
Abstract
Introduction In many Western countries, a vast amount of interventions exist that aim to facilitate return to work (RTW) after sickness absence. These interventions are usually focused on specific target populations such as employees with low back pain, stress-related complaints or adjustment disorders. The aim of the present study is to detect and identify characteristics of RTW interventions that generally facilitate return to work (i.e. in multiple target populations and across interventions). This type of knowledge is highly relevant to policy makers and health practitioners who want to deliver evidence based care that supports the employee’s health and participation in labour. Methods We performed a keyword search (systematic literature review) in seven databases (period: 1994–2010). In total, 23 articles were included and assessed for their methodological quality. The characteristics of the interventions were evaluated as well. Results Early interventions, initiated in the first 6 weeks of the RTW process were scarce. These were effective to support RTW though. Multidisciplinary interventions appeared effective to support RTW in multiple target groups (e.g. back pain and adjustment disorders). Time contingent interventions in which activities followed a pre-defined schedule were effective in all physical complaints studied in this review. Activating interventions such as gradual RTW were effective in physical complaints. They have not been studied for people with psychological complaints. Conclusions Early- and multidisciplinary intervention and time-contingent-, activating interventions appear most effective to support RTW.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Work can be beneficial for people’s health, reversing the harmful effects of prolonged sickness absence on the employee’s well-being. Improving the health and well-being of the working age population is critically important for individuals, organizations and society as a whole, in order to secure both higher economic growth and increased social justice [1]. In many Western countries, a large number of interventions exists to facilitate and hasten return to work (RTW) after sickness absence. These interventions include for example cognitive behavioural therapy [2], graded activity [3] and workplace adaptations [4].
Until now, systematic literature reviews that examined which interventions improved RTW, often focused on one diagnosis such as people with low back pain [5] or one intervention type such as interventions initiated by or integrated into the workplace, such as ergonomic work site visits [6]. However, we do not know yet whether and which intervention characteristics are generally effective, and therefore can be included in RTW interventions for multiple target populations. Therefore, the aim of this study is to detect and identify characteristics of RTW interventions that generally facilitate return to work (i.e. in multiple target populations and across interventions). Effective characteristics are part of RTW interventions that facilitate and hasten RTW, and at the same time are absent in interventions that do not facilitate RTW. We define facilitated RTW as either a significant reduction in the cumulate or mean number of (work, calendar or annual) days or weeks of sickness absence (whether or not measured at a certain follow up date) or an increase in work resumption rates (percentage of participants who resumed work partially or fully at a certain follow up date within the study period).
A problem, however, in this study is that standards by which we can classify RTW interventions do not exist yet. Therefore, we developed our own list of characteristics by which we classify the modern interventions that have been developed over the past two decades. This classification is based on earlier research [2, 4, 5] and consultations with other expert researchers. It appeared that modern RTW interventions can be characterized by one or more of the following characteristics:
-
Timing of intervention: early, initiated in the first 6 weeks of absence or not;
-
Care professionals involved: multidisciplinary, including multiple professionals (care providers) from more than one discipline or not;
-
Planning of activities to support RTW: time contingent, in which activities are performed according to a pre-defined schedule or not;
-
Target population: all employees on sickness absence irrespective of their specific medical diagnosis (generic) or only to employees with a specific diagnosis (specific);
-
Character of activities to support RTW: interventions including explicit actions to stimulate the employee to RTW, which are A: whether or not a decision was made as to when and/or how RTW will take place; B: whether or not there was gradual exposure to the workplace; and C: whether or not workplace adaptations were implemented;
-
Intensity: a high (≥10 h divided over multiple sessions), moderate (<10 h divided over multiple sessions) or low intensity (once);
-
Employee and employer role: decision latitude of the employee and/or employer about activities to support medical recovery or RTW and the timing of RTW or no decision latitude of the employee and/or employer.
Knowledge about intervention characteristics that facilitate RTW is highly relevant to the sick and absent employee who wants to consume care that optimally improves his/her health and the employer who aims to reduce productivity losses. Moreover, health, social security and insurance policy makers and practitioners can use this knowledge to deliver evidence based care that supports the employee’s health and labour participation, thereby preventing future care consumption and dependence on benefits.
