
Abstract
Background
Despite recent advances in immunosuppressive therapy for patients with primary nephrotic syndrome, its effectiveness and safety have not been fully studied in recent nationwide real-world clinical data in Japan.
Methods
A 5-year cohort study, the Japan Nephrotic Syndrome Cohort Study, enrolled 374 patients with primary nephrotic syndrome in 55 hospitals in Japan, including 155, 148, 38, and 33 patients with minimal change disease (MCD), membranous nephropathy (MN), focal segmental glomerulosclerosis (FSGS), and other glomerulonephritides, respectively. The incidence rates of remission and relapse of proteinuria, 50% and 100% increases in serum creatinine, end-stage kidney disease (ESKD), all-cause mortality, and other major adverse outcomes were compared among glomerulonephritides using the Log-rank test. Incidence of hospitalization for infection, the most common cause of mortality, was compared using a multivariable-adjusted Cox proportional hazard model.
Results
Immunosuppressive therapy was administered in 339 (90.6%) patients. The cumulative probabilities of complete remission within 3 years of the baseline visit was ≥ 0.75 in patients with MCD, MN, and FSGS (0.95, 0.77, and 0.79, respectively). Diabetes was the most common adverse events associated with immunosuppressive therapy (incidence rate, 71.0 per 1000 person-years). All-cause mortality (15.6 per 1000 person-years), mainly infection-related mortality (47.8%), was more common than ESKD (8.9 per 1000 person-years), especially in patients with MCD and MN. MCD was significantly associated with hospitalization for infection than MN.
Conclusions
Patients with MCD and MN had a higher mortality, especially infection-related mortality, than ESKD. Nephrologists should pay more attention to infections in patients with primary nephrotic syndrome.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Nephrotic syndrome is characterized by massive proteinuria, edema, and hypoalbuminuria [1]. Epidemiological studies have shown that patients with nephrotic syndrome are vulnerable to a wide variety of adverse events: end-stage kidney disease (ESKD) [2,3,4], thromboembolism [5], infection [6], malignancy [7], cardiovascular disease (CVD) [8], and all-cause mortality [9]. Primary nephrotic syndrome is the major cause of nephrotic syndrome diagnosed using kidney biopsy, including mainly minimal change disease (MCD), membranous nephropathy (MN), and focal segmental glomerulosclerosis (FSGS) [10]. A systematic review reported that incidences rates of MCD, MN, and FSGS were 0.2–0.8, 0.3–1.4, and 0.2–1.1 per 100,000 person-years, respectively [11].
Immunosuppressive therapy is the main treatment modality for patients with primary nephrotic syndrome as suggested by the clinical guidelines of primary nephrotic syndromes [12, 13]. Systematic reviews of randomized controlled trials on immunosuppressive therapy in patients with MN, the most extensively studied glomerulonephritis in primary nephrotic syndrome, clarified that some immunosuppressive drugs reduced all-cause mortality and risk of ESKD, although the number of trials with a high-quality design was relatively small and most trials did not have adequate follow-up and enough power to assess the prespecified definite outcomes [14, 15]. These systematic reviews also suggested that the drugs were associated with substantial toxicity leading to withdrawals or hospitalization. Their results potentially underestimated the toxicity of immunosuppressive therapy in the real world because patients with a higher risk of toxicity, such as elderly patients, are often excluded in randomized trials [16]. To establish the treatment strategy that has a high effectiveness and low risk of adverse effects, an observational study using real-world data, including patients with a high risk of toxicity from therapeutic interventions, is essential.
The aim of the present cohort study, the Japan Nephrotic Syndrome Cohort Study (JNSCS) [17], was to clarify the incidence of major clinical outcomes in 374 patients with primary nephrotic syndrome during the 5-year follow-up period. The outcomes of interest were remission and relapse of proteinuria, deterioration in kidney function (50% and 100% increases in serum creatinine level and ESKD), CVD, all-cause mortality, and other adverse events associated with immunosuppressive therapy, including infection, diabetes, arteriovenous thrombosis, aseptic osteonecrosis, and peptic ulcers. The results of the present study provide pivotal information to determine the clinical goals of the treatments for primary nephrotic syndrome.
Materials and methods
Participants
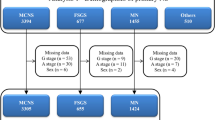
The JNSCS is a 5-year multicenter cohort study of primary nephrotic syndrome to clarify the incidence rates of major clinical outcomes and assess the effectiveness of immunosuppressive therapy in Japan. Details of the study design was described elsewhere [17]. Briefly, 455 nephrotic patients were registered in the JNSCS, who were diagnosed with primary nephrotic syndrome using kidney biopsy during the entry period between January 2009 and December 2010 in 56 hospitals (Fig. 1). The diagnosis of primary nephrotic syndrome was based on the clinical and histopathological characteristics [18]. Nephrotic patients with minor glomerular abnormalities by light microscopy was diagnosed as MCD. The diagnosis of MN was made by the detection of granular deposits of mainly IgG along the glomerular capillary walls by immunofluorescence microscopy with or without thickening of the glomerular capillary wall by light microscopy. FSGS included five variants: collapsing, tip, cellular, perihilar, and not-otherwise specified (NOS) variants [19]. After excluding 81 patients with no kidney biopsy (N = 20), kidney biopsy before or after the entry period (N = 32), no history of nephrotic syndrome (N = 1), diagnosis of secondary nephrotic syndrome (N = 13), sclerosing glomerulonephritis with unknown etiology (N = 1), incomplete informed consent (N = 7), duplicate registrations (N = 3) and unknown reason (N = 4), 374 patients with primary nephrotic syndrome in 55 hospitals were finally enrolled in JNSCS, including those with MCD (N = 155), MN (N = 148), FSGS (N = 38), IgA nephropathy (N = 15), membranoproliferative glomerulonephritis (N = 9), mesangial proliferative glomerulonephritis (N = 5), endocapillary proliferative glomerulonephritis (N = 2), and crescentic glomerulonephritis (N = 2). Because of the small number of patients with glomerulonephritides except those with MCD, MN, and FSGS, the patients were classified into four groups of glomerulonephritides: MCD, MN, FSGS, and other glomerulonephritides.

