
Abstract
Background
Squamocellular anal carcinoma is increasingly diagnosed in patients with risk factors.
Methods
State-of-the-art imaging with magnetic resonance imaging (MRI) using phased-array coils and volumetric multidetector computed tomography (CT) provides detailed visualisation of anal disorders, identification and extent assessment of neoplastic tissue, detection and characterisation of nodal and visceral metastases. MRI has been recommended by the European Society for Medical Oncology (ESMO) as the preferred modality of choice to stage anal cancer, taking into account the maximum tumour diameter, invasion of adjacent structures and regional lymph node involvement.
Results
Cross-sectional imaging techniques allow the identification of coexisting complications, and differentiation from other perineal abnormalities.
Conclusion
Cross-sectional imaging is useful for planning radiotherapy, surgical drainage or salvage abdomino-perineal resection. After chemo-radiotherapy, MRI follow-up provides confident reassessment of therapeutic response, persistent or recurrent disease.
Teaching Points
-
• Anal carcinoma is increasingly diagnosed in patients with human immunodeficiency virus (HIV), anoreceptive intercourse, chronic inflammatory bowel disease.
-
• An established association exists with human papillomavirus (HPV) infection and premalignant intra-epithelial dysplasia.
-
• Phased-array MRI is recommended as the preferred imaging modality for regional staging.
-
• Imaging allows detection of infectious complications, planning of radiotherapy or salvage surgery.
-
• Follow-up MRI allows reliable assessment of therapeutic response after chemo-radiotherapy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
An uncommon malignancy in the general population, squamocellular anal carcinoma (SCAC) accounts for approximately 1 % of all gastrointestinal neoplasms and less than 5 % of anorectal tumours. In past decades, SCAC was usually diagnosed at a relatively advanced age with a significant female predominance, and believed to be an indolent disease secondary to chronic irritation. In recent years, similarly to uterine cervix dysplastic changes, oncogenic human papillomavirus (HPV) has been detected in the vast majority (up to 90 %) of invasive SCACs, and linked to the development of low- and high-grade premalignant anal intra-epithelial neoplasms (AIN), particularly with high-risk or multiple HPV serotypes infection [1, 2].
Furthermore, the incidence of SCAC is steadily increasing, particularly in patients with risk factors such as human immunodeficiency virus (HIV) infection, history of anoreceptive intercourse, coexistent cervical dysplasia or cancer, immunosuppression, inflammatory bowel diseases (IBD) and cigarette smoking. Currently, at least half of SCACs occur in relatively young (40–60 years) HIV-positive individuals, most often men who have sex with men (MSM) [3–5].
Regional anatomy and imaging techniques
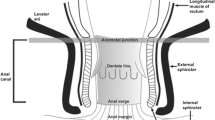
The surgical anus is about 4 cm long from the anorectal junction to the perianal skin on the external anal margin (verge). The internal anal sphincter consisting of smooth muscle is separated from the external, striated muscle sphincter by the fatty intersphincteric space. Along with the puborectalis and levator ani muscles, the external anal sphincter forms the sphincter complex. Located approximately halfway along the anus, the dentate line marks the transition from the squamous epithelium to the intestinal mucosa. Thus, histologically SCACs can be either keratinising or non-keratinising according to their origin below or above the dentate line, although with similar biological behaviour [6, 7].
Lymphatic drainage of anal neoplasms varies according to the primary lesion site. Anal margin and anal canal SCAC originating distal to the dentate line drain to the inguinal and femoral lymph nodes. When the primary tumour arises above the dentate line, regional lymph nodes include the inguinal, internal iliac and perirectal nodes, whereas the external, common iliac and para-aortic nodes are considered non-regional [6–8].
