
Abstract
Introduction
Nosocomial pneumonia is a common infection associated with high mortality in hospitalized patients. Nosocomial pneumonia, caused by gram-negative bacteria, often occurs in the elderly and patients with co-morbid diseases.
Methods
Original research using a prospective cross-sectional design was conducted on 281 patients in an intensive care unit setting with nosocomial pneumonia between July 2015 and July 2019. For each nosocomial pneumonia case, data regarding comorbidities, risk factors, patient characteristics, Charlson comorbidity index (CCI), Systemic Inflammatory Response Syndrome (SIRS), and quick Sepsis-Related Organ Failure Assessment (qSOFA) points and treatment outcomes were collected. Data were analyzed by SPSS 22.0.
Results
Nosocomial pneumonia due to gram-negative bacteria occurred in patients with neurological disorders (34.87%), heart diseases (16.37%), chronic renal failure (7.12%), and post-surgery (10.68%). Worse outcomes attributed to nosocomial pneumonia were high at 75.8%. Mechanical ventilation, change of antibiotics, and CCI ≥ 3 and qSOFA ≥ 2 were significantly negative prognostic factors (p < 0.05) on outcomes of nosocomial pneumonia. There was no difference in treatment effects between gender, age, time of onset pneumonia, SIRS score (p > 0.05). The pathogens were significant factors that influence treatment effects, but they weren’t independent risk factors for poor outcomes (p = 0.823).
Conclusions
Patients with nosocomial pneumonia hospitalized in intensive care units are usually associated with many underlying diseases, including neurological diseases. Mechanical ventilation, a change in antibiotics, CCI ≥ 3, and qSOFA ≥ 2 are also associated with a worse prognosis of nosocomial pneumonia. CCI and qSOFA might be used in predicting the outcome of nosocomial pneumonia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Nosocomial pneumonia (NP) due to gram-negative bacteria was the most acquired infection in hospitals. Finding risk factors was an important role that helps to improve mortality and poor outcomes of NP. |
This study found associations of risk factors and functions of quick Sepsis-Related Organ Failure Assessment (qSOFA), Systemic Inflammatory Response Syndrome (SIRS), and Charlson comorbidity index (CCI) scores in predicting worse clinical outcomes among patients with NP due to gram-negative bacteria. |
What was learned from the study? |
Neurological diseases increased to develop nosocomial pneumonia in intensive care unit patients. |
Risk factors, including mechanical ventilation and a change in antibiotics, were associated with a worse prognosis of nosocomial pneumonia. |
qSOFA and CCI scores were simple and valuable scores in predicting treatment outcomes to assist clinical decision-making. |
Introduction
Nosocomial pneumonia (NP) is the most commonly acquired infection in hospitals. In 2008, research on the incidence of NP in ten Asian countries, including China, Hong Kong, Malaysia, Pakistan, Philippines, Singapore, Korea, Taiwan, India, and Thailand, showed that infection rates ranged from 6.1 to 15% in an intensive care unit (ICU). In this study, China had 1.0 per 1000 admissions due to NP, but in 2016, the incidence of NP increased rapidly, comprising 30.1% of ICU patients in 25 hospitals [10, 18]. In Vietnam, the results of a nationwide investigation of 19 hospitals showed that NP accounted for 55.45% of hospital-acquired infections and lasted from 6 to 13 days, increasing the cost of hospitalization by 15–23 million VND [5].
Furthermore, there is evidence that gram-negative bacteria infection is a major factor that leads to increased mortality and morbidity of NP [17, 19]. In addition, some studies from different countries have shown that there are six factors, including late-onset NP, multilobar pneumonia, mechanical ventilation, inappropriate antibiotic therapy, severe sepsis, and septic shock, which might be significantly associated with high mortality and poor outcomes of NP [12, 22, 29]. Therefore, understanding risk factors that impact clinical effects is essential to predict and prevent adverse outcomes.
Several studies have investigated the utility of risk scores in predicting treatment outcomes to assist clinical decision-making in recent years. Charlson comorbidity index (CCI), quick Sepsis-Related Organ Failure Assessment (SOFA), and Systemic Inflammatory Response Syndrome (SIRS) scores are convenient and straightforward measures that have utility as clinical predictors. Research shows that qSOFA and CCI scores are useful for prognostication in patients with community-acquired pneumonia [2, 3, 16]. However, there is relatively little research regarding the roles of qSOFA and CCI scores in NP. In this study, we found associations of risk factors and functions of qSOFA, SIRS, and CCI scores in predicting worse clinical outcomes among patients with NP due to gram-negative bacteria at a public hospital in southern Vietnam.