Flow diagram of patients in the Japan Nephrotic Syndrome Cohort Study (JNSCS). *Including two patients who were diagnosed with MCD at the first kidney biopsy but re-diagnosed with FSGS (NOS variant) at the second biopsy 33 and 1344 days after the first biopsy
The study protocol of JNSCS was approved by the ethics committee of Osaka University Hospital (approval number 17035-4) and the institutional review board of each participating hospital. All procedures performed in the present study were in accordance with the World Medical Association Declaration of Helsinki.
Measurements
The clinical characteristics at the kidney biopsy and, if immunosuppressive therapy was administered, those at initiating immunosuppressive therapy were collected in JNSCS, including age, sex, body mass index, systolic and diastolic blood pressure, 24-h urinary protein, urinary protein-to-creatinine ratio, serum concentration of creatinine, albumin, and total cholesterol, hemoglobin A1c, and use of renin-angiotensin system (RAS) blockers, statins, and antidiabetic drugs. To calculate the estimated glomerular filtration rate (eGFR) in adult patients aged 18 years or older, the Japanese equation was used: eGFR = 194 × age (year)−0.287 × serum creatinine (mg/dL)−1.094 × 0.739 (if female) [20]. As a measure of the baseline urinary protein, 24-h urinary protein was preferred. Urinary protein-to-creatinine ratio was alternatively used only in patients with missing values of the baseline 24-h urinary protein. In the present study, the baseline visit was set at the kidney biopsy or the first date of immunosuppressive therapy, whichever came first.
The outcome measures of interest in the present study consisted of the time to remission and relapse of proteinuria; 50% and 100% irreversible increases in serum creatinine level; ESKD requiring kidney replacement therapy; use of antidiabetic drugs; hospitalization for infection, CVD, and arteriovenous thrombosis; diagnosis of malignancy, aseptic osteonecrosis, and peptic ulcer; and all-cause mortality. Remission of proteinuria was categorized into complete remission, incomplete remission type 1, and incomplete remission type 2; complete remission was defined as 24-h urinary protein of < 0.3 g/day or urinary protein-to-creatinine ratio of < 0.3 g/gCr; incomplete remission type 1 was defined as 24-h urinary protein of < 1.0 g/day or urinary protein-to-creatinine ratio of < 1.0 g/gCr; incomplete remission type 2 was defined as 24-h urinary protein of < 3.5 g/day or urinary protein-to-creatinine ratio of < 3.5 g/gCr [2, 13]. Relapse of proteinuria was defined as 24-h urinary protein of ≥ 1.0 g/day, urinary protein-to-creatinine ratio of ≥ 1.0 g/gCr, and/or 2 + or more of positive dipstick tests for urinary protein continued two times or more in patients with complete remission [13]. CVD included heart disease, stroke, peripheral arterial disease, and sudden death. In patients followed up for more than 5 years, the end of the follow-up was set at 5 years after the baseline visit of each patient. Patients who died were regarded as censored, except in the analyses of all-cause mortality (Supplementary Fig. 1A and B).
Statistical analyses
Baseline clinical characteristics among the four groups of glomerulonephritides were compared using the chi-square test, Fisher's exact test, ANOVA, or Kruskal–Wallis test, as appropriate.
To compare the incidence rates of each outcome among the four groups of glomerulonephritides, their cumulative probabilities were estimated using the Kaplan–Meier method and compared using the Log-rank test. The cumulative probabilities of complete remission, incomplete remission type 1, and incomplete remission type 2 were calculated in 292, 367, and 370 patients with baseline urinary protein of ≥ 0.3, ≥ 1.0, and ≥ 3.5 g/day (or g/gCr), respectively (Supplementary Fig. 1A). To calculate those of relapse of proteinuria after complete remission, 290 patients who achieved complete remission and were followed up thereafter were included. After excluding 16 patients with the baseline use of diabetic drugs, 358 patients with no baseline use of antidiabetic drugs were included for calculation of the cumulative probability of use of diabetic drugs (Supplementary Fig. 1B). The incidence rate of each outcome was calculated based on the Poisson distribution and expressed as the number of events per 1000 person-years.
