
Abstract
Immunoglobulin A vasculitis (IgAV) is an immune complex, small vessel vasculitis with dominant IgA deposits in vessel walls, predominantly affecting the pediatric population. However, adults frequently have more severe gastrointestinal tract (GIT) and renal involvements as compared to children. Our aim was to study serological and cellular biomarkers to support clinicians in their diagnosis and the course of IgAV in adult patients. This cross-sectional study included 62 adult IgAV patients and 53 healthy blood donors (HBDs). Demographic and clinical data, as well as routine laboratory tests, were meticulously analyzed. Serum levels of IL-1β, IL-2, IL-6, IL-8, IL-9, IL-10, IL-17A, IL-23, TNF-α and serum amyloid A (SAA) were measured. Percentages of neutrophils, lymphocytes, and monocytes with neutrophil expression of L-selectin and integrin αM were determined by flow cytometry. SAA (12-fold), IL-6 (3-fold), IL-8 (2-fold), and TNF-α (2-fold) were significantly elevated in sera of adult IgAV patients compared to HBDs. There was a 16% elevation in neutrophils in IgAV patients, with IgAV neutrophils showing significantly higher CD62L surface expression. IgAV patients with GIT involvement exhibited elevated numbers of leukocytes, neutrophils, and neutrophil/lymphocyte (NLR), but lower neutrophil CD11b expression, as compared to IgAV patients without GIT. IgAV patients exhibit a low–medium grade inflammatory, neutrophil-driven response. Patients with GIT can be distinguished by their elevated NLR.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Immunoglobulin A vasculitis (IgAV) is a small-vessel, immune complex leukocytoclastic vasculitis, characterized by dominant IgA deposits in vascular walls [1]. It represents the most common primary vasculitis in the pediatric population [2, 3]; however, it is also frequent in adults, as recently shown [4].
Clinical signs and symptoms of the disease include cutaneous purpura, joint, gastrointestinal tract (GIT), and renal involvement; however, they differ greatly depending on the age of the patients [5, 6]. Adults develop systemic involvement more frequently compared to children, with greater risk of severe bowel ischemia and chronic renal failure [7,8,9,10,11].
There are currently no diagnostic criteria for IgAV. The updated classification criteria for pediatric IgAV (EULAR/PRINTO/PRES classification criteria) [12], performed well also in adult IgAV [13]. Yet, the final diagnosis leans on histological characterization of IgAV [1, 14]. However, not all the expected significant changes are present in biopsy tissue, neither is IgA deposition pathognomonic for IgAV [14]. In approximately 10–20% of patients, GIT or joint symptoms may occur before the onset of skin purpura and setting an appropriate diagnosis of IgAV is difficult, when there is an atypical presentation [14, 15].
It would be advantageous to find a serological biomarker or group of analytes, which could support clinicians in their diagnosis in such cases. Moreover, there is a need of prognostic markers that would predict patients who are at risk of developing severe GIT and renal involvement, as well as complications during disease progression in order to facilitate appropriate therapeutic management of these patients [14].
The aims of this study were to evaluate serum levels of cytokines and acute phase proteins as well as determine the distribution of neutrophils, lymphocytes, and monocytes, together with neutrophil surface expression of L-selectin (CD62L) and integrin αM (CD11b), among adult IgAV patients.
Materials and methods
Human subjects
We included 62 adult, treatment-naïve IgAV patients, with histologically proven disease [12, 13]. For comparison, sera samples of 53 and peripheral blood of 15 healthy blood donors (HBDs) were obtained. All samples were fully anonymized, before we assessed them, and all subjects signed informed consent. The study was approved by the Slovene National Medical Ethics Committee (#99/04/15 and #65/01/17).
Data collection
The medical records from IgAV patients were analyzed and the following was recorded: age, gender, body mass index, smoking status, duration of clinical symptoms, and signs before sampling, concurrent infections, past malignancy, clinical signs and symptoms, Birmingham vasculitis activity score (BVAS), and results of routine laboratory testing.
