
Abstract
There is a lack of knowledge about specific components that make interventions effective in preventing or reducing child maltreatment. The aim of the present meta-analysis was to increase this knowledge by summarizing findings on effects of interventions for child maltreatment and by examining potential moderators of this effect, such as intervention components and study characteristics. Identifying effective components is essential for developing or improving child maltreatment interventions. A literature search yielded 121 independent studies (N = 39,044) examining the effects of interventions for preventing or reducing child maltreatment. From these studies, 352 effect sizes were extracted. The overall effect size was significant and small in magnitude for both preventive interventions (d = 0.26, p < .001) and curative interventions (d = 0.36, p < .001). Cognitive behavioral therapy, home visitation, parent training, family-based/multisystemic, substance abuse, and combined interventions were effective in preventing and/or reducing child maltreatment. For preventive interventions, larger effect sizes were found for short-term interventions (0–6 months), interventions focusing on increasing self-confidence of parents, and interventions delivered by professionals only. Further, effect sizes of preventive interventions increased as follow-up duration increased, which may indicate a sleeper effect of preventive interventions. For curative interventions, larger effect sizes were found for interventions focusing on improving parenting skills and interventions providing social and/or emotional support. Interventions can be effective in preventing or reducing child maltreatment. Theoretical and practical implications are discussed.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Child maltreatment is a serious problem that affects many children around the world. A recent series of meta-analyses showed that worldwide prevalence rates of child maltreatment ranged from 0.3% based on studies using maltreatment reports of professionals to 36.6% based on self-report studies (Stoltenborgh et al. 2014). Child maltreatment is associated with serious short-term and long-term negative consequences, such as physical, behavioral, and psychological problems, leading to high costs for individuals and society (Alink et al. 2012; Gilbert et al. 2008; Jonson-Reid et al. 2012) . Given the high prevalence rates and serious consequences of child maltreatment, effective prevention of child maltreatment is essential. The number of interventions aimed at preventing or reducing child maltreatment has grown over the years. However, several meta-analyses on the effectiveness of these interventions showed only a limited effect (e.g., Euser et al. 2015; Geeraerts et al. 2004; MacLeod and Nelson 2000; Sweet and Appelbaum 2004). Therefore, it is very important to unravel intervention components that contribute to intervention effectiveness from components not contributing to (or even negatively affecting) intervention effectiveness. Consequently, new promising interventions may be developed and existing interventions may be improved by integrating effective components in interventions and/or eliminating ineffective components from interventions. To enhance knowledge on how specific components of child maltreatment interventions affect the effectiveness of these interventions, a comprehensive meta-analysis was performed in the present study.
The number of interventions aimed at preventing or reducing child maltreatment has increased exponentially over the last decades (Daro 2011). Most interventions target a clearly defined population that is identified on the basis of risk factors for child maltreatment, such as teenage mothers, drug or alcohol addicted parents, or multiproblem families. Interventions may be aimed at reducing the incidence of child maltreatment in maltreating families or at preventing the occurrence of child maltreatment in at-risk, but non-maltreating families. The former are often system interventions, whereas the latter often comprise home visitation interventions in which parents are visited at home and provided with information, support, and/or training regarding child health, development, and care. These interventions often begin prenatally and continue during the child’s first 2 years of life, but may also begin after birth and last only a few months. In addition, some interventions are aimed at preventing the first occurrence of child maltreatment in the general population, for example by providing a short parental skills training to parents who visit a well-baby clinic.
A number of meta-analyses have synthesized results on the effectiveness of interventions aimed at preventing or reducing child maltreatment (e.g., Euser et al. 2015; Filene et al. 2013; Geeraerts et al. 2004; Guterman 1999; Layzer et al. 2001; Pinquart and Teubert 2010; Sweet and Appelbaum 2004). These studies generally found minor effects of interventions for reducing or preventing child maltreatment. In specific, Geeraerts et al. (2004) found a small effect (d = .29) of early prevention interventions for families with young children at risk for physical child abuse and neglect. Filene et al. (2013) found a small effect (d = .20) of home visitation interventions, and Pinquart and Teubert (2010) found a very small but significant effect (d = .13) of parent education interventions for expectant and new parents. Euser et al. (2015) also found a very small but significant effect (d = 0.13) of interventions aimed at preventing or reducing child maltreatment. However, this last effect was no longer significant after publication bias was taken into account by applying the trim-and-fill approach.
A few meta-analyses have attempted to identify characteristics of child maltreatment interventions associated with intervention effectiveness by examining potential moderators of the mean effect of interventions. However, none of these meta-analyses extensively examined whether and how specific intervention components, such as different content or delivery methods, influence intervention effectiveness. In studies on child maltreatment interventions, different terms are used for intervention components, such as practice elements (Chorpita and Daleiden 2009), kernels (Embry and Biglan 2008), behavior change techniques (Michie et al. 2013), and core components (Blase and Fixsen 2013). Blase and Fixsen (2013) classify core components into: (1) contextual factors, such as types of families served (e.g., low-income teenage parents, parents with alcohol or drug problems) and delivery settings (e.g., clinic-based therapy, home visits), (2) structural elements, such as the required number and specific sequence of sessions, and (3) specific intervention practices, such as teaching problem-solving behavior, practicing communication skills, and reinforcing appropriate behavior. Specific intervention practices can be further classified based on intervention content (such as increasing knowledge of typical child development, increasing parenting self-efficacy, and improving discipline and/or behavior management strategies) and delivery techniques used to engage parents and teach relevant content (such as group discussions, homework assignments, role-playing, and modeling).
The main objective of this meta-analysis was to determine whether and how intervention components (i.e., intervention content and delivery techniques) influence the effectiveness of child maltreatment interventions. In doing so, important insight can be gained into what components contribute to intervention effectiveness and, consequently, how child maltreatment interventions can best be designed to reach optimal effectiveness. For this purpose, we conducted a three-level meta-analysis in which we tested intervention components as potential moderators of the (mean) effect of child maltreatment interventions. As we aimed for a comprehensive meta-analysis, we included (a) two types of interventions: preventive interventions targeting the general population or families at risk for child maltreatment and curative interventions targeting maltreating families that are aimed at reducing maltreatment, (b) randomized controlled trials (RCTs) as well as high quality quasi-experimental studies, and (c) recently conducted studies, as previous meta-analyses included studies that were published until 2013.
Determining which components appear to be essential (or nonessential) across a variety of interventions aimed at reducing or preventing child maltreatment has important implications for clinical practice. First, when choosing among interventions to implement, such information could be used to select interventions containing components associated with greater intervention effectiveness. Second, the effectiveness of existing interventions could be improved by integrating specific components associated with greater effectiveness into interventions. Third, it may be possible to eliminate components associated with less effective interventions, thereby minimizing the burden on practitioners and families.
In the present study, we aimed to examine the effect of contextual factors (i.e., general aim of the intervention, types of families served, delivery setting, type of intervention, specific intervention, age of the children), structural elements (i.e., type of worker, duration of intervention, number and interval of intervention sessions), content (parenting skills, personal skills parents, self-confidence of parents, attitudes/expectations toward parenting, knowledge of typical child development, social network of family, relationship between parents, relationship between parent and child, parental mental health problems, parental empowerment, social/emotional support, well-being child, child skills, practical support, motivation to change), and delivery methods (i.e., modeling, role-playing, monitoring, (psycho) education, homework assignments, cognitive skills training, and family group conferencing). We also examined the effect of study design characteristics such as sample characteristics (i.e., sample size, age of parents, percentage of cultural minorities), design of the study (randomized controlled trial versus quasi-experimental), and outcome characteristics (follow-up duration, type of outcome measure).
Method
Inclusion Criteria
Studies were selected if they met the following three criteria. First, studies had to report on the effect of at least one intervention for preventing or reducing child maltreatment. In specific, we included two types of interventions: preventive interventions targeting the general population or targeting families at risk for child maltreatment and curative interventions targeting maltreating families aimed at reducing maltreatment or recurrence of maltreatment. In this review, we followed the definition of child maltreatment as formulated by the Centers for Disease Control and Prevention: “any act or series of acts of commission or omission by a parent or other caregiver that results in harm, potential for harm, or threat of harm to a child.” Given this broad definition, we included studies that reported on interventions for physical abuse, sexual abuse, and neglect. In addition, studies examining the effect of child maltreatment interventions on harsh parenting (such as corporal/physical punishment or parental aggression toward children) and out-of-home placement were also included. Second, experimental studies as well as quasi-experimental studies (in which a treatment condition is compared to a control condition) were included. Although randomized controlled trials can be regarded as the “golden standard” for studies examining the effectiveness of interventions (Farrington 2003), we decided to also include quasi-experimental studies, since RCTs are rather scarce in the field of child protection due to practical and ethical concerns for true experimental designs. Third, studies had to report at least one effect size or sufficient information to calculate at least one effect size.
Selection of Studies
The electronic databases PsychINFO, ERIC, PubMed, Web of Science, ScienceDirect, and Google Scholar were searched for articles, books, chapters, dissertations, and reports. Until March 2017, studies were collected using keywords regarding study design, intervention features, study outcomes, and participants in different combinations: ‘(quasi-)experiment’, ‘randomized control*’, ‘trial’, ‘RCT’ ‘child*’, ‘abus*’, ‘maltreat*’, ‘neglect*’, ‘interven*’, ‘preven*’, ‘home visit*’, ‘recur*’, ‘recidiv*’, ‘relaps*’, ‘family group conferencing’ ‘randomized’, ‘evaluat*’, and ‘experiment*’.
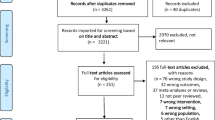
Next, manual searches of reference sections of the retrieved articles, reviews, and book chapters were conducted. Finally, we contacted authors by email to request for studies and unpublished manuscripts on the effect of child maltreatment interventions that may be relevant for inclusion in the present review. The search procedure is depicted in the flow diagram presented in Fig. 1. The search yielded 546 relevant studies of which 130 studies met the inclusion criteria.

Flowchart of selection of studies for inclusion in meta-analysis
Study Coding
Following the guidelines of Lipsey and Wilson (2001), a coding scheme was developed to code all study design and intervention characteristics that could moderate the effect of child maltreatment interventions.
