
Abstract
Background
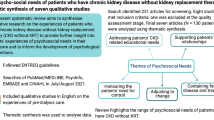
Little is known about psychological issues in patients with chronic kidney disease (CKD) facing transition to kidney failure and the involvement of their family in decision-making about kidney replacement therapy (KRT). This study investigated patients’ experience of their illness, their views on KRT choice and their perception of the influence of their relatives.
Methods
We conducted a qualitative study nested in the CKD-REIN prospective cohort study which included non-dialysis CKD patients from 40 nationally representative nephrology clinics. Among 1555 patients who returned a self-administered questionnaire, we used purposive sampling to select 50 participants who underwent semi-structured phone interviews with a psychologist.
Results
The patients' mean age was 62.2 ± 12 years, 42% were women, and 68% had CKD stage 4–5. The analysis yielded four lexical classes: “illness rhythm”, “considering dialysis”, “family and transplantation”, and “disease, treatment choice and introspection”. When experiencing few or mild symptoms, patients tended to avoid thinking about CKD, for the prospect of dialysis was the most stressful part of their experience. Surprisingly, the importance of family appeared when they talked about transplantation decision-making, but not about choice of dialysis modality.
Conclusions
Cognitive avoidance seems common in patients with advanced CKD. Transplantation and dialysis decision-making appear to be two distinct processes, with different levels of family involvement. More research is needed to better understand the frequency and impact of cognitive avoidance on patients’ well-being and decision-making.
Graphic abstract

Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Anxiety and depression are frequent in patients with moderate or advanced chronic kidney disease (CKD) [1, 2], and both are associated with worse outcomes [2, 3]. Moreover, patients reaching CKD stage 4–5 must make decisions about kidney replacement therapy (KRT), a stressful process [4]. Little is known about patients’ experience during this period. Most studies are retrospective and include patients already on dialysis, who reported feeling they lacked control over treatment choice, despite guidelines recommending shared decision-making [5, 6]. To make their choice, patients consider their preferences, and are influenced by professionals, other patients and their families [7,8,9]. A recent study did not find that depression and anxiety were associated with the choice of dialysis modality [10]. However, patients’ experience is likely to influence and be influenced by their mental health.
Previous studies on CKD have shown that patients often discuss treatment choices with their family [11, 12]. Qualitative studies investigating patients’ perspectives indicate that relatives provide support and information, and/or help patients accept KRT [6, 13]. Some patients consider the potential burden on their family in their choice [14]. As most of these studies are retrospective, investigating family influence on patients’ decision-making before KRT is necessary.
Statistical text analysis allows to investigate individuals’ experience through a quantitative analysis of their discourse. It investigates speech patterns (i.e., what they talk about and how they tell their experience). It aims to explore discourse through the words participants use and how these are associated with each other. It also allows to examine associations between parts of patients’ discourse and categorical variables. This method has previously been used in nephrology research [15, 16].
The aim of this study was to investigate patients’ experience of moderate and advanced CKD and their perception of KRT and the influence of their relatives.
Methods
Design and setting
The CKD-Renal Epidemiology and Information Network (CKD-REIN) study is a prospective cohort which enrolled 3033 patients with non-dialysis CKD from 40 nationally representative nephrology clinics between 2013 and 2016. This work was conducted under the approval of relevant ethics committees (including CCTIRS, N°12.360). Data were collected annually, including self-administered questionnaires. The study protocol and patient baseline characteristics have previously been published [17, 18]. At the third-year follow-up (2016–2019), 2260 patients who had not initiated KRT were invited to participate in a qualitative investigation by phone interview with a psychologist. Among the 1,555 pre-KRT patients who returned the self-administered questionnaire, 719 agreed to take part in the interview. We then used purposive sampling to select 50 participants so as to ensure diversity in our sample with regard to age, gender and CKD stage. The goal of this type of sampling is to intentionally select participants so they represent some explicit predefined traits. This provides for relatively equal numbers of different categories to enable exploration of the lived experience of each of these groups [19].