Laboratory parameters
Erythrocyte sedimentation rate and concentration of C-reactive protein, complete blood count with differential, basic biochemistry panels including electrolytes, creatinine, urea, serum protein electrophoresis, serum immunoglobulin (Ig) A, M, G levels, and urine analysis were determined.
Cytokine and serum amyloid A measurement
Concentrations of IL-1β, IL-2, IL-8, IL-9, IL-10, IL-17A, IL-23, and TNF-α were measured in sera of IgAV patients and HBDs by AtheNa Multi-Lyte (Luminex xMAP Technology) using human pre-mixed multi-analyte kits (R&D Systems). IL-6 sera proteins levels were measured by ELISA (Invitrogen). The concentrations of serum amyloid A (SAA) were determined using immunonephelometry (BN Prospec System, Siemens). All sera samples were collected following blood clotting and centrifugation at 3000×g for 5 min, aliquoted, and stored at −20 °C until ready for further analysis.
Flow cytometry
Venous blood was drawn from IgAV patients and HBDs and collected into heparin-containing tubes. Whole blood immunophenotyping was performed using 7-Color Immunphenotyping kit (Miltenyi Biotec). Briefly, 100 μl of whole blood was incubated with 10 μl immunophenotyping reagent for 10 min in the dark, at 4 °C. After incubation, erythrocytes were lysed using Red Blood Lysing Solution (Miltenyi Biotec). Neutrophil phenotyping was performed in 50 μl of whole blood, incubated for 30 min at 4 °C in the dark with mouse anti-human antibodies to CD16 (conjugated to PE, clone eBioCB16, eBioscience), CD62L (conjugated to PE-Cyanine 5, clone DREG56, eBioscience), and CD11b (conjugated to APC, clone ICRF44, eBioscience). After incubation, samples were lysed, using Whole Blood Lysing Reagent Kit (Beckman Coulter). All samples were analyzed using flow cytometer MACSQuant Analyzer 10 (Miltenyi Biotec). Analysis of flow cytometry data was performed using MACSQquantify (Analysis Software version 2.8) and FlowLogic (Flow Cytometry Analysis Package, version 700.0a).
Statistical analysis
The normality of distribution was determined by Shapiro–Wilk test. Due to non-normal distribution of the data, summary statistics were expressed as medians and 25–75th percentiles (Q25–Q75), and nonparametric tests were performed. Mann–Whitney U test was used to compare continuous variables between IgAV patients and HBDs, or between IgAV patients with/without different clinical symptoms and signs. Spearman’s rank correlation was calculated to measure the correlation between parameters. All statistical analysis was performed using SPSS statistical software package version 22.0 and Graph Pad Prism software 5.03. All tests were two-tailed and p values of < 0.05 were regarded as statistically significant.
Results
Characteristics of IgAV patients
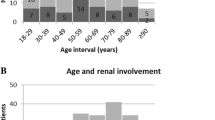
Sixty-two IgAV patients (52% males) with median (Q25–Q75) age of 56.0 (38.9–74.8) years were recruited in the study. Patients were included after a median (Q25–Q75) duration of symptoms of 10 (5–19) days. All patients presented with skin purpura (necrotic 45%, generalized 56%). Joint, GIT, and renal involvement were present in 40%, 39%, and 35%, respectively (Table 1).
Routine laboratory findings
Results of routine laboratory tests are present in Table 1. Sera levels of IgA were elevated in 29/62 (47%) of patients above 4 g/l.
Inflammatory cytokine profile
Levels of SAA (12-fold), an acute phase protein with cytokine-like properties, IL-6 (3-fold), IL-8 (2-fold), and TNF-α (2-fold) were statistically significantly elevated in sera of IgAV patients compared to HBDs (Table 2). IL-1β, IL-9, IL-10, and IL-23 were found to be unchanged in IgAV patients compared to HBDs (Table 2) and concentrations of IL-2 and IL-17A could not be determined due to their levels below the limits of detection of this assay.