First, with regard to study design characteristics, we collected information on publication year, sample size, parental age, percentage of cultural minorities in samples, research design (RCT, quasi-experimental design), pilot/feasibility study (yes/no), follow-up length (in months), and type of outcome measure (self-report of parents, official reports, observations, hospital data, self-report of children). Second, we retrieved information on intervention characteristics, which we divided into contextual factors, structural elements, and specific intervention practices (content and delivery techniques). The contextual factors included the general aim of the intervention (reducing risk for child maltreatment versus reducing actual child maltreatment), type of families served (maltreating parents, general population, risk group identified by means of a questionnaire, risk group identified based on the presence of one or two risk factors), delivery setting (home/ambulant, treatment center, combination of locations), post-/prenatal intervention (postnatal, prenatal, postnatal and prenatal), type of intervention (cognitive behavioral therapy, home visitation interventions [in which parents are visited at home and provided with information, support and/or training regarding child health, development and care], parent training interventions [aimed at learning specific parenting skills], family-based/multisystemic interventions [aimed at the whole family system/multiple social systems], substance abuse intervention [primarily targeting substance abuse of parents], before-school interventions, general prevention interventions [aimed at preventing the occurrence of child maltreatment in the general population], crisis interventions [aimed at solving acute problems], and combined interventions), specific individual interventions (ACT Parenting Raising Safe Kids, (Early) Head Start, PCIT, FGC/FCDM, Healthy Families, Healthy Start, Healthy Steps, Intensive Family Preservation Services, Incredible Years, MST (CAN/BSF), Nurse Family Partnership (NFP), Triple P, Parents as Teachers, Project 12-Ways, Safe Environment for Every Kid, Child Parent Enrichment Program, SafeCare, other), and age of the child (unborn child/baby (< 2), infant/toddler (2–5), primary school (6–12), high school (> 12). The structural elements included type of worker (professionals only versus professionals and others), the duration of the intervention (0–6 months, 7–12 months, 13–24 months, > 24 months), the minimum duration of the intervention, the maximum duration of the intervention, the average number of sessions, and the interval of the sessions (weekly, multiple sessions a week, every other week/monthly, ascending/descending intensity, every 3 months). The specific intervention practices (content) included parenting skills (yes/no), personal skills of parents (yes/no), parents’ self-confidence (yes/no), attitudes or expectations about parenting (yes/no), knowledge of typical child development (yes/no), social network of the family (yes/no), relationship between parents (yes/no), relationship between parent and child (yes/no), mental health problems parents (yes/no), parental empowerment (yes/no), social or emotional support (yes/no), well-being of the child (yes/no), child skills (yes/no), practical support (yes/no), and motivation (yes/no). Finally, we examined the following delivery techniques: modeling (yes/no), role-playing (yes/no), monitoring (yes/no), (psycho)education (yes/no), homework assignments (yes/no), cognitive skills training (yes/no), and family group conferencing (yes/no). Inter-rater agreement was based on a double-coding of 14 studies by two independent coders. An inter-rater agreement of 97% was found between the two coders on all coded variables.
Calculation of Effect Sizes
All outcomes of the primary studies were transformed into the standardized difference between two means, also referred to as Cohen’s d. The effect sizes were calculated using formulas of Ferguson (1966), Lipsey and Wilson (2001), and Rosenthal (1994). In most instances, proportions, means and standard deviations, and odd ratios were transformed into Cohen’s d. If insufficient statistical information was provided for calculating an effect size, we contacted the study authors and asked for the required information. In calculating each effect size, it was important that the direction of the effect (positive or negative) corresponded with the statistical data reported in the primary study. A positive effect indicated less child maltreatment (or levels of other factors, such as harsh parenting) was found in the intervention group than in the control group, whereas a negative effect indicated more child maltreatment in the intervention group than in the control group. If results were reported to be nonsignificant and additional statistical information required for calculating an effect size was not reported, the value of zero was assigned to an effect and added to the data set (Durlak and Lipsey 1991).
All coded data and calculated effect sizes were entered in SPSS version 22. Before the analyses were performed, continuous variables were centered around their mean, and categorical variables were recoded into dummy variables for each category of a variable. Further, extreme values of effect sizes and sample sizes (Z > 3.29 or Z < − 3.29; Tabachnik and Fidell 2013) were identified.
Statistical Analyses
For estimating the overall effect for all included child maltreatment interventions, only preventive interventions, and only curative interventions, as well as for examining potential moderating variables, a three-level meta-analysis technique was used. By applying a multilevel approach to meta-analysis, there is no need for aggregating or selecting data, implying that all relevant effect sizes can be extracted from primary studies (see also Assink et al. 2015; Assink and Wibbelink 2016). As a result, all information from primary studies is preserved and maximum statistical power can be achieved. In our meta-analytic model, three forms of variance were taken into account: random sampling variation of observed effect sizes (level 1), variance within studies (level 2), and variance between studies (level 3) (Cheung 2014; Hox 2002; Van den Noortgate et al. 2013, 2014). The sampling variance (level 1) was not estimated, but considered to be known and calculated using the formula of Cheung (2014, p. 2015). Because we considered the primary studies to be a random sample from a larger population of studies, we built random-effects models.
Estimating the overall effects was done in separate three-level intercept-only models. Effect sizes were weighted by the inverse of their variance (i.e., sampling error), so that effect sizes derived from studies using samples of larger size contributed more to the overall effect size estimate than effect sizes derived from studies using samples of smaller size. Next, the significance of the variance distributed on levels 2 and 3 were tested by conducting two separate one-tailed log-likelihood ratio tests. In these tests, the deviance of a model in which the variance on either level 2 or level 3 was set to zero, was compared to the deviance of the full model in which level 2 and level 3 variances were freely estimated. In case the level 2 and/or level 3 variance was significant, the distribution of effect sizes was considered to be heterogeneous. This indicates that the effect sizes could not be treated as estimates of one common effect size, and thus, moderator analyses were performed to search for variables that can explain the variance. Potential moderating variables (i.e., study design characteristics, contextual factors, structural elements, and specific intervention practices) were examined by testing them in a three-level meta-analytic model as covariates. In all meta-analytic models, the Knapp and Hartung correction (Knapp and Hartung 2003) was applied, implying that the significance of coefficients was tested using the t- and F- distributions rather than the z-distribution.
The statistical software package R (version 3.2.0) and the metafor package (Viechtbauer 2010) were used to build the 3-level meta-analytic models. We used the syntax as described by Assink and Wibbelink (2016). In all analyses, a 5% significant level was used.
Publication Bias and Sensitivity Analyses
A common problem in conducting a meta-analysis is that studies with nonsignificant or negative results are less likely to be published than studies with positive and significant results. This phenomenon is called publication bias and is often referred to as the ‘file drawer problem’ (Rosenthal 1995). So, the effects extracted from primary studies included in this meta-analysis may not be an adequate representation of the actual effect of child maltreatment interventions. Besides publication bias, the results may be affected by other forms of bias, such as coding or selection bias. Therefore, we examined the degree to which our results were affected by (different forms of) bias by conducting the nonparametric and funnel plot-based trim-and-fill analysis as described by Duval and Tweedie (2000a, b). A funnel plot is a scatter plot of the effect sizes against the effect size’s precision (1 divided by the standard error). In this analysis, the symmetry of the funnel is tested, as the plot would be asymmetric when bias is present. In case of an asymmetric plot, the asymmetry is restored by imputing “missing” effect sizes that are estimated on the basis of existing effect sizes in the data set. Subsequently, a “corrected” overall effect can be estimated in a sensitivity analysis using the data set to which the imputed effect sizes produced by the trim-and-fill algorithm have been added. In this way, the degree to which the results were affected by bias can be made visible.
As we identified seven outlying effect sizes (see above), we performed a sensitivity analysis in which we estimated an overall effect of child maltreatment interventions using the data in which the outlying effect sizes were excluded. In this way, we could determine the degree to which the initially estimated overall effect was robust against outliers in effect sizes. In addition, we estimated the overall effect of child maltreatment interventions excluding the results of pilot/feasibility studies, because these studies are more likely to show an effect that is larger than effects produced by well-powered trials.
Results
Descriptive Characteristics
The present meta-analysis included 130 studies with k = 121 non-overlapping samples, comprising N = 39.044 participants. A total of 352 effect sizes were extracted from all primary studies, which examined the effect of home visitation interventions (k = 50), parent training interventions (k = 29), family-based/multisystemic interventions (k = 17), substance abuse interventions (k = 4), before-school interventions (k = 4), general prevention interventions (k = 4), crisis interventions (k = 3), cognitive behavioral therapy (k = 2), and combined interventions (k = 15). These studies were published between 1977 and 2017 (with 2007 being the median publication year) and were conducted in the USA (k = 93), Europe (k = 11), Canada (k = 6), Australia or New Zealand (k = 6), and in various other countries (k = 5). The characteristics of the studies are presented in “Appendix 1,” including the name of the child maltreatment intervention, publication year, sample size, age of the child at the start of the intervention, study design (RCT or quasi-experimental), and type of families served (risk group, general population, or maltreating parents). The distribution of the moderators for preventive and curative interventions is presented in Table 1.
Overall Effect, Heterogeneity in Effect Sizes, and Sensitivity Analyses
A significant overall effect was found of interventions aimed at preventing or reducing child maltreatment with a Cohen’s d of 0.287; 95% CI [0.226; 0.348], t(351) = 9.209, p < .001 (see Table 2). According to the criteria formulated by Cohen (1988), this effect is small in magnitude. The two log-likelihood ratio tests showed that significant variance was present both at level 2 (χ 2(1) = 178.015, p < .001; one-sided) and level 3 (χ 2(1) = 48.182, p < .001; one-sided) of the meta-analytic model. Of the total variance, 32.8 and 56.1% were distributed at levels 2 and 3, respectively, and 11.1% was the percentage of sampling variance that was calculated using the formula of Cheung (2014, p. 2015).