Because of its anatomical location, in most cases SCAC is diagnosed clinically in patients with rectal bleeding, pain, discharge or palpable masses. Alternatively, lesions may be detected during follow-up of high-risk individuals. Following physical examination including digital rectal and vaginal examination, ano-proctoscopy and biopsy, imaging is required to evaluate the local extent of the lesion, lymph node involvement, possible invasion of adjacent organs and distant metastases [6, 9].
Imaging the anal canal and perianal structures may prove technically challenging to perform and interpret. In past years, trans-anal ultrasound (TRUS) and magnetic resonance imaging (MRI) techniques allowed an accurate assessment of tumour size and depth of mural invasion [7, 10, 11]. Unfortunately, in patients with anal lesions, positioning of endoanal sonography probes and MRI coils is hampered by pain and stricture. Trans-anal imaging combines an excellent spatial detail with a limited field-of-view that prevents panoramic assessment of entire ischiorectal spaces and of regional lymph nodes. Furthermore, TRUS has limited specificity for differentiation of residual tumour versus post-treatment fibrosis [11–13].
Currently, MRI performed using external phased-array coils on high-magnetic-field scanners is the imaging modality of choice to investigate the anal region. Significant advantages of MRI include its native multiplanar capability, superior soft-tissue differentiation, biological non-invasiveness and optimal safety profile of gadolinium-based contrast agents. No special patient preparation is needed. Acquisition protocols heavily rely on high-resolution T2-weighted sequences along three planes, with coronal and axial scans planned slightly oblique, respectively parallel and perpendicular to the long axis of the anal canal. Despite the increased tumour conspicuity provided by background fat suppression, short-tau inversion recovery (STIR) sequences are less useful because of limited spatial detail and difficulty to delineate anatomic landmarks. At our Centre, T1-weighted sequences including fat suppression in at least one plane are routinely acquired following standard-dose intravenous gadolinium contrast, to allow detection of lesion enhancement. Conversely, other authors discourage post-contrast MRI acquisitions by stating that enhanced images do not offer additional information to the high soft tissue contrast intrinsic to T2-weighted imaging [7, 10, 13–15].
Although with limited contrast resolution compared with MRI, volumetric multidetector computed tomography (MDCT) acquisitions including image reformations along arbitrary planes allow visualisation of anorectal abnormalities in their cranio-caudal extent with relationship to key anatomical landmarks such as the sphincter complex [16–18].
Imaging features and tumour staging
MRI provides a detailed visualisation of the anal canal and nearby anatomical structures. Although the dentate line is not directly recognisable, its position can be inferred as it corresponds approximately to the upper portion of external sphincter muscles. Sensitivity of TRUS and MRI for the identification of SCAC has been reported to approach 90–100 %, with high concordance regarding tumour size, although on a limited number of patients, and more precise results with ultrasound for smaller, superficial tumours [19].
Neoplastic tissue in the anal canal has low-to-intermediate T1 signal intensity and positive enhancement after intravenous gadolinium contrast. On T2-weighted and STIR sequences, untreated neoplasms display intermediate signal intensity, lower to that of normal ischioanal fat and almost always superior to the internal reference standard represented by uninvolved anal sphincters and gluteal muscles (Figs. 1, 2). Although with limited sensitivity compared with MRI, on CT images SCAC may be detected as solid, enhancing nodules or masses within the anus (Figs. 2, 3). Progressive heterogeneity is observed in larger lesions (Fig. 4) [7, 9, 10, 13].

