgeons and patients that have contributed with data to this study, and Carina Blom at the Swespine registry for the assistance with data retrieval.
Funding
This study was financially supported by funds from the Regional Agreement on Medical Training and Clinical Research (ALF) between Stockholm County Council and Karolinska Institutet, Karolinska Institutet research funds, and the Swedish Society of Spinal Surgeons. The funding bodies had no influence on the analysis, interpretation or writing of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Peter Elkan, Tobias Lagerbäck, Hans Möller, and Paul Gerdhem declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Elkan, P., Lagerbäck, T., Möller, H. et al. Response rate does not affect patient-reported outcome after lumbar discectomy. Eur Spine J 27, 1538–1546 (2018). https://doi.org/10.1007/s00586-018-5541-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-018-5541-0