Methods
Search
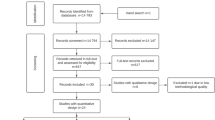
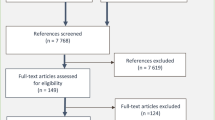
We performed a systematic literature review. First, we searched Pubmed using the MeSH terms ‘absenteeism’, ‘sick leave’, ‘absenteeism AND intervention studies’, ‘sick leave AND intervention studies’. We restricted the first two searches to studies in which the search terms were a ‘major topic’. We searched for articles covering our keywords somewhere in the title, abstract or text body. Table 1 shows the results of this search. Because searching Pubmed using the MeSH terms yielded only 6 relevant studies, we performed a broader keyword search in Pubmed, CINAHL, PsycINFO, Cochrane Library and Google Scholar. We searched all these databases by using various combinations of the following keywords: ‘return to work’, ‘sickness absence’, ‘early’, ‘intervention’, ‘occupational’, ‘work’, ‘training’, ‘low’, ‘back’, ‘pain’, ‘whiplash’, ‘resumption’, ‘disability management’, ‘ergonomic’. Table 1 only shows only those keyword searches that yielded positive results. Titles and/or abstracts were screened until saturation (200 irrelevant hits in a row) was reached. We again searched for articles covering our keywords in the title, abstract or text body. We restricted the Cochrane search to reviews and the Google Scholar Search to the subject areas of Social Sciences, Arts and Humanities.
This procedure covered mostly recent articles, given the fact that the databases presented these first. Studies were included when they:
-
Covered the effectiveness of interventions on RTW;
-
Described interventions tested in a population of workers on sickness absence;
-
Were full text articles;
-
Were written in English and published in the last 16 years (from 1994 to 2010);
-
Were empirical studies or systematic literature reviews.
We included systematic literature reviews to enlarge the body of evidence covered by this study. Such a large body of evidence is needed considering the broad scope of our study subject: to identify intervention characteristics facilitating RTW in multiple target populations (e.g. the employee on sickness absence with low back pain, psychological complaints, physical complaints etcetera). In total, 23 studies (18 quantitative studies and 5 systematic reviews) were included in this review.
We screened all literature lists of systematic literature reviews for overlap with the included empirical studies. In total 2 systematic reviews did not have any overlap with other empirical studies and 3 other reviews showed 3, 6 and 7% overlap with empirical studies. Considering these relatively small percentages, we included both the systematic reviews and the empirical studies. We also searched the literature lists of the systematic reviews for other relevant articles that met the inclusion criteria. This search resulted in the inclusion of one additional empirical study [7].
Analyses
We assessed the methodological quality of all selected articles by means of the rating scheme presented in Table 2. Separate criteria were used for quantitative studies [largely based on 8] and systematic reviews [largely based on 9]. The criteria for quantitative studies are largely based on an existing tool from the Effective Public Health Practice Project [8]. The inter-rater reliability of the final grade assigned by this tool is considered excellent (intra-class correlation coefficient = 0.77, 95% Confidence Interval 0.51–0.90) [10]. We took the methodological quality of the articles into account in our description of effective interventions by attaching more value to the higher-quality studies. In case of inconsistent evidence, we attached more value to the high-quality studies.
As regards the effectiveness of the interventions, data was extracted by reading and summarising articles. We used a standardised form that was developed for the purpose of this study. This form covered a description of the intervention and intervention characteristics, definitions of RTW/sickness absence and findings about the effectiveness of interventions. We included some systematic reviews in our study. We only read the primary studies in case the review article did not provide us all information needed to complete our form for data extraction.
To study the intervention characteristics that improve RTW, we defined several characteristics and developed a rating scheme by which we assessed all studies (Table 3). When descriptions of original studies were insufficient to rate a characteristic, we did not take this study into account in the results for this characteristic. For the systematic literature reviews, we rated whether the characteristics applied to one or more original studies included in those reviews. When this was the case, we took the results of these original studies into account in our results. In case a characteristic such as timing of the start of intervention varied largely across the original studies in the review, we rated this characteristic as neutral.
