
Abstract
Objectives
To analyze the incidence and distribution of branch canals in mandibular anterior teeth.
Materials and methods
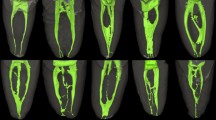
Three hundred mandibular anterior teeth, comprising 100 central incisors, 100 lateral incisors, and 100 canines, were scanned using a micro-computed tomography (micro-CT) system. Three-dimensional (3-D) visualization reconstruction of the root canal system and its branch canals was performed on each specimen. Data regarding the number of branch canals, the distance from the anatomical apex to the branch canal, and the orientation of each branch orifice were collected and analyzed.
Results
One hundred and fifty-three primary branch canals and 35 secondary branch canals were detected in the specimens overall. The incidence of branch canals in mandibular anterior teeth was 34%, with the highest incidence (50%) exhibited in mandibular canines, followed by lateral incisors (29%). Of the 153 primary branch canals found in the mandibular anterior tooth samples investigated, 82.35% appeared within 3 mm of the apical region, while 71.90% were labial and lingual canals.
Conclusions
There was regularity in the distribution and orientation of branch canals in mandibular anterior teeth.
Clinical relevance
This knowledge may be employed as a guide in clinical endodontic therapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
It is known that the root canal system is complex, exhibiting many anatomical variations, such as lateral canals, isthmuses, and intercanal communications [1]. Disintegration of the epithelial root sheath before dentin formation, or due to a lack of dentin formation, around a blood vessel may result in lateral canal and apical ramification formation [2]. These branch canals are present in dentin partitions formed by the physiological growth of dentin, or are present in the periradicular connective tissue, and hence influence the number and form of root canals [3]. Branch canals are often difficult to detect, poorly accessible to root canal instruments, irrigants, and medications, and may serve as tissue and bacterial reservoirs. They allow potential two-way communication between the main canal and the periodontal ligament (PDL), which might account for failure of nonsurgical or surgical therapy in some cases [2].
Knowledge of branch canal morphology and configuration is essential for successful endodontic therapy. The aim of this study was to analyze and detect the incidence and distribution of such branch canals in 300 mandibular anterior teeth by means of micro-computed tomography (micro-CT), using a three-dimensional (3-D) visualization and reconstruction technique, and to investigate the regularity of branch canals in the mandibular anterior region.
Materials and methods
Collection and preparation of samples
After approval from the Ethics Committee of School and Stomatology Wenzhou Medical University, 300 extracted mandibular anterior teeth, comprising 100 central incisors, 100 lateral incisors, and 100 canines, were randomly obtained from the dental outpatient clinic of the Hospital of Stomatology, Wenzhou Medical University. No information regarding the cause of extraction, age, or sex of the patients was available. We included extracted unrestored teeth that had intact crowns or where any carious defects present did not infringe on the pulp cavity. Teeth that had undergone endodontic treatment or had immature root formation were excluded.
After tooth extraction, the remaining soft tissue was removed using standard periodontal scalers; calculus was debrided with an ultrasonic scaler (SUPRASSOM P5; Satelec Co, Merignac, France). The teeth were then stored in 10% neutral-buffered formalin solution prior to further study.
Micro-CT scanning and 3-D visualization
The specimens were scanned from the crown to the apex, using a micro-CT system (mCT-80; Scanco Medical AG, Brüttisellen, Switzerland) with an isotropic voxel size of 30 μm. Raw data were then reconstructed into 3-D images using VGStudio MAX reconstruction software (Volume Graphics GmbH, Heidelberg, Germany). After image filtration and noise reduction, a region-growing algorithm, based on gray contrast, was used for selecting the edge of the root canal system. Volume rendering was performed for reconstruction of the tooth contour and for 3-D visualization of the root canal system.