Data collection
Clinical research associates collected clinical data from medical records. The CKD-EPI equation was used to estimate glomerular filtration rates (GFR). Participants completed a questionnaire collecting sociodemographic information and several patient-reported measurements. The Hospital Anxiety and Depression Scale was used with possible scores ranging from 0 to 21 [20, 21]. A score above 8 was used to identify patients with significant anxiety symptoms.
The Center for Epidemiologic Studies-Depression scale was used to screen for depression symptoms [22]. Psychometric properties were explored among the patients participating in the CKDREIN-Famille study. Two items with poor saturation were excluded. A final eight-item version, with possible scores ranging from 0 to 24, showed satisfactory internal consistency (Cronbach’s α = 0.82) and fit (Comparative Fit Index = 0.98, Goodness-of-Fit Index = 0.98, Standardized Root Mean Square Residual = 0.027). A score above 8 was used to identify patients with significant depression symptoms. This cut-off was determined with a cross-multiplication based on the initial version threshold. A first interview guide was pilot tested with 3 patients. Then, qualitative data were collected by LM from audio-recorded semi-structured individual phone interviews (see interview guide in Box 1). She was a PhD student and received training from AU regarding qualitative research. She did not know the participants beforehand. She introduced herself as a psychologist-researcher then presented the interview as a means to know more about patients’ experience of CKD. Participants were asked to be in a room alone for the interview. The interviews, which took place between January 2018 and January 2019, lasted a median of 42 min [range 16–95]. LM took notes during the interviews to help her prompt the participants, however no field notes were made after the exchanges. All data were transcribed verbatim and included in the analysis. A short subjectivity statement and a description of the interpretation process are available as supplementary material. We used the Consolidated Criteria for Reporting Qualitative Research (COREQ) [23] to report key aspects of our study.
Analysis
We described the patients’ characteristics at the time of the interview and compared them between patients who consented to be interviewed and those who did not. All interviews were transcribed. We used ALCESTE® software (Analysis of Co-occurring Lexemes in a Set of Text Segments) to perform quantitative analyses of qualitative data based on the units of contexts, i.e., elements of the interviews roughly equivalent to sentences used by individuals [24]. It allows for an inductive analysis of the data. Although ALCESTE® software was developed in France it is available and used in several other languages. ALCESTE® performs a descending hierarchical classification (DHC) which yields classes of words, to which the researcher then gives meaning by investigating the words comprised in each class and their associations (see supplementary material regarding the interpretation process). The association of each word with each class is tested by a Chi-square test. A detailed description of the ALCESTE® process is available as a supplementary file. This type of analysis was chosen because it allows a quantitative analysis of large text data while keeping the strength of a qualitative approach. The software provides an automatic analysis of speech, which forms classes without the subjectivity of the researcher [15]. Moreover, ALCESTE® emphasizes not only what participants talk about but also how they tell their experience, allowing to identify patients’ implicit views.
Data saturation is a methodological principle in qualitative research referring to the point in the analytic process when no new information is discovered in the analysis and data become redundant [25]. Data saturation often occurs after 12 interviews [26]. As stated above, we chose to undertake 50 to ensure diversity. LM analyzed ALCESTE® outputs supervised by AU. The details of her interpretation process are available in the supplementary material.
A chi-square test was also performed to assess the strength of the association between patient characteristics and the classes. The following categorical variables were considered in this analysis: CKD stage, participation in patient education sessions about KRT in the past year (yes/no), discussion of treatment choices within the family (yes/no), anxiety (yes/no), and depression (yes/no).
Results
Patients’ characteristics
Patients who consented to be interviewed were younger, were less likely to be widowed, had a higher education level, greater anxiety, had better literacy skills and had more often discussed KRT with relatives than those who did not consent to an interview (see supplementary material). Interviewed patients’ mean age was 62.2 (± 12.2), 42% were women and 68.0% had stage 4–5 CKD (Table 1).
