
Abstract
Liposomal irinotecan (nal-IRI; Onivyde®; also known as pegylated liposomal irinotecan) has been developed with the aim of maximising anti-tumour efficacy while minimising drug-related toxicities compared with the conventional (non-liposomal) formulation of this topoisomerase 1 inhibitor. In combination with 5-fluorouracil and leucovorin (5-FU/LV), nal-IRI is the first agent to be specifically approved for use in patients with metastatic pancreatic ductal adenocarcinoma (mPDAC) who have progressed following gemcitabine-based therapy. In the pivotal, phase III NAPOLI-1 trial, intravenous administration of nal-IRI + 5-FU/LV to gemcitabine-pretreated patients with mPDAC (as a second-line treatment in approximately two-thirds of cases) was associated with a significant ≈ 2-month median overall survival advantage compared with 5-FU/LV alone. Moreover, adding nal-IRI to 5-FU/LV extended survival with a manageable safety profile and without adversely affecting health-related quality of life, thereby producing significant and clinically meaningful gains in quality-adjusted survival relative to 5-FU/LV alone. Complementing the observed efficacy and safety of nal-IRI in NAPOLI-1 are an increasing number of real-world studies, which provide evidence of the effectiveness of this combination therapy in the treatment of mPDAC that has progressed following gemcitabine-based therapy in contemporary clinical practice in Europe, the USA and East Asia. Thus, nal-IRI, in combination with 5-FU/LV, is the first regimen specifically approved for use as a second- or subsequent-line therapy in gemcitabine-pretreated patients with mPDAC and, as such, represents a valuable treatment option in this setting.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
First agent specifically approved for use (in combination with 5-FU/LV) in this setting |
Added to 5-FU/LV, nal-IRI significantly improved survival outcomes vs. 5-FU/LV alone |
Most common grade 3–4 adverse events included neutropenia and diarrhoea |
Real-world data confirm effectiveness and safety of nal-IRI + 5-FU/LV in clinical practice |
Dose modifications for adverse events do not appear to adversely affect survival outcomes |
1 Introduction
Pancreatic ductal adenocarcinoma (PDAC) is the most common type of pancreatic malignancy, accounting for > 90% of all cases. It is an aggressive and highly lethal condition on account of its high metastatic potential which, combined with a lack of early symptoms and robust resistance to most conventional cytotoxic and targeted anticancer agents, results in the majority of patients being diagnosed with locally-advanced, unresectable (20–30%) or metastatic (50–55%) disease and having very few treatment options, mainly systemic chemotherapy of palliative intent. Therefore, despite some significant advances in the management of PDAC over the past decade, it continues to have a poor prognosis (5-year survival rate of 8–11%) [1,2,3,4].
Globally, the annual number of cases and deaths related to pancreatic cancer, which has increased more than two-fold since the 1990s, is expected to rise further by almost 80% by 2040 (to 815,276 and 777,423, respectively [5]), largely as a result of population aging, but also reflecting an increase in the prevalence of obesity and type 2 diabetes [1, 6, 7]. Smoking has also been recognized as a risk factor for the disease [7]. While there is considerable international variation, the highest age-standardized incidence and mortality rates of pancreatic cancer are seen in regions at a higher stage of socioeconomic development, such as western and central Europe, high-income North America and high-income Asia Pacific [6, 7].
Among the cytotoxic chemotherapeutic anticancer agents to have been investigated in the treatment of metastatic PDAC (mPDAC), the conventional formulation of the topoisomerase-1 inhibitor irinotecan has shown limited utility, attributed, in part, to its suboptimal pharmacokinetic profile (rapid elimination) and acute toxicities [8]. It is, nonetheless, an integral component of the FOLFIRINOX regimen [consisting of oxaliplatin, irinotecan, 5-fluouracil (5-FU) and leucovorin (LV)], which, alongside gemcitabine in combination with nanoparticle albumin-bound paclitaxel (nab-paclitaxel), is an established first-line therapy for patients with mPDAC and good performance status [9,10,11]. Although all patients eventually progress, the improvement in outcomes with these combination regimens relative to gemcitabine monotherapy (the previous standard of care that remains a treatment of choice for patients with poor performance status) has resulted in an increased number of individuals (≈ 40–50% [4]) being able to receive second-line treatment after progression on front-line therapy [12, 13]. Accordingly, the importance of determining the most appropriate second-line treatment following failure of a first-line combination regimen (i.e. optimal treatment sequencing) has also increased [2]. In this regard, second-line options for patients who have progressed following gemcitabine-based therapy have historically been lacking [8, 14, 15].
Liposomal irinotecan (nal-IRI; Onivyde®) (also known as pegylated liposomal irinotecan and abbreviated as MM-398 or PEP02) is an intravenously-administered, liposomal-encapsulated formulation of irinotecan that has been developed to overcome the pharmacological and clinical limitations of the conventional (non-liposomal) formulation of the drug, with the overall aim of maximising anti-tumour efficacy while minimising drug-related toxicities [8, 12, 13, 16]. Liposomal irinotecan, in combination with 5-FU and LV, has been approved in several regions or countries worldwide, including the EU [17], the USA [18], Canada [19], Australia [20], Japan [21], South Korea [22] and Taiwan [22], for the treatment of mPDAC in patients who have progressed following gemcitabine-based therapy. This article reviews clinical efficacy and tolerability data relevant to the use of nal-IRI in combination with 5-FU/LV in the treatment of gemcitabine-pretreated mPDAC; the pharmacological properties of nal-IRI/irinotecan are also summarized (Table 1).
2 Therapeutic Efficacy of Liposomal Irinotecan
The efficacy of nal-IRI combined with 5-FU/LV in adult patients with mPDAC that had progressed following gemcitabine-based therapy was assessed in NAPOLI-1, a prospective, randomized, open-label, multicenter, global phase III clinical trial conducted at 76 sites in 14 countries (Argentina, Australia, Brazil, Canada, Czech Republic, France, Germany, Hungary, Italy, South Korea, Spain, Taiwan, the UK and the USA) [23] (Sect. 2.1). More recently, the effectiveness of this combination has been evaluated in several retrospective, observational (real-world evidence) studies from one [24,25,26] or more [27,28,29,30,31,32] institutions in Austria [24], Italy [30], South Korea [27], Taiwan [26] or the USA [25, 28, 29, 31, 32] (Sect. 2.2).
2.1 NAPOLI-1
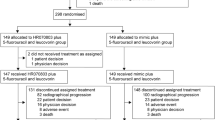
The history and conduct of the NAPOLI-1 study has been described in detail previously [8]. Briefly, this trial was initially designed to compare nal-IRI monotherapy with 5-FU/LV control therapy (under protocol version 1), but was subsequently modified to compare both nal-IRI monotherapy and nal-IRI + 5-FU/LV combination therapy with 5-FU/LV control therapy (under protocol version 2) [8, 23].