A 40-year-old MSM with bioptic diagnosis of SCAC. Axial (a) and sagittal (b) T2-weighted images show 2-cm hyperintense nodule contained within the internal sphincter muscle, intensely enhancing as seen on post-contrast fat-suppressed coronal T1-weighted image (c), consistent with T1 tumour (arrowheads)

A 62-year-old female with biopsy-proven SCAC. Axial T2-weighted (a), post-contrast fat-suppressed axial (b) and coronal (c) T1-weighted images, and corresponding enhanced image from body CT (d) show a 5.5-cm long (T3) enhancing tumour with infiltration of the left ischioanal fatty space (arrowheads)

A 57-year-old woman undergoing abdomino-pelvic MDCT for unrelated reasons. Post-contrast axial (a) and coronal reformatted (b) detailed images of the anorectal region identify an unexpected 2-cm right-sided enhancing anal nodule. Subsequent clinical and bioptic assessment confirmed poorly symptomatic ulcerated SCAC

An elderly, 92-year-old man with previous prostatectomy and kidney failure has unenhanced MRI. Sagittal T2- (a) and axial T1-weighted (b) images show 5-cm long solid, inhomogeneous neoplastic tissue (*) extending from the anus to encase the proximal urethra (note catheter in place)
Staging is essential for both prognostic information and correct therapeutic planning, and is performed according to the UICC/AJCC tumour-node-metastasis (TNM) system (Table 1), including local lesion extent, lymph node status and distant metastatic spread. In 2010 the European Society for Medical Oncology (ESMO) recommended MRI as the primary imaging modality to accurately stage SCAC, taking into account the maximum tumour diameter, possible invasion of adjacent organs and nodal involvement [6, 13].
Particular care should be applied to choosing the longest lesion diameter on T2-weighted images, since correct T parameter staging relies on this measure being below 2 cm, over 5 cm or intermediate (Fig. 1) [7, 9, 10, 13].
MRI demonstrates good correlation with physical findings concerning T stage, whereas infiltration of adjacent organs and sometimes tumour size are clinically underestimated. Extramural neoplastic spread may involve the sphincter complex muscles (external sphincter, levator ani and puborectalis) and most commonly occurs towards the anterior urogenital triangle with possible vaginal, urethral or bladder involvement. Sometimes, the tumour may also extend laterally with invasion of the ischioanal fossa (Fig. 2), superiorly to the rectum and mesorectal compartment, or inferiorly to the skin and subcutaneous planes of the perianal region. In such instances, T2-hyperintense solid tissue is seen infiltrating the even more hyperintense fat in the ischiorectal (Fig. 2) and subcutaneous spaces, encasing the lower signal intensity skeletal muscles, or isointense structures such as the vagina (Fig. 5), prostate and urethra (Fig. 4). Notably, radiologists should remember that anal canal carcinoma directly invading the rectal wall, perianal skin, subcutaneous or the sphincter muscle does not imply assessing the tumour stage as T4. For anal margin SCAC, a T4 lesion is defined by invasion of deeper structures such as the skeletal muscle or cartilage [9, 10, 13].

A 32-year-old HIV-positive woman with clinical diagnosis of anovaginal fistula. Axial T2-weighted (a) and post-contrast fat-suppressed axial T1-weighted (b) images show inhomogeneous anal tissue invading the left aspect of the vagina (arrowheads), with internal non-enhancing necrosis and peripheral enhancement. Biopsy diagnosed SCAC with superimposed infection
The incidence of regional nodal involvement increases with primary tumour size. Lymph node metastases may be present (in 25 % of cases) even with superficial (up to T2) SCACs, and are unreliably assessed clinically. Nodal staging evaluation relies on the distance from the primary tumour rather than on the number of involved nodes [6]. MRI is highly helpful to assess lymph node metastatic involvement, although the mere size criterion is far from accurate and associated with both false-positive and false-negative results. Short-axis threshold values of 8 mm, 5 mm and 10 mm have been suggested for pelvic, perirectal and inguinal lymph nodes, respectively. Additional helpful features to increase specificity include loss of the normal bean-shaped morphology and fatty hilum, internal T1 and T2 signal heterogeneity with central necrosis, and inhomogeneous enhancement (Figs. 6, 7) [10, 13].

A 65-year-old woman with history of previously treated small SCAC 3 years earlier. Axial T2- (a) and post-contrast T1-weighted (b) images show roundish 1-cm left inguinal node (arrowheads) with internal fluid-like necrosis and inhomogeneous enhancement, confirmed by ultrasound (c) as hypoechoic with loss of normal nodal structure. Surgical exeresis (postoperative status as seen in d, follow-up MRI) confirmed metastatic node from SCAC

The same patient as in Fig. 2. Axial T2-weighted (a,b) and post-contrast fat-suppressed T1-weighted (c) images show inguinal nodal metastases, larger on left side (arrowheads) plus bilateral enhancing perirectal adenopathies (arrows)
As suggested by ECCO guidelines, search for distant spread is usually performed by means of contrast-enhanced body MDCT, with conventional imaging appearances of liver and lung metastases. Dissemination is very uncommon (less than 5 % of patients at initial diagnosis, and is usually encountered in association with post-treatment recurrence [20]. Alternatively, in immunocompetent patients 18F-fluorodeoxygluocose positron emission tomography (FDG-PET/CT) has high specificity for nodal and visceral dissemination. At diagnosis, FDG-PET/CT may alter staging of anal SCAC in 20 % of patients, leading to inclusion of involved pelvic or inguinal lymph nodes in the radiation field [6, 7].
Complications
In our experience, not infrequently anal tumours coexist with inflammatory conditions such as proctitis and abscesses. In such instances, MDCT and MRI provide confident detection of perirectal inflammatory changes and purulent collections that are differentiated from solid neoplastic tissue, thus allowing a correct therapeutic choice including surgical drainage as necessary (Figs. 5, 8, 9, 10). Resolution of associated inflammatory changes during treatment is easily monitored by cross-sectional imaging (Figs. 9, 10) [15, 21].