The search and data analyses were discussed with peers. Please contact the corresponding author for more information about these procedures.
Results
Methodological Quality of the Studies
Table 4 shows the methodological quality of the studies included in this review.
In general, the quantitative studies had moderate to good quality, relating to their designs, study populations, control groups and data analyses. Studies [11–13] were of the best quality because of their longitudinal designs, sufficiently large, heterogeneous study populations and adequate control groups. These studies also provided a complete description of the outcome variables, which also matched study aims. To measure the outcomes, instruments were used that are likely to be accepted by the relevant profession. Data were analysed with advanced techniques such as multilevel regression analyses.
The quality of four of the selected systematic literature reviews was good to very good. Review [14] was of the best quality. This review was based on an adequate research question, good search methods, selection, quality evaluation (and description of this procedure), data extraction and description of original studies. It included a meta-analysis and described potential sources of heterogeneity of studies included in the review.
Intervention Characteristics and Their Effect on RTW
The interventions that were studied as well as their effects on RTW varied largely (Table 5). All interventions were compared to care as usual or a control treatment or to the results of similar studies. In one study, a comparison was made between the number of sickness absence days before and after the intervention in a single group of employees (pre/post test, no control) [15]. This study reduced annual sick leave days for 2 years. We refer to this as a positive effect on RTW.
Table 6 shows the characteristics of each intervention. The interventions are listed in order of the intervention studies’ methodological quality.
Based on Tables 5 and 6 we can describe characteristics of interventions that facilitate RTW:
Timing of intervention: early. Both interventions that started ‘early’ in the RTW process, namely in employees who were absent for 2 weeks [16] and 2–6 weeks of absence [17] facilitated RTW.
Care professionals involved: multidisciplinary. Multidisciplinary interventions included care providers and professionals from multiple disciplines such as general practitioners and physiotherapists [18] employer, case managers, occupational therapists/ergonomists [19], occupational physicians (OPs), occupational physiotherapists, chiropractors, psychologists and social workers having the role of case workers maintaining contact with the workplace and municipal case managers [20], OPs and psychiatrists [12].
Multidisciplinary interventions appeared to support RTW in physical complaints [14, 15, 17–21]. Two high quality studies showed that interventions that included contact with the employer/workplace improved RTW at 12 months follow up in employees with musculoskeletal complaints [19, 20]. The majority of the multidisciplinary interventions in psychological complaints were effective as well [12, 16]. However, one study did not show significant effects of multidisciplinary intervention in psychological complaints [22].
Planning of activities to support RTW: time contingent. In time contingent interventions, activities took place according to a pre-defined time schedule such as a treatment protocol prescribing the total number of sessions and the topics to be addressed in each session. Overall, evidence regarding the effect of time contingent interventions was inconsistent. Some interventions resulted in an earlier RTW [15, 16, 21, 23, 24], while others showed no significant effect on RTW [11, 22, 25]. Findings differed when subgroups are considered. Time contingent interventions were effective in physical complaints [15, 21, 23, 24]. Evidence was inconsistent about the effectiveness of time contingent interventions in psychological complaints. One intervention was effective [16], while two others showed no positive effects [11, 22].
Target population: generic or specific. Evidence regarding the effect of interventions targeted at workers with specific diagnoses such as low back pain or adjustment disorders (specific interventions) was inconsistent. A considerable part of these interventions had a positive effect on RTW [12, 14–21, 23, 24, 26–28]. Other interventions targeted at employees with specific diagnoses had no (significant) effect on RTW [11, 22, 29–31].
Interventions targeted at all absent workers (generic interventions: irrespective of a specific diagnosis) showed no significant effect on RTW [13, 25, 32].
Character of activities to support RTW: interventions including explicit actions to stimulate the employee to RTW. Interventions including actions to stimulate the employee to RTW improved RTW outcomes. All these interventions were evaluated only in employees with physical complaints. For example, interventions including decision making on RTW or RTW as part of the intervention all facilitated RTW [15, 17, 21, 23]. Similarly, interventions covering gradual exposure to the workplace, such as progressively augmented work tasks or partial RTW, had a positive effect on RTW [14, 17, 21]. Finally, interventions including the implementation of work related adaptations, e.g. ergonomic improvements of furniture facilitated RTW [14, 15, 19, 20].