Inflammatory cell profile and neutrophil phenotype
In peripheral blood of IgAV patients, there was a higher percentage of CD16+ neutrophils (p < 0.001) and lower percentages of CD3+ (p < 0.001), including CD4+ (p = 0.003) and CD8+ (p = 0.002) T-lymphocytes and CD20+ B-lymphocytes (p = 0.006), as compared to HBDs (Figs. 1 and 2; Supplemental Table 1). IgAV neutrophils showed significantly higher L-selectin (CD62L) surface expression with a median (Q25–Q75) of 86.5 (45.4–107.5) vs. 55.5 (44.3–64.9) p = 0.008 in HBDs (Fig. 2; Supplemental Table 1).

Cellular immunophenotyping in HBD (a) and IgAV patients (b) Median percentages are presented of neutrophils, T-lymphocytes, B-lymphocytes, NK cells, and monocytes in HBD (n = 15) and IgAV patients (n = 15); HBD, healthy blood donors; IgAV, immunoglobulin A vasculitis; NK, natural killer

Cell profiles and neutrophil surface protein expression in adult IgAV patients as compared to HBD. Medians with Q25–Q75 are shown for percentages of T-lymphocytes, CD4+ T-lymphocytes, CD8+ T-lymphocytes, B-lymphocytes, NK cells, monocytes, neutrophils, and median fluorescence intensity of CD62L and CD11b expression on CD16+ neutrophils. Numbers of IgAV patients and HBD are indicated in brackets; **p < 0.01; ***p < 0.001. IgAV, patients with immunoglobulin A vasculitis; HBD, healthy blood donors; NK, natural killer cells; MFI, median fluorescence intensity
IgAV patients with GIT involvement showed a significantly higher number of leukocytes (p < 0.0001), neutrophils (p = 0.001), and calculated neutrophil to lymphocyte ratio (NLR) (p = 0.02), while showing lower neutrophil CD11b expression (p = 0.005), as compared to IgAV patients without GIT involvement (Fig. 3; Supplemental Table 2).

Number of leukocytes, neutrophils, NLR, and CD11b neutrophil expression in IgAV patients with GIT involvement as compared to patients without GIT involvement. Medians with Q25–Q75 are shown for number of leukocytes a, neutrophils b, ratio between # of neutrophils and lymphocytes c, and median fluorescence intensity for CD11b expression on CD16+ neutrophils d. Numbers of included IgAV patients are indicated in brackets. *p < 0.05; **p < 0.01; ***p < 0.001. GIT, gastrointestinal tract; IgAV, patients with immunoglobulin A vasculitis; NLR, neutrophil to lymphocyte ratio; MFI, median fluorescence intensity
NLR positively correlated with SAA levels (r = 0.603, 95% CI = 0.410–0.744, p < 0.0001) and neutrophil CD11b expression showed good positive correlation with sera levels of IgA (r = 0.514, 95% CI = 0.177–0.743, p < 0.01) (Fig. 4).

Correlation between NLR and SAA concentration (a) and neutrophil CD11b expression and IgA levels (b) in IgAV patients. Shown are Spearman correlation coefficient (r), 95% confidence interval, p value, and numbers of included patients. CI, confidence interval; IgA, patients with immunoglobulin A vasculitis; NLR, neutrophil to lymphocyte ratio; MFI, median fluorescence intensity; SAA; serum amyloid A
Discussion
IgAV was thought to be mainly the disease of children; however, it can frequently occur in adults [4] whose disease course is usually more severe as compared to children [16]. Age, gender, and extent of purpura seem to forecast outcomes of IgA vasculitis in adults [17], but prompt diagnosis and identification of patients at risk, are a considerable challenge for clinicians, with no clinically useful laboratory biomarkers available to date [14].