Results of the lexicometric analysis
The corpus comprising all the interviews contained 264,875 different lexical forms (i.e., words) and 5715 units of context. The DHC shows the lexical forms and the supplementary forms associated with each class and how the classes are linked with each other (Fig. 1). ALCESTE® classified 68% of the corpus into four classes.

Figure of the descendant hierarchical classification. 1These occurrences have different meanings in French. ²Some conjugated forms of these verbs were analyzed separately from their lemmatized form because they can have homonyms.3As a chi-square cannot be negative, when a minus precedes the Chi-square value it is used by the software to indicate a “relative absence” of the word in the class
Class 1: rhythm of the illness
The first class encompasses 29% of the classified corpus, it is characterized by temporal indicators, e.g., “week” and “year”, and words showing temporal relationships, e.g., “since” and “when”. It is divided into two subclasses.
The “CKD monitoring” subclass is composed of words such as “month” and month names. These terms co-occur with words pertaining to monitoring such as “result”, “appointment”, “blood” and “test/taken/sample”. CKD manifests itself through these medical events and their repetition (Table 2, Class 1, Excerpt 1).
CKD does not hurt, even though “pain” belongs to the “Managing an illness among others” subclass. This word appears in negative sentences or refers to other diseases (Class 1, Excerpt 2). Moreover, this subclass is composed of words designating medical fields: “cardiologist” and “urologist”. This result shows that CKD is one illness among others (Class 1, Excerpts 3–4).
Words pertaining to KRT and decision-making, e.g., “choice” or “dialysis”, are significantly absent in class 1 and suggest that before they face kidney failure, patients are not thinking about KRT. Moreover, the absence of the terminology of family from this class indicates that CKD monitoring is an individual experience.
This class is associated with several variables: anxious and depressed patients, non-attendance at patient education about KRT, and not talking about KRT with relatives. Patients with stages 3 and 5 CKD are associated with this class while those living with stage 4 CKD are significantly absent from it.
Class 2: considering dialysis
This class covers 15% of the classified corpus and is divided into two subclasses.
“Dialys + ”, “machine”, “peritoneal + ” and “house/home” appear in the “Dialysis modalities and daily life” subclass. Patients describe different types of dialysis and how these could be implemented in their life. “Know”, “sort/kind”, “near” (found in the expression “à peu près”, literally, “a little near”, or roughly/almost) and “uh” show how patients may perceive their knowledge on this subject as approximate (Class 2, Excerpt 1).
Dialysis modalities are described according to where they can be implemented (“house/home”, “hospital”, “at”), when and how long the treatment takes place (“hour”, “night”) and the degree of freedom allowed (“autonom + ”, “free”) (Class 2, Excerpt 2). “Opt” and “choose” show the beginning of a decision-making process (Class 2, Excerpt 3).
The “Patient education and treatment choice” subclass includes words related to patient education (e.g., “meeting”, “to show” and “information”) (Class 2, Excerpt 4) which allows patients to grasp how treatments “function”, obtain information and understand the “advantages”/ “disadvantages” of each modality (Class 2, Excerpt 5). “Have to”, “can/be able”, “etc.” and “constraint” show that the obligations of dialysis are perceived as numerous and burdensome (Class 2, Excerpt 6). Words referring to family are significantly absent from class 2, relatives may not be considered in reflections on dialysis modalities.
This class is associated with: stage 4 CKD, attendance at patient education sessions, discussions about treatment with their family, and no depression.
Class 3: family and transplantation
The third class comprises the smallest part of the classified corpus (13%). It can be divided into two subclasses.
“To bother + ”, “to recount”, “mother” and “colleague” belong to the “Talking about the illness” subclass. Patients sometimes choose (not) to speak about their illness. The quantity of details they go into depends on who they are speaking to. They do not want to overwhelm their relatives (Class 3, Excerpts 1–3).
Patients are also informers. “Hide”, “current” (found in the expression “au courant” which means know about/be informed), “world” (found in the expression “tout le monde”, literally “all the world”, everyone) and “hear” show with whom patients share information and their experience (Class 3, Excerpts 2–3).