Because infection was the leading cause of mortality, the incidence of hospitalization for infection was compared among the four groups of glomerulonephritides using unadjusted and multivariable-adjusted Cox proportional hazards models. The proportional hazards assumption for covariates was checked using Schoenfeld residuals. Because the proportional hazards assumption of sex was violated, all multivariable-adjusted Cox proportional hazards models were stratified according to sex to control its potential confounding effect. Multivariable-adjusted model 1 included age as covariates. Models 2 and 3 included serum creatinine and urinary protein as covariates in an additive manner.
Normally distributed continuous variables are expressed as mean ± standard deviation, and non-normally distributed continuous variables as median (interquartile range). Categorical variables are expressed as numbers (proportions). P < 0.05 was considered statistically significant. All statistical analyses were performed using R version 3.6.0 (The R Foundation for Statistical Computing, https://www.r-project.org/).
Results
The clinical characteristics of 155 (41.4%), 148 (39.6%), 38 (10.2%), and 33 (8.8%) patients with MCD, MN, FSGS, and others, respectively, are listed in Table 1. The baseline visit was set at the beginning of immunosuppressive therapy in 45 (29.0%), 14 (9.5%), 9 (23.7%), and 4 (12.1%) patients with MCD, MN, FSGS, and others, respectively, because they underwent kidney biopsy after initiating immunosuppressive therapy, whereas it was set at the date of kidney biopsy in the remaining patients. At their baseline visits, significant differences among the four groups were observed in terms of the age, body mass index, systolic and diastolic blood pressure, urinary protein, serum creatinine, eGFR, serum albumin, serum total cholesterol, and use of RAS blockers, statin, and antidiabetic drugs (P < 0.05). Patients with MCD were likely to have received immunosuppressive therapy before kidney biopsy and have a younger age, higher levels of body mass index, eGFR, and serum total cholesterol, lower levels of blood pressure, serum creatinine and serum albumin, and lower proportion of use of RAS blockers, compared with that in patients with MN, FSGS, and others.
The majority of patients received immunosuppressive therapy within a median (interquartile range) of 3 (− 4, 7), 10 (4, 24), 6 (0, 14), and 10 (4, 14) days of kidney biopsy in 153 (98.7%), 127 (85.8%), 35 (92.1%), and 24 (72.7%) patients with MCD, MN, FSGS, and others, respectively (Table 1). Almost all patients received prednisolone within 24 months of immunosuppressive therapy (98.7%, 95.2%, 100.0%, and 100.0% in MCD, MN, FSGS, and others). One-third of the patients with MCD additionally received intravenous methylprednisolone (31.6%) and cyclosporine (35.5%) within 24 months of immunosuppressive therapy. In patients with MN and FSGS, cyclosporine (56.5% and 62.9%, respectively) was much more common than intravenous methylprednisolone (21.0% and 31.4%, respectively). In contrast, a half of patients with other glomerulonephritides received intravenous methylprednisolone (50.0%), followed by cyclosporine (27.3%). Other immunosuppressive drugs were rarely used, except mizoribine in patients with MN (18.5%).
The cumulative probabilities of remission and relapse of proteinuria during the median follow-up period of 5.0 years (interquartile range 3.2–5.0) are described in Fig. 2a–d. Within one year of the baseline visit, urinary protein decreased below the nephrotic range of proteinuria indicating incomplete remission type 2, in approximately 80% or more of the nephrotic patients at the baseline visit (cumulative probability of incomplete remission type 2 of proteinuria: 0.99 [95% confidence interval 0.95, 1.00], 0.87 [0.78, 0.92], 0.89 [0.69, 0.94], and 0.79 [0.55, 0.90] in patients with MCD, MN, FSGS, and others, respectively) (Table 2). Complete remission of proteinuria (24-h urinary protein of < 0.3 g/day or urinary protein-to-creatinine ratio of < 0.3 g/gCr) was observed in approximately half of the patients with MN and FSGS within one year of the baseline visit. Their cumulative probabilities of complete remission increased by 75% within 3 years of the baseline visit (0.77 [0.68, 0.83] and 0.79 [0.60, 0.89] in patients with MN and FSGS, respectively), whereas only 60% in patients with other glomerulonephritides (0.60 [0.39, 0.74]) (Table 2). Patients with MCD, who had the highest cumulative probability of complete remission, also had the highest cumulative probability of relapse of proteinuria (Table 3). Approximately half of the patients with MCD experienced relapse of proteinuria within 3 years of the baseline visit (0.48 [0.39, 0.56]). Relapse of proteinuria was also common in patients with FSGS (0.44 [0.20, 0.60]). Most patients with MCD and FSGS developed their first relapse during immunosuppressive therapy (79.1% and 90.9%, respectively).


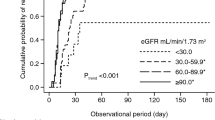
Cumulative probabilities of major clinical outcomes: incomplete remission type 1 (a) and 2 (b), complete remission (c), relapse of proteinuria after complete remission (d), 50% and 100% increase in serum creatinine and/or end-stage kidney disease (ESKD) (e, f), ESKD (g), all-cause mortality (h), and use of diabetic drugs (i)
Patients with other glomerulonephritides had a higher risk of decrease in GFR, followed by that in patients with MN, FSGS, and MCD (Figs. 2e–g, 3). The incidence rate per 1000 person-years of 50% increase in serum creatinine or ESKD was 6.5 (95% confidence interval, 1.8, 16.7), 41.3 (25.6, 63.1), 34.6 (11.2, 80.8), and 121.5 (62.8, 212.2) in patients with MCD, MN, FSGS, and others, respectively (Fig. 3). Because of a short follow-up period of 5 years, the incidence of ESKD was low in patients with MCD, MN, and FSGS (per 1000 person-years; 3.2 [0.4, 11.7], 5.3 [1.1, 15.4], 6.4 [0.2, 35.9], 59.1 [23.8, 121.8] in MCD, MN, FSGS, and others, respectively).

