
Abstract
Background
This study investigated the prevalence of Enterococcus faecalis, its putative virulence factors and antimicrobial susceptibility in individuals with and without dental diseases. A total of 159 oral rinse specimens were collected from patients (n = 109) suffering from dental diseases and healthy controls (n = 50).
Results
E. faecalis was detected using only culture in 8/109 (7.3%) of the patients with various types of dental diseases, whereas no E. faecalis was found in the healthy controls weather using both culture and PCR. Phenotype characterizations of the 8 E. faecalis isolates indicated that 25% of the isolates produced haemolysin and 37.5% produced gelatinase. Most important virulence genes; collagen binding protein (ace) and endocarditis antigen (efaA) were present in all 8 E. faecalis isolates, while haemolysin activator gene (cylA) was detected only in 25% of isolates, and all isolates were negative for esp gene. All E. faecalis isolates were 100% susceptible to ampicillin, chloramphenicol, ciprofloxacin, vancomycin, and teicoplanin, and to less extent to erythromycin (62.5%).
Conclusion
This study shows that all E. faecalis isolates were recovered only from patients with dental diseases especially necrotic pulps, and all isolates carried both collagen binding protein and endocarditis antigen genes and highly susceptible to frequently used antimicrobial drugs in Jordan.
Similar content being viewed by others


Background
Many studies demonstrated that E. faecalis is frequently found in patients suffering from oral infections like gingivitis, periodontitis, teeth with failed endodontic as well as acidic carious lesions associated with persistently infected root canals. [1–4] Other studies demonstrated the frequent presence of E. faecalis in association with a wide variety of aerobic and anaerobic bacterial species involved in various endodontic diseases and chronic apical periodontitis [4–7].
Virulent factors of E. faecalis include adherence to host tissue, invasion and abscess formation, modulation of host inflammatory responses, secretion of various products which enhances biofilm formation [8–10]. Data on oral prevalence of E. faecalis and its virulence factors vary from one study to another [1, 6, 7]. Therefore, more investigation on potential virulence factors of E. faecalis would be useful in understanding their role in dental infections. Moreover, clinical isolates of E. faecalis recovered from root canal infections can express antimicrobial resistance to conventional treatment regimens recommended for dental procedures [11–13].
This study aimed to investigate the occurrence of E. faecalis, its virulence factors and antimicrobial susceptibility in association with and without some dental diseases in a Jordanian population.
Results
Age of the patients ranged from 14 to 75 years (mean; 36.4 year), and the control persons were between 20 and 69 years (mean; 28.3 year). The prevalence of E. faecalis isolates in oral rinse specimens of patients with dental diseases was 8/109 (7.3%) using both culture and PCR tests, whereas all oral rinse specimens obtained from the 50 healthy control persons were negative for E. faecalis using both methods. All DNA extracted from 8 E. faecalis isolates were proved to be positive for specific E. faecalis 16s rRNA gene. The difference between the results of the two groups is statistically significant (P value = 0.031). In addition, there was 2 E. avium isolates (Table 1). The growth pattern of E. faecalis isolated from positive cases varied from few to numerous colonies (2 – 50 × 103 colonies/ml). The distribution of 8 E. faecalis isolates among patients in association of sex, smoking, oral hygiene and dental diseases is shown in (Table 2). Detection of putative virulence factor genes among 8 E. faecalis isolates using PCR were as follows; both ace and efaA genes were present in all isolates (100%), while cylA gene was detected only in 2 isolates, and all isolates were negative for esp gene (Table 3, Figure 1). All 8 E. faecalis isolates were 100% susceptible to, ampicillin, chloramphenicol, ciprofloxacin, teicoplanin and vancomycin, while 62.5% and 12.5% of the isolates were susceptible to erythromycin, imipenem, respectively, and all were resistant to gentamicin, clindamycin and Oxacillin

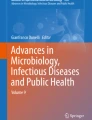
Distribution of efaA gene among the 8 oral E. faecalis isolates. M, 100 bp DNA marker; Lane 1, efaA (688 bp); positive control (E. faecalis ATCC 29212); Lane 2, efaA negative control; Lanes 3 to 10, positive to efaA among oral E. faecalis isolates.
Methods
A total of 159 subjects who were attending the Dental clinic/Jordan University Hospital (JUH), Amman, Jordan were examined for presence of dental diseases by two dentists (N. Dar-Odeh & O. Abu Hammad) during the study period of 2005. Subjects were divided into two groups according to the presence or absence of dental diseases. Control group consisted of 50 healthy persons who do not have any obvious dental disease. Dental diseases investigated include: dental caries, plaque-induced gingivitis, and root canal disease. Personal data, smoking history, presence or absence of clinical dental disease, oral hygiene and antibiotic treatment during the last month were recorded for each examined person. Dental caries and gingivitis were recorded as present/absent. Root canal disease included: irreversible pulpitis, necrotic pulp only, and periapical periodontitis. Oral hygiene was considered as either poor or good according to plaque index. All patients and control persons had given their written consent to be included in the study. All patients and controls were asked to rinse their mouths for 60 seconds with 10 ml sterile distilled water and returned the oral rinse to a sterile container.
