
Abstract
Background
Older people are more sensitive to drugs and adverse drug reactions than younger people because of age-related physiological changes such as impaired renal function. As people with dementia are particularly vulnerable to the effects of drugs, it is especially important to evaluate the dosages of renally cleared medications in this group.
Objective
The aim of this study was to estimate the prevalence of impaired renal function and inappropriate prescriptions on the basis of renal function among older patients with dementia or cognitive impairment.
Methods
The medical records of 428 patients aged ≥65 years who were admitted to two hospitals in northern Sweden were reviewed and renally cleared medications were identified. The Cockcroft–Gault equation was used to evaluate renal function. Doses were evaluated according to the Geriatric Dosage Handbook.
Results
Renal function was impaired (estimated glomerular filtration rate <60 ml/min) in 65.4 % of the study population. Impaired renal function was associated with increasing age. Among 547 prescriptions identified as renally cleared medications, 9.1 % were inappropriate based on the patient’s renal function; 13.5 % of the 326 patients prescribed renally cleared medications had inappropriate prescriptions. Inappropriate prescriptions were more common among patients living in nursing homes.
Conclusions
Impaired renal function is common and inappropriate prescription is prevalent among old people with cognitive impairment in northern Sweden. Continuous consideration of renal function is important when prescribing medications to this group.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Prescriptions classed as inappropriate on the basis of impaired renal function is prevalent among older people with cognitive impairment and dementia. |
Impaired renal function is common among older people with cognitive impairment and dementia. |
Continuous estimation of renal function is important in this group. |
1 Introduction
Ageing populations are characterised by an increased proportion of older people [1, 2]. In older populations, chronic diseases, including dementia and mild cognitive impairment, and comorbidity are common [2, 3]. Polypharmacy is common among older people with multiple chronic conditions. This situation is of particular concern as older people are more sensitive to drugs and adverse drug reactions (ADRs) than younger individuals [2, 4]. The changes in neurotransmitter substances that occur in people with dementia make this patient group especially vulnerable to the effects of drugs, including ADRs [1, 2, 5].
Age-related physiological changes affect the pharmacokinetic parameters of a drug, and the elimination of drugs is particularly affected by impairment of renal function [1, 2]. Renal mass declines with age as do the number and size of nephrons [6], and this process results in reduced glomerular and tubular filtration [2]. Chronic kidney disease (CKD), defined as estimated glomerular filtration rate (eGFR) <60 ml/min, is a common and growing problem in older populations [6–8]. Renally excreted drugs with narrow therapeutic indices, such as digoxin and lithium, can accumulate and concentrations can become toxic [9]. Drugs such as morphine and glibenclamide that have active metabolites may cause ADRs [10, 11]. Estimation of renal function is thus important when prescribing renally excreted drugs to older people to avoid inappropriate prescribing, which is defined as “a situation where risk from the adverse effects of a prescribed medication outweighs the desired clinical benefits of treating a particular condition” [4].
eGFR is increasingly used in healthcare to estimate patients’ renal function. The use of serum creatinine level alone as a measure of renal function is not reliable [12] because creatinine production, which is dependent on muscle mass, decreases with age; thus, the use of serum creatinine level alone leads to overestimation of renal function [1, 6]. Two commonly used methods for calculating eGFR on the basis of serum creatinine level are the Cockcroft–Gault (CG) equation and the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation [2, 13]. The CG equation calculates the absolute eGFR (ml/min) [14]. Most recommendations published in dosage handbooks are based on renal function estimated by the CG equation [2, 6]. The CKD-EPI equation calculates the relative eGFR (ml/min/1.73 m2) and is used to detect and characterise CKD [13–15]. Estimates of renal function obtained via creatinine-based equations are less accurate in certain patients such as those who are malnourished, amputees and the morbidly obese [2, 12]. Debate concerning the most suitable equation for calculating eGFR is ongoing [6, 13, 16, 17].
