
Abstract
Introduction
SARS-CoV-2 pneumonia is often associated with hyper-inflammation. The cytokine-storm-like is one of the targets of current therapies for coronavirus disease 2019 (COVID-19). High Interleukin-6 (IL6) blood levels have been identified in severe COVID-19 disease, but there are still uncertainties regarding the actual role of anti-IL6 antagonists in COVID-19 management. Our hypothesis was that the use of sarilumab plus corticosteroids at an early stage of the hyper-inflammatory syndrome would be beneficial and prevent progression to acute respiratory distress syndrome (ARDS).
Methods
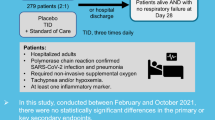
We randomly assigned (in a 1:1 ratio) COVID-19 pneumonia hospitalized patients under standard oxygen therapy and laboratory evidence of hyper-inflammation to receive sarilumab plus usual care (experimental group) or usual care alone (control group). Corticosteroids were given to all patients at a 1 mg/kg/day of methylprednisolone for at least 3 days. The primary outcome was the proportion of patients progressing to severe respiratory failure (defined as a score in the Brescia-COVID19 scale ≥ 3) up to day 15.
Results
A total of 201 patients underwent randomization: 99 patients in the sarilumab group and 102 patients in the control group. The rate of patients progressing to severe respiratory failure (Brescia-COVID scale score ≥ 3) up to day 15 was 16.16% in the Sarilumab group versus 15.69% in the control group (RR 1.03; 95% CI 0.48–2.20). No relevant safety issues were identified.
Conclusions
In hospitalized patients with Covid-19 pneumonia, who were under standard oxygen therapy and who presented analytical inflammatory parameters, an early therapeutic intervention with sarilumab plus standard of care (including corticosteroids) was not shown to be more effective than current standard of care alone. The study was registered at EudraCT with number: 2020-002037-15.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this trial? |
The so-called “cytokine storm” caused by SARS-CoV-2 in some patients is one of the targets of the current therapies for COVID-19. |
In a randomized, placebo-controlled trial, we hypothesized that the early use of anti-Interleukin-6 (IL6) plus corticosteroids would prevent progression to severe respiratory failure (defined as Brescia-COVID scale score ≥ 3) in patients with COVID19 pneumonia and laboratory evidence of hyper-inflammation. |
The role of sarilumab in the treatment of COVID19 remains partially uncertain due to limited published evidence with this medicinal product. |
What was learned from the trial? |
Contrary to recently publications in the field, our study failed to demonstrate the benefit of adding the IL6 antagonist sarilumab to a standard background medication that includes corticosteroids in patients with COVID-19 pneumonia. These results support the need to further investigate and to properly identify the right timing and correct identification of patients with COVID-19 pneumonia that can benefit from IL6 antagonists. |
Introduction
The life-threatening respiratory failure in COVID-19 patients seems to be driven by the inflammatory response to SARS-CoV-2, rather than by direct viral damage [1]. It may seem counterintuitive to treat a viral infection with anti-inflammatory drugs; however, during the second week of disease, when clinical deterioration occurs, viral load has usually fallen significantly [2]. This suggests that damage at that point is produced by the hyper-inflammation and not by the pathogen itself. SARS-CoV-2 replication in epithelial and endothelial cells leads to the production of type I interferon and an influx of neutrophils and macrophages, which in turn produce pro-inflammatory cytokines [3]. In some patients with COVID-19, a pathologic immune cell hyper-activation is triggered by SARS-CoV-2. This so-called “cytokine storm” is one of the targets of the current therapies for COVID-19 [4].
Some familiar drugs have been repurposed for COVID-19 treatment. Tocilizumab is a monoclonal antibody that binds to the interleukin-6 (IL6) receptor. IL6 seems to play a central role in the COVID-19 cytokine storm and the pathogenesis of acute respiratory distress syndrome (ARDS) [5]. Elevated levels of blood IL6 have been identified as a risk factor for severe COVID-19 disease. Tocilizumab is approved for the treatment of cytokine-release syndrome associated with chimeric antigen receptor T cell therapy both in the USA and in the Europe. Preliminary experiences with tocilizumab [6] at the beginning of the pandemic showed promising results that have been recently validated in different clinical trials [7, 8] and metanalysis [9].