Eligible patients had PDAC and documented distant metastatic disease (measurable or non-measurable) that had progressed after previous gemcitabine-based therapy administered in the neoadjuvant, adjuvant (only if distant metastases occurred within 6 months of therapy completion), locally advanced or metastatic setting. Other eligibility criteria included a Karnofsky performance status (KPS) score of ≥ 70 [equivalent to European Cooperative Oncology Group (ECOG) performance status (PS) 0–1] and satisfactory haematological, hepatic and renal function [23].
A total of 417 patients were randomly assigned to the three treatment arms of this trial: 151 to nal-IRI monotherapy (33 and 118 under protocol 1 and 2, respectively); 149 to 5-FU/LV control therapy (30 and 119 under protocol 1 and 2, respectively) and 117 to nal-IRI + 5-FU/LV combination therapy (all under protocol 2). Randomization was stratified by KPS (70 and 80 vs. ≤ 90), baseline albumin levels (≥ 40 vs. < 40 g/L) and ethnicity (White vs. East Asian vs. other). For patients homozygous for the UGT1A1*28 allele (n = 14), the initial nal-IRI dose was reduced by 20 mg/m2 and increased to the standard dose in the absence of drug-related toxicity. Treatment continued until disease progression or intolerable toxicity [23].
The primary efficacy endpoint was overall survival (OS) in the intention-to-treat (ITT) population; the primary analysis of OS was performed after 313 deaths had occurred across the three arms [23]. An updated (final) analysis of OS was performed once all patients were no longer receiving study treatment; 382 deaths had occurred across the three arms at the time of this data cut-off [33]. Secondary endpoints assessed at the time of the primary and final OS analyses included progression-free survival (PFS) and the proportion of patients achieving an objective response [23, 33].
This section focuses exclusively on findings for the 117 patients randomized to nal-IRI + 5-FU/LV combination therapy (i.e. the approved nal-IRI regimen; Sect. 4) and the 119 randomized to 5-FU/LV control therapy under protocol 2 [17, 18, 23, 33,34,35,36,37,38,39,40,41] (some results are only available as abstracts [38, 39]). See Table 2 for treatment regimen details. Baseline characteristics were well balanced between the two arms. The 236 randomized patients had a median age of 63 (range 34–81) years, 58% were males, and 63% and 30% were Whites and East Asians, respectively [23]. KPS was ≥ 70 in 98% of patients and serum carbohydrate antigen 19-9 (CA19-9) levels were ≥ 40 U/mL in 80% of evaluable patients. Liver, lung and peritoneal metastases were present in 67%, 31% and 25% of patients, respectively; 67% had ≥ 2 measureable metastatic lesion sites. Just over one-quarter (27%) had undergone a prior Whipple procedure; 10% had a biliary stent. Just over two-thirds (68%) were administered nal-IRI + 5-FU/LV in the second line (i.e. they had already received one prior line of gemcitabine-based therapy in the neoadjuvant or adjuvant setting, or for advanced disease); 33% had received ≥ 2 prior lines of gemcitabine-based therapy for metastatic disease. Just over half (54%) received prior gemcitabine-based combination therapy (as opposed to gemcitabine monotherapy) [23]; 13% received prior gemcitabine in combination with nab-paclitaxel [18].
In NAPOLI-1, nal-IRI + 5-FU/LV significantly prolonged median OS compared with 5-FU/LV alone in gemcitabine-pretreated patients with mPDAC [23]. At the time of the primary analysis, there was a 33% reduction in the risk of death in the nal-IRI + 5-FU/LV group relative to the 5-FU/LV group [unstratified hazard ratio (HR) 0.67; 95% CI 0.49–0.92; p = 0.012] (Table 2), with 64% and 67% of the patients allocated to these arms having died. The treatment effect persisted (i.e. HR 0.58; 95% CI 0.42–0.81) after adjusting for the following prognostic factors: baseline KPS; baseline albumin level; baseline CA19-9 level; time since receiving most recent anticancer therapy; tumour stage at diagnosis; and status of liver metastases [23].
Improvements in OS with nal-IRI + 5-FU/LV (i.e. HR < 1 vs. 5-FU/LV alone) were observed in most pre-planned subgroup analyses of patient, tumour and previous treatment characteristics at baseline, including sex, age (≤ 65; > 65 years), KPS (70–80; 90–100), albumin (< 40; ≥ 40 g/L), ethnicity (White; East Asian; other), CA19-9 level (< 40; ≥ 40 U/mL), body mass index (BMI) (< median; ≥ median), primary tumour site (locations including the pancreatic head; locations excluding the head), presence of liver metastases (yes; no), tumour stage at diagnosis (stage IV; other), number of previous lines of metastatic therapy (0; 1; ≥ 2), prior treatment with 5-FU (yes; no), prior treatment with radiotherapy (yes; no) and prior biliary stent (yes; no). Exceptions included prior exposure to conventional irinotecan [HR for OS = 1.25 (vs. 0.62 in patients not previously treated with conventional irinotecan)] and a prior Whipple procedure [HR for OS = 1.23 (vs. 0.50 in patients not previously undergoing a Whipple procedure)], albeit these were among the smallest subgroups [23].
An OS benefit with nal-IRI + 5-FU/LV (i.e. HR < 1 vs. 5-FU/LV alone) was also apparent in the following post hoc subgroups: prior treatment with gemcitabine monotherapy; prior treatment with gemcitabine-based combination therapy; prior surgery (yes; no); best response to prior anticancer therapy [complete response/partial response (yes; no) and complete response/partial response/stable disease (yes; no)]; and diabetes mellitus (with; without) [35].
Additional post hoc analyses have highlighted improvements in OS with nal-IRI + 5-FU/LV in patients with baseline neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios of ≤ 5 and ≤ 150 respectively [39], expanded on the OS benefit of treatment in older patients (e.g. aged ≥ 65; ≥ 70 and ≥ 75 years) [36] and confirmed the OS benefit in East Asian patients [37]. Notably, an improvement in OS with nal-IRI + 5-FU/LV relative to 5-FU/LV alone was seen irrespective of dose modifications used to manage adverse events, according to another post hoc analysis [38]. Median OS was 8.4 months in nal-IRI + 5-FU/LV recipients who had a dose reduction (n = 49) versus 4.2 months in 5-FU/LV recipients (n = 105) (HR 0.66; 95% CI 0.46–0.94); it was 9.4 months in nal-IRI + 5-FU/LV recipients who had a dose delay (n = 34) versus 4.2 months in 5-FU/LV recipients (n = 105) (HR 0.58; 95% CI 0.38–0.88) [38].
Regarding other endpoints assessed at the time of the primary analysis, nal-IRI + 5-FU/LV also significantly extended median PFS (Table 2) and median time to treatment failure [2.3 vs. 1.4 months (HR 0.6; 95% CI 0.45–0.78); p = 0.0002)] compared with 5-FU/LV alone; significantly more nal-IRI + 5-FU/LV recipients achieved an objective response (Table 2) or a CA19-9 response (≥ 50% decrease from abnormal baseline; 29% vs. 9%; p = 0.0006).