The “Talking about transplantation” subclass includes “to give”, “compatible, “to decease” and “to refuse.” When patients think about transplantation, they also think about their family. Relatives may, for example, offer a kidney, which may or may not be possible (Class 3, Excerpt 4). Moreover, patients may refuse a donation perceived as unthinkable to accept (e.g., a son offering a kidney to his mother) (Class 3, Excerpt 5).
More rarely, patients mention they have asked relatives if they could be donors or have talked to them about deceased-donor transplantation (Class 3, Excerpts 6–7). Interestingly, “dialysis” is significantly absent from this class.
Class 3 is associated with depression and attendance at patient education sessions. Moreover, Class 3 opposes Class 2 in the factorial correspondence analysis (Fig. 2). Dialysis (Class 2) and transplantation (Class 3) do not appear together in patients’ discourse. They belong to different decision-making processes.

Schematic representation of the factorial analysis of patients’ discourse
Class 4: disease, treatment choice and introspection
The fourth class contains the largest portion of the classified corpus (43%). It includes markers of discursive relations (e.g., “but”, “if”) and modal words (e.g., “no”, “I think”). These terms show how this class pertains to reflections about CKD. It is divided into three subclasses.
The “A normal life” subclass highlights how patients say they have a “normal” “life.” Their illness is not an important element of their day-to-day life (e.g., “sick”, “health”).The only symptom they report is fatigue (Class 4, Excerpts 1–2).
However, some words temper this idea. A French expression equivalent to “quotation mark” (found in the expression “in quotation marks”), “impression”, “to evolve” and “to arrive/to happen” show how this normality is perceived as relative. Patients know their disease will progress and fear its development (Class 4, Excerpts 3–4). “Haha”, “Pff” and other interjections show the participants’ affective attitudes (Class 4, Excerpt 5).
The “Avoiding thinking about CKD” subclass shows that as CKD has little impact on patients’ day-to-day life, participants say they do not “think” much about their illness (Class 4, Excerpt 6). However, words such as “instant” (found in the expression “for the instant”, for right now), “mind” and “happen” temper this conclusion. Patients do not want to “stress” in advance, but they are aware of the temporary nature of their situation (Class 4, Excerpt 7). “Try” and “manage” are used to describe the management of CKD. They can refer to present and future ways to cope with it (Class 4, Excerpts 9–10).
Class 4 is characterized by demonstratives, relatives and indefinites (e.g., “other”, “what + ”) that designate without naming. Moreover, “thing” is strongly associated with this class and subclass. These words are used to talk about CKD, KRT or their physical/psychological consequences (Class 4, Excerpt 8).
The subclass “Research participation, treatment choice and acceptance” shows how patients accept their illness under certain conditions (e.g., “to continue”). They do not think of themselves as sick. Therefore, “to accept” refers mainly to KRT (Excerpts 11–12). “Question” can refer to questions patients ask others (e.g., their nephrologist) and questions they ask themselves (e.g., about KRT). Moreover, patients feel decision-making is not a current concern, which makes “answering” the interview questions hard (Class 4, Excerpt 13).
This class is associated with patients who are neither depressed nor anxious.
Discussion
This study is one of the first to interview a diverse sample of patients about treatment decision-making before KRT and to investigate participants’ experience with moderate to advanced CKD. It shows that statistical text analysis is an interesting method as it allows the simultaneous investigation of what participants are talking about and how they are doing it. Our results show that CKD is manifested for patients not through symptoms but through its monitoring. They also emphasize how common cognitive avoidance about disease progression is in pre-KRT patients. Cognitive avoidance encompasses a variety of coping strategies aimed at escaping thoughts about undesirable situations, including denial of the disease [27]. It may be used by patients to reduce their anxiety regarding KRT decision-making. Although effective for reducing negative emotions in the short-term, avoidance probably leads to heightened negative affects (e.g., depression, anxiety) in the long term, as has been shown in other populations [28, 29]. Moreover, transplantation and dialysis belong to two distinct decision-making processes. Family plays an important role in transplantation choice by sharing opinions and by (not) offering a kidney. The novelty of this study is that patients were interviewed before KRT and thus it provides an accurate and contemporaneous understanding of patients’ decision-making process.