Incidence rates of major outcomes in primary nephrotic syndrome; causes of mortality included infection (N = 6, 5, and 1 in MCD, MN, and FSGS, respectively), malignancy (N = 1, 5, and 1 in MCD, MN, and other glomerulonephritides, respectively), cardiovascular disease (N = 1 and 1 in MCD and MN, respectively) and others (N = 1, 1, and 1 in MCD, MN, and other glomerulonephritides, respectively)
Compared with ESKD, all-cause mortality was more common in patients with MCD and MN (per 1000 person-years; 13.0 [5.6, 25.6] and 21.0 [10.9, 36.8] in MCD and MN, respectively) (Figs. 2g–h, 3). The leading cause of death was infection (N = 11 [47.8%]), followed by malignancy (N = 7 [30.4%]), CVD (N = 2 [8.7%]) and others (N = 3 [13.0%]) (Fig. 3). In patients with MCD and MN, infection was the leading cause of death (N = 6 [66.7%] and 5 [41.7%] in MCD and MN, respectively). Although the incidence of hospitalization for infection was comparable among the four groups of glomerulonephritides (per 1000 person-years; 22.1 [11.8, 37.8], 16.2 [7.4, 30.8], 20.4 [4.2, 59.6], 25.1 [5.2, 73.3] in MCD, MN, FSGS, and others, respectively) (Fig. 3), patients with MCD were associated with hospitalization for infection at a marginally significant level than those with MN, after controlling for age and sex (vs. MN; MCD, adjusted hazard ratio 2.41 [95% confidence interval 0.98, 5.94], P = 0.06; FSGS, 1.58 [0.43, 5.88], P = 0.5; others, 1.78 (0.48, 6.58), P = 0.4) (Table 4). After an additional adjustment for serum creatinine, MCD was significantly associated with hospitalization for infection (Model 2: MCD, 2.44 [1.00, 5.95], P = 0.05; FSGS, 1.48 [0.40, 5.50], P = 0.6; other glomerulonephritides, 1.26 [0.30, 5.29], P = 0.6). A further adjustment for urinary protein confirmed their associations (Model 3).
The use of antidiabetic drugs was common especially among patients with MN and FSGS (Fig. 2I). Their cumulative incidence of use of antidiabetic drugs was approximately 30% one year after the baseline visit (1-year cumulative probability in MCD, MN, FSGS, and other glomerulonephritides: 0.14 [0.08, 0.20], 0.28 [0.20, 0.35], 0.28 [0.12, 0.42], and 0.03 [0.00, 0.10], respectively). During the 5-year follow-up period, other clinical outcomes were relatively rare, including hospitalization for malignancy, CVD, thrombosis, aseptic osteonecrosis, and peptic ulcer (Fig. 3).
Discussion
The present 5-year cohort study, which included 374 patients with primary nephrotic syndrome in 55 hospitals in Japan, clarified the incidence rate of major clinical outcomes and disclosed that the incidence of all-cause mortality was higher than that of ESKD in patients with two major glomerulonephritides, MCD and MN. Hospitalization for infection, the leading cause of all-cause mortality, was significantly more common in patients with MCD than those with MN, suggesting that patients with MCD were vulnerable to infection. Several advantages of the present study include the nature of the cohort study design, the inclusion of two major glomerulonephritides, MCD and MN, the measurements of a wide variety of major clinical outcomes, and the collection of recent real-world clinical data in the most recent decade between 2009 and 2015.
Few studies have compared the incidence rates of ESKD and all-cause mortality among patients with primary nephrotic syndrome. A Korean single-center retrospective cohort study, including 187, 232, and 251 patients with MCD, MN, and FSGS, showed that all-cause mortality was more common than ESKD in MCD and MN during the median observational period of 7.5 years, whereas ESKD was more common than all-cause mortality in FSGS [21]. A similar finding was also reported in a Taiwanese single-center retrospective cohort study with a median observational period of 5.9 years, including 109, 209, and 132 patients with MCD, MN, and FSGS, respectively [22]. However, these studies did not clarify the causes of mortality. After confirming that all-cause mortality was more common than ESKD in patients with MCD and MN, the present multicenter cohort study identified infection as the leading cause of mortality (Fig. 3) and disclosed that patients with MCD were more vulnerable to infection compared to patients with MN (Table 4). One of the plausible reasons for the higher incidence rate of infection in patients with MCD might be due to the higher incidence of relapses of proteinuria with add-on use of immunosuppressive drugs. Compared to patients with MN, patients with MCD had a higher risk of relapse of proteinuria during immunosuppressive therapy (Table 3), probably leading to the higher doses of immunosuppressive drugs. Unfortunately, the dose of each immunosuppressive drug during the immunosuppressive therapy was not available in the present study. Further research with details of immunosuppressive drugs are essential to assess an association between immunosuppressive therapy and infection.