As people with dementia are particularly vulnerable to drugs, evaluation of whether medications need to be adjusted according to renal function is especially important in this group [5]. Several studies have evaluated older people’s prescriptions in relation to their renal function [4, 6, 8, 16, 18–22]. To our knowledge, no similar study has been conducted among people with dementia or cognitive impairment.
The purpose of this study was to estimate the prevalence of impaired renal function and inappropriate prescription of renally cleared medications among older people, aged ≥65 years, with dementia or cognitive impairment. Factors associated with impaired renal function and inappropriate prescription were also investigated.
2 Methods
2.1 Setting and Study Design
This cross-sectional study used data collected in a randomised controlled intervention study conducted in two hospitals in northern Sweden. The purpose of the intervention was to investigate whether drug-related readmissions were reduced when clinical pharmacists conducted medication reviews as part of ward teams. Patients admitted to the acute internal medicine or orthopaedic ward at Norrland University Hospital and to a medical ward at the county hospital in Skellefteå were recruited between 9 January 2012 and 2 December 2014. All admissions were emergencies, except for one that was elective. The most common reasons for admission were fractures/falls, heart failure or pneumonia. A total of 460 people were randomised to the intervention and control groups. Eligible patients were those aged ≥65 years who had dementia or cognitive impairment. Dementia diagnoses were collected from medical records. Patients were considered to have cognitive impairment if sufficient information related to memory, orientation or executive function was noted in their medical records prior to the index hospitalization. In addition, patients in whom dementia was suspected and medical investigation had been or would be commenced were included. Ambiguous or uncertain cases were excluded. The procedure described was chosen to avoid the risk of including people without dementia who had developed a delirious or confused state during the hospital stay (Gustafsson M et al., 2016, unpublished observations). Each patient in the intervention group received an additional medication review by a clinical pharmacist, while the control group received standard care.
Data for the present study were gathered from the intervention study, with the patients assigned to the intervention and control groups treated as a single study sample. The study population comprised 460 people with dementia or cognitive impairment. People who died (n = 31) or withdrew from the intervention study (n = 1) before discharge from the index hospitalization were excluded, resulting in a final sample of 428 people.
2.2 Data Extraction
Data about the patients’ medications were extracted from the medical records at the time of the patients’ index hospitalization, before any medication review was performed. The Geriatric Dosage Handbook (GDH) was used to identify renally cleared medications from among all prescribed drugs to obtain internationally applicable results [23]. Doses, strengths and drug formulations were noted for every drug at the individual patient level. Pro re nata medications, over-the-counter medications and formulations designed for local administration were not included in the analysis.
The GDH guidelines were used to evaluate whether prescriptions were inappropriate relative to patients’ renal function [23]. Another guideline was used for morphine prescriptions as the GDH guideline was considered unclear for this specific drug [10]. Moreover, mirabegron prescriptions were evaluated according to another guideline because the GDH did not include guidelines regarding this drug [24]. Angiotensin-converting enzyme inhibitors were excluded because of the large pharmacodynamic variations and because these drugs are monitored after clinical response [25]. Digoxin and dalteparin were excluded, as consideration of serum concentrations and therapeutic responses to these drugs is important [23, 26]. Inappropriate prescriptions were classified as representing excessive doses (more than the maximum daily dosage) or contraindications for patients with renal impairment according to previous research [4, 6, 19]. Prescriptions not requiring dosage adjustment were classified as having appropriate doses relative to renal function.
The classification system shown in Table 1 was used to define CKD stages. Renal function was considered to be impaired in stages 3–5 (i.e. eGFR < 60 ml/min[/1.73 m2]).
The CG equation, shown in Table S1 of the Electronic Supplementary Material (ESM), was used to calculate the eGFR (eGFRCG) to estimate the prevalence of impaired renal function and inappropriate prescription. To compare the frequencies of patients at different CKD stages using different estimation methods, the relative eGFR was calculated using the CKD-EPI equation, and the absolute eGFR was calculated from the relative eGFR values (equations shown in ESM Table S1).