Incidence of branch canals
In this study, canals branching from the main canal to the periodontal ligament were set as primary branch canals, while branches extending from these branch canals were regarded as secondary branch canals. From the 3-D visualization model of the branch canals and the cross-sectional image of the root canal, the number of branch canals in each sample was recorded, and the incidence of branch canals was calculated at various tooth locations.
Vertical distribution of branch canals
The method used for assessing the vertical distribution of branch canals is shown in Fig. 1. A cross-section of the anatomical apex was set as a starting plane, and each cross-section was calculated and marked at an average distance of 1 mm from the starting plane. The 3-D visualization model of each sample was analyzed and the start and stop points of the primary branch canals in cross-sectional images were recorded; from this record, the distance from the branch canal to the anatomical apex was determined.

Schematic diagram of the method used for investigating the vertical distribution of branch canals
Orientation and distribution of branch canals
Each branch canal orientation was classified according to criteria set forth by Yoshiuchi et al. [4]. In brief, the plane was divided into eight sections on an actual cross-section of a root containing a branch canal; the 12 o’clock position was assigned to the middle of the labial root surface, and 6 o’clock was assigned to the center of the lingual surfaces. The area between 11 and 1 o’clock was defined as labial (buccal) surfaces (B), that between 1 and 2 o’clock as the mesiolabial (BM or distolabial, BD), and that between 2 and 4 o’clock as the mesial (M, or distal D) regions. Branch orifice orientations were then determined according to these divisions (Fig. 2).

Schematic diagram of the method used to investigate the horizontal orientation of branch canals
Statistical analysis
Statistical analyses were performed using SPSS19.0. Differences between the vertical distributions of branch canals were assessed using the Kruskal−Wallis test, while the chi-square test was used to compare the root canal orientation and distribution among different teeth. Statistical significance was set at P < 0.05.
Results
Incidence of branch canals
Of the 300 mandibular anterior teeth, 102 (34%) had branch canals. The highest incidence of branch canals (50%) was seen in mandibular canines, followed by lateral incisors (29%). Of the mandibular anterior teeth with branch canals, 36.30% had no less than two primary branches, while 18.63% had at least one secondary branch canal. A total of 153 primary branch canals and 35 secondary branches were observed in all specimens. The incidence and number of branch canals in different anterior tooth locations are summarized in Table 1.
Vertical distribution of branch canals
As shown in Table 2, of the 153 primary branch root canals, about 82.35% were located in the apical 3 mm of the root. No significant differences in incidence of branch canals were observed in terms of the vertical distribution at different tooth locations (P > 0.05).
Horizontal orientation of branch canals
The orientation of branch canals at different tooth locations is shown in Table 3. Of the 153 branch canals, 71.90% were located on the labial and lingual aspects. The incidence was as high as 81.48% in mandibular central incisors, followed by 74.42 and 67.47% in mandibular lateral incisors and mandibular canines respectively. There were no significant differences in the orientation and distribution at different locations on the teeth (P > 0.05).
Discussion
In the present study, micro-CT was used to investigate branch canals in mandibular anterior teeth. Root canal systems in all specimens were reconstructed three-dimensionally for visualization, and the distance from 153 primary branch canals to the anatomical apex was also accurately measured. Cross-sections of each branch canal were analyzed to determine the orientation. This approach enhanced the ease and precision of evaluating the detailed morphology of the root canal system.
In the past, the dye-and-clearing technique, an inexpensive experimental procedure, which affords a 3-D view of the root canal system, and which allows processing large numbers of samples, has been used extensively in laboratory studies of the configurations of branch canals [5,6,7,8,9,10]. However, the accuracy of and results obtained with this technique are easily affected by a number of factors, including the staining stage, canal contents, and method of decalcification. This has led to significant variation in the reported incidence of branch canals in mandibular anterior teeth [7,8,9, 11]. In addition, it is difficult to measure the vertical distribution of branch canals accurately; thus, the whole root was roughly divided into three different locations: the coronal third, the middle third, and the apical third [12,13,14,15,16,17]. A hypothetical cross-section of the root was used in investigating the direction of branch canals, and the direction could only be determined relative to the orifice on the surface of the periodontal ligament [4, 18, 19]. Consequently, the dye-and-clearing technique presents inherent limitations to its usage.