A 60-year-old man with AIDS and clinical finding of ulcero-fungating anal mass. Axial (a) and coronal reformatted (b) CT images show moderately heterogeneous tissue (*) in its entire longitudinal extent from the anorectal junction to below the anal verge, associated with large necrotic iliac adenopathies (* in c). Biopsy confirmed superinfected SCAC

A 53-year-old man with purulent drainage and clinical diagnosis of perianal inflammation. Axial images (b,c) from urgent contrast-enhanced MDCT show solid circumferential thickening of the anal canal (arrowheads) associated with abscess collections with mixed gas-fluid content (*) and fistulas crossing the ischioanal space. Surgical examination under anaesthesia including biopsies revealed ulcerated SCAC with superinfection. After surgical drainage and subsequent chemo-radiotherapy, MRI (c) shows complete resolution of both inflammatory and neoplastic changes with residual T2-hypointense fibrotic tracks

A 39-year-old HIV-infected man with biopsy-proven SCAC. Staging MRI confirms left-sided anal thickening (arrowheads) with abnormal T2 signal intensity (a) and strong contrast enhancement (b). Incidentally, two abscess collections with necrotic content and peripheral enhancement are seen ventrally, connected to the anal canal by a fistulous track (arrow in c). Subtotal regression of changes after treatment is seen on follow-up MRI (d)
Furthermore, cross-sectional imaging particularly with MRI also proves useful to differentiate anal carcinoma from other causes of local pain and perineal masses, such as pilonidal sinus diseases, Gartner duct or Bartolini gland cysts, tailgut cysts, uncommon soft-tissue neoplasms, urethral cancer, lymphoma or metastases [14, 22].
Treatment
In the past, SCAC was treated with abdomino-perineal resection and permanent colostomy. Currently, anal margin and small canal tumours without evidence of nodal spread may be successfully excised. In all other cases, the standard treatment includes radiation combined with mitomycin-C plus infusional 5-FU chemotherapy, yielding an 80 % 5-year survival rate with preservation of sphincter function. Advanced T3/T4 tumours have worse outcomes with a 40–68 % 3-year disease-free survival. New neoadjuvant and adjuvant drugs are being investigated to treat advanced disease. Salvage surgery with abdomino-perineal resection is reserved for persistent or recurrent tumours [3, 6, 23–25].
After radio-chemotherapy, imaging follow-up with MRI represents a useful complement to clinical evaluation in the assessment of therapeutic response. Shortly after treatment completion, interpretation of MRI is usually challenging due to the superimposition of inflammatory changes resulting from radiotherapy. Performed at least 6–8 weeks after treatment completion, MRI provides confident, reproducible assessment of post-treatment modifications. Findings indicative of a positive response include size reduction and diminished T2 signal intensity of the treated tumour and associated adenopathies (Figs. 10, 11, 12). The appearance of T2-hypointense signal is consistent with fibrosis, although it does not allow excluding minor residual neoplastic foci for sure (Fig. 13). Size decrease usually becomes evident more than 6 months following treatment. Stability in size and signal intensity of any residual abnormality visible at MRI in the site of the treated lesion 1 year after therapy has been reported to be strongly associated with a favourable outcome. Locoregional and/or distant recurrence occurs in up to 35 % of treated patients, and is strongly associated with advanced (T3–T4) stage and nodal involvement at presentation [7, 20]. Persistent and locally recurrent tumours often display an aggressive behaviour, with possible extensive invasion of the adjacent organs and pelvic bony structures, and a tendency for lymphatic dissemination (Figs. 14) [9, 10, 13].