The results of a pre-specified analysis of the per-protocol (PP) population (patients receiving ≥ 80% of planned treatment during the first 6 weeks, with no major protocol violations) were consistent with those from the ITT population with respect to median OS, median PFS and the proportion of patients achieving an objective response (Table 2) [34].
The significant benefits of nal-IRI + 5-FU/LV over 5-FU/LV alone for median OS, median PFS and the proportion of patients achieving an objective response were also maintained at the time of the final analysis (Table 2) [33]. Furthermore, disease control rate (DCR) favoured nal-IRI + 5-FU/LV over 5-FU/LV therapy [52% (95% CI 43–61) vs. 24% (95% CI 17–33)]. Estimated 1-year OS rates were 26% and 16% in the nal-IRI + 5-FU/LV and 5-FU/LV arms, with the following baseline characteristics being associated with survival ≥ 1 year in the nal-IRI + 5-FU/LV arm: KPS ≥ 90; age ≤ 65 years; lower CA19-9 level, neutrophil-to-lymphocyte ratio < 5 and absence of liver metastases [33].
Overall, neither nal-IRI + 5-FU/LV nor 5-FU/LV alone adversely affected health-related quality of life (HRQOL), as measured during the first 12 weeks of NAPOLI-1using the European Organisation for Research and Treatment of Cancer questionnaire C30 (EORTC QLQ-C30) [40]. At week 12, the only change in EORTC QLQ-C30 global health status or functional and symptom scale scores of note in evaluable nal-IRI + 5-FU/LV recipients (n = 71) was an 11-point increase (i.e. ‘moderate’ deterioration) from baseline in the median fatigue score, which contrasted with no change in median fatigue score in 5-FU/LV recipients (n = 57) [40]. Moreover, applying the quality-adjusted time without symptoms or toxicity (Q-TWiST) method to the NAPOLI-1 trial data (ITT and PP results), nal-IRI + 5-FU/LV resulted in statistically significant and clinically meaningful gains in quality-adjusted survival versus 5-FU/LV alone [41]. In the ITT analysis, for example, mean Q-TWiST was 5.1 months in nal-IRI + 5-FU/LV recipients versus 3.9 months in 5-FU/LV recipients [between-group difference 1.3 (95% CI 0.4–2.1) months], corresponding to a 24% relative improvement [41].
2.2 Real-World Studies
Real-world studies investigating nal-IRI + 5-FU/LV have enrolled individuals (n = 44–296) with advanced PDAC (i.e. unresectable, locally advanced or metastatic disease) that had progressed following gemcitabine-based chemotherapy in the neoadjuvant or adjuvant setting, or in a prior line of treatment for advanced disease [24,25,26,27,28,29,30,31,32] (some results only available as an abstract and/or poster [28, 30, 32]). The median age of study populations was 60–69 years, 38–61% were males and, where specified, 54–100% of evaluable patients had ECOG PS 0–1, and 61–83% of evaluable patients had elevated CA 19-9 levels [24,25,26,27, 30,31,32]. Liver, lung and peritoneal metastases were present in 57–73%, 9–31% and 25–36% of patients, respectively (Table 3); 23–58% had ≥ 2 metastatic sites [24,25,26, 30]. Where stated, nal-IRI + 5-FU/LV was administered as a second-line or earlier therapy in 41–73% of patients [24,25,26,27, 30,31,32] and as a third-line or later therapy in 25–59% of patients [24,25,26,27, 30,31,32]. Of note, 44% and 76% of patients in multicentre studies from South Korea [27] and Italy [30], respectively, previously received nab-paclitaxel + gemcitabine as first-line therapy. Moreover, 45% and 49% of patients in single-centre studies from the USA [25] and Austria [24], respectively, who were administered nal-IRI + 5-FU/LV as a second-line therapy had previously received nab-paclitaxel + gemcitabine (or nab-paclitaxel + gemcitabine or gemcitabine alone [25]) as first-line therapy (Table 3).
The observed effectiveness of nal-IRI + 5-FU/LV in clinical practice studies across Europe (Austria, Italy), the USA and East Asia (South Korea, Taiwan) confirms the efficacy reported in the global NAPOLI-1 clinical trial (Sect. 2.1) [24,25,26,27, 30,31,32]. Some study populations were considered well matched to the cohort studied in NAPOLI-1 [24, 27], while others were less favourably selected, with an older median age and/or a higher proportion of patients with poorer PS [25, 26, 30, 31]. These variations in baseline patient characteristics notwithstanding, median OS (from the time of nal-IRI + 5-FU/LV initiation) ranged from 4.2–9.4 months; median PFS ranged from 2.3–3.84 months (Table 3). The proportions of patients achieving an objective response (per RECIST v1.1 criteria) ranged from 5–19.2%; DCRs ranged from 40–54.7% [24,25,26,27,28, 30].
Consistent with the results of pre-specified and/or post hoc analyses of NAPOLI-1 (Sect. 2.1), median OS was generally higher in patients who had not previously received conventional irinotecan compared with those who had previously received (and progressed on [25, 27]) conventional irinotecan [25, 27, 28, 31] (Table 3). Moreover, patients treated with nal-IRI + 5-FU/LV who had not progressed on prior conventional irinotecan showed improved survival outcomes compared with those who had progressed on prior conventional irinotecan [25] (Table 3). As expected, median OS and/or PFS were also generally longer in patients who received nal-IRI + 5-FU/LV in an earlier treatment line (e.g. second-line or earlier) as opposed to in a later treatment line (e.g. third-line or later) [24, 25, 27, 31] (Table 3). In this regard, sequential therapy with first-line gemcitabine, with or without nab-paclitaxel, followed by second-line nal-IRI + 5-FU/LV has demonstrated encouraging survival outcomes [25, 28] (Table 3). For example, median OS was 23 months from the time of advanced disease diagnosis in patients receiving nal-IRI + 5-FU/LV following gemcitabine-based front-line treatment at a single US centre (n = 25) [25]; it was 6.3 months from the time nal-IRI + 5-FU/LV was initiated following gemcitabine-based front-line therapy in patients treated at multiple US centres (n = 129) [29]. Indeed, median OS was 11 months from the time nal-IRI + 5-FU/LV was initiated following front-line nab-paclitaxel + gemcitabine in 15 patients treated at two US centres [28] (Table 3).