Micro-CT was first used in the field of endodontics by Nielsen, in 1995 [20]. Since then, its use has gradually increased, and it has been employed to evaluate the configuration of the root canal system, given its high resolution, high-quality imaging capability, more accurate 3-D reconstruction, excellent repeatability of its results, and its usefulness for quantification. In 2006, Cheung et al. [21] investigated the incidence of branch canals and apical deltas in the apical 5 mm of mandibular second molars using visualization of 3-D models obtained using micro-CT. Verma et al. [22] and Somma et al. [23] both studied the mesiobuccal root canal morphology of maxillary first molars using micro-CT. Somma et al. [23] reported that the prevalence of accessory canals in the coronal, middle, and apical thirds of the mesiobuccal roots of maxillary first molars was 8.3, 50.0, and 91.6%, respectively. All of these results confirmed the accuracy and reliability of micro-CT as a method for studying the ultrastructure of entities such as branch canals. Nevertheless, the complexity of the equipment, the high cost, and the time required to perform micro-CT investigations have restricted the application of micro-CT to small sample sizes, making it unsuitable for analyzing the surface morphology of large numbers of samples.
Current data on the incidence of branch canals in the mandibular anterior teeth are sparse and diverse [17,18,19,20]. Apart from differences in race, study design, and sample size, the inconsistency in the definitions used has also influenced the final results reported in these studies. In the present study, branch canals were defined as canals, including lateral canals, which communicated with the periodontal ligament, as well as bifurcated structures (not including accessory root canals deriving from the pulp chamber). Branches deriving from the main root were defined as primary branch canals, while those extending from lateral canals were designated as secondary branch canals. This classification allows a more accurate evaluation of complicated root canal systems.
Nearly all previous studies have confirmed that the incidence of branch canals was highest in the apical third of roots [12,13,14,15,16,17]. Research on the vertical distribution of branch canals in mandibular anterior teeth appears to be rare, and to date, there have been no reports on the distribution and orientation of branch canals in mandibular anterior teeth. Miyashita et al. [19] investigated 1047 transparent specimens of root canals of extracted mandibular incisors. They found that 88.6% of branch canals were located in the apical third of the root. Al-Qudah et al. [24] and Kartal et al. [25] also reported that 64.3 and 78.3% of branch canals were located in the apical third of the roots of mandibular incisors. Our study demonstrated that 82.35% of branch canals are found within 3 mm of the root apex, with 91.5% of these canals found within 4 mm of the anatomical apex. These results were consistent with previous findings. In order to remove as much of the tissue, bacteria, and debris harbored within branch canals in the apical region as possible, several devices and disinfection techniques have been developed. Tulus et al. [26] recommended the use of a dental microscope, NaOCl irrigant combined with ultrasonic activation, pre-bent preparation instruments, specially designed handpieces, and thermoplastic obturation technique to perform therapy of branched root canal systems. De Gregorio et al. [27] evaluated different irrigation activation systems and found that passive ultrasonic irrigation facilitated better penetration of irrigant into the lateral canals, whereas apical negative pressure irrigation facilitated efficient irrigation of the root canal system up to the working length.