Comparable with the results of the present cohort study, previous retrospective cohort studies on MCD reported that infection was one of the most common adverse events [23,24,25,26,27] and one of the leading causes of mortality [28]. To suppress the incidence of infection, a lower dose of and/or shorter term immunosuppressive therapy is desirable. Among pediatric patients with corticosteroid-sensitive nephrotic syndrome, two randomized trials in Japan [29] and India [30] recently demonstrated that the incidence of relapse of proteinuria was comparable between conventional 6-month corticosteroid therapy and 3-month corticosteroid therapy. In adult patients with MCD, only low-quality evidences in this regard are available. Several guidelines suggested longer corticosteroid therapy; the Kidney Disease Improving Global Outcomes (KDIGO) clinical guideline for glomerulonephritis suggested a daily dose of 1.0 mg/kg of prednisolone or an alternate-day single dose of 2 mg/kg tapered slowly over a total period of up to 6 months [12] and the Japanese evidence-based clinical practice guideline for nephrotic syndrome suggest 0.6–0.8 mg/kg of prednisolone tapered within 2 years [13]. Compared with these conventional long corticosteroid therapies, an intriguing Japanese observational study of adult patients with MCD suggested clinical advantages of a 2-month corticosteroid therapy, the lower incidence of adverse events, including diabetes and infection [31]. Because nephrologists might possibly maintain adult patients with MCD on corticosteroids for very long [32], an optimal immunosuppressive therapy should be explored in well-designed clinical studies to prevent critical events associated with immunosuppressive therapy, including infection.
The present study has several limitations. First, the incidence of all-cause mortality (N = 22) and ESKD (N = 12) was small; thus, the findings of the present study might not be reproducible. The JNSCS is planning to extend the 5-year follow-up period to 10 years, providing more precise details regarding the clinical impacts of major outcomes in patients with primary nephrotic syndrome. Second, the small number of patents with FSGS and other glomerulonephritides hindered statistically meaningful analyses in JNSCS. The results of the present study suggested the cumulative probabilities of complete remission of proteinuria and an increase of serum creatinine of FSGS were comparable to those of MN (Fig. 2c, e, f), although the higher rate of relapse of proteinuria of FSGS, which was comparable to that of MCD (Fig. 2d). Because the higher probability of relapse might contribute to the higher risk of infection in patients with MCD, those with FSGS might be similarly vulnerable to infection. To clarify their clinical courses, a larger cohort study is needed. Third, the incidences of some outcomes were dependent on the practice patterns of each hospital. For example, the thresholds of plasma glucose concentration and/or hemoglobin A1c to start antidiabetic drugs might be different among the hospitals.
In conclusion, the JNSCS revealed that patients with MCD and MN had a higher risk of all-cause mortality than that of ESKD. Patients with MCD were more vulnerable to infection, the leading cause of mortality, compared to patients with MN. These results provide pivotal information that identifies the treatment goals of primary nephrotic syndrome with the recent immunosuppressive therapy. Nephrologists might possibly pay more attention to infection in patients with primary nephrotic syndrome.
References
Agrawal S, Zaritsky JJ, Fornoni A, Smoyer WE. Dyslipidaemia in nephrotic syndrome: mechanisms and treatment. Nat Rev Nephrol. 2017;14:57–70.
Shiiki H, Saito T, Nishitani Y, Mitarai T, Yorioka N, Yoshimura A, et al. Prognosis and risk factors for idiopathic membranous nephropathy with nephrotic syndrome in Japan. Kidney Int. 2004;65:1400–7.
Troyanov S, Wall CA, Miller JA, Scholey JW, Cattran DC, Toronto Glomerulonephritis Registry Group. Focal and segmental glomerulosclerosis: definition and relevance of a partial remission. J Am Soc Nephrol. 2005;16:1061–8.
Kono M, Yasuda S, Kato M, Kanetsuka Y, Kurita T, Fujieda Y, et al. Long-term outcome in Japanese patients with lupus nephritis. Lupus. 2014;23:1124–32.
Christiansen CF, Schmidt M, Lamberg AL, Horváth-Puhó E, Baron JA, Jespersen B, et al. Kidney disease and risk of venous thromboembolism: a nationwide population-based case-control study. J Thromb Haemost. 2014;12:1449–544.
Wu HM, Tang JL, Cao L, Sha ZH, Li Y. Interventions for preventing infection in nephrotic syndrome. Cochrane Datab Syst Rev. 2012;4:CD003964.
Christiansen CF, Onega T, Sværke C, Körmendiné Farkas D, Jespersen B, Baron JA, et al. Risk and prognosis of cancer in patients with nephrotic syndrome. Am J Med. 2014;127(871–7):e1.
Ordoñez JD, Hiatt RA, Killebrew EJ, Fireman BH. The increased risk of coronary heart disease associated with nephrotic syndrome. Kidney Int. 1993;44:638–42.
Wakasugi M, Kazama JJ, Narita I. Premature mortality due to nephrotic syndrome and the trend in nephrotic syndrome mortality in Japan, 1995–2014. Clin Exp Nephrol. 2018;22:55–60.