Serological reports in IgAV have indicated dysregulated inflammatory cytokine production and elevated acute phase proteins. Namely, increased levels of systemic SAA (36-fold) were previously found in IgAV pediatric patients [18, 19] and associated with GIT manifestations [18]. The current report exposes significantly elevated levels of SAA (12-fold) in the sera of adult IgAV patients, indicating a low–medium inflammatory response.
While Th1-, as well as Th2-related cytokines, have been extensively studied in pediatric IgAV patients [19,20,21,22,23], data available on the adult population are scarce. Berthelot et al. recently found higher concentrations of IL-1β, IL-6, and IL-8 in the sera of adult IgAV patients, whereas levels of IL-10, IL-12p70, and TNF-α were similar between patients and control group [24]. Similarly, another study also reported on higher levels of IL-6 and IL-8 in IgAV patients, which were associated with GIT and renal involvement, respectively [25]. In the current study, we observed increased levels of pro-inflammatory cytokines IL-6, IL-8, and TNF-α in the sera of adult IgAV compared to HBDs; however, there was no association with clinical signs and symptoms.
Together with elevated sera concentrations of IgA and higher percentages of neutrophils, our results support the theory of the central role of IgA, endothelial cells, and neutrophils in IgAV pathogenesis, as recently reviewed in Heineke et al. [26]. Although, the origin and specific antigen targets of IgA remain unknown, these antibodies were found to bind antigens on the surface of endothelial cells [27], such as β2-glycoprotein I [21] and phosphatidylserine [25]. IgA binding to endothelial cells, together with the systemic inflammatory environment (with elevated IL-6 and SAA) promote endothelial activation and production of IL-8 [28, 29], a major chemoattractant for neutrophils leading to their recruitment and activation [26]. Indeed, SAA has been shown to induce paracrine IL-8 via Toll-like receptor 2, synergizing to recruit neutrophils [30]. In addition, increased levels of TNF-α in the sera of IgAV patients could further accelerate inflammation, as this cytokine can enhance binding of antibodies to endothelial cells and further induce IL-8 release [21, 29]. Moreover, IgA bound to Fc receptors (FcαRI) on neutrophils, leads to antibody-dependent cell-mediated cytotoxicity (ADCC) and production of reactive oxygen species. Thus, the cross-talk between IgA, endothelial cells, and neutrophils, even in a low inflammatory environment, can lead to substantial vascular damage [26].
We also found elevated expression of L-selectin (CD62L), an adhesion molecule expressed on neutrophils, that could be involved in early pathological events of IgAV, since it is important for the initial adhesion of neutrophils to vascular surfaces [31]. Indeed, a prominent role for neutrophils, with an escaped proinflammatory phenotype was previously proposed for another systemic vasculitis [32], with both neutrophil markers CD62L and CD11b indicating progression of the disease.
Interestingly, in our study, CD11b expression was elevated in IgAV and showed good positive correlation with IgA levels. CD11b (in complex with CD18 is named Mac-1) represents a predominant β2 integrin expressed on neutrophils. Mac-1 is not only important for firm adhesion of neutrophils to endothelial cells [33], but also plays a role in ADCC by interacting with Fc receptors on neutrophils [34]. This could indicate an independent pathogenic mechanism in IgAV, since increased levels of IgA and CD11b expression could lead to enhanced ADCC and vascular damage. On the other hand, the current report also shows a negative association of neutrophil CD11b expression with GIT involvement. Migration of neutrophils across cellular barriers, such as vascular endothelium and epithelium occurs due to the effects of chemoattractants and cell-adhesion molecule interactions; however it seems, through different mechanisms. Specifically, neutrophils can also migrate across the intestinal epithelium using a CD11b/CD18-independent mechanism [35], as suggested through the CD47 interaction with the signal regulatory protein α [36, 37]. It is therefore possible that neutrophils use different adhesion molecules to enter the site of inflammation in GIT of patients with IgAV, requiring a neutrophil phenotype distinct from the one observed in patients with skin limited involvement.