As the demand to save and maintain natural teeth has increased, more endodontic procedures are being performed, with a consequent increased risk for failure of root canal therapy or retreatment, and periradicular endodontic surgery. The success rate of endodontic surgery in the literature ranges from 59.1 to 96.8% [28, 29]. Most failures were due to inadequate root canal sealing. Access, visibility, and instrumentation are easier in anterior tooth sextants. Thus, endodontic surgery involving anterior teeth will be the preferred choice for endodontists and general practitioners. Most scholars have suggested that optimal resection of apical root tissue should be within 2–3 mm [30,31,32]. Kim et al. [33] found that, when the root resection level approached 3 mm, it resulted in elimination of 93% of branch canals, thus facilitating improved canal obturation, and apical sealing. Degerness et al. [34] conducted research on the mesiobuccal roots of maxillary molars and found that 80% of branch canals were located within 3.64 mm of the anatomical apex; they therefore recommended a minimum mesiobuccal root resection level for maxillary molars of 3.6 mm. The results of our experimental study showed that, when root resection was performed at 3 mm, 82.35% of branch canals were removed in mandibular anterior teeth, while resection at 4 mm yielded a 91.5% rate of branch canal removal. Therefore, after completing a root resection procedure, some branch canals remained in the tooth, and a surgical microscope plus auxiliary equipment, combined with methylene blue staining, was necessary to aid investigation of resected roots [29].
Additionally, our results showed that 71.90% of branch canals were located on the labial and lingual aspects of mandibular anterior teeth. That may be because the root canals of mandibular anterior teeth are usually broad buccolingually. The deposition of secondary dentine in ribbon-shaped canals results in the formation of partitions, which may cause extensive differentiation in root canals, finally forming branch canals [35]. Based on the findings of our research, we recommend that, when performing surgical endodontic therapy for mandibular anterior teeth, greater emphasis should be placed on locating branch canals on the labial and lingual aspects of these teeth. Furthermore, no significant difference was found among the mandibular anterior teeth in terms of the incidence of branch canals, in either vertical or horizontal orientation. Therefore, equal emphasis should be placed on the branch canals among the three mandibular anterior teeth. This will help to reduce the number of missed branch canals and improve complete root canal obturation and apical sealing.
References
Hess W (1921) Formation of root canals in human teeth. J Am Dent Assoc 3:704–734
Ricucci D, Siqueira JF (2010) Fate of the tissue in lateral canals and apical ramifications in response to pathologic conditions and treatment procedures. J Endod 36:1–15
Yu SF (2007) Oral histopathology, 6th edn. People Medical Publishing House, p 37
Yoshiuchi Y, Takahashi K, Yokochi C (1972) Studies on the anatomical forms of the pulp cavities with new method of vacuum injection (II)—accessory canal and apical ramification. Jpn J Oral Biol 14:156–185
Adorno CG, Yoshioka T, Suda H (2010) Incidence of accessory canals in Japanese anterior maxillary teeth following root canal filling ex vivo. Int Endod J 43:370–376
De Deus Q, Horizonte B (1975) Frequency, location, and direction of the lateral, secondary, and accessory canals. J Endod 1:361–366
Vertucci FJ (1984) Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 58:589–599
Çalişkan MK, Pehlivan Y, Sepetçioğlu F, Türkün M, Tuncer SS (1995) Root canal morphology of human permanent teeth in a Turkish population. J Endod 21:200–204
Sert S, Bayirli GS (2004) Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod 30:391–398
Weng XL, Yu SB, Zhao SL, Wang HG, Mu T, Tang RY, Zhou XD (2009) Root canal morphology of permanent maxillary teeth in the Han nationality in Chinese Guanzhong area: a new modified root canal staining technique. J Endod 35:651–656