The results of the trim-and-fill analysis showed that bias may be present in the data, as the distribution of all effect sizes (produced by both preventive and curative interventions) was asymmetrical. Figure 2 shows that a small number of effect sizes had to be imputed in the right side of the funnel to restore its symmetry. In specific, 3 effect sizes from 2 independent studies were added to the data and after re-estimating the overall effect, a slightly higher (Δd = 0.014) significant effect was found (d = 0.301 [95% CI 0.238; 0.365], t(354) = 9.343, p < .001). Besides asymmetry in the distribution of effect sizes, there were a number of effect sizes that seemed to be “outliers” compared with other effect sizes (i.e., the effects in the most right part of Fig. 2). To determine whether and how these “outlying” effect sizes influenced our estimated overall effect, we performed a sensitivity analysis in which we re-estimated an overall effect after excluding 7 effect sizes with a Z score exceeding 3.29 (Tabachnik and Fidell 2013) from the data. The results produced an overall effect of d = 0.257; 95% CI [0.204, 0.311], t(344) = 9.499, p < .001, which is slightly below our initial estimated overall effect (Δd = 0.030). In addition, we estimated the overall effect of all interventions using data without effects derived from the pilot studies (see Table 2). The influence of pilot/feasibility studies on the overall summary effect was only small (d = 0.287 with pilot/feasibility studies and d = 0.278 without pilot/feasibility studies; Δd = 0.009). All three sensitivity analyses showed that the estimated overall effect of d = 0.287 was rather robust.

Funnelplot
Next, we estimated an overall effect of only preventive interventions, and this yielded a Cohen’s d of 0.263; 95% CI [0.197; 0.329], which is a small effect according to the criteria of Cohen (1988). The two log-likelihood ratio tests showed once again that significant variance was present at level 2 (χ 2(1) = 141.121, p < .001; one-sided) and level 3 (χ 2(1) = 45.038, p < .001; one-sided) of the meta-analytic model. Of the total variance, 26.4 and 64.1% were distributed at levels 2 and 3, respectively, and 9.4% was distributed at level 1. As these results indicated substantial heterogeneity in effect sizes, we could test study design and intervention characteristics as potential moderators of the effect of preventive interventions. The estimated overall effect of curative interventions was also significant with a Cohen’s d of 0.364; 95% CI [0.227; 0.502] and was small in magnitude according to Cohen’s criteria. Both the level 2 variance (χ 2(1) = 55.467, p < .001; one-sided) and the level 3 variance (χ 2(1) = 3.975, p = .023; one-sided) were significant, and of the total variance, 21.3, 55.7, and 23.0% were distributed at levels 1, 2, and 3, respectively. So, also for curative interventions, moderator analyses could be performed to examine whether and how the intervention effect was influenced by study design and intervention characteristics.
Moderator Analyses Bivariate Models
Table 3 shows the results of the moderator analyses performed for the preventive interventions, and Table 4 shows the results of the moderator analyses performed for the curative interventions.
Study design characteristics For preventive interventions, a trend significant moderating effect was found for research design (larger effect sizes were found in quasi-experimental designs (d = .374) versus RCTs (d = .226)), and a significant positive moderating effect was found for follow-up period (intervention effects increased as follow-up length increased). For curative interventions, a trend significant negative moderating effect was found for sample size (larger sample sizes yielded smaller effect sizes), and a trend significant negative moderating effect was found for percentage of cultural minorities in samples (higher percentages of minorities yielded smaller effect sizes). A significant effect was found for type of outcome measure (larger effect sizes were found for official reports compared to self-reports of parents).
Contextual factors For preventive interventions, a significant moderating effect was found for the type of intervention: The effect of parent training interventions (d = .428) and substance abuse interventions (d = 1.852) were significantly higher than home visitation interventions (d = .210). The types of preventive interventions that were effective in preventing child maltreatment were: home visitation interventions (d = .210), parent training interventions (d = .428), family-based/multisystemic interventions (d = .343), substance abuse interventions (d = 1.852) and combined interventions (d = .174). Before-school interventions (d = .148), general prevention interventions (d = .024), and crisis interventions (d = .407) did not have a significant effect on preventing child maltreatment (the latter probably due to lack of power). Types of curative interventions that were effective in reducing child maltreatment were home visitation interventions (d = .344; trend significant), parent training interventions (d = .415), family-based/multisystemic interventions (d = 0.346), substance abuse interventions (d = .385; trend significant), and cognitive behavioral therapy (d = .445). Crisis interventions (d = .335) did not have a significant effect on reducing child maltreatment, probably due to lack of power.
Further, the moderator analysis showed that the effect of any of the specific individual interventions did not significantly deviate from the effect of the reference category (i.e., other interventions). Specific individual interventions were tested as a separate category only if the effect of the intervention has been examined in at least two studies. Specific individual interventions with a (trend) significant effect on preventing or reducing child maltreatment were: MST-CAN/BSF (d = .545), Triple P (d = .417), ACT-Parent’s Raising Safe Kids Program (d = .377), and Healthy Start (d = .339).
Structural elements For preventive interventions, higher effect sizes were found for interventions delivered by professionals only (d = .334) compared to interventions delivered by professionals and others (such as paraprofessionals or non-professionals; d = .184). Higher effect sizes were found for interventions with a shorter duration (d = .361 for 0–6 months) compared to interventions with a longer duration (d = −.051 for 7–12 months; d = .236 for 13–24 months (trend significant difference); and d = .190 for longer than 24 months). For curative interventions, none of the structural elements were significantly related to effect size.
Specific interventions practices and delivery techniques For preventive interventions, larger effect sizes were found for interventions focusing on increasing the self-confidence of parents (d = .397 versus d = .229). For curative interventions, larger effect sizes were found for improving parenting skills (d = .430 versus d = .190), improving personal skills of parents (d = .440 versus d = .177; trend significant difference), addressing mental health problems parents (d = .521 versus d = .258; trend significant difference), providing social and/or emotional support (d = .649 versus d = .296), and improving child well-being (d = .539 versus d = .272; trend significant difference). Smaller effect sizes were found for interventions focusing on empowerment (d = .203 versus d = .440; trend significant difference).
Moderator Analyses Multiple Moderator Models
Finally, the moderators that were significant in the bivariate models were tested jointly in a multiple moderator model for preventive and curative interventions separately. In this way, the unique contribution of moderators to the prediction of effect size could be examined (see Tables 5 and 6). In the multiple moderator model for preventive interventions, heterogeneity in intervention effects was particularly explained by follow-up duration, parent training interventions (versus other interventions; trend significant), substance abuse interventions (versus other interventions), and a focus on increasing self-confidence of parents (versus interventions without this focus). In the multiple moderator model for curative interventions, heterogeneity in intervention effects was particularly explained by outcome measure, a focus on improving parenting skills (versus interventions without this focus), and providing social/emotional support (versus interventions without this practice; trend significant). In both models, multicollinearity did not seem to be a problem, since all variance inflation factors were below 1.302 and all tolerance statistics were above 0.768.
Discussion
The aim of the present meta-analysis was to gain insight into components contributing to the effectiveness of child maltreatment interventions. Overall, a small but significant effect was found of interventions aimed at preventing or reducing child maltreatment (d = .287), which is in line with findings of previously conducted meta-analyses on the effect of these interventions (e.g., Geeraerts et al. 2004; Filene et al. 2013; MacLeod and Nelson 2000). The results of the trim-and-fill analysis suggested that bias was present in the data, and therefore, a “corrected” overall effect was estimated, resulting in an effect size of d = 0.301. Because there are several methodological shortcomings regarding the trim-and-fill method (see the Limitations section), this corrected effect size should not be interpreted as a true effect size, but only as an indicator of (possible) bias in the data.
Larger effect sizes were found for curative interventions targeting maltreating parents (d = .364) than for preventive interventions targeting at-risk families/the general population (d = .263), but this difference did not reach significance. Euser et al. (2015) did find a significantly higher effect for interventions aimed at reducing child maltreatment in maltreating families than for interventions aimed at preventing child maltreatment in at-risk families/the general population. The finding that curative interventions are more effective than preventive interventions may be explained by a lower prevalence of child maltreatment in at-risk families/the general population than in maltreating families, making it “more difficult” to find significant differences between intervention and control groups (because of lower statistical power) and consequently, to prove the effectiveness of an intervention. Furthermore, the detection of child maltreatment in the general population/at-risk families is particularly difficult when official records are used, as many maltreatment occurrences are not officially reported to child protection services. So, in primary studies examining the effect of a preventive intervention and in which official records are used produce rather small effect sizes. Therefore, relatively large research groups and long follow-up periods are needed to increase the power. This may also be a possible explanation for the significant effect of the variable follow-up period (higher effect sizes were produced in longer follow-up periods): the longer the follow-up period, the higher the prevalence of child abuse in the research groups, the more likely a possible effect is detected.
Study Design Characteristics
For preventive interventions, higher effect sizes were found for studies with quasi-experimental designs (d = .347) than for RCTs (d = .226; trend significant difference). Previous meta-analyses that included only RCT designs generally showed smaller effect sizes than meta-analysis including both RCTs and quasi-experimental designs, which is in line with the findings of our meta-analysis. For example, Pinquart and Teubert (2010) found a very small effect (d = .13) of RCTs on parenting interventions for families with newborns. Euser et al. (2015) also found a very small effect (d = 0.13) of RCTs on interventions for preventing or reducing child maltreatment. Ultimately, exclusively reviewing RCT studies is desirable, because effects of child maltreatment interventions can best be determined in RCT’s, as random assignment of participants to an experimental and a control group (theoretically) equalizes both groups on all other variables. Therefore, RCT’s are considered to be the most powerful study design in intervention research. However, at present, it is too early for such a review, because only a few RCTs have been performed on the effectiveness of child maltreatment interventions and their components. Consequently, a lot of essential information would be missing in a review of only RCTs and as a result, little knowledge could be obtained about effective components. Additionally, when matching procedures are properly applied in quasi-experimental studies, reasonable control groups can be formed so that generalization of results is quite feasible and realistic.