Sugiyama H, Yokoyama H, Sato H, Saito T, Kohda Y, Nishi S, et al. Japan renal biopsy registry: the first nationwide, web-based, and prospective registry system of renal biopsies in Japan. Clin Exp Nephrol. 2011;15:493–503.
McGrogan A, Franssen CFM, De Vries CS. The incidence of primary glomerulonephritis worldwide: a systematic review of the literature. Nephrol Dial Transpl. 2011;26:414–30.
Kidney Disease Improving Global Outcomes. KDIGO clinical practice guideline for glomerulonephritis. Kidnet Int Suppl. 2012;2:1–274.
Nishi S, Ubara Y, Utsunomiya Y, Okada K, Obata Y, Kai H, et al. Evidence-based clinical practice guidelines for nephrotic syndrome 2014. Clin Exp Nephrol. 2016;20:342–70.
Chen Y, Schieppati A, Chen X, Cai G, Zamora J, Giuliano GA, et al. Immunosuppressive treatment for idiopathic membranous nephropathy in adults with nephrotic syndrome. Cochrane database Syst Rev. 2014;10:CD004293.
Ren S, Wang Y, Xian L, Toyama T, Jardine M, Li G, et al. Comparative effectiveness and tolerance of immunosuppressive treatments for idiopathic membranous nephropathy: a network meta-analysis. PLoS ONE. 2017;12:1–15.
Van Spall HGC, Toren A, Kiss A, Fowler RA. Eligibility criteria of randomized controlled trials published in high-impact general medical journals: a systematic sampling review. JAMA. 2007;297:1233–40.
Yamamoto R, Imai E, Maruyama S, Yokoyama H, Sugiyama H, Nitta K, et al. Regional variations in immunosuppressive therapy in patients with primary nephrotic syndrome: the Japan nephrotic syndrome cohort study. Clin Exp Nephrol. 2018;22:1266–80.
Churg J, Bernstein J, Glassock R. Renal disease, classification and atlas of glomerular disease. 2nd ed. New York: Igaku-Shoin Medical Pub; 1995.
D’Agati VD, Fogo AB, Bruijn JA, Jennette JC. Pathologic classification of focal segmental glomerulosclerosis: a working proposal. Am J Kidney Dis. 2004;43:368–82.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Lee H, Kim DK, Oh K-H, Joo KW, Kim YS, Chae D-W, et al. Mortality and renal outcome of primary glomerulonephritis in Korea: observation in 1943 biopsied cases. Am J Nephrol. 2013;37:74–83.
Chou YH, Lien YC, Hu FC, Lin WC, Kao CC, Lai CF, et al. Clinical outcomes and predictors for ESRD and mortality in primary GN. Clin J Am Soc Nephrol. 2012;7:1401–8.
Waldman M, Crew RJ, Valeri A, Busch J, Stokes B, Markowitz G, et al. Adult minimal-change disease: clinical characteristics, treatment, and outcomes. Clin J Am Soc Nephrol. 2007;2:445–53.
Shinzawa M, Yamamoto R, Nagasawa Y, Oseto S, Mori D, Tomida K, et al. Age and prediction of remission and relapse of proteinuria and corticosteroid-related adverse events in adult-onset minimal-change disease: a retrospective cohort study. Clin Exp Nephrol. 2013;17:839–47.
Maas RJ, Deegens JK, Beukhof JR, Reichert LJ, ten Dam MA, Beutler JJ, et al. The clinical course of minimal change nephrotic syndrome with onset in adulthood or late adolescence: a case series. Am J Kidney Dis. 2017;69:637–46.
Fenton A, Smith SW, Hewins P. Adult minimal-change disease: observational data from a UK centre on patient characteristics, therapies, and outcomes. BMC Nephrol. 2018;19:1–8.
Ozeki T, Ando M, Yamaguchi M, Katsuno T, Kato S, Yasuda Y, et al. Treatment patterns and steroid dose for adult minimal change disease relapses: a retrospective cohort study. PLoS ONE. 2018;13:e0199228.
Szeto C-C, Lai FM-M, Chow K-M, Kwan BC-H, Kwong VW-K, Leung C-B, et al. Long-term outcome of biopsy-proven minimal change nephropathy in Chinese adults. Am J Kidney Dis. 2015;65:710–8.
Yoshikawa N, Nakanishi K, Sako M, Oba MS, Mori R, Ota E, et al. A multicenter randomized trial indicates initial prednisolone treatment for childhood nephrotic syndrome for two months is not inferior to six-month treatment. Kidney Int. 2015;87:225–32.
Sinha A, Saha A, Kumar M, Sharma S, Afzal K, Mehta A, et al. Extending initial prednisolone treatment in a randomized control trial from 3 to 6 months did not significantly influence the course of illness in children with steroid-sensitive nephrotic syndrome. Kidney Int. 2015;87:217–24.
Ozeki T, Katsuno T, Hayashi H, Kato S, Yasuda Y, Ando M, et al. Short-term steroid regimen for adult steroid-sensitive minimal change disease. Am J Nephrol. 2019;49:54–63.
Bomback AS. Shortening the duration of corticosteroid exposure in minimal change disease: can we treat adults like children? Am J Nephrol. 2019;49:52–3.