Venturi M, Di Lenarda R, Prati C, Breschi L (2005) An in vitro model to investigate filling of lateral canals. J Endod 31:877–881
Ng YL, Aung TH, Alavi A, Gulabivala K (2001) Root and canal morphology of Burmese maxillary molars. Int Endod J 34:620–630
Alavi AM, Opasanon A, Ng YL, Gulabivala K (2002) Root and canal morphology of Thai maxillary molars. Int Endod J 35:478–485
Peiris R, Takahashi M, Sasaki K, Kanazawa E (2007) Root and canal morphology of permanent mandibular molars in a Sri Lankan population. Odontology 95:16–23
Gulabivala K, Aung T, Alavi A, Ng YL (2001) Root and canal morphology of Burmese mandibular molars. Int Endod J 34:359–370
Gulabivala K, Opasanon A, Ng YL, Alavi A (2002) Root and canal morphology of Thai mandibular molars. Int Endod J 35:56–62
Peiris H, Pitakotuwage T, Takahashi M, Sasaki K, Kanazawa E (2008) Root canal morphology of mandibular permanent molars at different ages. Int Endod J 41:828–835
Kas ahara E, Yasuda E, Yamamoto A, Anzai M (1990) Root canal system of the maxillary central incisor. J Endod 16:158–161
Miyashita M, Kasahara E, Yasuda E, Yamamoto A, Sekizawa T (1997) Root canal system of the mandibular incisor. J Endod 23:479–484
Nielsen RB, Alyassin AM, Peters DD, Carnes DL, Lancaster J (1995) Microcomputed tomography: an advanced system for detailed endodontic research. J Endod 21:561–568
Cheung GSP, Yang J, Fan B (2007) Morphometric study of the apical anatomy of C-shaped root canal systems in mandibular second molars. Int Endod J 40:239–246
Verma P, Love RM (2011) A micro CT study of the mesiobuccal root canal morphology of the maxillary first molar tooth. Int Endod J 44(3):210–217
Somma F, Leoni D, Plotino G, Grande NM, Plasschaert A (2009) Root canal morphology of the mesiobuccal root of maxillary first molars: a micro-computed tomographic analysis. Int Endod J 42:165–174
Al-Qudah A, Awawdeh L (2006) Root canal morphology of mandibular incisors in a Jordanian population. Int Endod J 39:873–877
Kartal N, Yanıkoğlu FÇ (1992) Root canal morphology of mandibular incisors. J Endod 18:562–564
Tulus G, Weber T, Petrovits A (2015) Diagnosis and therapy of branched root canal systems. ENDO 9:267–282
De Gregorio C, Estevez R, Cisneros R, Paranjpe A, Cohenca N (2010) Efficacy of different irrigation and activation systems on the penetration of sodium hypochlorite into simulated lateral canals and up to working length: an in vitro study. J Endod 36:1216–1221
Chércoles-Ruiz A, Sánchez-Torres A, Gay-Escoda C (2017) Endodontics, endodontic retreatment, and apical surgery versus tooth extraction and implant placement: a systematic review. J Endod 43:679–686
Floratos S, Kim S (2017) Modern endodontic microsurgery concepts: a clinical update. Dent Clin North Am 61:81–91
Pomeranz HH, Fishelberg G (1974) The secondary mesiobuccal canal of maxillary molars. J Am Dental Assoc 88:119–124
Kim S (2001) Color atlas of microsurgery in endodontics. WB Saunders Co., Philadelphia
Ingle JI (1994) Ingle’s endodontics. 4th ed. Pmph USA Ltd., pp. 689–763
Kim S, Pecora G, Rubenstein R (2001) Osteotomy and apical root resection. Color atlas of microsurgery in endodontics. WB Saunders, Philadelphia, pp 85–94
Degerness R, Bowles W (2008) Anatomic determination of the mesiobuccal root resection level in maxillary molars. J Endod 34:1182–1186
Hess W (1925) The anatomy of the root canals of the teeth of the permanent dentitions, 1st edn. John Bale, Sons & Danielsson Ltd, London
Funding
This study was supported by the Technology Innovation Plan for College Students in Zhejiang Province (Xinmiao Talents Program) (No. 2015R413085) and Wenzhou Science and Technology Planning Project (No. Y20140330).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Ethics Committee of School and Stomatology Wenzhou Medical University and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
For this type of study, formal consent is not required.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Wang, M., Ren, X. & Pan, Y. Micro-computed tomography-based anatomical study of the branch canals in mandibular anterior teeth in a Chinese population. Clin Oral Invest 23, 81–86 (2019). https://doi.org/10.1007/s00784-018-2409-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-018-2409-y