Conclusion
Taken together, and to the best of our knowledge, this is the first study to date to determine both, serological and cellular markers in histologically-proven adult treatment-naïve IgAV. We confirmed the association of the NLR with GIT involvement [38,39,40,41] that could be a viable marker in the future. Neutrophils and their surface molecules (CD62L and CD11b), in the presence of low–medium grade inflammation, may all contribute to the vicious cycle of IgAV pathogenesis.
References
Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, Flores-Suarez LF, Gross WL, Guillevin L, Hagen EC, Hoffman GS, Jayne DR, Kallenberg CG, Lamprecht P, Langford CA, Luqmani RA, Mahr AD, Matteson EL, Merkel PA, Ozen S, Pusey CD, Rasmussen N, Rees AJ, Scott DG, Specks U, Stone JH, Takahashi K, Watts RA (2013) 2012 revised international chapel hill consensus conference nomenclature of vasculitides. Arthritis Rheum 65(1):1–11. https://doi.org/10.1002/art.37715
Penny K, Fleming M, Kazmierczak D, Thomas A (2010) An epidemiological study of Henoch–Schonlein purpura. Paediatr Nurs 22(10):30–35. https://doi.org/10.7748/paed2010.12.22.10.30.c8135
Piram M, Mahr A (2013) Epidemiology of immunoglobulin A vasculitis (Henoch–Schonlein): current state of knowledge. Curr Opin Rheumatol 25(2):171–178. https://doi.org/10.1097/BOR.0b013e32835d8e2a
Hocevar A, Rotar Z, Ostrovrsnik J, Jurcic V, Vizjak A, Dolenc Voljc M, Lindic J, Tomsic M (2014) Incidence of IgA vasculitis in the adult Slovenian population. Br J Dermatol 171(3):524–527. https://doi.org/10.1111/bjd.12946
Pillebout E, Thervet E, Hill G, Alberti C, Vanhille P, Nochy D (2002) Henoch–Schonlein purpura in adults: outcome and prognostic factors. J Am Soc Nephrol 13(5):1271–1278
Calvo-Rio V, Loricera J, Mata C, Martin L, Ortiz-Sanjuan F, Alvarez L, Gonzalez-Vela MC, Gonzalez-Lamuno D, Rueda-Gotor J, Fernandez-Llaca H, Gonzalez-Lopez MA, Armesto S, Peiro E, Arias M, Gonzalez-Gay MA, Blanco R (2014) Henoch–Schonlein purpura in northern Spain: clinical spectrum of the disease in 417 patients from a single center. Medicine 93(2):106–113. https://doi.org/10.1097/MD.0000000000000019
Garcia-Porrua C, Calvino MC, Llorca J, Couselo JM, Gonzalez-Gay MA (2002) Henoch–Schonlein purpura in children and adults: clinical differences in a defined population. Semin Arthritis Rheum 32(3):149–156. https://doi.org/10.1053/sarh.2002.33980
Lu S, Liu D, Xiao J, Yuan W, Wang X, Zhang X, Zhang J, Liu Z, Zhao Z (2015) Comparison between adults and children with Henoch–Schonlein purpura nephritis. Pediatr Nephrol 30(5):791–796. https://doi.org/10.1007/s00467-014-3016-z
Kang Y, Park JS, Ha YJ, Kang MI, Park HJ, Lee SW, Lee SK, Park YB (2014) Differences in clinical manifestations and outcomes between adult and child patients with Henoch–Schonlein purpura. J Korean Med Sci 29(2):198–203. https://doi.org/10.3346/jkms.2014.29.2.198
Audemard-Verger A, Pillebout E, Guillevin L, Thervet E, Terrier B (2015) IgA vasculitis (Henoch–Shonlein purpura) in adults: diagnostic and therapeutic aspects. Autoimmun Rev 14(7):579–585. https://doi.org/10.1016/j.autrev.2015.02.003