Sarilumab is a recombinant human immunoglobulin 1 monoclonal antibody that, like tocilizumab, binds specifically to both soluble and membrane-bound IL6 alfa-receptors and inhibits IL6-mediated signaling. It is approved for the treatment of moderate to severe rheumatoid arthritis. Compared to tocilizumab, it has a 20-fold greater affinity for its target and a longer half-life.
Currently, the WHO recommends treatment with IL-6 inhibitors (tocilizumab or sarilumab) for patients with severe or critical COVID-19 infection [10]. A recent clinical trial showed that tocilizumab and sarilumab are similarly effective at improving survival in patients with severe COVID-19 receiving organ support [11]. Nevertheless, some institutions, such as the National Institutes of Health, recommend sarilumab only when tocilizumab is not available or not feasible to use [12]. The role of sarilumab in the treatment of COVID19 partially remains uncertain and is not as well established as tocilizumab.
In spite of that, several uncertainties regarding the actual role of anti-IL6 antagonists in COVID-19 management still remain [13], and include the optimal timing according to the onset of symptoms and to the degree of inflammation, the effects both beneficial and deleterious when administered together with steroids, and potential differences in efficacy among different IL6 antagonists.
The aim of the present study [14] is to evaluate if an early therapeutic intervention with sarilumab plus standard of care (SOC) may be more effective than current SOC alone, which includes weight-adjusted corticosteroids (CS), in preventing progression to respiratory failure (BRESCIA-COVID ≥ 3) in SARS-CoV-2-infected patients with pneumonia. We also intend to provide data to support the safety of the use of sarilumab in this indication.
Our hypothesis was that the use of IL6 antagonists at an early stage during the hyper-inflammatory syndrome would be beneficial and may avoid progression to ARDS. In accordance to the national guidelines for SOC, we included the use of CS [15] as part of the SOC in the treatment of COVID-19 pneumonia, which will also allow us to address whether anti-IL6 administered concomitantly with CS may potentiate the anti-inflammatory response and lead to better disease outcomes.
Methods
Trial Design
Our clinical trial was a national, multicenter, randomized, open label, controlled clinical study, conducted at eight Spanish tertiary hospitals. The trial was approved by the Spanish Regulatory Authority (Spanish Agency of Medicines and Medical Devices) and by the Research Ethics Committee at Hospital Universitario Puerta de Hierro-Majadahonda (registry number 77/20). The study was conducted in accordance with Good Clinical Practice guidelines and the Declaration of Helsinki. The investigators designed the trial, collected the data, and performed the analysis.
The study was registered at EudraCT with number: 2020-002037-15. Full details of the trial protocol have been published in advance [14], and can be found at the Supplementary Material.
Patients
Patients were eligible for enrollment if they were at least 18 years of age and hospitalized due to COVID-19 confirmed by positive RT-PCR or antigen test, presented pneumonia defined by the radiographic evidence of pulmonary infiltrates by imaging, or rales/crackles on examination, and required standard oxygen supplement due to SpO2 ≤ 94% on room air. Time from symptom onset to inclusion must be at least 7 days and patients must present elevation of IL-6 > 40 pg/mL, or d-dimer > 1.0 mcg/ml, or at least two of the following analytical inflammatory parameters: elevated C-reactive protein (CRP), lactate dehydrogenase (LDH), serum ferritin, or lymphopenia. Patients were excluded if they had high oxygen requirements (including face mask with reservoir bag, non-invasive mechanical ventilation or high flow nasal cannula, or mechanical ventilation), had been on treatment with CS for more than 1 day, were admitted to the intensive care unit (ICU), pregnant or lactating, had allergy or hypersensitivity to sarilumab or CS, had received immunosuppressive monoclonal antibody therapy within the past 5 months, presented AST/ALT values > 10 × ULN, neutropenia (< 0.5 × 109/L), severe thrombocytopenia (< 50 × 109/L), sepsis caused by an alternative pathogen, diverticulitis with risk of perforation, or ongoing infectious dermatitis. The full list of entry criteria is provided in the protocol (Supplementary Material).
Randomization and Treatment
After signing informed consent, participants were randomly assigned in a 1:1 ratio to receive either sarilumab plus SOC (experimental group) or SOC (control group).