Specimens Processing
All specimens were transferred immediately to the Microbiology Research Laboratory/Faculty of Medicine/University of Jordan. Oral rinse specimens were poured into sterile tube and centrifuged for 10 min at 10,000 g. The supernatant discarded and the remaining pellets were re-suspended by vortex in one ml of sterile normal saline 0.9% [14].
Isolation of Enterococcus species
A loop full of the suspended pellets (0.01 ml) was cultured on bile-esculin agar plates to detect and count the presence of gray to black colonies of Enterococcus species. The rest of the suspended specimens were stored at -70°C for further investigations. At least three colonies grown on bile-esculin plates were sub-cultured into blood agar plates to isolate Enterococcus species (Oxoid, England). All cultures carried out through the study were incubated in a candle jar (5% CO2) for 24–48 hrs at 37°C. Pure growth obtained from blood agar plates was again inoculated onto Cysteine Lactose Electrolyte Deficient (CLED) agar plates (Oxoid, England), 6.5% NaCl solution and bile-esculin tube agar. Every growth showing gram-positive cocci, positive bile-esculin, positive 6.5% NaCl tests, catalase-negative and appearing as yellow, small/medium in size on CLED agar (Oxoid, England) were recorded tentatively as Enterococcus isolates. E. faecalis ATCC 29212 was included as a positive control through out the study.
Biochemical detection of E. faecalis isolates
All tentative Enterococcus isolates were subcultured on brain heart infusion agar plates (Oxoid, England) and tested using biochemical Remel system (RapID™ STR system, USA) to confirm their identity as E. faecalis.
Hemolysin and gelatinase activities
E. faecalis isolates were assessed for hemolytic activity on blood base agar (Oxoid, England) supplemented with 5% (v/v) human blood. A single colony was cultured onto blood agar plates and its hemolytic activity was determined by presence of clear zone around the colonies (β hemolysis) as reported by Creti et al. [15]. Gelatinase activity was assessed by inoculation of single colonies of each isolate as spot form on 12% gelatin plates (Defico, USA). The plates were incubated at room temperature for 48 hrs. Gelatinase activity was evident by the presence of liquefied zone around the colonies. Serratia mercenses ATCC 13880 was used as a positive control for gelatinase production test.
Antimicrobial susceptibility test
Susceptibility of E. faecalis isolates to 9 antimicrobial agents was determined using disc diffusion method according to NCCLS (now CLSI) guidelines [16].
Detection of E. faecalis in oral rinse sample by PCR
DNA extraction was performed using Wizard Genomic DNA Purification Kit (Promega, USA), according to manufacturer's instructions. The DNA extractions were used for detecting the specific gene 16S rRNA of E. faecalis in oral rinse samples [17]. PCR conditions were accomplished by a PCR thermocycler (MJ research- INC, USA), and were as follows: 15 min initial enzyme activation/DNA denaturation step at 95°C followed by 35 consecutive cycles at 94°C for 20 s; 68°C for 45 s; 72°C for 15s. PCR products were analyzed by electrophoresis using 2% agarose gel (Promega, USA) containing ethidium bromide in 1× TBE buffer, and run for 1 hr with 70V, and visualized by UV Trans-illuminator (UVP) and Gel Documentation System (UVP). The same PCR reaction was tested with each single control strain of E. faecium and S. mutans which were isolated from other clinical specimens at JUH, and by using E. faecalis ATCC 29212.
The PCR test used, gave a negative result with DNA extracted from E. faecium and S. mutans. Also, DNA extraction of recovered and identified E. faecalis isolates were confirmed using the same DNA extraction and PCR procedure under the same conditions used for oral rinse specimens (Table 4).
Detection of E. faecalis putative virulence genes
DNA of E. faecalis isolates was prepared by suspending a loop full of overnight growth colonies grown on blood agar in a tube that contained 500 μl sterile distilled water, followed by boiling for 10 min and then centrifuged at 12,000 g for 6 min. An aliquot of the supernatant (5 μl) was used as the template in a final volume of 25 μl PCR mixture [15]. PCR amplification for the following genes: collagen binding protein (ace), endocarditis antigen (efaA), haemolysin activator (cylA), and a surface protein (esp) were prepared as uniplex in a 25 μl final reaction volume. Table 5 shows the primers used in the study [15, 17, 18].