Importantly, the results of real-world studies support the suggestion (based on a post hoc analysis of NAPOLI-1; Sect. 2.1) that appropriate dose adjustments/modifications of nal-IRI + 5-FU/LV due to adverse events do not appear to adversely affect survival outcomes [24, 25, 28, 32]. Indeed, based on experience at one [25] or more [32] US centres, median OS was ≈ 7.1 months in patients with ≥ 1 dose reduction versus 4.5 [25] or 3.7 [32] months in patients with no dose reductions; PFS was significantly prolonged (5.4 vs. 2.6 months; p = 0.035) [25]. Similarly, according to experience reported from a single centre in Austria [24], patients with ≥ 1 dose reduction compared with none had, respectively, a median OS of 6.95 and 6.79 months (HR 0.89, 95% CI 0.46–1.7) and a median PFS of 4.26 and 3.44 months (HR 0.86, 95% CI 0.46–1.6). The impact of nal-IRI dose reduction before the start of treatment (i.e. pre-emptive dose reduction at the physician’ discretion for better tolerability) has also been reported. At the aforementioned single US centre, 70% of patients underwent pre-emptive dose reduction; the initial nal-IRI dose was not significantly associated with survival [25]. Two-thirds (66%) of the patients in the Taiwanese cohort underwent pre-emptive nal-IRI dose reduction; among those with ECOG PS 0–1, median OS was 7.5 and 8.4 months in patients with and without starting dose reductions, respectively [26].
3 Tolerability of Liposomal Irinotecan
Liposomal irinotecan combined with 5-FU/LV was generally well tolerated with a manageable safety profile in the NAPOLI-1 study [23] (Sect. 2.1). The most common grade 3–4 treatment-emergent adverse events [TEAEs; i.e. occurring in ≥ 5% of nal-IRI combination therapy recipients (n = 117) and with a ≥ 2% higher incidence than in 5-FU/LV recipients randomized under either the original or revised trial protocols (n = 134)] were neutropenia (27% vs. 1% in the 5-FU/LV group), fatigue (14% vs. 4%), diarrhoea (13% vs. 4%), vomiting (11% vs. 3%), anaemia (9% vs. 7%) and nausea (8% vs. 3%) [23]. Grade 3–4 lymphopenia (27% vs. 17%) and thrombocytopenia (2% vs. 0%) also occurred with a ≥ 2% higher incidence in nal-IRI + 5-FU/LV recipients compared with 5-FU/LV recipients [18].
Neutropenia/leukopenia and diarrhoea are the most notable important haematological and non-haematological adverse events associated with the administration of nal-IRI [17, 18]. Grade 3–4 neutropenic sepsis (including febrile neutropenia) appeared in three patients in the nal-IRI + 5-FU/LV group compared with none of the patients in the 5-FU/LV control group; supportive care with granulocyte colony stimulating factor (G-CSF) was administered to 17% and 1% of patients, respectively [23]. Grade 3 or 4 early-onset diarrhoea (≤ 24 h after treatment administration) occurred in 3% of patients in the nal-IRI + 5-FU/LV group compared with no patients in the 5-FU/LV group, while grade 3 or 4 late-onset diarrhoea (> 1 day after treatment administration) occurred in 9% and 4% of patients, respectively [18]. Neutropenia and diarrhoea typically first occurred early in the course of therapy (i.e. weeks 1–6) and tended to decrease in incidence and severity thereafter (abstract [42]).
TEAEs (most frequently neutropenia, diarrhoea, fatigue, vomiting and thrombocytopenia) led to the withholding or delaying of nal-IRI in 62% of patients in the nal-IRI + 5-FU/LV group [18]. TEAEs resulting in dose reduction occurred in 33% of nal-IRI + 5-FU/LV recipients (most frequently neutropenia, diarrhoea, nausea and anaemia) versus 4% of 5-FU/LV recipients; TEAEs resulting in treatment discontinuation occurred in 11% (most frequently diarrhoea, vomiting and sepsis) and 7%, respectively [18, 23]. The 30-day mortality rate was low (3%) in both treatment groups; a treatment-related adverse event (septic shock) resulted in one death in the nal-IRI + 5-FU/LV group [23].
The safety profile of nal-IRI + 5-FU/LV was generally similar across pre-specified subgroups, based on sex, age, ethnicity, UGT1A1*28 status, prior exposure to conventional irinotecan and prior treatment with 5-FU (abstract [43]). A notable exception was a higher rate of grade ≥ 3 neutropenia in Asian compared with Caucasian patients (55% vs. 18%; n = 33 and 73); neutropenic fever/neutropenic sepsis occurred in 6% and 1% of Asian and Caucasian patients, respectively [17, 18]. This notwithstanding, the safety profile of nal-IRI + 5-FU/LV in the Asian cohort of NAPOLI-1 was manageable (abstract [44]). Indeed, Asian patients had a lower incidence of grade ≥ 3 diarrhoea compared with Caucasian patients (3% vs. 19%) [17, 43]. There were no differences in the incidence, type and severity of TEAEs between patients homozygous for the UGT1A1*28 allele (n = 7) who initiated nal-IRI at a reduced dose of 50 mg/m2 in combination with 5-FU/LV and those who were not homozygous for the UGT1A1*28 allele (n = 110) who started nal-IRI at a dose of 70 mg/m2 in combination with 5-FU/LV. The frequency of grade 3–4 neutropenia, for example, was 28.6% and 27.3% in homozygous and non-homozygous patients, respectively [17, 18]. Three of the seven homozygous patients dose-escalated to 70 mg/m2 without requiring subsequent dose reductions. One patient required a dose reduction to 40 mg/m2 and one patient discontinued treatment due to grade 3 vomiting [29].
At the time of the final analysis of NAPOLI-1, the safety profile of nal-IRI + 5-FU/LV [mean treatment exposure 18.6 weeks (median 8.7 weeks; range 2–127 weeks)] was not substantially different to that reported in the primary analysis, and no new safety concerns were detected [33].
Data from clinical practice concerning the safety of nal-IRI combination therapy in patients with advanced PDAC are generally consistent with the results of the NAPOLI-1 trial [24,25,26,27,28, 30, 32]. However, real-world treatment patterns, such as pre-emptive nal-IRI dose reduction [25, 28] and administration of anti-emetic and anti-diarrhoeal drugs [24], have likely contributed to the relatively low rates of serious TEAEs, including grade 3–4 neutropenia (2–14%) and grade 3–4 diarrhoea (2–8%), reported in some studies from Austria [24] and the USA [25, 28]. Moreover, while G-CSF prophylaxis was not part of the NAPOLI-1 trial, nearly half (47.9%) of the patients in the largest study from the USA (n = 257, of whom 242 had previously been treated with gemcitabine and 230 were given nal-IRI in combination with 5-FU/LV) received G-CSF during treatment with nal-IRI; almost two-thirds (64%) received G-CSF prior to initiating nal-IRI [31]. A total of 18 patients (7%) experienced grade 3 neutropenia and five (2%) experienced grade 4 neutropenia while undergoing nal-IRI therapy [31].
The safety profile of nal-IRI + 5-FU/LV in clinical practice in East Asia was similar to that seen in the NAPOLI-1 Asian subgroup in terms of the comparatively high and low incidences of grade ≥ 3 neutropenia and diarrhoea, respectively, relative to those seen in the NAPOLI-1 Caucasian subgroup [26, 27, 37]. Among South Korean patients, the most common grade 3–4 adverse events with nal-IRI + 5-FU/LV were neutropenia (37.2%), nausea (10.5%), vomiting (9.3%) and diarrhoea (4.7%); febrile neutropenia occurred in seven patients (8%) [27]. Among Taiwanese patients, the incidence of grade 3–4 neutropenia with nal-IRI + 5-FU/LV was 27% (i.e. approximately half that seen in the NAPOLI-1 Asian subgroup); this was partially attributed to pre-emptive dose reduction (Sect. 2.2) and to a lower mean dose intensity of nal-IRI in the Taiwanese cohort compared with the NAPOLI-1 Asian subgroup (61 vs. 75%) [26, 37]. No patient in the Taiwanese cohort experienced grade 3–4 diarrhoea [26].