The analysis encompasses 68% of the entire corpus, which is satisfactory according to recommendations (> 50%) [30]. The most important class in terms of analyzed corpus quantity shows that patients report having a normal life (class 4). It is patients’ monitoring that attests to the existence of CKD (class 1). What makes it stressful is not its physical impact but its progression towards kidney failure. Previous studies showed similar results [31, 32]. Patients' current health status may lead to cognitive avoidance, which may delay decision-making [31, 33]. It might nonetheless be adaptive in the short term, especially at stage 3, if it does not prevent patients from engaging in healthy behaviors. Further research should investigate the frequency and impact of cognitive avoidance in advanced-stage CKD patients.
Regarding KRT decision-making, dialysis choice seems guided by patient education, whereas family has a central role in decision-making about transplantation, especially living donation. Interestingly, family does not influence the consideration of dialysis in this pre-decision stage, according to patients. Yet, other authors have emphasized how family influences the choice of home dialysis [34]. Two reasons might explain these conflicting results. First, most past studies are retrospective [6, 8, 34]. Thus, patients may have experienced retrospective bias and overestimated family influence. Second, nearly half of our participants were at stage 3 and might not yet have reached this decision-making process. Patients may contemplate dialysis only when transplantation is impossible, while most of them undergo dialysis before transplantation [35]. Some patients have a strong aversion toward dialysis [36]. Consequently, some may talk about dialysis with their relatives in a second phase.
Classes identified by our analysis were associated with categorical variables. Class 1 (“Rhythm of the illness”) does not include KRT decision-making. It is associated with patients with stage 3 or 5 CKD whereas class 2 (“Considering Dialysis”) is associated with stage 4 CKD. This may show that treatment choice occurs during stage 4. Patients in stage 3 may not feel concerned by KRT whereas stage 5 patients may have already made their choice. This result is consistent with the current guidelines for KRT decision-making [5]. Class 4 is associated with low levels of depression and anxiety, it is characterized by self-reflection linked to better mood [37,38,39]. Treatment choice may be hindered by mental health issues. Indeed, several studies showed that decision-making is affected by depression and anxiety [40].
Limitations in our study warrant mention. First, it is cross-sectional and what the patients said reflected what they were experiencing at the time of the interview. Some participants were not facing impending KRT decision-making. Treatment choice requires further research aimed at advanced-stage patients to assess changes in their discourse. Second, despite the strengths of statistical text analysis, it is based on word count [24]. Yet people may use different words to describe similar experiences. Some topics could be mentioned once and be meaningful without being statistically significant (e.g., thoughts about death). Moreover, due to the qualitative nature of this study and the use of purposive sampling, the results are not generalizable. Indeed, qualitative research usually does not aim for generalizability but rather for transferability [41]. Finally, we can hypothesize that the interviewees were more concerned by KRT as they are younger, more educated, with stage 4 or 5 CKD and anxious.
Clinical perspectives
Investigating patients’ perspective on CKD and their care path allows to open new perspectives to improve care and patients’ quality of life. Attending education programs to select KRT is important, but does not seem to be sufficient [42]. Patients should be educated and empowered to achieve the health outcomes and life goals that are meaningful and important to them, through communication and education skills, patient resilience, strengthening social connections, and access to support [42, 43]. Social workers, fellow patients and psychologists should be included in the conception of such programs in order to help reduce patient cognitive avoidance and decisional conflict [44]. Our results also highlight the importance of including patients’ families in educational interventions, especially regarding transplantation, which have proved to be effective [45]. Moreover, coordinating patients’ care pathways, as recently implemented for those with CKD stage 4 or higher in France, could reduce cognitive avoidance and lead to more satisfying KRT choices.