Audemard-Verger A, Terrier B, Dechartres A, Chanal J, Amoura Z, Le Gouellec N, Cacoub P, Jourde-Chiche N, Urbanski G, Augusto JF, Moulis G, Raffray L, Deroux A, Hummel A, Lioger B, Catroux M, Faguer S, Goutte J, Martis N, Maurier F, Riviere E, Sanges S, Baldolli A, Costedoat-Chalumeau N, Roriz M, Puechal X, Andre M, Lavigne C, Bienvenu B, Mekinian A, Zagdoun E, Girard C, Berezne A, Guillevin L, Thervet E, Pillebout E (2017) Characteristics and management of IgA vasculitis (Henoch–Schonlein) in adults: data from 260 patients included in a French multicenter retrospective survey. Arthritis Rheumatol 69(9):1862–1870. https://doi.org/10.1002/art.40178
Ozen S, Pistorio A, Iusan SM, Bakkaloglu A, Herlin T, Brik R, Buoncompagni A, Lazar C, Bilge I, Uziel Y, Rigante D, Cantarini L, Hilario MO, Silva CA, Alegria M, Norambuena X, Belot A, Berkun Y, Estrella AI, Olivieri AN, Alpigiani MG, Rumba I, Sztajnbok F, Tambic-Bukovac L, Breda L, Al-Mayouf S, Mihaylova D, Chasnyk V, Sengler C, Klein-Gitelman M, Djeddi D, Nuno L, Pruunsild C, Brunner J, Kondi A, Pagava K, Pederzoli S, Martini A, Ruperto N (2010) EULAR/PRINTO/PRES criteria for Henoch–Schonlein purpura, childhood polyarteritis nodosa, childhood Wegener granulomatosis and childhood Takayasu arteritis: Ankara 2008. Part II: final classification criteria. Ann Rheum Dis 69(5):798–806. https://doi.org/10.1136/ard.2009.116657
Hocevar A, Rotar Z, Jurcic V, Pizem J, Cucnik S, Vizjak A, van den Broeke R, Tomsic M (2016) IgA vasculitis in adults: the performance of the EULAR/PRINTO/PRES classification criteria in adults. Arthritis Res Ther 18:58. https://doi.org/10.1186/s13075-016-0959-4
Hetland LE, Susrud KS, Lindahl KH, Bygum A (2017) Henoch–Schonlein purpura: a literature review. Acta Derm Venereol 97(10):1160–1166. https://doi.org/10.2340/00015555-2733
Hong J, Yang HR (2015) Laboratory markers indicating gastrointestinal involvement of Henoch-Schonlein purpura in children. Pediatr Gastroenterol Hepatol Nutr 18(1):39–47. https://doi.org/10.5223/pghn.2015.18.1.39
Hung SP, Yang YH, Lin YT, Wang LC, Lee JH, Chiang BL (2009) Clinical manifestations and outcomes of Henoch-Schonlein purpura: comparison between adults and children. Pediatr Neonatol 50(4):162–168. https://doi.org/10.1016/S1875-9572(09)60056-5
Hocevar A, Rotar Z, Jurcic V, Cucnik S, Tomsic M (2015) Patient age, gender and extent of purpura may suggest short-term outcomes in adults with IgA vasculitis. Rheumatology (Oxford) 54(7):1330–1332. https://doi.org/10.1093/rheumatology/kev122
He X, Zhao Y, Li Y, Kang S, Ding Y, Luan J, Zhao P, Liu N, Yin W (2012) Serum amyloid a levels associated with gastrointestinal manifestations in Henoch-Schonlein purpura. Inflammation 35(4):1251–1255
Purevdorj N, Mu Y, Gu Y, Zheng F, Wang R, Yu J, Sun X (2018) Clinical significance of the serum biomarker index detection in children with Henoch-Schonlein purpura. Clin Biochem 52:167–170. https://doi.org/10.1016/j.clinbiochem.2017.11.006
Besbas N, Saatci U, Ruacan S, Ozen S, Sungur A, Bakkaloglu A, Elnahas AM (1997) The role of cytokines in Henoch Schonlein purpura. Scand J Rheumatol 26(6):456–460