Methods
Design and Patients
This prospective cross-sectional study was undertaken in an ICU at Can Tho General Central Hospital Vietnam with 281 patients from July 2015 until July 2019. Adult patients (aged 18 years old and over) diagnosed with first-ever NP with any underlying diseases or conditions and treated in an ICU were considered for possible inclusion in the study. NP was defined as pneumonia that occurred 48 h or more after admission within an ICU or other wards. NP participants were followed up on the seventh day after commencing treatment with antibiotics for NP or death. Exclusion criteria were acute pulmonary edema, other active pulmonary diseases, or lack of diagnostic tests to confirm pneumonia, or gram-positive bacteria or AFB positive test.
The study was conducted at Can Tho Central General hospital with 500 beds, including 30 beds in the ICU. We chose to routinely evaluate patients on the seventh day, as the average length of stay at an ICU ranged between 7 and 10 days.
Researchers responsible for data collection obtained consent from the participants who were given information regarding the purpose of the study and understood that they could withdraw at any point in the survey without it affecting their care. The Institutional Review Board approved this observational study of Can Tho University of Medicine and Pharmacy, Vietnam with 1530/QD—DHYDCT in June 2015. This study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments. Antibiotic treatment was administered according to hospital guidelines.
Definition of Nosocomial Pneumonia
NP was defined as pneumonia 48 h or more after admission with: the presence of new or worsened pulmonary infiltrates on chest X-ray and at least one of the following criteria: leukocyte count above 12,000/mm3 or below 4000/mm3 or temperature above 38.3 °C, and at least two clinical criteria: purulent sputum; cough, or dyspnea; declining oxygenation or increased oxygen-requirement or need for respiratory assistance. NP included hospital-acquired pneumonia (HAP) and ventilator-associated pneumonia (VAP) [20]. HAP was an episode of NP that was not associated with mechanical ventilation for at least 48 h. VAP is defined as a condition developed more than 48 h after intubation and ventilation [13, 23].
Definition of Variables
Charlson comorbidity index (CCI) is a combined risk score used to quantify an individual’s disease burden and corresponding 1-year mortality risk. We calculated the CCI score based on the methodology applied in previous studies [9, 24]. As a CCI score ≥ 3 was found to be associated with a high risk of death or failure treatment, we used this cut-off point for our analyses [7].
Systemic inflammatory response syndrome (SIRS) and Quick Sequential Organ Failure Assessment (qSOFA) are system scores for predicting mortality in sepsis patients [6, 27]. A high risk for sepsis is defined as SIRS ≥ 2 or qSOFA ≥ 2 [15].
Early onset NP and late-onset NP are defined as occurring within 4 days of admission, respectively [14].
A change of antibiotics was defined as adding or switching to another antibiotic with a broader antibacterial spectrum after having results of antimicrobial susceptibility testing [22].
Data Collection
Datasets of patients in the ICU department were obtained from medical records as soon as patients were diagnosed with NP. The following data were recorded for all patients on baseline characteristics: age, sex, risk factors, underlying disease, calculated Charlson comorbidity index (CCI), systemic inflammatory response syndrome (SIRS), and quick Sequential Organ Failure Assessment (qSOFA) scores. The time of onset of pneumonia and antibiotic use process was recorded as well.
Changing the initial antibiotic was considered a bad factor for treatment progress. Antibiotic is the most important option for treating infectious diseases. Nevertheless, there are various reasons leading to difficulty in selecting the initial antibiotic therapy. Changing initial antibiotics often occurs when an antibiogram shows the resistance of bacteria to prescribed antibiotics or the worse clinical status after conducting initial antibiotic therapy. All participants were monitored for use and change of antibiotics and mortality/morbidity on day 7. We also evaluated clinical outcomes on day 7.
Outcomes
The primary outcome measure was any negative outcome at 7 days after NP. Worse outcome (or adverse prognosis) was defined as mortality for any causes after diagnosing NP, or a worsening of clinical status (C-reactive protein ratio of > 0.4 and no improvement in pulse, temperature, blood pressure, and oxygen saturation) at 7 days [8].