Intensity: high, moderate or low. Evidence regarding high intensity interventions (>10 h divided over multiple sessions) was inconsistent. Some of them facilitated RTW [15, 20, 23], while others had no significant effect [22, 25, 29–31]. Evidence regarding interventions having a moderate (<10 h divided over multiple sessions) low (once) or variable intensity was also inconsistent (Tables 5 and 6).
Employee and employer role: decision authority. In nine studies, the employee and/or employer had decision authority with respect to activities to support medical recovery/RTW and/or actual RTW [11, 16, 20, 22, 24, 25, 29, 31, 32]. For example, the employee had the opportunity to comment on an RTW plan composed by professionals [20]. Often, only the employee and not the employer was given decision authority, for example to decide on (solutions on bottlenecks for) RTW [11, 16, 20, 29, 31, 32]. Evidence regarding the effect of these interventions was inconsistent. Some facilitated RTW [16, 20, 24] while in the majority of the studies no positive effect on RTW was found [11, 22, 25, 29, 31, 32].
Conclusion
The aim of this study was to detect and identify characteristics of RTW interventions that generally facilitate return to work (i.e. in multiple target populations and across interventions). Generally, we found two intervention characteristics that consistently facilitated RTW. Early interventions, that is, interventions initiated in the first 6 weeks of sickness absence, support RTW in multiple target groups. Early interventions appear to be scarce though. Multidisciplinary interventions appear effective to support RTW in physical complaints and in the majority of the studies in employees with psychological complaints. Particularly contact with the employer/workplace improves RTW at 12 months follow up in comparison with usual care for subjects with musculoskeletal complaints.
Moreover, we found two intervention characteristics that were effective in all physical complaints groups: time contingent and activating interventions. Time contingent interventions are effective in physical complaints. Evidence on effectiveness of this characteristic for psychological complaints is somewhat inconsistent. Activating interventions such as gradual RTW are relatively scarce and only found in studies about physical complaints.
Evidence is inconsistent about the effectiveness of interventions targeted at employees with specific diagnoses (although in more than half of the studies with this type of intervention, the results are positive), interventions of varying intensity and interventions covering employee and/or employer decision latitude.
The results of this review show that generic interventions, targeted at all employees on sick leave, irrespective of their diagnoses, show no positive effect.
Discussion
In this study, we focused on characteristics of RTW interventions that generally were effective. The wide range of target populations and interventions may have diluted the more specific findings though. Therefore, we assessed the effectiveness of the intervention characteristics in physical- and psychological complaints separately. It appeared that early and multidisciplinary interventions were effective in both target groups, while for example time contingent interventions were particularly effective for employees with physical complaints.
Our findings showing the general effectiveness of multidisciplinary intervention suggest the importance of cooperation between care professionals and/or case managers and/or employers to for instance align the medical recovery- and RTW process. Particularly contact with the employer/workplace resulted in improved RTW after 12 months follow up [19, 20]. These interventions may help to find mutually desired work adaptations, supporting the employee’s long-term employability. Second, we found that early intervention stimulates early RTW. Researchers found that early intervention has some other effects than early RTW as well. Early intervention was associated with less repeated sickness absence [33]. At the same time, (early return to) work can be beneficial for the employee’s health [34], hence these effects somehow benefit employees and employers alike.
Additionally, we found that there were more interventions for physical complaints than for psychological complaints. Interestingly, interventions in physical complaints were more often effective than those in psychological complaints. This for example applies to time contingent interventions and might be explained by the following. The course of psychological complaints (such as stress-related disorders) might be more instable than that of physical complaints such as low back pain. Therefore, it might be relatively difficult for people with psychological complaints to follow a pre-defined time schedule for intervention. Also, professionals and employers might be less inclined to do so. Further, it might be that RTW professionals and scientists tend to choose physical complaints as a target population to increase their chances of success. Nevertheless, our study results suggest that early and multidisciplinary interventions are generally effective and should be included in all interventions for RTW.