Randomization codes were produced by means of the RERAND system integrated within the eCRF system based on Oracle, stratified by center and using blocks multiple of 2 elements. The randomization schedule was managed through the eCRF in a concealed manner.
CS were given to all patients at a 1 mg/kg/day of methylprednisolone for at least 3 days as part of the SOC background medication. Sarilumab was administered intravenously (IV) at a single dose of 200 mg for patients < 75 kg body weight, or 400 mg for patients weighing ≥ 75 kg. SOC also included antibiotic agents, antiviral agents, steroid boluses, vasopressor support, and anticoagulants that were provided at the discretion of the investigators.
Patients in the control group progressing to Brescia-COVID ≥ 2 plus inflammatory parameters were given the option to be rescued with sarilumab at the same weight-adjusted doses. Patients randomly assigned to sarilumab therapy at baseline progressing to Brescia-COVID ≥ 2 were rescued according to local clinical practice protocols.
Efficacy was evaluated at day 15, and patients were followed for a total of 28 days. Patients who were discharged before day 28 had their efficacy/safety follow-up visits conducted by phone call at days 15 and 28.
Outcomes
The primary outcome was the proportion of patients progressing to severe respiratory failure (Brescia-COVID ≥ 3, defined by the need of high frequency nasal ventilation, CPAP or non-invasive ventilation or mechanical ventilation) [16], admission to the ICU, or death. The first version of the protocol proposed as the primary outcome the proportion of patients progressing to Brescia-COVID ≥ 2, but this was amended immediately after the start of the trial to include a more objective definition of respiratory progression. Secondary outcomes were: the proportion of patients progressing to respiratory failure (Brescia-COVID ≥ 2); Brescia-COVID ≥ 3, admission to the ICU or death by day 28; time to progression to severe respiratory failure (defined as Brescia-COVID ≥ 2); time to reduction of supplemental oxygen requirements; time to non-invasive or invasive ventilation; clinical status assessed with the WHO-CPS at days 15 and 28; overall survival; rate of hospital discharge; mortality rate; and adverse events.
The incidence and severity of adverse events were evaluated. These events were categorized according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 5.0.
Statistical Analysis
We estimated that the assignment of 200 patients with a 1:1 randomization would provide an 80.00% power to detect differences in the contrast of the null hypothesis H0: p1 = p2 by means of a bilateral chi-square test for two independent samples, taking into account that the level of significance is 5.00%, and assuming that the proportion of treatment failure in the control group would be 17% and 5% in the experimental group.
The primary analysis follows the intention-to-treat principle and includes all randomized patients. The primary and secondary endpoints were planned to be estimated using the exact chi-square test and a log-binomial regression model including center as a covariate. Survival function was estimated by the Kaplan–Meier method, group comparisons done by log-rank test and the hazard ratios by the Cox model. Missing data due to patients lost to follow up were imputed using the last observation carried forward method. Analysis was performed using SAS® v.9.4 scientific software.
Results
Between 4 August 2020 and 23 March 2021, 201 patients underwent randomization (99 to the experimental group and 102 to the control group). Of them, 98 patients in the experimental group and 101 patients in the control group received the allocated intervention. Overall, 12 patients did not complete the trial (5,97%): 2 patients, 1 in each group, underwent randomization but did not receive the allocated intervention because they withdrew their consent to participate in the study; 5 patients in each group were lost to follow-up (8 after being discharged and 2 after transfer to ICU in a different hospital) (Fig. 1).

Consort flow diagram
Baseline demographic and disease characteristics were evenly distributed across study arms. Median age was 60 years and 70.15% were men. Median time interval between symptoms onset and randomization was 9 days, and 100% of the patients were under standard oxygen therapy (BRESCIA-COVID scale score 1) at the time of randomization and received systemic CS (methylprednisolone mg/kg/day or equivalent) as part of the standard treatment for at least 3 days after being included in the study. Patient’s baseline characteristics are described in Table 1.
Primary Efficacy Outcome
The proportion of patients progressing to severe respiratory failure (Brescia-COVID scale score ≥ 3) at any time from randomization up to day 15 was 16.16% in the sarilumab plus SOC group and 15.69% in the control SOC group (RR 1.03; 95% CI 0.48–2.20) (Table 2).