Around one-fifth to a half (22–50%) of patients enrolled in real-world studies from Europe and the USA had at least one nal-IRI dose reduction [24, 25, 28, 30,31,32]; diarrhea and fatigue were the most common reasons for dose reduction [24, 25, 28]. Notably, neither reduced starting doses nor dose reductions (or delays) of nal-IRI were associated with worse survival outcomes [25, 28] (Sect. 2). Liposomal irinotecan doses were also reduced or delayed in half (50%) of patients in South Korea; however, neutropenia was the most frequent reason for dose modification (in 23% of patients), with diarrhoea only accounting for dose modifications in two patients (5%) [27]. Approximately one-fifth (21%) of patients in Taiwan (66% of whom had undergone pre-emptive nal-IRI dose reduction) required a further nal-IRI dose reduction after the start of treatment [26].
4 Dosage and Administration of Liposomal Irinotecan
The recommended dosage of nal-IRI administered in combination with 5-FU/LV for the treatment of mPDAC in adults who have progressed following gemcitabine-based therapy is 80 mg/m2 (expressed as hydrochloride trihydrate salt; equivalent to 70 mg/m2 irinotecan free base) infused intravenously over 90 min every 2 weeks [17, 18]. These three therapies should be administered sequentially, with nal-IRI followed by LV (400 mg/m2 given intravenously over 30 min) and 5-FU (2400 mg/m2 given intravenously over 46 h) [17]. A reduced starting dose of nal-IRI 60 mg/m2 (50 mg/m2 irinotecan free base) should be considered in the EU [17] and is recommended in the USA [18] for patients known to be homozygous for the UGT1A1*28 allele; if tolerated, this dose can be increased to 80 mg/m2 (70 mg/m2 irinotecan free base) in subsequent cycles [17, 18]. Patients should be pre-medicated with a corticosteroid (e.g., dexamethasone) and an anti-emetic (e.g., a 5-HT3 antagonist) 30 [18] or ≥ 30 [17] min prior to nal-IRI infusion. Liposomal irinotecan is not indicated as monotherapy for the treatment of gemcitabine-pretreated patients with mPDAC nor is it interchangeable with conventional irinotecan [17, 18].
Local prescribing information should be consulted for detailed information regarding recommended dose modifications for grade 3–4 haematological and non-haematological adverse reactions, as well as drug interactions, precautions, warnings, contraindications and use in specific patient populations.
5 Place of Liposomal Irinotecan in the Management of Metastatic Pancreatic Cancer
Liposomal irinotecan, in combination with 5-FU/LV, is the first agent to be specifically approved for use in patients with mPDAC who have progressed following gemcitabine-based therapy. This approval rests on the results of the phase III NAPOLI-1 study, in which the intravenous administration of nal-IRI + 5-FU/LV to gemcitabine-pretreated patients with mPDAC (as a second-line treatment in approximately two-thirds of cases) was associated with a significant ≈ 2-month median OS advantage compared with 5-FU/LV alone (Sect. 2.1). Of particular importance, given that most patients are treated palliatively for mPDAC, the addition of nal-IRI to 5-FU/LV extended survival with a manageable safety profile and without adversely affecting HRQOL, thereby producing significant and clinically meaningful gains in quality-adjusted survival relative to 5-FU/LV alone (Sect. 2.1). Grade 3–4 TEAEs in nal-IRI + 5-FU/LV recipients included myelosuppressive events (notably neutropenia) and gastrointestinal toxicities (notably diarrhoea) (Sect. 3); there are special warnings and precautions (including a black box warning in the USA [18]) concerning the potential for severe or life-threatening neutropenia and diarrhoea to occur during nal-IRI therapy (Sect. 4). The rate of nal-IRI + 5-FU/LV discontinuation due to TEAEs was, however, low (11%) (Sect. 3).
The findings of the pivotal NAPOLI-1 study are also reflected in current US [10, 11], European [45] and Japanese [46] guidelines, which recommend considering nal-IRI + 5-FU/LV as a second-line treatment option in patients with metastatic disease that has progressed on gemcitabine-based therapy and good PS. Specifically, the American Society of Clinical Oncology (ASCO) guideline on the management of mPDAC [11] states that nal-IRI + 5-FU is preferred as second-line therapy for patients with first-line treatment with gemcitabine + nab-paclitaxel, an ECOG PS of 0–1 and a relatively favourable comorbidity profile. Similarly, the National Comprehensive Cancer Network (NCCN) guideline includes a category 1 recommendation (i.e. based upon high-level evidence and uniform consensus) for the use of nal-IRI + 5-FU/LV as a second-line option in patients with mPDAC previously treated with gemcitabine-based therapy and good PS [10, 46]. Additionally, as set out in an update [45] to the European Society for Medical Oncology (ESMO) guideline [9], nal-IRI + 5-FU/LV may constitute an active and tolerable second-line treatment option for fit patients with mPDAC previously treated with gemcitabine-based therapy.
By substantiating a sequential approach to treatment, whereby first-line gemcitabine-based therapy is followed by second-line nal-IRI + 5-FU/LV, the NAPOLI-1 study has contributed greatly to an emerging therapeutic paradigm in mPDAC [13]. Moreover, the advent and availability of nal-IRI + 5-FU/LV as an approved and accepted second-line therapy following first-line gemcitabine may influence the choice between gemcitabine + nab-paclitaxel and FOLFIRINOX as the preferred front-line therapy. This decision normally takes into account a number of factors, in particular patient age, PS, associated comorbidities and tolerance for cytotoxic chemotherapy regimen; these factors also affect the choice of second-line therapy, which usually includes agents not included in the first-line regimen [25, 47]. The optimal sequencing of PDAC therapy has, however, still to be defined [2, 25]; the results of randomized comparisons of nal-IRI + 5-FU/LV versus FOLFIRINOX as second-line therapy in patients with mPDAC experiencing progression on first-line gemcitabine + nab-paclitaxel and of nal-IRI + 5-FU/LV versus gemcitabine + nab-paclitaxel as second-line therapy in patients with mPDAC experiencing progression on first-line FOLFIRINOX will be highly relevant in this regard.
NAPOLI-1 was a global study and included patients enrolled at centres across Europe, North and South America, East Asia and Australasia (Sect. 2.1). Nearly a third of participants were from East Asia (Sect. 2.1), although none were from Japan. In this regard, therefore, it is interesting to note the results of a recent, randomized phase II study, which found treatment with nal-IRI + 5-FU/LV as per the NAPOLI-1 regimen to be associated with a clinically meaningful and statistically significant gain in investigator-assessed PFS compared with 5-FU/LV alone in gemcitabine-pretreated Japanese patients with mPDAC; there were no new or unexpected safety signals in this population [48].