An 83-year-old man with known SCAC. Initial MRI shows moderate circumferential thickening of the anus with T2-hyperintense signal (a) and contrast enhancement (b) (arrowheads). Complete disappearance of the lesion is observed on axial T2 (c) and post-contrast fat-suppressed T1-weighted (d) images following chemo-radiotherapy

A 46-year-old female patient with biopsy-proven SCAC. MRI staging including axial (a) and coronal (b) T2-weighted images detect a solid, 3-cm eccentric anal mass (arrowhead) consistent with T2 tumour, associated with right inguinal adenopathies with analogous signal features. After chemo-radiotherapy, MRI follow-up (c, d) shows complete disappearance of both anal neoplastic solid tissue and lymphadenopathies

A 46-year-old HIV-infected man with biopsy-proven SCAC. Initially, MDCT (a) shows left-sided thickening with involvement of the external sphincter (arrowheads). After chemo-radiotherapy, lesion regression is observed on MRI with appearance of T2-hypointense fibrosis (*) and hyperintense nodule (arrow) consistent with residual tumour

An elderly, 85-year-old lady with biopsy-proven SCAC and multiple comorbidities. Initial MRI (a,b) shows showed circumferential anal wall thickening with abnormal solid signal (arrowheads) measuring 6 cm in length, plus a suspicious centimetric left inguinal lymph node (arrow in a), findings consistent with T3N2 lesion. After reduced chemo-radiotherapy, follow-up MRI (c, d) 4 months later disclosed progression and partial necrosis of both primary tumour (arrowhead) and inguinal adenopathy (arrow), plus appearance of an exophytic tissue mass protruding from the external anal orifice (* in d)
HIV-associated anal carcinoma
After the introduction of highly active anti-retroviral treatment (HAART), people with HIV infection or acquired immunodeficiency syndrome (AIDS) gained a greatly improved life expectancy with better immune conditions, at the price of an increased tendency to develop tumours. Although it is considered a non-AIDS-defining malignancy, currently SCAC ranks third (8.2 %) among neoplasms observed in HIV/AIDS populations, with a substantially higher incidence in MSMs and in long-standing infected people [4, 26].
Dysplastic intraepithelial lesions are highly prevalent in HIV-infected people, and HIV represents a marker for coinfection with other sexually transmitted diseases such as HPV. Since the risk of developing SCAC increases with the total time elapsed with CD4+ count below 200 cells/μl, it has been hypothesised that HIV-related immune suppression acts as a cofactor to HPV in the development of anal dysplasia and progression to overt carcinoma [1, 3, 4].
Screening procedures including high-resolution anoscopy and cytology smears are increasingly adopted at HIV care centres, to allow detection of SCAC precursors and early-stage tumours amenable to limited excision and topical therapies. Prevention should limit the occurrence of advanced stages at diagnosis in the future [4, 26–29].
A high prevalence (at least 30 %) of anorectal complaints is characteristic of HIV-positive patients, particularly those practicing anoreceptive intercourse. Differential diagnosis encompasses a wide spectrum of abnormalities, including non-specific anal diseases such as haemorrhoids, fissures, fistulas and abscesses, along with venereal infections, viral ulcers, and a non-negligible (7 %) rate of neoplasms such as SCAC, lymphoma and Kaposi’s sarcoma. Therefore, when performing cross-sectional imaging procedures on HIV-infected patients, even for unrelated complaints, special attention should be paid to the anal region, with a focus on the possible identification of solid, enhancing tissue consistent with tumour that indicates need for biopsy (Figs. 5, 8, 10, 13) [21, 30, 31].
Despite initial discouraging reports, in the HAART era HIV-positive patients are likewise treated with standard chemo-radiation regimens, reaching satisfactory results in terms of local control and survival rates, although with increased toxicity and frequent local recurrences [4, 5, 26, 27, 32].
Anal carcinoma in inflammatory bowel diseases
Some literature reports have highlighted the increased risk of anus and lower rectum carcinomas associated with long-standing, severe perianal fistulising Crohn’s disease (CD) (Fig. 15). In patients with CD, SCAC reaches a 14 % proportion among all colorectal cancers, which is ten-times higher than the usual figure. Furthermore, CD patients develop anorectal carcinomas at a younger age (20 years earlier) than the general population. According to the hypothesised pathogenesis, fistulas probably allow HPV an easier access to the epithelial layers, and chronic mucosal regeneration may ultimately lead to neoplastic changes. However, anal tumours may occasionally develop in patients with ulcerative colitis (UC)-related (Fig. 16) or cryptogenetic chronic perianal inflammation [33, 34].