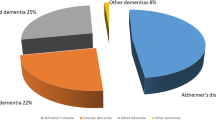
The values required to calculate eGFR were extracted from patients’ medical records. Data were collected on the date of randomisation, which was usually within 2 days (maximum 22 days) of admission date. We recorded patients’ age, sex, serum creatinine level, weight (actual) and height as well as the type of dementia, classified as Alzheimer’s disease, vascular dementia or other or unspecified (UNS) dementia. When available, Mini-Mental State Examination (MMSE) scores were recorded. Patients’ living situations were classified as living at home or in a nursing home.
2.3 Data Analysis
Descriptive statistics were used to summarise the data. Frequencies and proportions were calculated for dichotomous variables, and continuous variables are presented as mean values with standard deviations.
Simple logistic regression analyses were conducted to investigate the association between impaired renal function and factors extracted from the medical record: age, sex, living situation and MMSE score. A multiple logistic regression analysis was conducted including all variables from the simple models except MMSE score because of the large proportion of missing values and the absence of any differences found on univariate analysis.
Further, simple logistic regression analyses were conducted to investigate the association between inappropriate prescription and factors extracted from the medical record (age, sex, living situation and MMSE score). A multiple logistic regression analysis was conducted including all variables from the simple models except MMSE score because of a large proportion of missing values and the absence of any differences found on univariate analysis.
Results are presented as odds ratios (ORs) with 95 % confidence intervals (CIs). All analyses were conducted using IBM SPSS Statistics 22 (Somers, NY, USA).
3 Results
Of the 428 people included in the study, 270 (63.1 %) were women; the mean age was 83.2 ± 6.6 years. The mean ± standard deviation (SD) serum creatinine level was 89.0 ± 39.7 µmol/l. The mean eGFR, calculated using the CG equation, was 55.3 ± 22.6 ml/min. The absolute and relative eGFRs using the CKD-EPI equation were 64.8 ± 22.0 ml/min and 64.6 ± 21.1 ml/min/1.73 m2, respectively. The most common type of cognitive impairment was other or UNS dementia (n = 225 [52.6 %]), and the majority of patients (n = 304 [71.0 %]) lived at home (Table 2).
The distribution of the five CKD stages in the study sample is presented in Table 3. According to the absolute eGFR calculated using the CKD-EPI equation, 173 (41.0 %) patients were estimated to have CKD stages 3–5 (i.e. eGFR < 60 ml/min). Calculation of the relative eGFR indicated that 173 (40.4 %) patients had eGFRs < 60 ml/min/1.73 m2. According to the CG equation, 280 (65.4 %) patients were estimated to have impaired renal function (i.e. eGFR < 60 ml/min). Impaired renal function was more common among women (OR 2.046 [95 % CI 1.358–3.082]) and in older patients (OR 1.204 [95 % CI 1.154–1.256]). There were no significant differences between people with and without impaired renal function in relation to living situation or MMSE score. In a multivariable model in which impaired renal function was the dependent variable and sex, age and living situation were independent variables, age remained significant (OR 1.203 [95 % CI 1.152–1.257]) (Table 4).
Of the drugs prescribed to the 428 patients, 58 were classified as renally cleared medications; 547 prescriptions of these 58 drugs were recorded (Table 5). Of these 547 prescriptions, 50 (9.1 %) were classified as inappropriate and 497 prescriptions (90.9 %) were considered appropriate on the basis of the patient’s renal function. When absolute and relative eGFR were calculated according to the CKD-EPI equation, the corresponding prevalences of inappropriate prescriptions were 28 (5.1 %) and 32 (5.9 %), respectively. Inappropriate prescriptions were found for 20 (34.5 %) of the 58 identified drugs. Of the 50 inappropriate prescriptions, 17 were for doses that were too high and 33 were for contraindicated drugs; these constituted 3.1 % (17/547) and 6.0 % (33/547), respectively, of all identified prescriptions. Eight (47.1 %) prescriptions with excessive doses were for allopurinol and 12 (36.4 %) contraindicated prescriptions were for metformin (Table 5).