The OS benefit with nal-IRI + 5-FU/LV over 5-FU/LV alone was seen in most pre-planned and post hoc exploratory subgroup analyses of patient, tumour and previous treatment characteristics at baseline, the most notable exception being in patients previously exposed to conventional irinotecan (Sect. 2.1). Another post hoc analysis of NAPOLI-1 has identified eight baseline factors significantly associated with OS (including treatment with nal-IRI + 5-FU/LV); these have been used to develop a nomogram for predicting survival in patients with mPDAC previously treated with gemcitabine who receive nal-IRI + 5-FU/LV [47].
An acknowledged limitation of NAPOLI-1, however, was that the study population was favourably selected, consisting mostly of patients with good PS (> 90% were ECOG ≤ 1); hence the results may not, necessarily, be applicable to real-world settings with less-selected patient populations [23]. Furthermore, this trial was performed prior to the widespread adoption of gemcitabine + nab-paclitaxel and FOLFIRINOX as the preferred front-line regimens; only a small proportion of participants had been pretreated with gemcitabine + nab-paclitaxel (Sect. 2.1). In terms of addressing these issues, relevant real-world data are accumulating; to date, the effectiveness of nal-IRI + 5-FU/LV observed in gemcitabine-pretreated patients with advanced PDAC treated in contemporary clinical practice in Europe, the USA and East Asia has been largely consistent with the efficacy of this combination therapy seen in the NAPOLI-1 trial, despite some study populations being less favourably selected (e.g. older median age; more patients with poorer PS) and some differences in treatment patterns (e.g. pre-emptive dose reductions) (Sects. 2.2 and 3). In particular, real-world experience supports the suggestions that OS in nal-IRI + 5-FU/LV-treated patients may be favourably (rather than adversely) affected by appropriate dose adjustments/modifications for adverse events (Sects. 2.2 and 3), but is shorter in those who have (versus those who have not) received—and progressed on—prior conventional irinotecan (Sect. 2.2). In addition to previous exposure to conventional irinotecan, baseline serum albumin < 40 g/L and baseline neutrophil-to-lymphocyte ratio > 5 were associated with reduced survival in the largest real-world study from the US; accordingly, it has been suggested that these patient attributes can be used as association biomarkers to aid appropriate patient selection for nal-IRI therapy [31]. As expected, earlier (e.g. second-line) use of nal-IRI + 5-FU/LV is associated with improved survival compared with later (third- or subsequent-line) use (Sect. 2), albeit investigators at one US institute noted that median survival from the time of advanced disease diagnosis did not differ significantly between patients who received first-line gemcitabine + nab-paclitaxel followed by second-line nal-IRI + 5-FU/LV and those who received first-line FOLFIRINOX followed by second-line gemcitabine + nab-paclitaxel and third-line nal-IRI + 5-FU/LV (23 vs. 25.5 months) [25]. Real-world experience of sequential therapy with first-line gemcitabine + nab-paclitaxel followed by second-line nal-IRI + 5-FU/LV is nonetheless encouraging (Sect. 2.2). For example, a small number of patients treated at two US centres had a median OS from the time nal-IRI + 5-FU/LV was initiated following front-line nab-paclitaxel + gemcitabine of 11 months (Sect. 2.2); this approximates the median OS seen in early-stage pancreatic patients managed with Whipple resection (≈ 16 months [49]). In Europe, Austrian investigators have attributed the improvement in survival benefit observed at their institution over time to changes in treatment patterns, in particular to the introduction of sequential therapy with first-line gemcitabine + nab-paclitaxel followed by second-line nal-IRI + 5-FU/LV [50]. Elsewhere in Europe, the efficacy of second-line nal-IRI + 5-FU/LV in patients with advanced PDAC following the failure of first-line gemcitabine + nab-paclitaxel is currently being evaluated as part of a phase III trial being conducted in Germany (PREDICT; NCT03468335).
Prior to the approval of nal-IRI + 5-FU/LV, the most commonly employed regimens for the treatment of gemcitabine-pretreated PDAC were 5-FU/LV in combination with either conventional irinotecan (FOLFIRI) or oxaliplatin-based treatment (FOLFOX; OFF), albeit these regimens were supported by no (FOLFIRI) or conflicting (FOLFOX; OFF) data from randomized phase III trials [25]. Retrospective, single-centre observational studies suggest survival outcomes with nal-IRI + 5-FU/LV are at least comparable to those with FOLFIRI [51] or FOLFOX [24], and prospective, randomized, multicentre comparisons of these regimens would be of interest.
In conclusion, nal-IRI, in combination with 5-FU/LV, is the first regimen specifically approved for use as a second- or subsequent-line therapy in gemcitabine-pretreated patients with mPDAC and, as such, represents a valuable treatment option in this setting.
Data Selection Liposomal Irinotecan: 325 records identified
Duplicates removed | 122 |
Excluded during initial screening (e.g. press releases; news reports; not relevant drug/indication; preclinical study; reviews; case reports; not randomized trial) | 40 |
Excluded during writing (e.g. reviews; duplicate data; small patient number; nonrandomized/phase I/II trials) | 107 |
Cited efficacy/tolerability articles | 22 |
Cited articles not efficacy/tolerability | 34 |
Search Strategy: EMBASE, MEDLINE and PubMed from 2017 to present. Previous Adis Drug Evaluation published in 2017 was hand-searched for relevant data. Clinical trial registries/databases and websites were also searched for relevant data. Key words were liposomal irinotecan, Onivyde, pancreatic cancer. Records were limited to those in English language. Searches last updated 4 Jun 2020 | |
Change history
03 July 2020
The article Liposomal Irinotecan: A Review in Metastatic Pancreatic Adenocarcinoma, written by James E. Frampton, was originally published Online First without Open Access.
21 July 2020
The article Liposomal Irinotecan: A Review in Metastatic Pancreatic Adenocarcinoma, written by James E. Frampton, was originally published Online First without Open Access.
References
Orth M, Metzger P, Gerum S, et al. Pancreatic ductal adenocarcinoma: biological hallmarks, current status, and future perspectives of combined modality treatment approaches. Radiat Oncol. 2019;14(1):141.
Uccello M, Moschetta M, Mak G, et al. Towards an optimal treatment algorithm for metastatic pancreatic ductal adenocarcinoma (PDA). Curr Oncol. 2018;25(1):e90–4.
Ansari D, Tingstedt B, Andersson B, et al. Pancreatic cancer: yesterday, today and tomorrow. Future Oncol. 2016;12(16):1929–46.
Lambert A, Schwarz L, Borbath I, et al. An update on treatment options for pancreatic adenocarcinoma. Ther Adv Med Oncol. 2019;11:1–43.