Acknowledgements
JNSCS was supported by a Grant-in-Aid for intractable Renal Diseases Research, Research on rare and intractable diseases, Health and Labour Sciences Research Grants for the Ministry of Health, Labor, and Welfare of Japan. JNSCS has been supported by a large number of investigator in 56 participating facilities; Hokkaido University Hospital, Sapporo, Hokkaido (Saori Nishio, Yasunobu Ishikawa, Daigo Nakazawa, and Tasuku Nakagaki); JCHO Sendai Hospital, Sendai, Miyagi (Toshinobu Sato, Mitsuhiro Sato, and Satoru Sanada); Tohoku University Hospital, Sendai, Miyagai (Hiroshi Sato, Mariko Miyazaki, Takashi Nakamichi, Tae Yamamoto, Kaori Narumi, and Gen Yamada); Yamagata University Hospital, Yamagata, Yamagata (Tsuneo Konta, and Kazuobu Ichikawa); Fukushima Medical University Hospital, Fukushima, Fukushima (Junichiro James Kazama, Tsuyoshi Watanabe, Koichi Asahi, Yuki Kusano, and Kimio Watanabe); University of Tsukuba Hospital, Tsukuba, Ibaraki (Kunihiro Yamagata, Joichi Usui, Shuzo Kaneko, and Tetsuya Kawamura); Gunma University Hospital, Maeashi, Gunma (Keiju Hiromura, Akito Maeshima, Yoriaki Kaneko, Hidekazu Ikeuchi, Toru Sakairi, and Masao Nakasatomi); Saitama Medical Center, Saitama Medical University, Kawagoe, Saitama (Hajime Hasegawa, Takatsugu Iwashita, Taisuke Shimizu, Koichi Kanozawa, Tomonari Ogawa, Kaori Takayanagi, and Tetsuya Mitarai); Department of Nephrology, Saitama Medical University, Irumagun, Saitama (Hirokazu Okada, Tsutomu Inoue, Hiromichi Suzuki, and Kouji Tomori); Tokyo Women's Medical University, Shinjuku-ku, Tokyo (Kosaku Nitta, Takahito Moriyama, Akemi Ino, and Masayo Sato); Teikyo University School of Medicine, Itabashi-ku, Tokyo (Shunya Uchida, Hideaki Nakajima, Hitoshi Homma, Nichito Nagura, Yoshifuru Tamura, Shigeru Shibata, and Yoshihide Fujigaki); Juntendo Faculty of Medicine, Bunkyo-ku, Tokyo (Yusuke Suzuki, Yukihiko Takeda, Isao Osawa, and Teruo Hidaka); St. Marianna University, Kawasaki, Kanagawa (Yugo Shibagaki, Sayuri Shirai, Daisuke Ichikawa, Tsutomu Sakurada, Tomo Suzuki, and Mikako Hisamichi); Niigata University Medical and Dental Hospital, Niigata, Niigata (Ichiei Narita, Naohumi Imai, Yumi Ito, Shin Goto, Yoshikatsu Kaneko, and Rhohei Kaseda); Kanazawa Medical University, Uchinada, Ishikawa (Hitoshi Yokoyama, Keiji Fujimoto, and Norifumi Hayashi); Kanazawa Univeristy Hospital, Kanazawa, Ishikawa (Takashi Wada, Miho Shimizu, Kengo Furuichi, Norihiko Sakai, Yasunori Iwata, Tadashi Toyama, and Shinji Kitajima); National Hospital Organization Kanazawa Medical Center, Kanazawa, Ishikawa (Kiyoki Kitagawa); Ogaki Municipal Hospital, Ogaki, Gifu (Hiroshi Sobajima, Norimi Ohashi, So Oshitani, and Kiyohito Kawashima); Gifu Prefectural Tajimi Hospital, Tajimi, Gifu (Tetsushi Mimura); Hamamatsu University Hospital, Hamamatsu, Shizuoka (Hidemo Yasuda, Akira Hishida, and Yoshihide Fujigaki); Shizuoka General Hospital, Shizuoka, Shizuoka (Satoshi Tanaka, and Noriko Mori); Chutoen General Medical Center, Kakegawa, Shizuoka (Toshiyuki Akahori, and Yutaka Fujita); Nagoya University Graduate School of Medicine, Nagoya, Aichi (Shoichi Maruyama, Naotake Tsuboi, Tomoki Kosugi, Takuji Ishimoto, Takayuki Katsuno, Noritoshi Kato, and Waichi Sato); Japanese Red Cross Nagoya Daini Hospital, Nagoya, Aichi (Asami Takeda, Kunio Morozumi, Yasuhiro Ohtsuka, Hibiki Shinjo, and Akihito Tanaka); Fujita Health University School of Medicine, Toyoake, Aichi (Hiroki Hayashi, Yukio Yuzawa, Midori Hasegawa, Daijo Inaguma, Shigehisa Koide, and Kazuo Takahashi); Konan Kosei Hospital, Konan, Aichi (Takeyuki Hiramatsu, Shinji Furuta, and Hideaki Ishikawa); Anjo Kosei hospital, Anjo, Aichi (Hirofumi Tamai, and Takatoshi Morinaga); Ichinomiya Municipal Hospital, Ichinomiya, Aichi (Arimasa Shirasaki, Toshiki Kimura, and Mina Kato); Japanese Red Cross Nagoya Daiichi Hospital, Nagaoya, Aichi (Shizunori Ichida, and Nobuhide Endo); Kasugai Municipal Hospital, Kasugai, Aichi (Tomohiko Naruse, Yuzo Watanabe, and