Methodological Reflections
This study has some strengths. We performed a comprehensive methodological quality assessment and description of steps that were taken. These features increased the study’s reliability and validity.
Most previous systematic reviews [7, 17, 27, 28] focused on one specific target population such as back pain. We applied our taxonomy of intervention characteristics to multiple target populations including psychological complaints and musculoskeletal complaints. Our study results regarding early and multidisciplinary intervention hold for multiple target populations. This enhanced our current knowledge of strategies to support RTW.
However, our study also has some limitations. It was not possible to perform a meta-analysis due to heterogeneity of the outcome measure (RTW) as defined in the included studies.
Our study results showed the effectiveness of interventions initiated in the first 6 weeks of the RTW process and multidisciplinary interventions. This conclusion is based on only two early interventions that we included in our review. This may be insufficient to consider the study results to be a theoretical framework. However, our results may indicate some successful strategies to support RTW.
Surprisingly, we found that activating interventions (for example those including a decision about RTW) support RTW in employees with physical complaints, while we did not find such interventions for employees with psychological complaints. Possibly, interventions for employees with psychological complaints tend to activate in other ways than measured in this study (that is: deciding about RTW, gradual exposure to the workplace and/or implemented workplace adaptations). For example, interventions may primarily focus on regaining feelings of control and support subjects’ own responsibility to identify and solve bottlenecks for participation [11, 16].
Our taxonomy may not have detail enough to inform professionals in RTW such as OPs about the exact content of appropriate interventions (for example the content of contacts with the employer). To the authors’ knowledge though, this is the first study that assessed the effect of intervention characteristics on RTW in a systematic way, and may as such be a good starting point for RTW professionals.
Implications for Practice and Research
This review focused on intervention characteristics that facilitate RTW. Our findings have implications for practice and research.
In the first place, the results showed the effectiveness of early interventions and multidisciplinary interventions including contact with the employer. Activating interventions were effective, but only found in physical complaints. Early-, multidisciplinary- and activating interventions should be applied more often, especially in psychological complaints. To start early in the RTW process, general practitioners and OPs need to refer employees and employers to these interventions within the first 6 weeks of the employee’s absence. Interventions should incorporate interdisciplinary cooperation between professionals in health care and contact with the employer. A matrix structure may support this cooperation. It is essential that professionals have enough resources such as time for interdisciplinary contacts. In the Netherlands, the employee and employer have a legal responsibility to cooperate with each other in order to support the employee’s RTW [35]. Researchers and policy makers could study the Dutch situation to find tools for involving the employer in employee RTW. Interventions and other care products should empower both the employee and the employer by incorporating explicit measures to stimulate them to realise RTW.
To know the exact content of successful interventions to support RTW, future studies may focus on detailing our taxonomy of intervention characteristics. Researchers may particularly focus on further detailing the effective intervention characteristics such as appropriate cut-off scores for early intervention and the exact content or intensity of multidisciplinary contact between care providers and employers.
In addition, because we found quite some inconsistent results (e.g. regarding the intensity of the intervention or the involvement of the employer), future research should focus on multifactorial analyses such as meta-analyses. This may help to study which individual or combined intervention characteristics facilitate RTW. Researchers should define RTW precisely and include this single definition as an outcome in any study to increase possibilities for meta-analyses.
In this study, we classified intervention characteristics. Researchers can use our taxonomy to classify the characteristics of RTW interventions in future systematic reviews. This would enable comparison of study results and strengthen the evidence about intervention characteristics that support RTW.
Finally, we found very few early interventions, despite their wide use by professionals (e.g. by many OPs and employers). The gap between research and practice appears to be large. To support evidence-based practice, we advise more cooperation between professionals in practice and research, for example in formulating research questions.
References
Black C. Working for a healthier tomorrow. TSO. 2008. http://www.dwp.gov.uk/docs/hwwb-working-for-a-healthier-tomorrow.pdf. Accessed 9 Dec 2011.
Ektor-Andersen J, Ingvarsson E, Kullendorff M, Orbaek P. High cost-benefit of early team-based biomedical and cognitive-behaviour intervention for long-term pain-related sickness absence. J Rehabil Med. 2008;40:1–8.