Secondary Outcomes
The proportion of patients progressing to severe respiratory failure (Brescia-COVID scale score ≥ 3) until day 28 was the same as the proportions seen at day 15. The rate of patients progressing to respiratory failure (Brescia-COVID scale score ≥ 2) at any time until day 15 was 42.42% in the sarilumab plus SOC group compared to 39.22% in the control SOC group (RR, 1.14; 95% CI 0.65–2.00). Mortality by day 28 was 2.02% in sarilumab plus SOC group and 1.96% in the control group (RR, 1.03; 95% CI 0.14–7.46). The proportion of patients admitted at the ICU at any time from randomization until day 28 was 7.07% in the sarilumab plus SOC group versus 9.8% in the control group (RR, 0.7; 95% CI 0.25–1.91) (Table 2). Figure 2 shows time to progression to invasive mechanical ventilation or death.

Progression to VMI or death patients
The median time to hospital discharge over the 28-day period was 7 days (95% CI 6–8) in both treatment arms (hazard ratio, 0.903; 95% CI 0.68–1.21) (Fig. 3).

Time to hospital discharge
Rescue treatment with any IL6 antagonists (sarilumab or tocilizumab) or Interleukin 1 (IL1) antagonists (anakinra) was received by 27 (26.47%) patients in the control group and 18 (18.18%) patients in the experimental group by day 28 (eTable 4, Supplementary Material).
The results of the remaining secondary outcomes are shown in Supplementary Material (eTables 2, 3, eFigures 1, 2, 3, 4).
Subgroup Analyses
No statistically significant differences have been seen in any of the planned subgroup analysis, i.e. by CRP levels (< 75 mg/L, 75–150 mg/L, > 150 mg/L), age (< 70 vs. ≥ 70 years old), gender, sarilumab dose (200 mg vs. 400 mg) (Fig. 4).

Forest plot BRESCIA ≥ 3 by subgroups
Safety
Adverse events are shown in Table 3. No new safety issues for sarilumab + CS emerged. TEAEs with CTCAE grade 3 or higher were reported by 4 (4.04%) patients in the experimental group and 6 patients (5.88%) in the control group. There were 9 treatment related TEAEs in the experimental group and 4 in the control group. No noticeable differences were found in the incidence of any specific adverse event among treatment groups.
Discussion
Our open label, multicenter, randomized, controlled trial included a population of patients admitted to hospital with confirmed COVID-19 pneumonia requiring standard oxygen supplements accompanied by an early increase in inflammatory parameters but not having progressed to clinical deterioration.
In this clinical setting, the early use of the IL6 antagonist sarilumab added to the standard background medication in the participant centers did not result in better clinical outcomes, as measured by the proportion of patients progressing to either severe respiratory failure (Brescia-COVID ≥ 3), ICU admission, or death, at days 15 or 28. Mortality at day 28 did not show statistically significant differences. Consistent lack of significant differences among treatment groups were observed for the remaining secondary endpoints analyzed, including progression of respiratory failure (to Brescia-COVID ≥ 2), time to hospital discharge, proportion of patients admitted at the ICU, or death at days 15 or 28.
Our results are somewhat unexpected in view of the mechanism of action of IL6 antagonists and the observed rapid increase in cytokines that usually accompanies an increase in inflammatory parameters and clinical deterioration in patients with COVID-19 [5]. The results are also unexpected in view of the published favorable results observed with IL6 antagonists [8, 17]. The population of our study included patients with COVID19 pneumonia, which can explain this divergence in comparison with other studies which included more severe patients, such as the RECOVERY trial. More recently, the results of a prospective meta-analysis (PMA) aimed to estimate the efficacy of all IL6 antagonists in the treatment of COVID19 pneumonia [9] have been published. It is worth mentioning that interim results of the SARTRE study as of the data cut-off date, 28 February 2021, with 28-day mortality results for a subset of 140 patients who had completed 28 days of follow up, were included. This PMA, which included a total of 10,930 patients treated with tocilizumab, sarilumab, or siltuximab, and provides a more robust body of evidence, concluded that the administration of IL6 antagonists was associated with lower 28-day all-cause mortality [9]. However, this PMA provides a more marked and precise association of benefit for tocilizumab than for sarilumab, which is attributed to the limited representation of sarilumab studies which included a low use of concomitant corticosteroids. Moreover, a recently published clinical trial which included 420 severe and critical patients with COVID19 did not show efficacy of sarilumab [18].