Statistical Analysis
Risk factors were calculated as frequency and estimated with 95% confidence intervals (CIs). Data were analyzed using SPSS version 22.0. Statistically significant differences in values (age, sex, ventilate invasion, antibiotic essentials, Charlson comorbidity index, SIRS, and qSOFA score) between cases were analyzed using conditional logistic regression modeling, with variables with a p value < 0.1 on the univariate analysis included in the models. Statistical significance was established at p < 0.05. Odds ratio (OR), 95% CIs, and p values were performed for all univariate and multivariate models. OR > 1 may increase the odds of an outcome.
Results
Characteristic of Patients
During the 4 years, 281 patients were identified as having NP due to gram-negative bacteria, including 161 men (57.3%) and 120 (42.7%) women (Fig. 1). The mean ((± SD) value of the age of patients was 70.49 ± 15.04 years, with two-thirds aged 65 years old and over. Of the patients, 67.62% had late-onset pneumonia, and 58.01% had VAP. Neurological disorders were the most common comorbidity associated with NP. Almost all patients were treated with antibiotics, but 82.92% had antibiotics added or changed (Table 1). Microbial etiology was the significant difference between HAP and VAP (Table 2). The pathogens were also associated with the department before being admitted to the ICU (Table 3).

Flow diagram of the study population
Outcome of Treatment
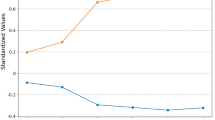
The rate of worse outcomes was high at 75.8%. Many factors were associated with negative effects such as age, sex, time onset of pneumonia, underlying disease, ventilator, and scores. Pathogens, mechanical ventilation (MV), change of antibiotics, and qSOFA ≥ 2 were significantly associated with an unfavorable prognosis (p < 0.01). In contrast, SIRS was not significant in predicting outcomes (Table 4), and the association of MV and CCI ≥ 3 with worse results was stronger after accounting for covariates in a fully adjusted model (Fig. 2).

Risk factors for predicting negative treatment effect of nosocomial pneumonia due to gram-negative bacteria. The worse outcome was defined as mortality for any causes or a worsening of clinical status (C-reactive protein ratio of > 0.4 and no improvement in pulse, temperature, blood pressure, and oxygen saturation) at 7 days after nosocomial pneumonia. Statistics performed by binary logistic regression. Statistical significance was established at p < 0.05 and OR > 1 may increase the odds of an outcome. Charlson comorbidity index (CCI) is a combined risk score used to quantify an individual’s disease burden and corresponding 1-year mortality risk. Quick Sequential Organ Failure Assessment (qSOFA) scores are system scores for predicting mortality in sepsis patients
Discussion
In the present study, CCI was a strong predictor of worse outcomes for NP. This was consistent with published research. In 2021, a study of 459 pneumonia patients reported that CCI was a significantly good predictor of mortality with AUC (0.83) [3]. As indicated by CCI ≥ 3, multimorbidity was a strong predictor of poor outcomes among patients with NP [7].
Initial qSOFA was found to be useful in predicting response to treatment in NP patients. Our study, to our knowledge, is the first to date to demonstrate the utility of qSOFA among patients with NP in an ICU setting. In a cohort study of 6874 patients from two Spanish university hospitals, SIRS and qSOFA scores were calculated to evaluate their clinical utility and hospital mortality. SIRS had a lower net benefit than qSOFA, significantly increasing the risk of over-treatment and underperforming in predicting mortality [21, 25]. Similarly, in our research, qSOFA ≥ 2 was associated with an increased risk for worse outcomes. This suggests that the qSOFA is straightforward but helpful for evaluating the severity of community-acquired pneumonia [27, 30] and NP.
MV and change of initial antibiotics were important predictive factors of poor outcomes after NP. The findings are consistent with those from previous studies [1, 4, 11, 22, 23]. Any change in antibiotic therapy after 72 h can cause increased antibiotic resistance, which is considered a factor in increasing the length of days in hospital and treatment failure [22, 23]. Furthermore, ventilation was required for severe respiratory failure, and multiple infiltrates in the lung, which did not respond to initial antibiotics [4, 11].