Adams A, Ellis T, Stanish WD, Sullivan MJL. Psychosocial factors related to return to work following rehabilitation of whiplash injuries. J Occup Rehabil. 2007;17:305–15.
Ouellette V, Badii M, Lockhart K, Yassi A. Worker satisfaction with a workplace injury prevention and return-to-work program in a large Canadian hospital: the importance of an integrated approach. Work. 2007;28:175–81.
Elders LAM, van der Beek AJ, Burdorf A. Return to work after sickness absence due to back disorders. a systematic review on intervention strategies. Int Arch Occup Environ Health. 2000;73:339–48.
Franche R-L, Cullen K, Clarke J, Irvin E, Sinclair S, Frank J, et al. Workplace-based return-to-work interventions: a systematic review of the quantitative literature. J Occup Rehabil. 2005;15:607–31.
Meijer EM, Sluiter JK, Frings-Dresen MHW. Evaluation of effective return-to-work treatment programs for sick-listed patients with non-specific musculoskeletal complaints: a systematic review. Int Arch Occup Environ Health. 2005;78:523–32.
McMaster University. Faculty of Health Sciences. Quality assessment tool for quantitative studies. In: Effective public health practice project. 2009. http://www.ephpp.ca/images/PDF/QATool.pdf. Accessed 9 Dec 2011.
Cochrane. Formulier Vc voor het beoordelen van een systematische review van observationeel onderzoek [Form Vc for the assessment of a systematic review of observational research]. In: Dutch Cochrane Centre. [date unknown] http://www.cochrane.nl/Files/documents/Checklists/SR-Obs.pdf. Accessed 9 Dec 2011.
Armijo-Olivo S, Stiles CR, Hagen NA, Biondo PD, Cummings GC. Assessment of study quality for systematic reviews: a comparison of the Cochrane collaboration risk of bias tool and the effective public health practice project. Quality assessment tool: methodological research. J Eval Clin Pract. 2010. doi:10.1111/j.1365-2753.2010.01516.x.
Brouwers EPM, Tiemens BG, Terluin B, Verhaak PFM. Effectiveness of an intervention to reduce sickness absence in patients with emotional distress or minor mental disorders: a randomised controlled effectiveness trial. Gen Hospital Psychiatry. 2006;28:223–9.
van der Feldtz-Cornelis C, Hoedeman R, de Jong FJ, Meeuwissen JAC, Drewes HW, van der Laa NC, et al. Faster return to work after psychiatric consultation for sicklisted employees with common mental disorders compared to care as usual. A randomized clinical trial. Neuropsych Dis Treat. 2010;6:375–85.
Mortelmans AK, Donceel P, Lahaye D, Bulterys S. Does enhanced information exchange between social insurance physicians and occupational physicians improve patient work resumption? A controlled intervention study. Occup Environ Med. 2006;63:495–502.
van Oostrom SH, Driessen MT, de Vet HCW, Franche RL, Schonstein E, Loisel P, et al. Workplace interventions for preventing work disability (Review). Cochrane Library. 2009;. doi:10.1002/14651858.CD006955.pub2.
Weiler SW, Foeh KP, van Mark A, Toussaint R, Sonntag N, Gaessler A, et al. Outpatient rehabilitation of workers with musculoskeletal disorders using structured workplace description. Int Arch Occup Environ Health. 2009;82:427–34.
van der Klink, Blonk RWB, Schene AH, van Dijk FJH. Reducing long term sickness absence by an activating intervention in adjustment disorders: a cluster randomised controlled design. J Occup Environ Med. 2003;60:429–37.
Carroll C, Rick J, Pilgrim H, Cameron J, Hillage J. Workplace involvement improves return to work rates among employees with back pain on long-term sick leave: a systematic review of the effectiveness and cost-effectiveness of interventions. Disabil Rehabil. 2010;32:607–21.
Bogefeldt J, Grunnesjö M, Svärdsudd K, Blomberg S. Sick leave reductions from a comprehensive manual therapy programme for low back pain: the Gotland low back pain study. Clin Rehabil. 2008;22:529–41.