Our study hypothesis was that the use of IL6 antagonists at an early stage during the hyper-inflammatory syndrome would be beneficial and may avoid progressing to ARDS. However, it might well be that, at such an early stage, the benefit of an anti-inflammatory intervention is already addressed by the effect of CS, which were administered to all patients in both study arms, or that the present study might be underpowered to properly assess the modest benefit of sarilumab in addition to an effective intervention [15]. The first study that demonstrated the beneficial effect of tocilizumab [8] in a population of COVID-19 included patients with an overall more severe clinical status (based on the need of mechanical ventilation and the death rate). Other studies evaluating IL6 antagonists with a small sample size failed to demonstrate any benefit [19,20,21,22]. Existing differences between sarilumab and other IL6 antagonists may also play a role in such differences [9], but this is more debatable after the recent publication (preprint) of a clinical trial, which shows that tocilizumab and sarilumab are similarly effective at improving survival in patients with severe COVID-19 [11].
Lastly, the use of rescue medication (IL6 antagonists or IL1 antagonists) upon progression of respiratory failure was allowed in our study. A total of 27 (26.47%) patients received rescue medication in the control group (mainly sarilumab or tocilizumab) and 18 (18.18%) patients in the experimental group (mainly tocilizumab). It cannot be ruled out that the higher use of rescue medication in the control group might have contributed to dilute any potential benefits of sarilumab. Nevertheless, the results are still valid for the conclusion that the early use of sarilumab does not improve the clinical outcomes in our study population.
The main strength of our study is being the first multicenter, randomized, controlled clinical trial conducted with the IL6 antagonist sarilumab in patients with COVID19 pneumonia and analytical inflammatory parameters, who were under standard oxygen therapy. An additional strength of our study is that the study protocol required that all patients should receive intravenous CS as part of the SOC background medication. At the time of planning the study protocol, the efficacy of CS had not yet been formally demonstrated, but it was extensively used in many centers in Spain, and it was not feasible to include a third treatment arm without CS. The efficacy of CS in the treatment of patients with COVID19 pneumonia and requiring oxygen supplements is now well established, so that our study can respond to the question on whether the addition of the IL6 antagonist sarilumab adds any benefits to an already optimized SOC regimen in the studied population.
Our study has some limitations. The sample size is limited to 201 patients. The small size of the trial might well explain the negative outcomes observed in some of the published clinical trials [9]. The estimate magnitude of the effect of the drug on progression to severe respiratory failure (BRESCIA ≥ 3) from which the sample size was established was very high. At the time of the study design, there was uncertainty about the benefit of CS and, owing to what is currently known, the study might have been underpowered. The study was not blinded due to practical difficulties in having access to the placebo of sarilumab. We addressed this limitation by amending the primary endpoint to include a more stringent and objective definition of progression of respiratory failure, i.e., patients requiring high-flow nasal cannula. Open-label follow up is also a limitation, but, nevertheless, medical decisions to increase oxygen support were taken by different physicians on COVID-19 wards, many of them not investigators of the trial and in all cases following requirements established at local protocols. Despite the multicenter nature of the study, enrolment was largely driven by a single center. Recruiting and conducting an academic clinical trial was an added burden to the clinical investigators that in most of the centers could not count on the support of specialized research units, i.e., Clinical Pharmacology Research Units, as happened to be the case in the top recruiting center. Fluctuations in the pandemic incidence over time posed additional difficulties for a swift recruitment of patients.
Conclusions
Our clinical trial failed to demonstrate any benefits of an early therapeutic intervention with sarilumab when added to an optimized SOC regimen that includes CS in the treatment of hospitalized patients with COVID-19 pneumonia with inflammatory parameters, who were under standard oxygen therapy. No new safety issues were identified. (EudraCT Number: 2020-002037-15).
References
Moore JB, June CH. Cytokine release syndrome in severe COVID-19. Science (80-). 2020;368(6490):473–4. https://doi.org/10.1126/science.abb8925.
Jang S, Rhee J-Y, Wi YM, Jung BK. Viral kinetics of SARS-CoV-2 over the preclinical, clinical, and postclinical period. Int J Infect Dis. 2021;102:561–5.