The pathogens were major factors of worse outcomes, but they were not independent risk factors that influenced treatment outcomes. The pathogens are different in the department and types of NP. Acinetobacter baumannii, Pseudomonas aeruginosa, and Klebsiella pneumoniae) were common pathogens for NP in Asian countries and they were also multidrug-resistant bacteria in Vietnam. Therefore, treatment for microbial etiology in NP was complex [10, 11].
Our study showed no differences in age and time onset of pneumonia between groups, consistent with other studies. Similarly, there were no differences in antibiotic treatment, treatment failure rate, pathogens, and antibiotic resistance between younger and older patients (aged 65 and over) or patients with early and late-onset NP [14, 26].
Obviously, our findings were consistent with the conventional studies on risk variables such as MV, first antibiotic change, and infections, all of which had a substantial influence on the outcomes of NP therapy [1, 4, 11, 22, 23]. Moreover, based on the studies above on the role of qSOFA and CCI in community-acquired pneumonia, we have collected and analyzed data to determine the helpfulness of qSOFA and CCI scores to NP [2, 3, 28]. The studies’ strengths should be acknowledged, including prospective study design with 4 years of data collection and the use of qSOFA and CCI to predict outcomes among NP in an ICU setting.
The limitations in our study were: short follow-up time (7 days), lack of etiology of treatment failure of pneumonia, and insufficient sample for further statistical analysis (e.g., predictive modeling with areas under the curve). Therefore, other studies are needed to design a model for predicting the clinical effect of NP.
Conclusions
Patients with nosocomial pneumonia hospitalized in intensive care units are usually associated with many underlying diseases, including neurological diseases. Mechanical ventilation, a change in antibiotics, CCI ≥ 3, and qSOFA ≥ 2 are also associated with a worse prognosis of nosocomial pneumonia. CCI and qSOFA might be used in predicting the outcome of nosocomial pneumonia.
References
American Thoracic Society, and the Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388–416.
Asai N, Watanabe H, Shiota A, Kato H, et al. Efficacy and accuracy of qSOFA and SOFA scores as prognostic tools for community-acquired and healthcare- associated pneumonia. Int J Infect Dis. 2019;84:89–96.
Bahlis LF, Diogo LP, Fuchs SC. Charlson Comorbidity Index and other predictors of in-hospital mortality among adults with community-acquired pneumonia. J Bras Pneumol. 2021;47(1):e20200257.
Binh TTN, Thang DV. Antibiotic resistance of bacteria in nosocomial pneumonia in ventilated patients treated at ICU people hospital 115. Med J Ho Chi Minh City. 2014;18(1):324–9.
Center for Disease Dynamics, Economics & Policy. Situation Analysis: Antibiotic Use and Resistance in Vietnam. 2011. https://cddep.org/publications/situation_analysis_antibiotic_use_and_resistance_vietnam/. Accessed 20 May 2021.
Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101:1644–55.
Cacciatore F, Gaudiosi C, Mazzella F, Scognamiglio A, et al. Pneumonia and hospitalizations in the elderly. Geriatric Care. 2017;3:20–8.
Cao B, Tan TT, Poon E. Consensus statement on the management of methicillin-resistant Staphylococcus aureus nosocomial pneumonia in Asia. Clin Respir J. 2015;9:130–42.
Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83.
Chawla R. Epidemiology, etiology, and diagnosis of hospital-acquired pneumonia and ventilator-associated pneumonia in Asian countries. Am J Infect Control. 2008;36:93–100.
Duc TH, Yen VN. Antibiotic resistance of bacteria that cause hospital pneumonia, mechanical ventilation pneumonia, healthcare-associated pneumonia in the intensive care unit. Med J Ho Chi Minh City. 2012;8:42–9.
Esperatti M, Ferrer MV. Validation of predictors of adverse outcomes in hospital acquired pneumonia in the ICU. Crit Care Med. 2013;41(9):2151–61.
Ferrer M, Torres A. Epidemiology of ICU-acquired pneumonia. Curr Opin Crit Care. 2018;24:325–31.
Gastmeier P, Sohr D, Geffers C, et al. Early- and late-onset pneumonia: is this still a useful classification? Antimicrob Agents Chemother. 2009;53(7):2714–8.
Gaynes R, Edwards RJ. Overview of nosocomial infections caused by gram-negative bacilli. Clin Infect Dis. 2005;41:848–54.