A 40-year-old male patient with long-standing perianal Crohn’s disease, being treated with seton. Contrast-enhanced MDCT images (a, b, c in cranio-caudal order) show right-sided levator ani abscess (*), extensive perianal fistulisation occupying the ischioanal space (arrow), and marked solid-appearing circumferential anorectal thickening (arrowheads). Abdomino-perineal resection for SCAC was performed

A 39-year-old woman with history of ulcerative colitis and perianal inflammation. Initial multiplanar MDCT (a, b) identified enhancing anal thickening (arrowheads) with right-sided vaginal infiltration and solid tissue (*) extending to reach the internal obturator muscle. After biopsy confirmation of SCAC and surgical debulking with colostomy, repeat MDCT (c, d) detected enlarging neoplastic residue (*). Shortly after chemo-radiotherapy, MRI (e) detected the formation of a thick hypointense fibrotic band in the site of the regressed tumour (thin arrows). MRI follow-up (e) identified appearance of a contralateral enhancing tissue band interpreted as suspicious for local recurrence (arrow). After negative clinical reassessment and PET findings, this post-treatment finding remained stable on further MRI studies (not shown)
Diagnosis is often unsuspected or delayed because of pre-existent, unspecific complaints and clinical assessment is hampered by complex inflammation with stricture and local pain. As a result, IBD-associated anal cancers are often advanced at presentation, may require extensive surgery plus chemotherapy and radiotherapy, and are associated with a severe prognosis [34]. Therefore, patients with early-onset or long-standing perianal CD should undergo clinical and imaging surveillance, particularly when new or changed symptoms develop. Radiologists should be aware of the increased risk for anorectal cancer in middle-aged IBD patients, and clearly report any solid tissue as suspicious for neoplasm and suggest biopsy (Figs. 15, 16) [33–35].
Conclusion
The established association with HPV infection and premalignant intra-epithelial dysplastic changes provides insight into the pathogenesis of HIV- and IBD-related anal cancers, and the possibility of prevention or early diagnosis through screening of high-risk individuals [1, 2].
State-of-the-art cross-sectional imaging with high-resolution MRI using external phased-array coils and multiplanar MDCT allow detailed, comprehensive visualisation of abnormalities involving the anus and perineal region. Currently, MRI represents the modality of choice for primary regional staging of SCAC, assessment of complications, of therapeutic response following chemo-radiotherapy, and of possible recurrences [9, 10, 13].
References
Uronis HE, Bendell JC (2007) Anal cancer: an overview. Oncologist 12:524–534
Palefsky J (2008) Human papillomavirus and anal neoplasia. Curr HIV/AIDS Rep 5:78–85
Nagle D (2009) Anal squamous cell carcinoma in the HIV-positive patient. Clin Colon Rectal Surg 22:102–106
Gervaz P, Calmy A, Durmishi Y et al (2011) Squamous cell carcinoma of the anus—an opportunistic cancer in HIV-positive male homosexuals. World J Gastroenterol 17:2987–2991
Maurel J, Fernandez-Martos C, Feliu J et al (2011) SEOM clinical guidelines for the treatment of anal cancer. Clin Transl Oncol 13:525–527
Glynne-Jones R, Northover JM, Cervantes A (2010) Anal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 21(Suppl 5):v87–v92
Kochhar R, Plumb AA, Carrington BM et al (2012) Imaging of anal carcinoma. AJR Am J Roentgenol 199:W335–W344
McMahon CJ, Rofsky NM, Pedrosa I (2010) Lymphatic metastases from pelvic tumors: anatomic classification, characterization, and staging. Radiology 254:31–46
Koh DM, Dzik-Jurasz A, O’Neill B et al (2008) Pelvic phased-array MR imaging of anal carcinoma before and after chemoradiation. Br J Radiol 81:91–98