Cantini F, Goletti D, Petrone L, Najafi Fard S, Niccoli L, Foti R. Immune therapy, or antiviral therapy, or both for covid-19: a systematic review. Drugs. 2020;80(18):1929–46. https://doi.org/10.1007/s40265-020-01421-w.
Fu Y, Cheng Y, Wu Y. Understanding SARS-CoV-2-mediated inflammatory responses: from mechanisms to potential therapeutic tools. Virol Sin. 2020;35(3):266–71. https://doi.org/10.1007/s12250-020-00207-4.
Fajgenbaum DC, June CH. Cytokine storm. N Engl J Med. 2020;383(23):2255–73. https://doi.org/10.1056/NEJMra2026131.
Ruiz-Antorán B, Sancho-López A, Torres F, Moreno-Torres V, de Pablo-López I, García-López P, et al. Combination of tocilizumab and steroids to improve mortality in patients with severe covid-19 infection: a Spanish, multicenter, cohort study. Infect Dis Ther. 2021;10(1):347–62. https://doi.org/10.1007/s40121-020-00373-8.
REMAP-CAP Investigators, Gordon AC, Mouncey PR, Al-Beidh F, Rowan KM, Nichol AD, et al. Interleukin-6 receptor antagonists in critically ill patients with Covid-19. N Engl J Med. 2021;384(16):1491–502.
RECOVERY Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. Lancet (London, England). 2021;397(10285):1637–45.
Shankar-Hari M, Claire L, Vale P, Godolphin PJ, Fisher D, Higgins JPT, Spiga F, et al. Association between administration of IL-6 antagonists and mortality among patients hospitalized for COVID-19. JAMA. 2021;326(6):499–518.
WHO. Therapeutics and COVID19: living guidance. 2021. https://app.magicapp.org/#/guideline/nBkO1E/section/LrV7OL. Accessed 01 Sep 2021.
Investigators TR-C, Derde LPG. Effectiveness of tocilizumab, sarilumab, and anakinra for critically ill patients with COVID-19 the REMAP-CAP COVID-19 immune modulation therapy domain randomized clinical trial. medRxiv. 2021. https://doi.org/10.1101/2021.06.18.21259133v2.
National Institutes of Health. COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. 2021. https://www.covid19treatmentguidelines.nih.gov/. Accessed 01 Sep 2021.
Rubin EJ, Longo DL, Baden LR. Interleukin-6 receptor inhibition in Covid-19: cooling the inflammatory soup. N Engl J Med. 2021;384(16):1564–5.
Caballero Bermejo AF, Ruiz-Antorán B, Cruz AF, Sempere ED, Díaz AC, Rubio EM, et al. Sarilumab versus standard of care for the early treatment of COVID-19 pneumonia in hospitalized patients: SARTRE: a structured summary of a study protocol for a randomised controlled trial. Trials. 2020;21(1):794.
RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. 2021;384(8):693–704. https://doi.org/10.1056/NEJMoa2021436.
Duca A, Piva S, Focà E, Latronico N, Rizzi M. Calculated decisions: Brescia-COVID Respiratory Severity Scale (BCRSS)/algorithm. Emerg Med Pract. 2020;22(5 Suppl):CD1-2.
Rosas IO, Bräu N, Waters M, Go RC, Hunter BD, Bhagani S, et al. Tocilizumab in hospitalized patients with severe Covid-19 pneumonia. N Engl J Med. 2021;384(16):1503–16. https://doi.org/10.1056/NEJMoa2028700.
Lescure F-X, Honda H, Fowler RA, Lazar JS, Shi G, Wung P, et al. Sarilumab in patients admitted to hospital with severe or critical COVID-19: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir Med. 2021;9(5):522–32.
Stone JH, Frigault MJ, Serling-Boyd NJ, Fernandes AD, Harvey L, Foulkes AS, et al. Efficacy of tocilizumab in patients hospitalized with Covid-19. N Engl J Med. 2020. https://doi.org/10.1056/NEJMoa2028836.
Veiga VC, Prats JAGG, Farias DLC, Rosa RG, Dourado LK, Zampieri FG, et al. Effect of tocilizumab on clinical outcomes at 15 days in patients with severe or critical coronavirus disease 2019: randomised controlled trial. BMJ. 2019. https://doi.org/10.1136/bmj.n84.