Further, for preventive interventions, larger positive intervention effects were found at later follow-up than at immediate post-intervention, which may be attributed to sleeper effects of interventions (Maurer et al. 2007). Sleeper effects in the context of child maltreatment interventions imply that positive intervention effects—at least to some extent—need time to emerge after interventions have ended. For example, parents may be unsure about applying newly learned parenting practices in their own home environment without being helped or supervised and, consequently, time passes until parents are able to apply these practices effectively. As soon as parents have practiced and acquired more confidence, the newly learned practices may be reinforced by positive responses of the child, other family members, and/or members of the social network of the family. It takes a considerable amount of time until positive parenting practices sink in with parents, simply because replacing adverse parenting practices and/or beliefs with positive parenting strategies cannot be expected to occur within a short time period. In general, child maltreatment interventions aim for a sustained change in parent–child interactions over time by improving parenting practices and/or beliefs, so that (the recurrence of) child maltreatment is prevented. Therefore, it is important in primary research to thoroughly conduct follow-up evaluations of considerable length, as the true effects of child maltreatment interventions may be particularly expressed in follow-up rather than in post-treatment evaluations.
For curative interventions, a moderating effect was found for type of outcome (smaller effect sizes were found for studies using self-report data obtained from parents compared to studies using official reports). This may be explained by two difficulties that arise when using self-report methods, such as interviews or questionnaires. First, it may be difficult for parents to be honest about the way they raise their children and to admit any neglectful or abusive parenting practices. As a result, parents may give socially desirable answers. Second, parents may be biased toward presenting a more favorable image of their own parenting behavior (see, for instance, Schwarz et al. 1985). Both issues may result in an underestimation of the true number of maltreatment occurrences, which in turn influences the magnitude of effect sizes. On the other hand, it can be assumed that official reports also lead to an underrepresentation of child abuse because researchers found that many occurrences of child maltreatment do not appear in official records (e.g., Fergusson et al. 2000; Finkelhor 2008; MacMillan et al. 2003).
Effective Components
As for intervention duration, we found that preventive interventions with a short duration (up to 6 months) were more effective than preventive interventions of longer duration, whereas for curative interventions, no significant effect of intervention duration was found. This finding is in line with findings of a meta-analysis on effective ingredients of prevention programs for youth at risk for juvenile delinquency, which also showed that preventive interventions of shorter duration were more effective than preventive interventions of longer duration (De Vries et al. 2015). In contrast, Euser et al. (2015) concluded in their meta-analysis that interventions with an average length (6–12 months) were most effective, but this conclusion seems too strong. There was hardly any absolute difference in mean effect between their 0–6 month category (d = .22) and their 6–12 month category (d = .23). The “less is more” effect in attachment-based interventions found by Bakermans-Kranenburg et al. (2003) seems also applicable to interventions aimed at reducing or preventing child maltreatment. However, intervention duration was no longer a significant predictor of effect size in the multiple moderator model, which implies that intervention duration does not make a unique contribution to the prediction of effect size above follow-up duration (in months), and whether or not interventions were a parent training intervention, a substance abuse intervention, and focusing on improving parents’ self-confidence.
Moreover, it seems to be important to adjust the intensity of an intervention to the level of risk present in a family. In case of high risk, it may be important to intervene intensively, whereas in case of low risk, less intensive interventions are appropriate. This principle is known as the risk principle of the risk–need–responsivity (RNR) model (e.g., Andrews and Bonta 2010a, b; Andrews et al. 1990). This model is widely used for preventing recidivism in the (juvenile) criminal justice system, as various meta-analyses have shown that judicial interventions aimed at behavioral change are most effective when delivered according to this model (Andrews et al. 1990; Andrews and Dowden 1999). It can be assumed that the RNR principles also apply to interventions aimed at preventing or reducing child maltreatment, because child maltreatment, like delinquent behavior, is caused by the accumulation of risk factors in multiple systems (Belsky 1980, 1993; Brown et al. 1998). Furthermore, many risk factors of delinquent behavior resemble risk factors for child maltreatment, like poverty, stress in the family, and psychiatric problems of parents, including alcohol or drug problems (Stith et al. 2009).
For preventive interventions, lager effect sizes were found for interventions focusing on increasing self-confidence of parents. For curative interventions, larger effect sizes were found for improving parenting skills, improving personal skills of parents (trend significant), addressing mental health problems of parents (trend significant), providing social and/or emotional support, and improving a child’s well-being (trend significant). These findings offer possibilities to improve interventions. For curative interventions, smaller effect sizes were found for interventions focusing on empowerment (trend significant). This finding is in line with studies reporting that children from high-risk families benefit less from the presence of protective factors (e.g., Luthar and Goldstein 2004; Miller et al. 1999; Vanderbilt-Adriance and Shaw 2008), indicating that interventions aimed at increasing or strengthening protective factors in high-risk families do not necessarily lead to a decrease in child maltreatement. Vanderbilt-Adriance and Shaw (2008) concluded in their review of studies on resilience that in high-risk families, there should be a focus on both strengthening protective factors and reducing risks, because there are limits to the amount of risk that can be mitigated.
Implications for Policy and Clinical Practice
First, when implementing best practices, clinical professionals and policy makers should opt for interventions that produce the largest effects on preventing or reducing child maltreatment. Cognitive behavioral therapy, home visitation, parent training, family-based/multisystemic, substance abuse, and combined interventions were effective in preventing and/or reducing child maltreatment. Specific individual interventions with a (trend) significant effect on preventing or reducing child maltreatment that were examined in at least two independent studies were: MST-CAN/BSF (intensive family therapy), Triple P (a parent training), ACT-Parent’s Raising Safe Kids Program (a short-term parent training), and Healthy Start (a home visitation intervention). Implementing these (types of) interventions in clinical practice may therefore be fruitful.
Second, the effectiveness of existing interventions could be improved by integrating specific components associated with greater effectiveness into interventions, such as focusing on improving parenting skills and providing social and/or emotional support in curative interventions, and increasing self-confidence of parents in preventive interventions. For curative interventions, it seems important to screen for mental health problems in parents and if present, to address these problems in interventions. Interventions targeting substance-abusing parents appeared to be very effective, as well as interventions addressing other mental health problems. Furthermore, improving child well-being and providing social and/or emotional support seems to be effective components of interventions aimed at maltreating families.
Limitations
Several limitations need to be discussed. First, a large amount of literature is available on the effectiveness of interventions aimed at preventing or reducing child maltreatment, and therefore, it is possible that we may have missed primary studies. However, we included a rather large number of studies in our meta-analysis (121 independent studies) and this led us to assume that our sample of studies is representative of all studies on the effect of child maltreatment interventions that have been conducted to date. Second, the reported information of the studies included in the meta-analysis was sometimes limited. A relatively large number of studies failed to report important information on intervention characteristics, such as specific intervention practices and delivery techniques.
A third limitation is related to the outcome measure that was assessed in primary studies. In some studies, it is assumed that a report, investigation, or a recurrence in child protection is indicative of abuse or neglect. However, the relationship between contact with the child protection system and maltreatment is not straightforward (Jenkins et al. 2017). Several studies showed that a large proportion of child maltreatment is not reported to child protection authorities (Cyr et al. 2013; Finkelhor et al. 2005, 2009). Population-based surveys showed that rates of maltreatment are more than ten times the rates of substantiated maltreatment in those same jurisdictions (e.g., Fergusson et al. 2000; Finkelhor 2008; MacMillan et al. 2003). Further, in many cases reported to child protection authorities, maltreatment is not substantiated.
Fourth, there are several methodological difficulties regarding the trim-and-fill method. The performance of the trim-and-fill method is limited when effect sizes prove to be heterogeneous (Peters et al. 2007; Terrin et al. 2003). In addition, the application of the trim-and-fill method could mean adding and adjusting for nonexistent effect sizes in response to funnel plots that are asymmetrical, simply because of random variation (Egger et al. 2001). Finally, Nakagawa and Santos (2012) mentioned that this method has originally been designed for meta-analytic reviews in which independence of effect sizes can be assumed. Despite these shortcomings, there is no best method for detecting and handling missing data in meta-analysis, and therefore, the results from the trim and fill method should be interpreted with caution. In the present study, we only used the trim-and-fill method to calculate a “corrected” overall effect. A fifth limitation is that several moderator analyses were based on a rather small number of effect sizes, implying a low statistical power in the moderator analyses. Finally, it should be kept in mind that the present review was mainly based on primary studies that were conducted in Western countries, and in particular the USA. Since countries differ in social and political climate, organization of child welfare health services, and in ethnic and cultural background of clients served by child welfare, it is questionable whether the present results are representative for nonwestern countries.
Despite these limitations, our study provides important knowledge for science and practice. Our findings show that interventions can be effective in preventing or reducing child maltreatment. The results of this meta-analysis can be used to improve existing interventions, for example by integrating effective components in interventions, or by developing new promising interventions comprising of the most effective components.
References
(*References marked with an asterisk were included in the meta-analysis)
*Akai, C. E., Guttentag, C. L., Baggett, K. M., & Noria, C. W. (2008). Enhancing parenting practices of at-risk mothers. Journal of Primary Prevention, 29, 223–242.
Alink, L. R. A., Cicchetti, D., Kim, J., & Rogosch, F. A. (2012). Longitudinal associations among child maltreatment, social functioning, and cortisol regulation. Developmental Psychology, 48, 224–236.
*Andrews, S. R., Blumenthal, J. B., Johnson, D. L., Kahn, A. J., Ferguson, C. J., Lasater, T. M., et al. (1982). The skills of mothering: A study of parent child development centers. Monographs of the Society for Research in Child Development, 47, 1–83.
Andrews, D. A., & Bonta, J. (2010a). The psychology of criminal conduct (4th ed.). Newark: Lexis/Nexis.
Andrews, D. A., & Bonta, J. (2010b). Rehabilitating criminal justice policy and practice. Psychology, Public Policy, and Law, 16, 39–55.
Andrews, D. A., Bonta, J., & Hoge, R. D. (1990a). Classification for effective rehabilitation: Rediscovering psychology. Criminal Justice and Behavior, 17, 19–52.
Andrews, D. A., & Dowden, C. (1999). A meta-analytic investigation into effective correctional intervention for female offenders. Forum on Corrections Research, 11, 18–21.
Andrews, D. A., Zinger, I., Hoge, R. D., Bonta, J., Gendreau, P., & Cullen, F. T. (1990b). Does correctional treatment work? A clinically relevant and psychologically informed meta-analysis. Criminology, 28, 369–404.
*Antle, B. F., Barbee, A. P., Christensen, D. N., & Sullivan, D. J. (2009). The prevention of child maltreatment recidivism through the Solution-Based Casework model of child welfare practice. Children and Youth Services Review, 31, 1346–1351.