World Health Organization. International Agency for Research on Cancer. Cancer tomorrow. https://gco.iarc.fr. Accessed 21 Apr 2020.
Rawla P, Sunkara T, Vinaya G. Epidemiology of pancreatic cancer: global trends, aetiology and risk factors. World J Oncol. 2019;10(1):10–27.
GBD 2017 Pancreatic Cancer Collaborators. The global, regional, and national burden of pancreatic cancer and its attributable risk factors in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2019;4(12):934–47.
Lamb YN, Scott LJ. Liposomal irinotecan: a review in metastatic pancreatic adenocarcinoma. Drugs. 2017;77(7):785–92.
Ducreux M, Cuhna AS, Caramella C, et al. Cancer of the pancreas: ESMO clinical practice guidelines for diagnosis treatment and follow-up. Ann Oncol. 2015;26(Suppl 5):v56–v68.
Tempero MA, Mokenge P, Malafa M, et al. Pancreatic adenocarcinoma, Version 2.2017, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw. 2017;15:1028–106.
Sohal DPS, Kennedy EB, Khorana A, et al. Metastatic pancreatic cancer: ASCO clinical practice guideline update. J Clin Oncol. 2018;36(24):2545–56.
Woo W, Carey ET, Choi M. Spotlight on liposomal irinotecan for metastatic pancreatic cancer: patient selection and perspectives. OncoTargets Ther. 2019;12:1455–63.
Kipps E, Young K, Starling N. Liposomal irinotecan in gemcitabine-refractory metastatic pancreatic cancer: efficacy, safety and place in therapy. Ther Adv Med Oncol. 2017;9(3):159–70.
Passero FC Jr, Saif MW. Second line treatment options for pancreatic cancer. Expert Opin Pharmacother. 2017;18(15):1607–17.
Ur Rehman SS, Lim K, Wang-Gillam A. Nanoliposomal irinotecan plus fluorouracil and folinic acid: a new treatment option in metastatic pancreatic cancer. Expert Rev Anticancer Ther. 2016;16(5):485–92.
Ko AH. Nanomedicine developments in the treatment of metastatic pancreatic cancer: focus on nanoliposomal irinotecan. Int J Nanomed. 2016;11:1225–35.
European Medicines Agency. Onivyde (irinotecan liposome injection): EU summary of product characteristics. https://www.ema.europa.eu/en/. Accessed 8 May 2020.
Ipsen Biopharmaceuticals. Onivyde (irinotecan liposome injection) US Prescribing Information. https://www.onivyde.com. Accessed 8 May 2020.
Shire Pharma Canada ULC. ONIVYDE® (irinotecan liposome for injection): Canadian product monograph. http://www.shirecanada.com. Accessed 2 Feb 2020.
Australian Government Therapeutic Goods Administration. Public summary: Onivyde irinotecan (as sucrosofate) 43 mg/10 mL nanoliposomal concentrated injection for infusion. https://www.ebs.tga.gov.au/. Accessed 20 Feb 2020.
Nippon Servier Co. Ltd. Onivyde® intravenous infusion 43 mg. Japanese prescribing information; 2020. https://www.pmda.go.jp. Accessed 11 May 2020.
PharmaEngine. R&D pipeline about PharmaEngine - Onivyde™ (nal-IRI, MM-398, PEP02). https://www.pharmaengine.com/. Accessed 5 Apr 2017.
Wang-Gillam A, Li CP, Bodoky G, et al. Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1): a global, randomised, open-label, phase 3 trial. Lancet. 2016;387(10018):545–57.
Kieler M, Unseld M, Bianconi D, et al. A real-world analysis of second-line treatment options in pancreatic cancer: liposomal-irinotecan plus 5-fluorouracil and folinic acid. Ther Adv Med Oncol. 2019;11:1–13.
Glassman DC, Palmaira RL, Covington CM, et al. Nanoliposomal irinotecan with fluorouracil for the treatment of advanced pancreatic cancer, a single institution experience. BMC Cancer. 2018;18:693.
Su Y-Y, Chiang N-J, Tsai H-J, et al. The impact of liposomal irinotecan on the treatment of advanced pancreatic adenocarcinoma: real-world experience in a Taiwanese cohort. Sci Rep. 2020;10:7420.
Yoo C, Im HS, Kim KP, et al. Real-world efficacy and safety of liposomal irinotecan plus fluorouracil/leucovorin in patients with metastatic pancreatic adenocarcinoma: a study by the Korean Cancer Study Group. Ther Adv Med Oncol. 2019;11:1–9.
Paluri R, Kasi A, McGinnis T, et al. Efficacy and tolerability of the combination of liposomal irinotecan and 5-fluorouracil/leucovorin in advanced pancreatic cancers: postapproval clinic experience [abstract no. P-271]. Ann Oncol. 2019;30(Suppl 4):74.
Kim GP, Surinach A, Corvino FA, et al. Impact of treatment sequence on overall survival in metastatic pancreatic cancer patients treated with liposomal irinotecan in the real-world setting [abstract no. PCN16]. Value Health. 2019;22:S58.
Pellino A, Merz V, Scartozzi M, et al. Observational retrospective evaluation of treatment with liposomal irinotecan plus fluorouracil/leucovorin for metastatic pancreatic cancer patients:an Italian large real-world analysis [abstract plus poster no. 660]. In: Gastrointestinal Cancers Symposium-American Society of Clinical Oncology; 2020.
Barzi A, Miksad R, Surinach A, et al. Real-world dosing patterns and outcomes of patients with metastatic pancreatic cancer treated with a liposomal irinotecan regimen in the United States. Pancreas. 2020;49(2):193–200.
Cockrum P, Surinach A, Kim G, et al. Impact of dose reductions on clinical outcomes among patients with metastatic pancreatic cancer treated with liposomal irinotecan in oncology clinics in the US [poster no. H18]. In: Gastrointestinal Cancers Symposium-American Society of Clinical Oncology; 2020.
Wang-Gillam A, Hubner RA, Siveke JT, et al. NAPOLI-1 phase 3 study of liposomal irinotecan in metastatic pancreatic cancer: final overall survival analysis and characteristics of long-term survivors. Eur J Cancer. 2019;108:78–877.
Chen LT, Siveke JT, Wang-Gillam A, et al. Survival with nal-IRI (liposomal irinotecan) plus 5-fluorouracil and leucovorin versus 5-fluorouracil and leucovorin in per-protocol and non-per-protocol populations of NAPOLI-1: expanded analysis of a global phase 3 trial. Eur J Cancer. 2018;105:71–8.
Macarulla T, Chen LT, Li CP, et al. Liposomal irinotecan + 5-FU/LV in metastatic pancreatic cancer: subgroup analyses of patient, tumor and previous treatment characteristics in the pivotal NAPOLI-1 trial. Pancreas. 2020;49(1):62–75.
Macarulla T, Blanc JF, Wang-Gillam A, et al. Liposomal irinotecan and 5-fluorouracil/leucovorin in older patients with metastatic pancreatic cancer: a subgroup analysis of the pivotal NAPOLI-1 trial. J Geriatr Oncol. 2019;10(3):427–35.