Arnetz BB, Sjörgen B, Rydéhn B, Meisel B. Early workplace intervention for employees with musculoskeletal-related absenteeism: a prospective controlled intervention study. J Occup Environ Res. 2003;45:499–506.
Bültmann U, Sherson D, Olsen J, Lysbeck Hansen C, Lund T, Kilsgaard J. Coordinated and tailored work rehabilitation: a randomised controlled trial with economic evaluation undertaken with workers on sick leave due to musculoskeletal disorders. J Occup Rehabil. 2009;19:81–93.
Matheson LN, Brophy RG. Aggressive early intervention after occupational back injury: some preliminary observations. J Occup Rehabil. 1997;7:107–17.
Grossi G, Santell B. Quasi-experimental evaluation of a stress management programme for female county and municipal employees on long-term sick leave due to work-related psychological complaints. J Rehabil Med. 2009;41:632–8.
Marhold C, Linton SJ, Melin L. A cognitive-behavioral return-to-work program: effects on pain patients with a history of long-term versus short-term sick leave. Pain. 2001;91:155–63.
Fleten N, Johnsen R. Reducing sick leave by minimal postal intervention: a randomised, controlled intervention study. J Occup Environ Med. 2006;63:676–82.
Braathen TN, Veiersted KB, Heggenes J. Improved work ability and return to work following vocational multidisciplinary rehabilitation of subjects on long-term sick leave. J Rehabil Med. 2007;39:493–9.
Godges JJ, Anger MA, Zimmerman G, Delitto A. Effects of education on return-to-work status for people with fear-avoidance beliefs and acute low back pain. Phys Ther. 2008;88:231–9.
Norlund A, Ropponen A, Alexanderson K. Multidisciplinary interventions: review of studies of return to work after rehabilitation for low back pain. J Rehabil Med. 2009;41:115–21.
Tveito TH, Hysing M, Eriksen HR. Low back pain interventions at the workplace: a systematic literature review. Occup Med. 2004;54:3–13.
Bakker IM, Terluin B, van Marwijk HWJ, van der Windt DAWM, Rijmen F, van Mechelen W, et al. A cluster-randomised trial evaluating an intervention for patients with stress-related mental disorders and sick leave in primary care. PLoS Clin Trials. 2007;. doi:10.1371/0020026.
Hagen EM, Ødelien KH, Lie SA, Eriksen HR. Adding a physical exercise programme to brief intervention for low back pain patients did not increase return to work. Scand J Public Health. 2010;38:731–8.
Nystuen P, Hagen KB. Solution-focused intervention for sick listed employees with psychological problems or muscle skeletal pain: a randomised controlled trial. BMC Public Health. 2006;16:69.
Drews B, Nielsen CV, Rasmussen MS, Hjort J, Bonde JP. Improving motivation and goal-setting for return to work in a population on sick leave: a controlled study. Scand J Public Health. 2007;35:86–94.
Øyeflaten I, Lie Stein A, Ihlebaeck C, Eriksen HR. Complex patterns for shifting between work and benefits during a 5-year follow-up after work-related rehabilitation!—Need for differentiated interventions? Poster session presented at: EUPHA, Annual Conference of the European Public Health Association; 2010 Nov 10–13; Amsterdam, The Netherlands.
Waddell G, Burton AK. Is work good for your health and well-being? TSO. 2006. http://www.kendallburton.com/Library/downloadpdfs.html. Accessed 9 Dec 2011.
Ministerie van Sociale Zaken en Werkgelegenheid. Ziekteverzuim van het werk. [Sickness absence] Rijksoverheid. [date unknown]. http://www.rijksoverheid.nl/onderwerpen/ziekteverzuim-van-het-werk. Accessed 9 Dec 2011.
Open Access
This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Hoefsmit, N., Houkes, I. & Nijhuis, F.J.N. Intervention Characteristics that Facilitate Return to Work After Sickness Absence: A Systematic Literature Review. J Occup Rehabil 22, 462–477 (2012). https://doi.org/10.1007/s10926-012-9359-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10926-012-9359-z