Conclusion
This study underlines that cognitive avoidance is common in patients and that dialysis and transplantation belong to two distinct decision-making processes. Although cognitive avoidance may be adaptive, healthcare teams should be watchful as it may affect patients’ well-being and their satisfaction with decision-making. Patients seem not to contemplate dialysis when transplantation is an option and may rush their dialysis modality choice when reaching kidney failure. Finally, family plays an important role in treatment choice, especially when transplantation is considered. Thus, caring for patients and their families seems relevant during KRT decision-making. Further research should investigate relatives’ experiences to better understand their role.
References
Palmer SC, Vecchio M, Craig JC et al (2013) Association between depression and death in people with CKD: a meta-analysis of cohort studies. Am J Kidney Dis 62:493–505
Loosman WL, Rottier MA, Honig A, Siegert CEH (2015) Association of depressive and anxiety symptoms with adverse events in Dutch chronic kidney disease patients: a prospective cohort study. BMC Nephrol 16:155
Tsai Y-C, Chiu Y-W, Hung C-C et al (2012) Association of symptoms of depression with progression of CKD. Am J Kidney Dis 60:54–61
Harwood L, Clark AM (2013) Understanding pre-dialysis modality decision-making: A meta-synthesis of qualitative studies. Int J Nurs Stud 50:109–120
Covic A, Bammens B, Lobbedez T et al (2010) Educating end-stage renal disease patients on dialysis modality selection: clinical advice from the European Renal Best Practice (ERBP) Advisory Board. Nephrol Dial Transpl 25:1757–1759
Morton RL, Tong A, Howard K, Snelling P, Webster AC (2010) The views of patients and carers in treatment decision making for chronic kidney disease: systematic review and thematic synthesis of qualitative studies. BMJ 340:c112
Harwood L, Clark AM (2014) Dialysis modality decision-making for older adults with chronic kidney disease. J Clin Nurs 23:3378–3390
Murray MA, Brunier G, Chung JO et al (2009) A systematic review of factors influencing decision-making in adults living with chronic kidney disease. Patient Educ Couns 76:149–158
Walker RC, Howard K, Morton RL, Palmer SC, Marshall MR, Tong A (2016) Patient and caregiver values, beliefs and experiences when considering home dialysis as a treatment option: a semi-structured interview study. Nephrol Dial Transpl 31:133–141
Bezerra CIL, Silva BC, Elias RM (2018) Decision-making process in the pre-dialysis CKD patients: do anxiety, stress and depression matter? BMC Nephrol 19:98
Griva K, Li ZH, Lai AY, Choong MC, Foo MWY (2013) Perspectives of patients, families, and health care professionals on decision-making about dialysis modality–the good, the bad, and the misunderstandings! Perit Dial Int 33:280–289
Lamore K, Montalescot L, Untas A (2017) Treatment decision-making in chronic diseases: What are the family members’ roles, needs and attitudes? A systematic review. Patient Educ Couns 100:2172–2181
Loiselle M-C, Michaud C, O’Connor A (2016) Decisional needs assessment to help patients with advanced chronic kidney disease make better dialysis choices. Nephrol Nurs J 43:463–493
Tong A, Palmer S, Manns B et al (2013) The beliefs and expectations of patients and caregivers about home haemodialysis: an interview study. BMJ Open 3:e002148
Vioulac C, Aubree C, Massy ZA, Untas A (2016) Empathy and stress in nurses working in haemodialysis: a qualitative study. J Adv Nurs 72:1075–1085
Montalescot L, Rascle N, Combe C, Untas A (2021) Patients’ experience one year after dialysis initiation: a lexicometric analysis. Health Psychol Behav Med 9:380–397
Stengel B, Combe C, Jacquelinet C et al (2014) The French Chronic Kidney Disease-Renal Epidemiology and Information Network (CKD-REIN) cohort study. Nephrol Dial Transpl 29:1500–1507