Yang YH, Chang CJ, Chuang YH, Hsu HY, Yu HH, Lee JH, Wang LC, Lin YT, Chiang BL (2012) Identification and characterization of IgA antibodies against beta2-glycoprotein I in childhood Henoch-Schonlein purpura. Br J Dermatol 167(4):874–881. https://doi.org/10.1111/j.1365-2133.2012.11068.x
Pan YX, Ye Q, Shao WX, Shang SQ, Mao JH, Zhang T, Shen HQ, Zhao N (2014) Relationship between immune parameters and organ involvement in children with Henoch-Schonlein purpura. PLoS One 9(12):e115261. https://doi.org/10.1371/journal.pone.0115261
Pillebout E, Jamin A, Ayari H, Housset P, Pierre M, Sauvaget V, Viglietti D, Deschenes G, Monteiro RC, Berthelot L (2017) Biomarkers of IgA vasculitis nephritis in children. PLoS One 12(11):e0188718. https://doi.org/10.1371/journal.pone.0188718
Berthelot L, Jamin A, Viglietti D, Chemouny JM, Ayari H, Pierre M, Housset P, Sauvaget V, Hurtado-Nedelec M, Vrtovsnik F, Daugas E, Monteiro RC, Pillebout E (2017) Value of biomarkers for predicting immunoglobulin a vasculitis nephritis outcome in an adult prospective cohort. Nephrol Dial Transplant. https://doi.org/10.1093/ndt/gfx300
Kimura S, Takeuchi S, Soma Y, Kawakami T (2013) Raised serum levels of interleukins 6 and 8 and antiphospholipid antibodies in an adult patient with Henoch-Schonlein purpura. Clin Exp Dermatol 38(7):730–736. https://doi.org/10.1111/ced.12089
Heineke MH, Ballering AV, Jamin A, Ben Mkaddem S, Monteiro RC, Van Egmond M (2017) New insights in the pathogenesis of immunoglobulin a vasculitis (Henoch-Schonlein purpura). Autoimmun Rev 16(12):1246–1253. https://doi.org/10.1016/j.autrev.2017.10.009
Yang YH, Wang SJ, Chuang YH, Lin YT, Chiang BL (2002) The level of IgA antibodies to human umbilical vein endothelial cells can be enhanced by TNF-alpha treatment in children with Henoch-Schonlein purpura. Clin Exp Immunol 130(2):352–357
Yang YH, Lai HJ, Huang CM, Wang LC, Lin YT, Chiang BL (2004) Sera from children with active Henoch-Schonlein purpura can enhance the production of interleukin 8 by human umbilical venous endothelial cells. Ann Rheum Dis 63(11):1511–1513. https://doi.org/10.1136/ard.2003.016196
Yang YH, Huang YH, Lin YL, Wang LC, Chuang YH, Yu HH, Lin YT, Chiang BL (2006) Circulating IgA from acute stage of childhood Henoch-Schonlein purpura can enhance endothelial interleukin (IL)-8 production through MEK/ERK signalling pathway. Clin Exp Immunol 144(2):247–253. https://doi.org/10.1111/j.1365-2249.2006.03076.x
De Buck M, Berghmans N, Portner N, Vanbrabant L, Cockx M, Struyf S, Opdenakker G, Proost P, Van Damme J, Gouwy M (2015) Serum amyloid A1alpha induces paracrine IL-8/CXCL8 via TLR2 and directly synergizes with this chemokine via CXCR2 and formyl peptide receptor 2 to recruit neutrophils. J Leukoc Biol 98(6):1049–1060. https://doi.org/10.1189/jlb.3A0315-085R
Liu Z, Yago T, Zhang N, Panicker SR, Wang Y, Yao L, Mehta-D'souza P, Xia L, Zhu C, McEver RP (2017) L-selectin mechanochemistry restricts neutrophil priming in vivo. Nat Commun 8:15196. https://doi.org/10.1038/ncomms15196
Nadkarni S, Dalli J, Hollywood J, Mason JC, Dasgupta B, Perretti M (2014) Investigational analysis reveals a potential role for neutrophils in giant-cell arteritis disease progression. Circ Res 114(2):242–248. https://doi.org/10.1161/CIRCRESAHA.114.301374