Salama C, Han J, Yau L, Reiss WG, Kramer B, Neidhart JD, et al. Tocilizumab in patients hospitalized with Covid-19 pneumonia. N Engl J Med. 2021;384(1):20–30. https://doi.org/10.1056/NEJMoa2030340.
Hermine O, Mariette X, Tharaux P-L, Resche-Rigon M, Porcher R, Ravaud P, et al. Effect of tocilizumab vs usual care in adults hospitalized with COVID-19 and moderate or severe pneumonia. JAMA Intern Med. 2021;181(1):32.
Acknowledgements
We thank the participants of the study and all healthcare professionals who helped looking after COVID-19 patients and generating scientific evidence, both in emergency departments and COVID-19 wards in all participating hospitals, in the context of the exceptional burden of the pandemic. SARTRE Study group: HOSPITAL UNIVERSITARIO PUERTA DE HIERRO: Aránzazu Sancho-López, Antonio F Caballero Bermejo, Belén Ruiz-Antorán, Ana Fernández-Cruz, Elena Múñez, Antonio Ramos Martínez, Cristina Avendaño-Solá, Elena Diago-Sempere, Pedro Durán del Campo, Fátima Ibáñez, Alberto Díaz de Santiago, Yolanda Romero, Jorge Calderón Parra, Ilduara Pinto, Gustavo Centeno, Concepción Payares, Almudena Ramírez-García, Laura Javaloyes, María de la Encina Higuera, Rocío Layunta Acero, Laura Vicente, Paloma Rodríguez Araque, Piedad Ussetti-Gil, Rosa Malo de Molina, Andrea Trisan Alonso, Manuel Valle Falconés, Fernando Montoya, María Luisa Jiménez, Laura Ferrer, Jorge Ramos, Alejandro Junco, José Campos, Alejandro Callejas Díaz, Sara de la Fuente Moral, Pedro Laguna, Gema Vázquez Contreras, Alejandro Muñoz Serrano, Isolina Baños Pérez, Víctor Moreno Torres-Concha, Alfonso Ángel-Moreno Maroto, Mª Carmen Máinez Saíz, Esther Montero Hernández, Mª Cruz Carreño Hernández, Rosa Muñoz de Benito, Susana Mellor Pita, Pablo Tutor de Ureta, Miriam Aguilar Pérez, Gema Guadalupe Díaz Nuevo, Christian García Fadul, Beatriz Jara Chinarro, Rosalía Laporta Hernández, María Lázaro Carrasco de la Fuente, Cristina López García Gallo, Patricia Mínguez Clemente, Roberto Carabias Arca, Marta Erro Iribarren, Ane Andrés Eisenhofer, Itziar Diego Yagüe, Ignacio Donate Velasco, Gabriela Escudero López, Esther Expósito Palomo, Amy Galán Gómez, Sonia García Prieto, Javier Gómez Irusta, Edith Vanessa Gutiérrez Abreu, Isabel Gutiérrez Martín, Ángela Gutiérrez Rojas, Andrea Gutiérrez Villanueva, Jesús Herráiz Jiménez, María Martínez Urbistondo, Fernando Martínez Vara, Patricia Mills Sánchez, Alberto Mora Vargas, Ignacio Morrás de la Torre, Enrique Sánchez Chica, Ángela Valencia Alijo, José Manuel Vázquez Comendador, Ana Arias Milla, Juan Antonio Vargas Núñez, Valentín Cuervas-Mons Martínez, Carmen Cubero, Celia Rodríguez Olleros, Elvira Ramos Carral, Yale Tung. HOSPITAL UNIVERSITARIO SON ESPASES: Mercedes García Gasalla, Adrián Ferré Beltrán, Pere Ventayol Bosch, Juana Maria Ferrer Balaguer, Francisca Artigues Serra, Alfredo Manuel Santos Pinheiro, Helem H Vilchez Rueda, Antonio Palomero. HOSPITAL UNIVERSITARIO INFANTA CRISTINA: Ana Muñoz Gómez, Francisco Javier Teigell Muñoz, Elena García Guijarro, Francisco García Sánchez, José Antonio Melero Bermejo, María Mateos González, Aitor Olmo Sánchez, Juan Vicente de la Sota, Elena Matilla. HOSPITAL UNIVERSITARIO DE BURGOS: María López Veloso, Julio Barraza Vengoechea, Enrique Iglesias Julián, Ana Marta Espeja Martínez, Fernando Orza García, Luis Buzón Martin, Marta Ubeira Iglesias. HOSPITAL UNIVERSITARIO EL ESCORIAL: Ana Belén Cuenca Abarca, Pedro Gargantilla Madera, Luis Miguel Belda Bilbao, Juan González González, Juan Francisco Montoro Lara, Almudena García Tobaruela, Francisco