Bang YJ, Li CP, Lee KH, et al. Liposomal irinotecan in metastatic pancreatic adenocarcinoma in Asian patients: subgroup analysis of the NAPOLI-1 study. Cancer Sci. 2020;111(2):513–27.
Wang-Gillam A, Hubner R, Mirakhur B, et al. Dose modifications of liposomal irinotecan (nal-IRI) + 5-fluorouracil/leucovorin (5-FU/LV) in NAPOLI-1: impact on efficacy [abstract no. 388]. J Clin Oncol. 2018;36(4 Suppl):388.
Wang-Gillam A, Chen LT, Li CP, et al. The prognostic value of baseline neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) for predicting clinical outcome in patients with metastatic pancreatic ductal adenocarcinoma (mPDAC) treated with liposomal irinotecan (nal-IRI; MM-398) + 5-fluorouracil and leucovorin (5-FU/LV) vs 5-FU/LV [abstract no. e15795]. J Clin Oncol. 2017;35(15 Suppl):e15795.
Hubner RA, Cubillo A, Blanc JF, et al. Quality of life in metastatic pancreatic cancer patients receiving liposomal irinotecan plus 5-fluorouracil and leucovorin. Eur J Cancer. 2019;106:24–33.
Pelzer U, Blanc JF, Melisi D, et al. Quality-adjusted survival with combination nal-IRI+5-FU/LV vs 5-FU/LV alone in metastatic pancreatic cancer patients previously treated with gemcitabine-based therapy: a Q-TWiST analysis. Br J Cancer. 2017;116(10):1247–53.
Hubner RA, Chen L-T, Siveke JT, et al. Time course of selected treatment-emergent adverse events (TEAEs) in NAPOLI- 1: a phase 3 study of nal-IRI (MM-398) ± 5-fluorouracil and leucovorin (5-FU/LV) vs 5-FU/LV in metastatic pancreatic cancer (mPAC) previously treated with gemacitabine-based therapy [abstract no. 693P]. Ann Oncol. 2016;27(Suppl 6):vi207–42.
Chen L-T, Siveke J, Wang-Gillam A, et al. Safety across subgroups in NAPOLI- 1: a phase 3 study of nal-IRI (MM-398) ± 5-fluorouracil and leucovorin (5-FU/LV) versus 5-FU/LV in metastatic pancreatic cancer (mPAC) previously treated with gemcitabine-based therapy [abstract no. PD-023]. Ann Oncol. 2016;27(Suppl 2):ii102–7.
Chen L-T, Li C-P, Chiu C-F, et al. Efficacy and safety of nanoliposomal irinotecan (nal-IRI, MM-398, PEP02, BAX-2398) in patients with metastatic pancreatic cancer in Asia: a subgroup analysis of the phase 3 NAPOLI-1 study [abstract no 221PD]. Ann Oncol. 2016;27(Suppl 9):ix68–85.
ESMO Guidelines Committee. eUpdate—cancer of the pancreas treatment recommendations. Published: 20 June 2017. https://www.esmo.org. Accessed 25 Feb 2020.
National Comprehensive Cancer Network. NCCN guidelines version 1. 2020. Pancreatic adenocarcinoma (in Japanese). https://www.nccn.org/professionals/physician_gls/PDF/pancreatic-japanese.pdf. Accessed 21 Apr 2020.
Chen LT, Macarulla T, Blanc JF, et al. Nomogram for predicting survival in patients treated with liposomal irinotecan plus fluorouracil and leucovorin in metastatic pancreatic cancer. Cancers. 2019;11(8):1068.
Ioka T, Ueno M, Ueno H, et al. Liposomal irinotecan (nal-IRI) plus 5-fluorouracil/levoleucovorin (5 FU/LV) vs 5-FU/LV in Japanese patients (pts) with gemcitabine-refractory metastatic pancreatic cancer (mPAC) [abstract no. 132P]. Ann Oncol. 2019;30(Suppl 9):ix42–67.
Speer AG, Thursfield VJ, Torn-Broers Y, et al. Pancreatic cancer: surgical management and outcomes after 6 years of follow-up. Med J Aust. 2012;196(8):511–5.
Kieler M, Unseld M, Bianconi D, et al. Impact of new chemotherapy regimens on the treatment landscape and survival of locally advanced and metastatic pancreatic cancer patients. J Clin Med. 2020;9:648.
Tossey JC, Reardon J, VanDeusen JB, et al. Comparison of conventional versus liposomal irinotecan in combination with fluorouracil for advanced pancreatic cancer: a single-institution experience. Med Oncol. 2019;36:87.
de Man FM, Goey AKL, van Schaik RHN, et al. Individualization of irinotecan treatment: a review of pharmacokinetics, pharmacodynamics, and pharmacogenetics. Clin Pharmacokinet. 2018;57:1229–544.
Drummond DC, Noble CO, Guo Z, et al. Development of a highly active nanoliposomal irinotecan using a novel intraliposomal stabilization strategy. Cancer Res. 2006;66(6):3271–7.
Ko AH, Tempero MA, Shan YS, et al. A multinational phase 2 study of nanoliposomal irinotecan sucrosofate (PEP02, MM-398) for patients with gemcitabine-refractory metastatic pancreatic cancer. Br J Cancer. 2013;109(4):920–5.
Macarulla T, Brendel K, Lieu C, et al. Integrated population pharmacokinetic modelling of liposomal irinotecan in patients with various tumour types, including untreated metastatic pancreatic cancer (mPC) [abstract no. 691P]. Ann Oncol. 2019;30(Suppl 5):v263.
Adiwijaya BS, Kim J, Lang I, et al. Population pharmacokinetics of liposomal irinotecan in patients with cancer. Clin Pharmacol Ther. 2017;102(6):997–1005.
Acknowledgements
During the peer review process, the manufacturer of liposomal irinotecan was also offered an opportunity to review this article. Changes resulting from comments received were made on the basis of scientific and editorial merit.
Funding
The preparation of this review was not supported by any external funding
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
James Frampton is a salaried employee of Adis International Ltd/Springer Nature, is responsible for the article content and declares no relevant conflicts of interest.
Additional information
Enhanced material for this Adis Drug Evaluation can be found at https://doi.org/10.6084/m9.figshare.12270707.
The manuscript was reviewed by:D. Grapsa, National and Kapodistrian University of Athens, Athens, Greece; M. Harris, Department of Medical Oncology, Monash Health, Melbourne, Victoria, Australia; T. Macarulla, Gastrointestinal and Endocrine Tumor Unit, Vall d'Hebron University Hospital and Vall d'Hebron Institute of Oncology, Barcelona, Spain.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Frampton, J.E. Liposomal Irinotecan: A Review in Metastatic Pancreatic Adenocarcinoma. Drugs 80, 1007–1018 (2020). https://doi.org/10.1007/s40265-020-01336-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40265-020-01336-6