*Arancena, M., Krause, M., Pérez, C., Méndez, M. J., Salvatierra, L., Soto, M., et al. (2009). A cost-effectiveness evaluation of a home visit program for adolescent mothers. Journal of Health Psychology, 14, 878–887.
*Armstrong, K. L., & Morris, J. (2000). Promoting secure attachment, maternal mood and child health in a vulnerable population: a randomized controlled trial. Journal of Pediatrics and Child Health, 36, 555–562.
*Asscher, J. J., Hermanns, J., & Deković, M. (2008). Effectiveness of the home-start parenting support program: Behavioral outcomes for parents and children. Infant Mental Health Journal, 29, 95–113.
Assink, M., Van der Put, C. E., Hoeve, M., De Vries, S. L. A., Stams, G. J. J. M., & Oort, F. J. (2015). Risk factors for persistent delinquent behavior among juveniles: A meta-analytic review. Clinical Psychology Review, 42, 47–61. https://doi.org/10.1016/j.cpr.2015.08.002.
Assink, M., & Wibbelink, C. J. M. (2016). Fitting three-level meta-analytic models in R: A step-by-step tutorial. The Quantitative Methods for Psychology, 12(3), 154–174. https://doi.org/10.20982/tqmp.12.3.p154.
Bakermans-Kranenburg, M. J., Van Ijzendoorn, M. H., & Juffer, F. (2003). Less is more: meta-analyses of sensitivity and attachment interventions in early childhood. Psychological Bulletin, 129(2), 195.
*Barnet, B., Duggan, A. K., DeVoe, M., & Burrell, L. (2002). The effect of volunteer home visitation for adolescent mothers on parenting and mental health. Archives of Pediatrics and Adolescent Medicine, 156, 1216–1222.
*Barnet, B., Liu, J., DeVoe, M., Alperovitz-Bichell, K., & Duggan, A. K. (2007). Home visiting for adolescent mothers: Effects on parenting, maternal life course, and primary care linkage. Annals of Family Medicine, 5, 224–232.
*Barth, R. P. (1991). An experimental evaluation of in-home child abuse prevention services. Child Abuse and Neglect, 15, 363–375.
*Barth, R. P., Hacking, S., & Ash, J. R. (1988). Preventing child abuse: An experimental evaluation of the child parent enrichment project. Journal of Primary Prevention, 8, 201–217.
Belsky, J. (1980). Child maltreatment: An ecological integration. American Psychologist, 35(4), 320–335.
Belsky, J. (1993). Etiology of child maltreatment: A developmental ecological analysis. Psychological Bulletin, 114(3), 413–434.
*Berzin, S. C., Cohen, E., Thomas, K., & Dawson, W. C. (2008). Does family group decision making affect child welfare outcomes? Findings from a randomized control study. Child Welfare, 87, 35–54.
*Black, M. M., Nair, P., Kight, C., Wachtel, R., Roby, P., & Schuler, M. (1994). Parenting and early development among children of drug abusing women: Effects of home intervention. Pediatrics, 94, 440–448.
Blase, K., & Fixsen, D. (2013). Core intervention components. Identifying and operationalizing what makes programs work. Washington, DC: Office of Human Services Policy, US Department of Health and Human Services.
*Bouwmeester-Landweer, M. B. R. (2006). Early home visitation in families at risk for child maltreatment (Proefschrift, Universiteit Leiden). Verkregen van https://openaccess.leidenuniv.nl/handle/1887/4396.
*Brayden, R. M., Altemeier, W. A., Dietrich, M. S., Tucker, D. D., Christensen, M. J., McLaughlin, F. J., et al. (1993). A prospective study of secondary prevention of child maltreatment. The Journal of Pediatrics, 122, 511–516.
*Britner, P. A., & Reppucci, N. D. (1997). Prevention of child maltreatment: Evaluation of a parent education program for teen mothers. Journal of Child and Family Studies, 6, 165–175.
*Brooten, D., Kumar, S., Brown., L. P., Butts, P., Finkler, S. A., Bakewell-Sachs, S., et al. (1986). A randomized clinical trial of early hospital discharge and home follow-up of very-low birth-weight infants. The New England Journal of Medicine, 315, 934–939.
Brown, J., Cohen, P., Johnson, J. G., & Salzinger, S. (1998). A longitudinal analysis of risk factors for child maltreatment: Findings of a 17-year prospective study of officially recorded and self-reported child abuse and neglect. Child Abuse and Neglect, 22, 1065–1078.
*Bugental, D. B., Ellerson, P. C., Lin, E. K., Rainey, B., & Kokotovic, A. (2002). A cognitive approach to child abuse prevention. Journal of Family Psychology, 16, 243–258.
*Bugental, D. B., & Schwartz, A. (2009). A cognitive approach to child mistreatment prevention among medically at-risk infants. Developmental Psychology, 45, 284–288.
*Casanueva, C., Martin, S. L., Runyan, D. K., Barth, R. P., & Bradly, R. H. (2008). Parenting services for mothers involved with child protective services: Do they change maternal parenting and spanking behaviors with young children? Children and Youth Services Review, 30, 861–878.
*Casiro, O. G., McKenzie, M. E., McFadyen, L., Shapiro, C., Seshia, M. M., MacDonald, N., et al. (1993). Earlier discharge with community-based intervention for low birth weight infants: A randomized trial. Pediatrics, 92, 128–134.
*Chaffin, M., Funderburk, B., Bard, D., Valle, L. A., & Gurwitch, R. (2011). A combined motivation and parent–child interaction therapy package reduces child welfare recidivism in a randomized dismantling field trial. Journal of Consulting and Clinical Psychology, 79, 84–95.
*Chaffin, M., Silovsky, J. F., Funderburk, B., Valle, L. A., Brestan, E. V., Balachova, et al. (2004). Parent–child interaction therapy with physically abusive parents: Efficacy for reducing future abuse reports. Journal of Consulting and Clinical Psychology, 72, 500–610.
Cheung, M. W. L. (2014). Modeling dependent effect sizes with three-level meta-analyses: A structural equation modeling approach. Psychological Methods, 19, 211–229.
Chorpita, B. F., & Daleiden, E. L. (2009). Mapping evidence-based treatments for children and adolescents: application of the distillation and matching model to 615 treatments from 322 randomized trials. Journal of Consulting and Clinical Psychology, 77, 566–579.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Hillsdale: Lawrence Erlbaum.
*Crampton, D., & Jackson, W. L. (2007). Family group decision making and disproportionality in foster care: a case study. ChildWelfare, 86, 51–69.
*Culp, A. M., Culp, R. E., Hechtner-Galvin, T., Howell, C. S., Saathoff-Wells, T., & Marr, P. (2004). First-time mothers in home visitation services utilizing child development specialists. Infant Mental Health Journal, 25, 1–15.
Cyr, K., Chamberland, C., Clément, M., Lessard, G., Wemmers, J.-A., Collin-Vézina, D., et al. (2013). Polyvictimization and victimization of children and youth: Results from a populational survey. Child Abuse and Neglect, 37(10), 814.
*Dakof, G. A., Cohen, J. B., Henderson, C. E., Duarte, E., Boustani, M., Blackburn, A., et al. (2010). A randomized pilot study of the Engaging Moms Program for family drug court. Journal of Substance Abuse Treatment, 38, 263–274.
Daro, D. (2011). Prevention of child abuse and neglect. In J. E. B. Meyers (Ed.), The APSAC handbook on child maltreatment (3rd ed., pp. 17–37). Thousand Oaks: SAGE Publications.
*Dawe, S., & Harnett, P. (2007). Reducing potential for child abuse among methadone-maintained parents: Results from a randomized controlled trial. Journal of Substance Abuse Treatment, 32, 381–390.
*Dawson, P., Van Doorninck, W. J., & Robinson, J. L. (1989). Effects of home-based, informal social support on child health. Developmental and Behavioral Pediatrics, 10, 63–67.
De Vries, S. L., Hoeve, M., Assink, M., Stams, G. J. J., & Asscher, J. J. (2015). Practitioner review: effective ingredients of prevention programs for youth at risk of persistent juvenile delinquency—recommendations for clinical practice. Journal of Child Psychology and Psychiatry, 56(2), 108–121.
*Dew, B., & Breakey, G. F. (2014). An evaluation of Hawaii’s Healthy Start Program using child abuse hospitalization data. Journal of Family Violence, 29, 893–900.
*Donohue, B., Azrin, N. H., Bradshaw, K., Van Hasselt, V. B., Cross, C. L., Urgelles, J., et al. (2014). A controlled evaluation of Family Behavior Therapy in concurrent child neglect and drug abuse. Journal of Consult Clinical Psychology, 82, 706–720.
*Dubowitz, H., Fiegelman, S., Lane, W. G., & Kim, J. (2009). Pediatric primary care to help prevent child maltreatment: The Safe Environment for Every Kid (SEEK) Model. Pediatrics, 123, 858–864.
*Dubowitz, H., Lane, W. G., Semiatin, J. N., & Magder, L. S. (2012). The SEEK Model of pediatric primary care: Can child maltreatment be prevented in a low-risk population? Academic Pediatrics, 12, 259–268.
*Duggan, A., Caldera, D., Rodriguez, K., Burrel, L., Rohde, C., & Crowne, S. S. (2007). Impact of a statewide home visiting program to prevent child abuse. Child Abuse and Neglect, 31, 801–827.
*Duggan, A., McFarlane, E., Fubby, L., Burrell, L., Higman, S. M., Windham, A., et al. (2004). Randomized trial of a statewide home visiting program: impact in preventing child abuse and neglect. Child Abuse and Neglect, 28, 597–622.
*DuMont, K., Kirkland, K., Mitchell-Herzfeld, S., Ehrhard-Dietzel, S., Rodriguez, M. L., Lee, E., et al. (2011). A randomized trial of Healthy Families New York (HFNY): Does home visiting prevent child maltreatment. Verkregen van https://www.ncjrs.gov/pdffiles1/nij/grants/232945.pdf.
*DuMont, K., Mitchell-Herzfeld, S., Greene, R., Lee, E., Lowenfels, A., Rodriquez, M., et al. (2008). Healthy Families New York (HFNY) randomized trial: Effects on early child abuse and neglect. Child Abuse and Neglect, 32, 295–315.