Javier Montero Jiménez, Silvana Emilise Fiorante, Susana Sánchez Suárez, Carolina Aguilar Casado, Carla Ruth Mejía Medina, Pablo Carrasco Lara, María Isabel Barcia Martín, Mercedes García Gimeno. HOSPITAL UNIVERSITARI SON LLÁTZER: Juan Buades, Inés Losada, Aroa Villoslada, Salvador Pons, Monserrat Vilanova, Adrián Rodríguez, Eugenia Cisneros Barroso, Mónica Sanz. COMPLEJO ASISTENCIAL DE SEGOVIA: Marta González Rozas, Pablo Bachiller Luque, Ana Carrero Gras, Raquel Coloma Peral, Mª Teresa Criado Illana, Eva Ferreira Pasos, Laura Martin Ventura, Javier Moreno Palomares, Fuencisla Gómez Ruiz.
Funding
This work was partially supported by the Biomedical Research Foundation of the Puerta de Hierro Majadahonda University Hospital, and by Sanofi, who provided sarilumab free of charge. None of the funders had any role in the study’s design, collection, management, analysis and interpretation of data, writing of the report and the decision to submit the report for publication. Biomedical Research Foundation of the Puerta de Hierro Majadahonda University Hospital also funded the journal’s Rapid Service Fee.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
Conceptualization and study design: A.S.L., B.R.A, A.C.B., A.F.C. Methodology: A.S.L., B.R.A, A.C.B., A.F.C. Data collection: All authors. Data interpretation: A.S.L., B.R.A, A.C.B., A.F.C. Writing first draft: A.S.L., B.R.A, A.C.B., A.F.C. Critical revision for important intellectual content: All authors. Final approval: All authors. All authors agree to be accountable for all aspects of the work by ensuring that questions related to the accuracy or integrity of any part of the work will be appropriately investigated and resolved. A.S.L., A.C.B and B.R.A. had full access to all the data in this study and take complete responsibility for the integrity of the data and the accuracy of the data analysis. The authors grant their Copyright permissions for published all figures and tables.
Disclosures
Aránzazu Sancho-López, Antonio F Caballero-Bermejo, Belén Ruiz-Antorán, Elena Múñez Rubio, Mercedes García Gasalla, Juan Buades, Marta González Rozas, María López Veloso, Ana Muñoz Gómez, Ana Cuenca Abarca, Pedro Durán del Campo, Fátima Ibáñez, Alberto Díaz de Santiago, Yolanda Romero, Jorge Calderón, Ilduara Pintos, Adrián Ferre Beltrán, Gustavo Centeno Soto, José Campos, Antonio Ramos Martínez, Cristina Avendaño-Solá, Ana Fernández Cruz have nothing to disclose.
Compliance with Ethics Guidelines
The trial was approved by the Spanish Regulatory Authority (Spanish Agency of Medicines and Medical Devices, AEMPS) and by the Research Ethics Committee (REC) at Hospital Universitario Puerta de Hierro-Majadahonda (registry number 77/20). The study was conducted in accordance with Good Clinical Practice guidelines and the Declaration of Helsinki. All patients provided informed consent to participate in the study The investigators designed the trial, collected the data, and performed the analysis.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Consortia
Corresponding authors
Additional information
The members of the SARTRE Study group are mentioned "Acknowledgments section".
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Sancho-López, A., Caballero-Bermejo, A.F., Ruiz-Antorán, B. et al. Efficacy and Safety of Sarilumab in patients with COVID19 Pneumonia: A Randomized, Phase III Clinical Trial (SARTRE Study). Infect Dis Ther 10, 2735–2748 (2021). https://doi.org/10.1007/s40121-021-00543-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40121-021-00543-2