Yosuke Saka); Kainan hospital, Yatomi, Aichi (Satashi Suzuki, Michiko Yamazaki, and Rieko Morita); Masuko Memorial Hospital, Nagoya, Aichi (Kunio Morozumi, Kunio Morozumi, Kaoru Yasuda, Chika Kondo, Takahiro Morohiro, Rho Sato, and Yuichi Shirasawa); Chubu Rosai Hospital, Nagoya, Aichi (Yoshiro Fujita, Hideaki Shimizu, and Tatsuhito Tomino); Handa City Hospital, Handa, Aichi (Makoto Mizutani); Yokkaichi Municipal Hospital, Yokkaichi, Mie (Yosuke Saka, Hiroshi Nagaya, and Makoto Yamaguchi); Kitano Hospital, Osaka, Osaka (Tatsuo Tsukamoto, Eri Muso, Hiroyuki Suzuki, Tomomi Endo, and Hiroko Kakita); Toyonaka Municipal Hospital, Toyonaka, Osaka (Megumu Fukunaga); Osaka General Medical Center, Osaka, Osaka (Tatsuya Shoji, and Terumasa Hayashi); Osaka City University Hospital, Osaka, Osaka (Eiji Ishimura, Akihiro Tsuda, Shinya Nakatani, Ikue Kobayashi, Mitsuru Ichii, Akinobu Ochi, and Yoshiteru Ohno); Osaka Univeristy hospital, Suita, Osaka (Yoshitaka Isaka, Enyu Imai, Yasuyuki Nagasawa, Hirotsugu Iwatani, Ryohei Yamamoto, and Tomoko Namba); Kobe University hospital, Kobe, Hyogo (Shunsuke Goto MD, and Shinichi Nishi); Nara Medical University Hospital, Kashihara, Nara (Yasuhiro Akai, Ken-ichi Samejima, Masaru Matsui, Miho Tagawa, Kaori Tanabe, and Hideo Tsushima); Wakayama Medical University Hospital, Wakayama, Wakayama (Takashi Shigematsu MD, Masaki Ohya, Shigeo Negi, and Toru Mima); Shimane University Hospital, Izumo, Shimane (Takafumi Ito); Okayama Univeristy Hospital, Okayama, Okayama (Hitoshi Sugiyama, Keiko Tanaka, Toshio Yamanari, Masashi Kitagawa, Akifumi Onishi, and Koki Mise); Kawasaki Medical School, Kurashiki, Okayama (Naoki Kashihara, Tamaki Sasaki, Sohachi Fujimoto, and Hajime Nagasu); Graduate School of Medicine, The University of Tokushima,Tokushima,Tokushima (Kojiro Nagai, and Toshio Doi); Kagawa University, Miki-cho, Takamatsu, Japan (Tadashi Sofue, Hideyasu Kiyomoto, Kumiko Moriwaki, Taiga Hara, Yoko Nishijima, Yoshio Kushida, and Tetsuo Minamino); Kochi Medical School, Kochi University, Nankoku, Kochi (Yoshio Terada, Taro Horino, Yoshinori Taniguchi, Kosuke Inoue, Yoshiko Shimamura, and Tatsuki Matsumoto); Kyushu University Hospital, Fukuoka, Fukuoka (Kazuhiko Tsuruya, Hisako Yoshida, Naoki Haruyama, Shunsuke Yamada, Akihiro Tsuchimoto, and Yuta Matsukuma); Fukuoka University Hospital, Fukuoka, Fukuoka (Kosuke Masutani, Yasuhiro Abe, Aki Hamauchi, Tetsuhiko Yasuno, and Kenji Ito); Kurume University Hospital, Kurume, Fukuoka (Kei Fukami, Junko Yano, Chika Yoshida, Yuka Kurokawa, and Nao Nakamura); National Fukuoka Higashi Medical Center, Koga, Fukuoka (Ritsuko Katafuchi, Hiroshi Nagae, Shumei Matsueda, and Kazuto Abe); Nagasaki University Hospital, Nagasaki, Nagasaki (Tomoya Nishino, Tadashi Uramatsu, and Yoko Obata); Miyazaki University Hospital, Miyazaki, Miyazaki (Shouichi Fujimoto, Yuji Sato, Masao Kikuchi, Ryuzo Nishizono, Takashi Iwakiri, and Hiroyuki Komatsu).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no conflict of interest exists.
Ethical approval
All procedures performed in JNSCS involving human participants were in accordance with the ethical standards of the institutional research committee at which the studies were conducted (IRB approval number 17035-4 at the ethics committee of Osaka University Hospital) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from participants in 54 hospitals and a single hospital used an opt-out approach to informed consent, according to Japanese Ethical Guidelines for Medical and Health Research Involving Human Subjects.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Yamamoto, R., Imai, E., Maruyama, S. et al. Incidence of remission and relapse of proteinuria, end-stage kidney disease, mortality, and major outcomes in primary nephrotic syndrome: the Japan Nephrotic Syndrome Cohort Study (JNSCS). Clin Exp Nephrol 24, 526–540 (2020). https://doi.org/10.1007/s10157-020-01864-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-020-01864-1