Durlak, J. A., & Lipsey, M. W. (1991). A practitioner’s guide to meta-analysis. American Journal of Community Psychology, 19, 291–332.
Duval, S., & Tweedie, R. (2000a). A nonparametric ‘trim and fill’ method of accounting for publication bias in meta-analysis. Journal of the American Statistical Association, 95, 89–99.
Duval, S., & Tweedie, R. (2000b). Trim and fill: A simple funnel-plot based method of testing and adjusting for publication bias in meta-analysis. Biometrics, 56, 455–460.
*Easterbrooks, M. A., Jacobs, F. H., Bartlett, J. D., Goldberg, J., Contreras, M. M., Kotake, C., et al. (2012). Initial findings from a randomized, controlled trial of Healthy Families Massachusetts: Early program impacts on young mothers’ parenting. Verkregen van http://www.aws.pewtrusts.org/~/media/legacy/uploadedfiles/pcs_assets/2013/healthyfamiliesmassachusettsreportpdf.pdf.
Egger, M., Davey-Smith, G., & Altman, D. (2001). Systematic reviews in healthcare. London: British Medical Journal Books.
Embry, D. D., & Biglan, A. (2008). Evidence-based kernels: Fundamental units of behavioral influence. Clinical Child and Family Psychology Review, 11, 75–113.
Euser, S., Alink, L. R. A., Stoltenborgh, M., Bakermans-Kranenburg, M. J., & Van Ijzendoorn, M. H. (2015). A gloomy picture: a meta-analysis of randomized controlled trials reveals disappointing effectiveness of programs aiming at preventing child maltreatment. BMC Public Health, 15, 1–14.
*Falconer, M. K., Clark, M. H., & Parris, D. (2011). Validity in an evaluation of Healthy Families Florida—A program to prevent child abuse and neglect. Children and Youth Services Review, 33, 66–77.
Farrington, D. P. (2003). Methodological quality standards for evaluation research. The Annals of the American Academy of Political and Social Science, 587(1), 49–68.
*Fennell, D. C., & Fishel, A. H. (1998). Parent education: an evaluation of STEP on abusive parents’ perceptions and abuse potential. Journal of Child and Adolescent Psychiatric Nursing, 11, 107–120.
Ferguson, G. A. (1966). Statistical analysis in psychology & education (p. 244). New York: McGraw-Hill.
*Fergusson, D. M., Boden, J. M., & Horwood, L. J. (2013). Nine-year follow-up of a home-visitation program: A randomized trial. Pediatrics, 131, 297–303.
*Fergusson, D. M., Grant, H., Horwood, L. J., & Ridder, E. M. (2005). Randomized trial of the Early Start Program of home visitation. Pediatrics, 116, 803–809.
Fergusson, D. M., Horwood, L. J., & Woodward, L. J. (2000). The stability of child abuse reports: a longitudinal study of the reporting behaviour of young adults. Psychological Medicine, 30, 529–544.
Filene, J. H., Kaminski, J. W., Valle, L. A., & Cachet, P. (2013). Components associated with home visiting program outcomes: A meta-analysis. Pediatrics, 132, 100–109.
Finkelhor, D. (2008). Childhood victimization. Violence, crime and abuse in the lives of young people. Oxford: Oxford University Press.
Finkelhor, D., Ormrod, R. K., & Turner, H. A. (2005). The victimization of children and youth: A comprehensive, national survey. Child Maltreatment, 10(1), 5–25.
Finkelhor, D., Ormrod, R. K., & Turner, H. A. (2009). Lifetime assessment of poly-victimization in a national sample of children and youth. Child Abuse and Neglect, 33(7), 403–411.
*Fraser, J. A., Armstrong, K. L., Morris, J. P., & Dadds, M. R. (2000). Home visiting intervention for vulnerable families with newborns: follow-up results of a randomized controlled trial. Child Abuse and Neglect, 24, 1399–1429.
*Fujiwara, T., Kato, N., & Sanders, M. R. (2011). Effectiveness of Group Positive Parenting Program (Triple P) in changing child behavior, parenting style, and parental adjustment: An intervention study in Japan. Journal of Child and Family Studies, 20, 804–813.
*Galanter, R., Self-Brown, S., Valente, R. R., Dorsey, S., Whitaker, D. J., Bertuglia-Haley, M., et al. (2012). Effectiveness of Parent–Child Interaction Therapy delivered to at-risk families in the home setting. Child & Family Behavior Therapy, 34, 177–196.
Geeraerts, L., Van den Noortgate, W., Grietens, H., & Ongehena, P. (2004). The effects of early prevention programs for families with young children at risk for physical child abuse and neglect: A meta-Analysis. Child Maltreatment, 9, 277–291.
*Gershater-Molko, R. N., Lutzker, J. R., & Wesch, D. (2002). Using recidivism data to evaluate project Safecare: Teaching bonding, safety, and health care skills to parents. Child Maltreatment, 7, 277–285.
*Gessner, B. D. (2008). The effect of Alaska’s home visitation program for high-risk families on trends in abuse and neglect. Child Abuse and Neglect, 32, 317–333.
Gilbert, R., Spatz Widom, C., Browne, K., Fergusson, D., Webb, E., & Janson, S. (2008). Child Maltreatment 1: Burden and consequences of child maltreatment in high-income countries. Lancet. https://doi.org/10.1016/S0140-6736(08)61706-7.
*Gray, J. D., Cutler, C. A., Dean, J. G., & Kempe, C. H. (1977). Prediction and prevention of child abuse and neglect. Child Abuse and Neglect, 1, 45–58.
*Green, B. L., Ayoub, C., Dym Barlett, J., Von Ende, A., Furrer, C., Chazan-Cohen, R., et al. (2014a). The effect of Early Head Start on child welfare system involvement: A first look at longitudinal child maltreatment outcomes. Children and Youth Services Review, 42, 127–135.
*Green, B. L., Tarte, J. M., Harrison, P. M., Nygren, M., & Sanders, M. B. (2014b). Results from a randomized trial of the Healthy Families Oregon accredited statewide program: Early program impacts on parenting. Children and Youth Services Review, 44, 288–298.
*Guterman, N. B. (1999). Enrollment strategies in early home visitation to prevent physical child abuse and neglect and the “universal versus targeted” debate: A meta-analysis of population-based and screening-based programs. Child Abuse and Neglect, 23(9), 863–890.
Guterman, N. B., Tabone, J. K., Bryan, G. M., Taylor, C. A., Napoleon-Hanger, C., & Banman, A. (2013). Examining the effectiveness of home-based parent aide services to reduce risk for physical child abuse and neglect: Six-month findings from a randomized clinical trial. Child Abuse and Neglect, 37(8), 566–577.
*Guthrie, K. F., Gaziano, C., & Gaziano, E. P. (2009). Toward better beginnings: Enhancing healthy child development and parent–child relationships in a high-risk population. Home Health Care Management & Practice, 21, 99–108.
*Hans, S. L., Thullen, M., Henson, L. G., Lee, H., Edwards, R. C., & Bernstein, V. J. (2013). Promoting positive mother–infant relationships: A randomized trial of community doula support for young mothers. Infant Mental Health Journal, 34, 446–457.
*Harden, B. J., Sandstrom, H., & Chazan-Cohen, R. (2012). Early Head Start and African American families: Impacts and mechanisms of child outcomes. Early Childhood Research Quarterly, 27, 572–581.
*Harder, J. (2005). Prevention of child abuse and neglect: An evaluation of a home visitation parent aide program using recidivism data. Research on Social Work Practice, 15, 246–256.
*Hardy, J. B., & Streett, R. (1989). Family support and parenting education in the home: an effective extension of clinic-based preventive health care services for poor children. The Journal of pediatrics, 115, 927–931.
*Honig, A. S., & Morin, c. (2001). When should programs for teen parents and babies begin? Longitudinal evaluation of a teen parents and babies program. Journal of Primary Prevention, 21, 447–454.
Hox, J. (2002). Multilevel analysis: Techniques and applications. Mahwah: Lawrence Erlbaum Associates.
*Hurlburt, M. S., Nguyen, K., Reid, J., Webster-Stratton, C., & Zhang, J. (2013). Efficacy of the Incredible Years group parent program with families in Head Start who self-reported a history of child maltreatment. Child Abuse and Neglect, 37, 531–543.
*Huxley, P., & Warner, R. (1993). Primary prevention of parenting dysfunction in high-risk cases. American Journal of Orthopsychiatry, 63, 582–588.
*Jacobs, F., Easterbrooks, A., Goldberg, J., Mistry, J., Bumgarnder, E., Raskin, M., et al. (2016). Improving adolescent parenting: Results from a randomized controlled trial of a home visiting program for young families. AJPH Research, 106, 342–349.
*Javier, J. R., Coffey, D. M., Schrager, S. M., Palinkas, L. A., & Miranda, J. (2016). Parenting intervention for prevention of behavioral problems in elementary school-age Filipino-American children: A pilot study in churches. Journal of Developmental and Behavioral Pediatrics, 37, 737–745.
Jenkins, B. Q., Tilbury, C., Mazerolle, P., & Hayes, H. (2017). The complexity of child protection recurrence: The case for a systems approach. Child Abuse and Neglect, 63, 162–171.
*Johnston, B. D., Huebner, C. E., Anderson, M. L., Tyll, L. T., & Thompson, R. S. (2006). Healthy steps in an integrated delivery system: Child and parent outcomes at 30 months. Archives of Pediatric and Adolescent Medicine, 160, 793–800.
*Jones Harden, B., Chazan-Cohen, R., Raikes, H., & Vogel, C. (2012). Early head start home visitation: The role of implementation in bolstering program benefits. Journal of Community Psychology, 40, 438–455.
Jonson-Reid, M., Kohl, P. L., & Drake, B. (2012). Child and adult outcomes of chronic child maltreatment. Pediatrics, 129, 839–845.
*Jouriles, E. N., McDonald, R., Rosenfield, D., Spiller, L., Corbitt-Shindler, D., Norwoodm, W. D., et al. (2010). Improving parenting in families peferred for child maltreatment: A randomized controlled trial examining effects of project support. Journal of Family Psychology, 24, 328–338.