Stengel B, Metzger M, Combe C et al (2019) Risk profile, quality of life and care of patients with moderate and advanced CKD: The French CKD-REIN Cohort Study. Nephrol Dial Transpl 34:277–286
Luborsky MR, Rubinstein RL (1995) Sampling in qualitative research. Res Aging 17:89–113
Zigmond AS, Snaith RP (1983) The Hospital Anxiety And Depression Scale. Acta Psychiatr Scand 67:361–370
Untas A, Aguirrezabal M, Chauveau P, Leguen E, Combe C, Rascle N (2009) Anxiété et dépression en hémodialyse : validation de l’Hospital Anxiety and Depression Scale (HADS). Nephrol Ther 5:193–200
Kohout FJ, Berkman LF, Evans DA, Cornoni-Huntley J (1993) Two shorter forms of the CES-D (Center for Epidemiological Studies Depression) depression symptoms index. J Aging Health 5:179–193
Tong A, Sainsbury P, Craig J (2007) Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care 19:349–357
Reinert M (1990) Alceste une méthodologie d’analyse des données textuelles et une application: Aurelia De Gerard De Nerval. Bull Methodol Sociol 26:24–54
Saunders B, Sim J, Kingstone T et al (2018) Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant 52:1893–1907
Guest G, Bunce A, Johnson L (2006) How many interviews are enough? An experiment with data saturation and variability. Field Methods 18:59–82
Sagui-Henson SJ (2017) Cognitive avoidance. In: Zeigler-Hill V, Shackelford TK (eds) Encyclopedia of personality and individual differences. Springer International Publishing, New-York City, pp 1–3
Dickson KS, Ciesla JA, Reilly LC (2012) Rumination, worry, cognitive avoidance, and behavioral avoidance: examination of temporal effects. Behav Ther 43:629–640
Tan PZ, Forbes EE, Dahl RE et al (2012) Emotional reactivity and regulation in anxious and nonanxious youth: a cell-phone ecological momentary assessment study. J Child Psychol Psychiatry 53:197–206
Rastier F, Cavazza M, Abeillé A (1994) Sémantique pour l’analyse: De la linguistique à l’informatique. Dunod, Malakoff
Lissanu L, Lopez F, King A et al (2019) “I Try Not to Even Think About My Health Going Bad”: a Qualitative Study of Chronic Kidney Disease Knowledge and Coping Among a Group of Urban African-American Patients with CKD. J Racial Ethn Health Disparities 6:625–634
Jennette C, Derebail V, Baldwin J, Cameron S (2009) Renal replacement Therapy and Barriers to choice: using a Mixed Methods approach to explore the Patient’s Perspective. J Nephrol Soc Work 32:15–26
Lovell S, Walker RJ, Schollum JBW, Marshall MR, McNoe BM, Derrett S (2017) To dialyse or delay: a qualitative study of older New Zealanders’ perceptions and experiences of decision-making, with stage 5 chronic kidney disease. BMJ Open 7:e014781
Walker RC, Hanson CS, Palmer SC et al (2015) Patient and caregiver perspectives on home hemodialysis: a systematic review. Am J Kidney Dis 65:451–463
European Renal Association-European Dialysis and Transplant Association (2016) ERA-EDTA Registry Annual Report 2016. Amsterdam, The Netherlands
Hanson CS, Chadban SJ, Chapman JR et al (2015) The expectations and attitudes of patients with chronic kidney disease toward living kidney donor transplantation: a thematic synthesis of qualitative studies. Transplantation 99:540–554
Kross E, Ayduk O (2017) Self-distancing: theory, research, and current directions. Adv Exp Soc Psychol 55:81–136
Kauer SD, Reid SC, Crooke AHD et al (2012) Self-monitoring using mobile phones in the early stages of adolescent depression: randomized controlled trial. J Med Internet Res 14:e67
Takano K, Tanno Y (2009) Self-rumination, self-reflection, and depression: self-rumination counteracts the adaptive effect of self-reflection. Behav Res Ther 47:260–264
Bishop SJ, Gagne C (2018) Anxiety, depression, and decision making: a computational perspective. Annu Rev Neurosci 41:371–388
Lincoln YS, Guba EG (1985) Naturalistic inquiry. SAGE, London