The majority (326/428 [76.2 %]) of patients in the study sample were prescribed one or more renally cleared medications. Of these 326 patients, 44 (13.5 %) had inappropriate prescriptions on the basis of their renal function; these patients constituted 10.3 % of the total study sample. Among the 326 patients prescribed one or more of the identified medications, 15 (4.6 %) had one or more prescriptions with excessive doses and 31 (9.5 %) had one or more contraindicated prescription.
Inappropriate prescriptions were more common among people living in nursing homes (OR 2.060 [95 % CI 1.073–3.954]). No significant difference was seen between people with and without inappropriate prescriptions in terms of sex, age or MMSE score. Nor were any significant associations seen in a multivariable model in which inappropriate prescriptions was the dependent variable and sex, age and living situation were independent variables (Table 6).
4 Discussion
In the present study, nearly two-thirds of patients had impaired renal function, which was associated with advancing age. Close to 10 % of the identified prescriptions were inappropriate, affecting more than 10 % of patients. The drugs most commonly involved were metformin, representing the majority of the contraindicated prescriptions, and allopurinol, representing the majority of the prescriptions with excessive doses.
According to values calculated using the CG equation, the prevalence of impaired renal function was high in the present study. The reported prevalence of impaired renal function among older people ranges from 12 to 66 % [15, 17, 27]. The wide variation in this parameter may be due to differences in study setting, individual parameters and the estimation equations used. The association between impaired renal function and advancing age found in the present study was expected and has been reported in several other studies [8, 19, 28, 29]. The rate of decline in renal function has been found to be greater in people with concomitant diseases; diabetes, for example, is one of the most common diseases associated with impaired renal function [30, 31]. In this study, no significant difference was seen between people with and without impaired renal function regarding degree of cognitive impairment. A similar result was seen in another study [27], which found no association between CKD and cognitive decline or the incidence of all-cause dementia. As the prevalence of impaired renal function in this group was high, and as impairment is often under-recognised among older people, routine monitoring to detect deteriorating renal function is important to avoid the consequences of inappropriate prescriptions [8].
In the present study, close to 10 % of the identified prescriptions were inappropriate when the CG equation was used to estimate renal function; one-third of these prescriptions had excessive doses given the patient’s renal function and two-thirds were contraindicated. When the CKD-EPI equation was used, the prevalence of inappropriate prescriptions was between 5 and 6 %. These prevalence figures differ from those reported in previous studies of drug prescriptions that were inappropriate given impaired renal function. In one study of patients aged ≥70 years, 42.2 % of identified prescriptions had doses exceeding current guidelines [21]. Another study found 13 % of prescriptions to be potentially inappropriate [18], similar to our results. While the chosen renal function estimation method might have affected the end result, we also found that the CKD-EPI equation overestimates and the CG equation underestimates renal function, which may explain the differences in prevalence seen in the present study [13, 15, 16]. Differences in the reported prevalence of inappropriate prescriptions may also be because prescribers and researchers use different prescribing or dosage guidelines [4, 6, 8, 18–21]. For example, recommendations on dosage limits for metformin differ between guidelines [23, 26, 32]. In the present study, the majority of contraindicated prescriptions were for metformin, probably because it is commonly prescribed and considered contraindicated for patients with an eGFR < 60 ml/min, according to the GDH [23]. Other guidelines continue to recommend low-dose metformin in patients with eGFRs > 30 ml/min, which would alter the prevalence of inappropriate prescription of this drug [26]. When metformin was excluded from the analysis, the prevalence of inappropriate prescription was 7.4 %. Metformin is considered the first-line treatment for type 2 diabetes mellitus, and monitoring of renal function is essential to avoid lactic acidosis in patients receiving this drug [26, 32]. In addition to metformin and allopurinol, we also documented more than one