*Kagitcibasi, C., Sunar, D., & Bekman, S. (2001). Long-term effects of early intervention: Turkish low-income mothers and children. Journal of Applied Developmental Psychology, 22, 333–361.
*Kan, M. L., & Feinberg, M. E. (2014). Can a family-focused, transition-to-parenthood program prevent parent and partner aggression among couples with young children? Violence and Victims, 29, 967–980.
*Kirk, R. S., & Griffith, d P. (2004). Intensive family preservation services: Demonstrating placement prevention using event history analysis. Social Work Research, 28, 5–16.
Knapp, G., & Hartung, J. (2003). Improved tests for a random effects meta-regression with a single covariate. Statistics in Medicine, 22, 2693–2710.
*Knox, M., Burkhart, K., & Cromly, A. (2013). Supporting positive parenting in community health centers: The ACT Raising Safe Kids program. Journal of Community Psychology, 41, 395–407.
*Knox, M. S., Burkhart, K., & Hunter, K. E. (2011). ACT against Violence Parents Raising Safe Kids Program: Effects on maltreatment-related parenting behaviors and beliefs. Journal of Family Issues, 32, 55–74.
*Kolko, D. J. (1996). Individual cognitive behavioral treatment an family therapy for physically abused children and their offending parents: A comparison of clinical outcomes. Child Maltreatment, 1, 322–342.
*Lam, W. K., Fals-Stewart, W., & Kelley, M. L. (2009). Parent training with behavioral couples therapy for fathers’ alcohol abuse: Effects on substance use, parental relationships, parenting, and CPS involvement. Child Maltreatment, 14, 243–254.
*Larson, C. P. (1980). Efficacy of prenatal and postpartum home visits on child health and development. Pediatrics, 66, 191–197.
Layzer, J. I., Goodson, B. D., Bernstein, L., & Price, C. (2001). National Evaluation of family support programs. Final report volume A: The meta-analysis.
*Lealman, G. T., Haigh, D., Philips, J. M., Stone, J., & Ord-Smith, C. (1983). Prediction and prevention of child abuse: An empty hope? Lancet, 25, 1423–1424.
*LeCroy, C. W., & Krysik, J. (2011). Randomized trial of the Healthy Families Arizona home visiting program. Children and Youth Services Review, 33, 1761–1766.
*Leijten, P., Overbeek, G., & Janssens, J. M. A. M. (2012). Effectiveness of a parent training program in (pre)adolescence: Evidence from a randomized controlled trial. Journal of Adolescence, 35, 833–842.
*Letarte, M.-J., Normandeau, S., & Allard, J. (2010). Effectiveness of a parent training program “Incredible Years” in a child protection service. Child Abuse and Neglect, 34, 253–261.
*Linares, O. L., Montalto, D., Li, M., & Oza, V. S. (2006). A promising parenting intervention in foster care. Journal of Consulting and Clinical Psychology, 74, 32–41.
Lipsey, M. W., & Wilson, D. B. (2001). Practical meta-analysis. Thousand Oaks: Sage.
*Love, J. M., Kisker, E. E., Ross, C., Raikes, H., Constantine, J., Boller, K., et al. (2005). The effectiveness of early head start for 3-year-old children and their parents: lessons for policy and programs. Developmental Psychology, 41, 885–901.
*Lowell, D. I., Carter, A. S., Godoy, L., Paulicin, B., & Briggs-Gowan, M. J. (2011). A randomized controlled trial of Child FIRST: A comprehensive home-based intervention translating research into early childhood practice. Child Development, 82, 193–208.
Luthar, S. S., & Goldstein, A. (2004). Children’s exposure to community violence: Implications for understanding risk and resilience. Journal of clinical Child and Adolescent Psychology, 33(3), 499–505.
*Lutzker, J. R., & Rice, J. M. (1984). Project 12-ways: Measuring outcome of a large in-home service for treatment and prevention of child abuse and neglect. Child Abuse and Neglect, 8, 519–524.
MacLeod, J., & Nelson, G. (2000). Programs for the promotion of family wellness and the prevention of child maltreatment: A meta-analytic review. Child Abuse and Neglect, 24(9), 1127–1149.
MacMillan, H. L., Jamieson, E., & Walsh, C. A. (2003). Reported contact with child protection services among those reporting child physical and sexual abuse: results from a community survey. Child Abuse and Neglect, 27, 1397–1408.
*MacMillan, H. L., Thomas, B. H., Jamieson, E., Walsh, C. A., Boyle, M. H., Shannon, H. S., et al. (2005). Effectiveness of home visitation by public-health nurses in prevention of the recurrence of child physical abuse and neglect: A randomized controlled trial. Lancet, 365, 1786–1793.
*Marcenko, M. O., & Spence, M. (1994). Home visitation services for at-risk pregnant and postpartum women: a randomized trial. American Journal of Orthopsychiatry, 64, 468–478.
Marcenko, M. O., Spence, M., & Samost, L. (1996). Outcomes of a home visitation trial for pregnant and postpartum women at risk for child placement. Children and Youth Services Review, 18, 243–259.
Maurer, D., Mondloch, C. J., & Lewis, T. L. (2007). Sleeper effects. Developmental Science, 10, 40–47. https://doi.org/10.1111/j.1467-7687.2007.00562.x.
*McKelvey, L. M., Burrow, N. A., Balamurugan, A., Whiteside-Mansell, L., & Plummer, P. (2012). Effects of home visiting on adolescent mothers’ parenting attitudes. American Journal of Public Health, 102, 1860–1862.
*Mejdoubi, J., Van den Heijkant, S. C. C. M., Van Leerdam, F. J. M., Heymans, M. W., Crijnen, A., & Hirasing, R. A. (2015). The effect of VoorZorg, the Dutch Nurse- Family Partnership, on child maltreatment and development: A randomized controlled trial. PLoS ONE, 10, 1–14.
Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., et al. (2013). The behaviour change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behaviour change interventions. Annals of Behavioral Medicine, 46(1), 81–95.
Miller, L. S., Wasserman, G. A., Neugebauer, R., Gorman-Smith, D., & Kamboukos, D. (1999). Witnessed community violence and antisocial behavior in high-risk, urban boys. Journal of Clinical Child Psychology, 28, 2–11.
Minkovitz, C. S., Hughart, N., Strobino, D., Scharfstein, D., Grason, H., Hou, W., et al. (2003). A practice-based intervention to enhance quality of care in the first 3 years of life: The Healthy Steps for Young Children Program. The Journal of the American Medical Association, 290, 3081–3091.
*Minkovitz, C. S., Strobino, D., Mistry, K. B., Scharfstein, D. O., Grason, H., Hou, W., et al. (2007). Healthy Steps for Young Children: sustained results at 5.5 years. Pediatrics, 120, 658–668.
*Nair, P., Schuler, M. E., Black, M. M., Kettinger, L., & Harrington, D. (2003). Cumulative environmental risk in substance abusing women: early intervention, parenting stress, child abuse potential and child development. Child Abuse and Neglect, 27, 997–1017.
Nakagawa, S., & Santos, E. S. A. (2012). Methodological issues and advances in biological meta-analysis. Evolutionary Ecology, 26(5), 1253–1274.
*Norr, K. F., Crittenden, K. S., Lehrer, E. L., Reyes, O., Boyd, C. B., Nacion, K. W., et al. (2003). Maternal and infant outcomes at one year for a nurse-health advocate home visiting program serving African Americans and Mexican Americans. Public Health Nursing, 20, 190–203.
*Olds, D. L., Eckenrode, J., Henderson, C. R., Kitzman, H., Powers, J., Cole, R., et al. (1997). Long-term effects of home visitation on maternal life course and child abuse and neglect: Fifteen-year follow-up of a randomized trial. JAMA, 278, 637–643.
*Olds, D. L., Henderson, C. R., Chamberlin, R., & Tatelbaum, R. (1986). Preventing child abuse and neglect: A randomized trial of nurse home visitation. Pediatrics, 78, 65–78.
*Olds, D. L., Henderson, C. R., & Kitzman, H. (1994). Does prenatal and infancy nurse home visitation have enduring effects on qualities of parental caregiving and child health at 25 to 50 months of life? Pediatrics, 93, 89–98.
*Oveisi, S., Ardabili, H. E., Dadds, M. R., Majdzadeh, R., Mohammadkhani, P., Rad, J. A., et al. (2010). Primary prevention of parent-child conflict and abuse in Iranian mothers: A randomized-controlled trial. Child Abuse and Neglect, 34, 206–213.
*Paradis, H. A., Sandler, M., Todd Manly, J., & Valentine, L. (2013). Building Healthy Children: Evidence-based home visitation integrated with pediatric medical homes. Pediatrics, 132, 174–179.
*Pataki, G. E., & Johnson, J. A. (2005). Evaluation of Healthy Families New York (HFNY): First year program impacts. Verkregen van http://www.ocfs.state.ny.us/main/prevention/assets/HFNY_FirstYearProgramImpacts.pdf.
*Pennell, J., & Burford, G. (2000). Family group decision making: Protecting children and women. Child welfare, 79, 131–158.
Peters, J. L., Sutton, A. J., Jones, D. R., Abrams, K. R., & Rushton, L. (2007). Performance of the trim and fill method in the presence of publication bias and between-study heterogeneity. Statistics in Medicine, 26(25), 4544–4562.
*Peterson, L., Tremblay, G., Ewigman, B., & Saldana, L. (2003). Multilevel selected primary prevention of child maltreatment. Journal of Consulting and Clinical Psychology, 71, 601–612.
Pinquart, M., & Teubert, D. (2010). Effects of parenting education with expectant and new parents: A meta-Analysis. Journal of Family Psychology, 24, 316–327.
*Portwood, S. G., Lambert, R. G., Abrams, L. P., & Nelson, E. B. (2011). An evaluation of the Adults and Children Together (ACT) against violence parents raising safe kids program. The Journal of Primary Prevention, 32, 147–160.
*Posthumus, J. A., Raaijmakers, M. A., Maassen, G. H., Van Engeland, H., & Matthys, W. (2012). Sustained effects of Incredible Years as a preventive intervention in preschool children with conduct problems. Journal of Abnormal Child Psychology, 40, 487–500.