Yeh M-Y, Wu S-C, Tung T-H (2018) The relation between patient education, patient empowerment and patient satisfaction: a cross-sectional-comparison study. Appl Nurs Res 39:11–17
Joseph-Williams N (2014) Knowledge is not power for patients: a systematic review and thematic synthesis of patient-reported barriers and facilitators to shared decision making. Patient Educ Couns. https://doi.org/10.1016/j.pec.2013.10.031
Zarling A, Lawrence E, Marchman J (2015) A randomized controlled trial of acceptance and commitment therapy for aggressive behavior. J Consult Clin Psychol 83:199–212
Lopez-Vargas PA, Tong A, Howell M, Craig JC (2016) Educational interventions for patients with CKD: a systematic review. Am J Kidney Dis 68:353–370
Acknowledgements
We acknowledge the CKD-REIN study coordination staff for their efforts in setting up the CKD-REIN cohort: Marie Metzger, Elodie Speyer, Céline Lange, Reine Ketchemin, Sophie LIabeuf, Christian Jacquelinet, Natalia Alencar de Pinho and all the clinical research associates. We thank Jo-Ann Cahn for editing the English version. Authorizations: All legal authorizations were obtained including those from the Comité consultatif sur le traitement de l'information en matière de recherche dans le domaine de la santé (CCTIRS N°12.360), the Commission nationale de l’informatique et des libertés (CNIL N°DR-2012-469), and from the Kremlin-Bicêtre Comité de protection des personnes (CPP N°IDRCB 2012-A00902-41). CKD-REIN biological collection is registered in the management application of the COnservation D'Eléments du COrps Humain (CODECOCH N°-2012-1624). The Institut national de la santé et de la recherche médical (Inserm) Institutional Review Board approved the study protocol (IRB00003888). ClinicalTrials.gov Identifier: NCT03381950.
Funding
CKD-REIN is funded by the Agence Nationale de la Recherche through the 2010 «Cohortes-Investissements d’Avenir» program (ANR-IA-COH-2012/3731) and by the 2010 national Programme Hospitalier de Recherche Clinique. CKD-REIN is also supported through a public–private partnership with Amgen, Fresenius Medical Care, and GlaxoSmithKline (GSK), since 2012, Lilly France since 2013, and Otsuka Pharmaceutical since 2015, Baxter and Merck Sharp & Dohme-Chibret (MSD France) from 2012 to 2017, Sanofi-Genzyme from 2012 to 2015, Vifor Fresenius, and AstraZeneca, since 2018. Inserm Transfert set up and has managed this partnership since 2011. CKDREIN-Famille was supported by France Rein (a patient association) and the Fondation de France from 2017 to 2019.
Author information
Authors and Affiliations
Contributions
LM drafted the article. GD, ES, KL, CA, CC, BS and AU contributed to the study design and/or the conception of questionnaires, provided intellectual content to the work described and revised the manuscript. LM performed the analyses supervised by AU. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
CKD-REIN is supported by a public–private partnership with funding from 9 pharmaceutical companies as listed above. This paper has not been published previously in whole or part.
Ethical statement
All legal authorizations were obtained including those from the Comité consultatif sur le traitement de l'information en matière de recherche dans le domaine de la santé (CCTIRS N°12.360), the Commission nationale de l’informatique et des libertés (CNIL N°DR-2012-469), and from the Kremlin-Bicêtre Comité de protection des personnes (CPP N°IDRCB 2012-A00902-41).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Montalescot, L., Dorard, G., Speyer, E. et al. Patient perspectives on chronic kidney disease and decision-making about treatment. Discourse of participants in the French CKD-REIN cohort study. J Nephrol 35, 1387–1397 (2022). https://doi.org/10.1007/s40620-022-01345-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40620-022-01345-6