inappropriate prescription each for alendronate, glibenclamide, hydrochlorothiazide, memantine, morphine, nitrofurantoin and spironolactone. In other studies, the most frequently inappropriately prescribed drugs were non-steroidal anti-inflammatory drugs, atenolol, gabapentin, glyburide, ranitidine and nitrofurantoin [6, 8]. Glibenclamide has been associated with an increased risk of hypoglycaemia compared with other sulfonylureas, and other drugs in this class should be used for patients with impaired renal function [23, 32]. Nitrofurantoin is contraindicated because impaired renal function decreases its efficacy [23]. In general, patients with dementia or cognitive impairment are especially vulnerable to ADRs, and it is essential to avoid adverse reactions [33]. Hypoglycaemia as an adverse reaction to glibenclamide or worsening symptoms of urinary infection due to decreased nitrofurantoin efficacy may have particularly harmful consequences in this group. Older people with dementia are, on average, prescribed more medicines than older people without dementia [34]. This means it is even more important and urgent to evaluate prescriptions of renally excreted drugs to ensure that the correct doses are used and further ADRs are avoided.
In this study, multiple logistic regression analysis showed that age, sex and living in a nursing home were not significantly associated with the record of one or more potentially inappropriate prescription. In contrast, other studies have found that inappropriate prescription in relation to renal function is more common in older people and among those living in nursing homes [6, 22]. Our univariate model showed that living situation was associated with inappropriate prescription, but this association was not significant in the multivariable model. People who live in nursing homes may be older and have more concomitant diseases that affect renal function than older people living at home.
Some limitations of the present study should be recognised. No baseline data about serum creatinine were collected, nor were changes in values followed-up during hospitalization. Therefore, we could not determine whether patients’ GFRs were stable because we analysed only one serum creatinine level measurement per patient [12]. Also, no other markers of kidney damage were collected. Only one patient was admitted to the acute internal medicine ward because of acute kidney injury (AKI), but more people could possibly have suffered from AKI even if the admission was classified otherwise. Serum creatinine level was recorded on the date of randomisation, which may have differed slightly from the date of hospital admission—from which the medication prescription data were taken. Actual body weight was also used for all patients, regardless of body composition, which may have affected eGFR values for patients with unusual muscle mass. Pro re nata drugs were not included in the analysis, which may have led to underestimation of the prevalence of inappropriate prescription; for example, pro re nata doses of morphine are often prescribed. Dosage guidelines may differ between different dosage references. The GDH was chosen because of its international application and because it specifically addresses recommended doses for older people. However, the ranges for renal function were quite narrow for some of the drug dosage guidelines, which may have led to significant confounding in the present study. The cross-sectional design of the study, which involved assessment of patients’ prescriptions at the time of the medication record review, means we cannot comment on the appropriateness of medications when they were initially prescribed. Height data were lacking for six patients, which affected the absolute eGFR values calculated from the relative GFRs estimated using the CKD-EPI equation. MMSE test results were available for only 155 patients in the sample.
The study’s strengths include the examination of a well-defined group of patients and the collection of data from hospital settings and medical records, which are reliable sources of information for cross-sectional studies [35]. Data such as serum creatinine level, weight and prescribed medications were current. The CG equation was used to estimate renal function for the purpose of estimating dosages in a medical care setting at the time the study was conducted [2]. However, only serum creatinine was reported in the medical records and prescribers then had to calculate the eGFR themselves. Subsequent to completion of the study, the CKD-EPI equation has become the current standard method used to calculate the eGFR in medical records. The results thus provide a representative picture of clinical reality at the time of the study [6, 17, 23, 25].