George N, Turenne MCE, Seethala RR, Aisiku PI, et al. External validation of the qSOFA score in emergency department patients with pneumonia. J Emerg Med. 2019;57(6):755–64.
Jiao J, Yang X, Li Z, Zhao Y, et al. Incidence and related factors for hospital-acquired pneumonia among older bedridden patients in China: a hospital-based multicenter registry data based study. Infect Dis Surveil Prevent Treat Sec J Front Public Health. 2019;7:1–10.
Kieu NP, Trung NP, Tho TTT, Binh TN (2015) Microbiological characteristic causes of hospital acquired pneumonia in ICU department An Giang hospital. In: Scientific Conference of An Giang Hospital, p 1–8
Kollef HM, Shorr A, et al. Epidemiology and outcomes of health-care–associated pneumonia. Chest. 2005;128:3854–62.
Mecham ID, Dean NC, Wilson EL, et al. The association of qSOFA, SOFA, and SIRS with mortality in emergency department pneumonia patients. Univ Louisville J Respir Infect. 2018;2:12–8.
Ott SR, Hauptmeier BM, Ernen C, Lepper PM. Treatment failure in pneumonia: impact of antibiotic treatment and cost analysis. Eur Respir J. 2012;39(3):611–8.
Peerawong W, Pattarachai K, Visanu T. Hospital-acquired pneumonia and ventilator-associated pneumonia in adults at Siriraj hospital: etiology, clinical outcomes, and impact of antimicrobial resistance. J Med Assoc Thai. 2010;1:126–38.
Huong QL. Study on clinical and subclinical characteristics and assessment of treatment effectiveness of hospital pneumonia at the respiratory center at Bach Mai Hospital. Hanoi: Hanoi Medical University; 2012.
Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–9.
Ranzani OT, Prina E, Menéndez R, et al. New sepsis definition (sepsis-3) and community-acquired pneumonia mortality a validation and clinical decision-making study. Am J Respir Crit Care Med. 2017;196(10):1287–97.
Ruiz LA, España PP, Gómez A. Age-related differences in management and outcomes in hospitalized healthy and well-functioning bacteremic pneumococcal pneumonia patients: a cohort study. BMC Geriatr. 2017;17:130–7.
Singer M, Deutschman CS, Seymou CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801–10.
Spagnolello O, Ceccarelli G, Borrazzo C, Macrì A, et al. qSOFA as a new community-acquired pneumonia severity score in the emergency setting. Emerg Med J. 2020;1:1–7.
Wałaszek M, Kosiarska A, Gniadek A, Kołpa M, et al. The risk factors for hospital-acquired pneumonia in the intensive care unit. Przegl Epidemiol. 2016;70:15–20.
Zhang X, Liu B, Liu Y, et al. Efficacy of the quick sequential organ failure assessment for predicting clinical outcomes among community-acquired pneumonia patients presenting in the emergency department. BMC Infect Dis. 2020;20:316–24.
Acknowledgements
We would like to thank all the participants of the study.
Funding
No funding or sponsorship was received for this study or publication of this article.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by SD-Q, TV-P-M, VD-T-T, TN, QP-T-X, and PD-T. The first draft of the manuscript was written by SD-Q, TV-P-M, VD-T-T, HP-T, and TB-A and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. SD-Q is in charge of responding to reviews.
Disclosures
Thu Vo-Pham-Minh, Van Duong-Thi-Thanh, Thang Nguyen, Quyen Phan-Tran-Xuan, Hoang Phan-Thi, Tram Bui-Anh, Phuoc Duong-Thien, and Sy Duong-Quy have nothing to disclose.
Compliance with Ethics Guidelines
Researchers responsible for data collection obtained consent from the participants who were given information regarding the purpose of the study and understood that they could withdraw at any point in the survey without it affecting their care. The Institutional Review Board approved this observational study of Can Tho University of Medicine and Pharmacy, Vietnam with 1530/QD—DHYDCT in June 2015. This study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Vo-Pham-Minh, T., Duong-Thi-Thanh, V., Nguyen, T. et al. The Impact of Risk Factors on Treatment Outcomes of Nosocomial Pneumonia Due to Gram-Negative Bacteria in the Intensive Care Unit. Pulm Ther 7, 563–574 (2021). https://doi.org/10.1007/s41030-021-00175-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41030-021-00175-4