*Puffer, E. S., Green, E. P., Chase, R. M., Sim, A. L., Zayzay, J., Friis, E., et al. (2015). Parents make the difference: A randomized-controlled trial of a parenting intervention in Liberia. Global Mental Health, 2, 1–13.
*Reynolds, A. J., & Robertson, D. L. (2003). School–based early intervention and later child maltreatment in the Chicago longitudinal study. Child Development, 74, 3–26.
*Rodrigo, M. J., Maiquez, M. L., Correa, A. D., Martin, J. C., & Rodriguez, G. (2006). Outcome evaluation of a community center-based program for mothers at high psychosocial risk. Child Abuse and Neglect, 30, 1049–1064.
*Rodriguez, M. L., Dumont, K., Mitchell-Herzfeld, S. D., Walden, N. J., & Greene, R. (2010). Effects of Healthy Families New York on the promotion of maternal parenting competencies and the prevention of harsh parenting. Child Abuse and Neglect, 34, 711–723.
Rosenthal, R. (1994). Parametric measures of effect size. In H. Cooper & L. V. Hedges (Eds.), The Handbook of Research Synthesis (p. 239). New York: Sage.
Rosenthal, R. (1995). Writing meta-analytic reviews. Psychological Bulletin, 118, 183–192.
*Runyon, M. K., Deblinger, E., & Steer, R. A. (2010). Group cognitive behavioral treatment for parents and children at-risk for physical abuse: An initial study. Child & Family Behavior Therapy, 32, 196–218.
*Sanders, M. R., Baker, S., & Turner, K. M. T. (2012). A randomized controlled trial evaluating the efficacy of Triple P Online with parents of children with early-onset conduct problems. Behaviour Research and Therapy, 50, 675–684.
*Sanders, M. R., Pidgeon, A. M., Gravestock, F., Connors, M. D., Brown, S., & Young, R. W. (2004). Does parental attributional retraining and anger management enhance the effects of the Triple P-Positive Parenting Program with parents at risk of child maltreatment? Behavior Therapy, 35, 513–535.
*Sawasdipanich, N., Srisuphan, W., Yenbut, J., Tiansawad, S., & Humphreys, J. (2010). Effects of a cognitive adjustment program for Thai parents. Nursing and Health Sciences, 12, 1–8.
*Schaeffer, C. M., Swenson, C. C., Tuerk, E. H., & Henggeler, S. W. (2013). Comprehensive treatment for co-occurring child maltreatment and parental substance abuse: Outcomes from a 24-month pilot study of the MST-Building Stronger Families program. Child Abuse and Neglect, 37, 596–607.
*Schilling, S., French, B., Berkowitz, S. J., Dougherthy, S. L., Scribano, P., & Wood, J. N. (2017). Child–Adult Relationship Enhancement in Primary Care (PriCARE): A randomized trial of a parent training for child behavior problems. Academic Pediatrics, 17, 53–60.
*Scholer, S. J., Hamilton, E. C., Johnson, M. C., & Scott, T. A. (2010). A brief intervention may affect parents’ attitudes toward using less physical punishment. Family & Community Health, 33, 106–116.
*Schuler, M. E., Nair, P., Black, M. M., & Kettinger, L. (2000). Mother–infant interaction: effects of a home intervention and ongoing maternal drug use. Journal of Clinical Child Psychology, 29(3), 424–431.
Schwarz, J. C., Barton-Henry, M. L., & Pruzinsky, T. (1985). Assessing child-rearing behaviors: A comparison of ratings made by mother, father, child, and sibling on the CRPBI. Child development, 56, 462–479.
*Shapiro, C. J., Kilburn, J., & Hardin, J. W. (2014). Prevention of behavior problems in a Selected population: Stepping Stones Triple P for parents of young children with disabilities. Research in Developmental Disabilities, 35, 2958–2975.
*Siegel, E., Bauman, K. E., Schaefer, E. S., Saunders, M. M., & Ingram, D. D. (1980). Hospital and home support during infancy: impact on maternal attachment, child abuse and neglect, and health care utilization. Pediatrics, 66, 183–190.
*Silovsky, J. F., Bard, D., Chaffin, M., Hecht, D., Burris, L., Owara, A., et al. (2011). Prevention of child maltreatment in high-risk rural families: A randomized clinical trial with child welfare outcomes. Children and Youth Services Review, 33, 1435–1444.
*Stevens-Simon, C., Nelligan, D., & Kelly, L. (2001). Adolescents at risk for mistreating their children Part II: A home- and clinic-based prevention program. Child Abuse and Neglect, 25, 753–769.
Stith, S. M., Liu, T., Davies, L. C., Boykin, E. L., Alder, M. C., Harris, J. M., et al. (2009). Risk factors in child maltreatment: A meta-analytic review of the literature. Aggression and Violent Behavior, 14(1), 13–29.
Stoltenborgh, M., Bakermans-Kranenburg, M. J., Alink, L. R. A., & Van Ijzendoorn, M. H. (2014). The prevalence of child maltreatment across the globe: Review of a series of meta-analyses. Child Abuse Review, 24, 37–50.
*Suess, G. J., Bohlen, U., Carlson, E. A., Spangler, G., & Frumentia Maier, M. (2016). Effectiveness of attachment based STEEP™ intervention in a German high-risk sample. Attachment & Human Development, 18, 443–460.
*Sundell, K., & Vinnerljung, B. (2004). Outcomes of family group conferencing in Sweden: A 3-year follow-up. Child Abuse and Neglect, 28, 267–287.
Sweet, M. A., & Appelbaum, M. I. (2004). Is home visiting an effective strategy? A meta-analytic review of home visiting programs for families with young children. Child Development, 75, 1435–1456.
*Swenson, C. C., Schaeffer, C. M., Henggler, S. W., & Faldowski, R. (2010). Multisystemic therapy for child abuse and neglect: A randomized effectiveness trial. Journal of Family Psychology, 24, 497–507.
*Szykula, S. A., & Fleischman, M. J. (1985). Reducing out-of-home placements of abused children: Two controlled field studies. Child Abuse and Neglect, 9, 277–283.
Tabachnik, B. G., & Fidell, L. S. (2013). Using multivariate statistics (6th ed.). Boston: Allyn and Bacon.
Terrin, N., Schmid, C. H., Lau, J., & Olkin, I. (2003). Adjusting for publication bias in the presence of heterogeneity. Statistics in Medicine, 22, 2113–2126.
*Thomas, R., & Zimmer-Gembeck, M. J. (2011). Accumulating evidence for Parent–Child Interaction Therapy in the prevention of child maltreatment. Child Development, 82, 177–192.
*Thomas, R., & Zimmer-Gembeck, M. J. (2012). Parent–Child Interaction Therapy: An evidence-based treatment for child maltreatment. Child Maltreatment, 17, 253–266.
Van den Noortgate, W., López-López, J. A., Marin-Martinez, F., & Sánchez-Meca, J. (2013). Three-level meta-analysis of dependent effect sizes. Behavior Research Methods, 45, 576–594.
Van den Noortgate, W., López-López, J. A., Marin-Martinez, F., & Sánchez-Meca, J. (2014). Meta-analysis of multiple outcomes: A multilevel approach. Behavior Research Methods, 47, 1274–1294.
Vanderbilt-Adriance, E., & Shaw, D. S. (2008). Protective factors and the development of resilience in the context of neighborhood disadvantage. Journal of Abnormal Child Psychology, 36(6), 887–901.
*Velasques, J., Christensen, M. L., & Schommer, B. L. (1984). Part II: Intensive services help prevent child abuse. The American Journal of Maternal/Child Nursing, 9, 113–117.
Viechtbauer, W. (2010). Conducting meta-analyses in R with the metafor package. Journal of Statistical Software, 36, 1–48.
*Wagner, M. M., & Clayton, S. L. (1999). The Parents as Teachers program: Results from two demonstrations. The Future of Children, 9, 91–115.
*Wagner, M. M., Spiker, D., & Linn, M. I. (2002). The effectiveness of the Parents as Teachers program with low-income parents and children. Topics in Early Childhood Special Education, 22, 67–81.
*Walton, E. (1997). Enhancing investigative decisions in child welfare: An exploratory use of intensive family preservation services. Child welfare, 76, 447–461.
*Walton, E. (2001). Combining abuse and neglect investigations with intensive family preservation services: An innovative approach to protecting children. Research on Social Work Practice, 11, 627–644.
*Walton, E., Fraser, M. W., Lewis, R. E., Pecora, P. J., & Walton, W. K. (1992). In-home family-focused reunification: an experimental study. Child welfare, 72, 473–487.
*Weigensberg, E. C., Barth, R. P., & Guo, S. (2009). Family group decision making: A propensity score analysis to evaluate child and family services at baseline and after 36-months. Children and Youth Services Review, 31, 383–390.
*Wesch, D., & Lutzker, J. R. (1991). A comprehensive 5-year evaluation of Project 12-Ways: An ecobehavioral program for treating and preventing child abuse and neglect. Journal of Family Violence, 6, 17–35.
*Wolfe, D. A., Edwards, B., Manion, I., & Koverola, C. (1988). Early intervention for parents at risk of child abuse and neglect: a preliminary investigation. Journal of Consulting and Clinical Psychology, 56, 40–47.
*Wood, S., Barton, K., & Schroeder, C. (1988). In-home treatment of abusive families: Cost and placement at one year. Psychotherapy: Theory Research, Practice, Training, 25, 409–414.
*Zhai, F., Waldfogel, J., & Brooks-Gunn, J. (2013). Estimating the effects of Head Start on parenting and child maltreatment. Children and Youth Services Review, 35, 1119–1129.
Funding
This work was supported by a grant from ZonMw, the Netherlands Organization for Health Research and Development (Grant Number 74110.0001).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None of the authors of this review have any conflicts of interest to declare.
Ethical Approval
This research did not involve human subjects, it did not require consent or assent forms that needed approval by an ethics committee.
Appendix 1
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
van der Put, C.E., Assink, M., Gubbels, J. et al. Identifying Effective Components of Child Maltreatment Interventions: A Meta-analysis. Clin Child Fam Psychol Rev 21, 171–202 (2018). https://doi.org/10.1007/s10567-017-0250-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10567-017-0250-5