5 Conclusion
Impaired renal function is common and inappropriate prescription is prevalent among old people with cognitive impairment in northern Sweden. When prescribing medications, continuous consideration of renal function is important to avoid ADRs among older people with dementia or cognitive impairment.
References
Rowland M, Tozer TN. Clinical pharmacokinetics and pharmacodynamics concepts and applications. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2011.
Walker R, Whittlesea C. Clinical pharmacy and therapeutics. 5th ed. Edinburgh: Churchill Livingstone Elsevier; 2012.
Eshkoor SA, Hamid TA, Mun CY, et al. Mild cognitive impairment and its management in older people. Clin Interv Aging. 2015;10:687–93.
Gheewala PA, Peterson GM, Curtain CM, et al. Impact of the pharmacist medication review services on drug-related problems and potentially inappropriate prescribing of renally cleared medications in residents of aged care facilities. Drugs Aging. 2014;31(11):825–35.
Olsson J, Bergman A, Carlsten A, et al. Quality of drug prescribing in elderly people in nursing homes and special care units for dementia: a cross-sectional computerized pharmacy register analysis. Clin Drug Investig. 2010;30(5):289–300.
Hanlon JT, Wang X, Handler SM, et al. Potentially inappropriate prescribing of primarily renally cleared medications for older veterans affairs nursing home patients. J Am Med Dir Assoc. 2011;12(5):377–83.
Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298(17):2038–47.
Rothberg MB, Kehoe ED, Courtemanche AL, et al. Recognition and management of chronic kidney disease in an elderly ambulatory population. J Gen Intern Med. 2008;23(8):1125–30.
Lucas C, Donovan P. ‘Just a repeat’—when drug monitoring is indicated. Aust Fam Physician. 2013;42(1–2):18–22.
King S, Forbes K, Hanks GW, et al. A systematic review of the use of opioid medication for those with moderate to severe cancer pain and renal impairment: a European Palliative Care Research Collaborative opioid guidelines project. Palliat Med. 2011;25(5):525–52.
Harrower AD. Pharmacokinetics of oral antihyperglycaemic agents in patients with renal insufficiency. Clin Pharmacokinet. 1996;31(2):111–9.
Stevens LA, Levey AS. Measured GFR as a confirmatory test for estimated GFR. J Am Soc Nephrol. 2009;20(11):2305–13.
Dowling TC, Wang ES, Ferrucci L, et al. Glomerular filtration rate equations overestimate creatinine clearance in older individuals enrolled in the Baltimore Longitudinal Study on Aging: impact on renal drug dosing. Pharmacotherapy. 2013;33(9):912–21.
Elinder CG, Bárány P, Heimbürger O. The use of estimated glomerular filtration rate for dose adjustment of medications in the elderly. Drugs Aging. 2014;31(7):493–9.
Corsonello A, Pedone C, Lattanzio F, et al. Association between glomerular filtration rate and adverse drug reactions in elderly hospitalized patients: the role of the estimating equation. Drugs Aging. 2011;28(5):379–90.
Karsch-Völk M, Schmid E, Wagenpfeil S, et al. Kidney function and clinical recommendations of drug dose adjustment in geriatric patients. BMC Geriatr. 2013;13:92.
Fabre EE, Raynaud-Simon A, Golmard JL, et al. Interest and limits of glomerular filtration rate (GFR) estimation with formulae using creatinine or cystatin C in the malnourished elderly population. Arch Gerontol Geriatr. 2010;50(3):e55–8.
Jones SA, Bhandari S. The prevalence of potentially inappropriate medication prescribing in elderly patients with chronic kidney disease. Postgrad Med J. 1051;2013(89):247–50.
Van Pottelbergh G, Mertens A, Azermai M, et al. Drug prescriptions unadapted to the renal function in patients aged 80 years and older. Eur J Gen Pract. 2014;20(3):190–5.
Nielsen AL, Henriksen DP, Marinakis C, et al. Drug dosing in patients with renal insufficiency in a hospital setting using electronic prescribing and automated reporting of estimated glomerular filtration rate. Basic Clin Pharmacol Toxicol. 2014;114(5):407–13.