Anderson SI, Hotchin NA, Nash GB (2000) Role of the cytoskeleton in rapid activation of CD11b/CD18 function and its subsequent downregulation in neutrophils. J Cell Sci 113(Pt 15):2737–2745
van Spriel AB, Leusen JH, van Egmond M, Dijkman HB, Assmann KJ, Mayadas TN, van de Winkel JG (2001) Mac-1 (CD11b/CD18) is essential for Fc receptor-mediated neutrophil cytotoxicity and immunologic synapse formation. Blood 97(8):2478–2486
Blake KM, Carrigan SO, Issekutz AC, Stadnyk AW (2004) Neutrophils migrate across intestinal epithelium using beta2 integrin (CD11b/CD18)-independent mechanisms. Clin Exp Immunol 136(2):262–268. https://doi.org/10.1111/j.1365-2249.2004.02429.x
Parkos CA, Colgan SP, Liang TW, Nusrat A, Bacarra AE, Carnes DK, Madara JL (1996) CD47 mediates post-adhesive events required for neutrophil migration across polarized intestinal epithelia. J Cell Biol 132(3):437–450
Liu Y, Buhring HJ, Zen K, Burst SL, Schnell FJ, Williams IR, Parkos CA (2002) Signal regulatory protein (SIRPalpha), a cellular ligand for CD47, regulates neutrophil transmigration. J Biol Chem 277(12):10028–10036. https://doi.org/10.1074/jbc.M109720200
Nagy GR, Kemeny L, Bata-Csorgo Z (2017) Neutrophil-to-lymphocyte ratio: a biomarker for predicting systemic involvement in adult IgA vasculitis patients. J Eur Acad Dermatol Venereol : JEADV 31(6):1033–1037. https://doi.org/10.1111/jdv.14176
Park CH, Han DS, Jeong JY, Eun CS, Yoo KS, Jeon YC, Sohn JH (2016) The optimal cut-off value of neutrophil-to-lymphocyte ratio for predicting prognosis in adult patients with Henoch–Schonlein purpura. PLoS One 11(4):e0153238. https://doi.org/10.1371/journal.pone.0153238
Makay B, Gucenmez OA, Duman M, Unsal E (2014) The relationship of neutrophil-to-lymphocyte ratio with gastrointestinal bleeding in Henoch-Schonlein purpura. Rheumatol Int 34(9):1323–1327. https://doi.org/10.1007/s00296-014-2986-2
Gayret OB, Erol M, Tekin Nacaroglu H (2016) The relationship of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio with gastrointestinal bleeding in Henoch–Schonlein purpura. Iran J Pediatr 26(5):e8191. https://doi.org/10.5812/ijp.8191
Acknowledgements
We would especially like to thank Prof. Mauro Peretti and Dr. Suchita Nadkarni from WHRI, Queen Mary, University of London for their support in the neutrophil experiments. We acknowledge Biomedis M.B./Biomedica gruppe for kindly providing the AtheNa Multi-Lyte Luminex xMAP Technology needed to perform the multiplex cytokine experiments.
Funding
This study received financial support from the Slovene Research Agency (ARRS) for the National Research Program P3-0314.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None.
Ethical approval and consent to participate
Ethical approval for the study was obtained by the Slovenian National Medical Ethics Committee (#99/04/15 and #65/01/17).
Additional information
Rheumatology in Slovenia: Clinical practice and translational research
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Kuret, T., Lakota, K., Žigon, P. et al. Insight into inflammatory cell and cytokine profiles in adult IgA vasculitis. Clin Rheumatol 38, 331–338 (2019). https://doi.org/10.1007/s10067-018-4234-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-018-4234-8