Parikh J, Shaw A, Grant LA et al (2011) Anal carcinomas: the role of endoanal ultrasound and magnetic resonance imaging in staging, response evaluation and follow-up. Eur Radiol 21:776–785
Drudi FM, Raffetto N, De Rubeis M et al (2003) TRUS staging and follow-up in patients with anal canal cancer. Radiol Med 106:329–337
Rouse HC, Godoy MC, Lee WK et al (2008) Imaging findings of unusual anorectal and perirectal pathology: a multi-modality approach. Clin Radiol 63:1350–1360
Roach SC, Hulse PA, Moulding FJ et al (2005) Magnetic resonance imaging of anal cancer. Clin Radiol 60:1111–1119
Tappouni RF, Sarwani NI, Tice JG et al (2011) Imaging of unusual perineal masses. AJR Am J Roentgenol 196:W412–W420
Hoeffel CC, Azizi L, Mourra N et al (2006) MRI of rectal disorders. AJR Am J Roentgenol 187:W275–W284
Kuhlman JE, Fishman EK (1990) Acute abdomen in AIDS: CT diagnosis and triage. Radiographics 10:621–634
Horton KM, Corl FM, Fishman EK (2000) CT evaluation of the colon: inflammatory disease. Radiographics 20:399–418
Carucci LR, Halvorsen RA (2004) Abdominal and pelvic CT in the HIV-positive population. Abdom Imaging 29:631–642
Otto SD, Lee L, Buhr HJ et al (2009) Staging anal cancer: prospective comparison of transanal endoscopic ultrasound and magnetic resonance imaging. J Gastrointest Surg 13:1292–1298
Klas JV, Rothenberger DA, Wong WD et al (1999) Malignant tumors of the anal canal: the spectrum of disease, treatment, and outcomes. Cancer 85:1686–1693
Nadal SR, Manzione CR, Galvao VM et al (1999) Perianal diseases in HIV-positive patients compared with a seronegative population. Dis Colon Rectum 42:649–654
Hoeffel C, Crema MD, Azizi L et al (2007) Magnetic resonance imaging of the ischiorectal fossa: spectrum of disease. J Comput Assist Tomogr 31:251–257
Meyer J, Willett C, Czito B (2010) Current and emerging treatment strategies for anal cancer. Curr Oncol Rep 12:168–174
Martin FT, Kavanagh D, Waldron R (2009) Squamous cell carcinoma of the anal canal. Surgeon 7:232–237
Lim F, Glynne-Jones R (2011) Chemotherapy/chemoradiation in anal cancer: a systematic review. Cancer Treat Rev 37:520–532
Hammad N, Heilbrun LK, Gupta S et al (2011) Squamous cell cancer of the anal canal in HIV-infected patients receiving highly active antiretroviral therapy: a single institution experience. Am J Clin Oncol 34:135–139
Zanet E, Berretta M, Martellotta F et al (2011) Anal cancer: focus on HIV-positive patients in the HAART-era. Curr HIV Res 9:70–81
Crum-Cianflone NF, Hullsiek KH, Marconi VC et al (2010) Anal cancers among HIV-infected persons: HAART is not slowing rising incidence. AIDS 24:535–543
Lanoy E, Spano JP, Bonnet F et al (2011) The spectrum of malignancies in HIV-infected patients in 2006 in France: the ONCOVIH study. Int J Cancer 129:467–475
Barrett WL, Callahan TD, Orkin BA (1998) Perianal manifestations of human immunodeficiency virus infection: experience with 260 patients. Dis Colon Rectum 41:606–611, discussion 611-602
Yuhan R, Orsay C, DelPino A et al (1998) Anorectal disease in HIV-infected patients. Dis Colon Rectum 41:1367–1370
Munoz-Bongrand N, Poghosyan T, Zohar S et al (2011) Anal carcinoma in HIV-infected patients in the era of antiretroviral therapy: a comparative study. Dis Colon Rectum 54:729–735
Ky A, Sohn N, Weinstein MA et al (1998) Carcinoma arising in anorectal fistulas of Crohn’s disease. Dis Colon Rectum 41:992–996
Sjodahl RI, Myrelid P, Soderholm JD (2003) Anal and rectal cancer in Crohn’s disease. Colorectal Dis 5:490–495
Devon KM, Brown CJ, Burnstein M et al (2009) Cancer of the anus complicating perianal Crohn’s disease. Dis Colon Rectum 52:211–216
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Tonolini, M., Bianco, R. MRI and CT of anal carcinoma: a pictorial review. Insights Imaging 4, 53–62 (2013). https://doi.org/10.1007/s13244-012-0199-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13244-012-0199-3