Kalender-Rich JL, Mahnken JD, Wetmore JB, et al. Transient impact of automated glomerular filtration rate reporting on drug dosing for hospitalized older adults with concealed renal insufficiency. Am J Geriatr Pharmacother. 2011;9(5):320–7.
Khanal A, Peterson GM, Castelino RL, et al. Potentially inappropriate prescribing of renally cleared drugs in elderly patients in community and aged care settings. Drugs Aging. 2015;32(5):391–400.
Semla TP, Beizer JL, Higbee MD. Geriatric Dosage Handbook. 16th ed. Ohio: Lexicomp; 2011.
FASS. LIF—The research-based pharmaceutical industry. http://www.fass.se/LIF/product?4&userType=2&nplId=20110922000140&docType=3. Accessed 1 Oct 2014.
Khanal A, Castelino RL, Peterson GM, et al. Dose adjustment guidelines for medications in patients with renal impairment: how consistent are drug information sources? Intern Med J. 2014;44(1):77–85.
Renal Handbook. University of Louisville Division of Nephrology & Hypertension. Available from: https://kdpnet.kdp.louisville.edu/drugbook/adult/. Accessed 14 July 2015.
Helmer C, Stengel B, Metzger M, et al. Chronic kidney disease, cognitive decline, and incident dementia: the 3C Study. Neurology. 2011;77(23):2043–51.
Wang H, Fang C, Cai L, et al. Chronic kidney disease and cognitive impairment among the very old in China. Aging Clin Exp Res. 2015;. doi:10.1007/s40520-015-0433-1.
Liu W, Yu F, Wu Y, et al. A retrospective analysis of kidney function and risk factors by Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation in elderly Chinese patients. Ren Fail. 2015;37(8):1323–8.
Lindeman RD, Tobin JD, Shock NW. Association between blood pressure and the rate of decline in renal function with age. Kidney Int. 1984;26(6):861–8.
Nissenson AR, Pereira BJ, Collins AJ, et al. Prevalence and characteristics of individuals with chronic kidney disease in a large health maintenance organization. Am J Kidney Dis. 2001;37(6):1177–83.
Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association 2013 clinical practice guidelines for the prevention and management of diabetes in Canada. Pharmacologic Management of Type 2 Diabetes. Can J Diabetes. 2013;37(Suppl 1):61–8.
Hajjar ER, Hanlon JT, Artz MB, et al. Adverse drug reaction risk factors in older outpatients. Am J Geriatr Pharmacother. 2003;1(2):82–9.
Lau DT, Mercaldo ND, Harris AT, et al. Polypharmacy and potentially inappropriate medication use among community-dwelling elders with dementia. Alzheimer Dis Assoc Disord. 2010;24(1):56–63.
Strom B. Textbook of pharmacoepidemiology. 1st ed. Chichester: John Wiley Sons; 2007.
Acknowledgments
E. Sönnerstam, M. Gustafsson and M. Sjölander analysed and interpreted the data and prepared the manuscript. E. Sönnerstam and M. Gustafsson were responsible for the study concept and design and for acquisition of subjects. All authors participated in critical revision of the manuscript, contributed comments and approved the final version.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was supported financially by grants from the Swedish Dementia Association and the County Council of Västerbotten.
Conflict of interest
Eva Sönnerstam, Maria Sjölander and Maria Gustafsson have no conflicts of interest to disclose.
Ethical approval
The Regional Ethical Review Board of Umeå approved this study (Registration No. 2011-148-31M).
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Sönnerstam, E., Sjölander, M. & Gustafsson, M. Inappropriate Prescription and Renal Function Among Older Patients with Cognitive Impairment. Drugs Aging 33, 889–899 (2016). https://doi.org/10.1007/s40266-016-0408-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40266-016-0408-8