Samples were amplified in a PCR thermal cycler (MJ research- INC, USA), by heating for 5 min at 95°C, followed by 30 cycles of 95°C for 60 s, 58°C for 60 s (63°C for esp) and 72°C for 60 s, and a final step of 72°C for 10 min. PCR products were analyzed in 0.8% agarose gel electrophoresis (containing 0.5% ethidium bromide in 1× TBE buffer) which run for 50 minutes by 80 voltages using horizontal electrophoresis apparatus, and visualized by Gel Documentation System (UVP, USA). E. faecalis ATCC 29212 was used as a positive control in each PCR run to detect cylA, ace, efaA genes, and to test DNA prepared from certain E. faecalis strains (EFS121, EFS87, EFS16, EFS27B, EFSU85, and EFS118) which were obtained from Dr. Roberta Creti (Dipartimeno Di Malattie Infecttive, Parassitarie ED Immunomediate, Istituto Superiore di Sanità, Viale Regina Elena, 299–00161 Rome, Italy). These DNA preparations were used as a positive control for esp gene along with 1 Kb/100 bp Ladder marker (promega, USA).
Statistical analysis
Z test was used to compare the prevalence of E. faecalis in patients group and control group according to the following equation:
Z = P1 - P2/√P(1-P) (1/n1 + 1/n2). P < 0.05 was considered statistically significant.
Discussion
The present study shows that E. faecalis isolates were recovered from Jordanian patients in association with one or more of the following dental diseases; caries, gingivitis, plaque-induced gingivitis, and endodontic infection, and in a significant rate (7.3%; P = 0.031) compared to healthy control persons (Zero). Despite the fact that generally PCR is more sensitive than culture method in detection of bacteria in clinical specimens, this study has not detected any positive E. faecalis using direct oral rinse specimens. Sedgley CM et al., 2005 (19) found that a quantitative real-time PCR reported a higher incidence of E. faecalis in oral rinse samples than culture techniques and afforded greater sensitivity. The study revealed that poor oral hygiene, gingivitis and necrotic pulps appear to be important predisposing factors for infection with E. faecalis (Table 2). A recent similar study from USA has isolated E. faecalis from 11% of oral rinse samples of patients receiving endodontic treatment, but only 1% of E. faecalis was recovered from dental students with no history of endodontic treatment [14]. Enterococci are able to colonize the oral cavity, particularly in patients with periodontitis or root canal infections associated with oral mucosal lesions and in immuno-compromised patients [20, 21]. Also, E. faecalis is the most commonly isolated species from root canals samples with endodontic failure [2, 21, 22]. E. faecalis has been often isolated in pure culture or as a predominant organism in previously root- filled teeth with periapical lesions or chronic apical periodontitis [3, 19, 23, 24]. Furthermore, it has been found that this organism persistently infected root canal where calcium hydroxide medication is ineffective [25].
This study shows that the production of hemolysin and gelatinase as putative virulence determinants were not always expressed by E. faecalis isolates in association with dental diseases, since only 25% of E. faecalis isolates expressed hemolysin and 37.5% gelatinase activity in vitro, respectively. Two studies carried by Sedgley et al. [14, 23] reported different results with hemolysin production, first study has proved that 36% of the E. faecalis strains recovered from endodontic patients produced hemolysin, while the second has not detected production of hemolysin in any enterococcal isolates from endodontic cases. Also, Sedgley et al. [22] found that gelatinase gene (gelE) was detected in all endodontic isolates of E. faecalis while expressed gelatinase activity was observed in two thirds of the isolates. These studies concluded that evidence of potential virulence factors were identified in endodontic Enterococcus spp., specifically production of gelatinase and response to pheromones. Other studies indicated that expression of gelatinase gene contributed to the increased dissemination of E. faecalis in high-density environments and was associated with increased adhesion of E. faecalis to dentine in vitro [26, 27].
The present study has shown that both ace and efaA genes were present in all E. faecalis isolates, while cylA gene was detected only in two isolates, and all isolates were negative for esp gene which is mostly found in E. faecalis strains isolated from urinary tract infections [18].
A recent molecular-based study indicated that virulence determinants efaA and ace genes has been found in all E. faecalis isolates from root canal of endodontic patients, whereas esp gene was present in (58%) and cylA gene in (19.4%) of the isolates [11]. These results are in agreement with our results except for esp gene. In general, the expression of hemolysin and gelatinase activity or their genes along with the occurrence of other virulence genes (esp, cylA, ace, efa A) in E. faecalis strains varied widely from one study to another and probably due to the difference in their clinical and geographic origins [5, 9, 11, 26–29]. Furthermore, neither esp nor gelatinase seemed to be required for biofilm formation; both E. faecalis and E. faecium did not show a correlation between the presence of either esp or the production of gelatinase and biofilm formation [30]. It appears that many environmental and genetic factors may be associated with the production of biofilm by E. faecalis [31].
In recent years, enterococci have received increasing attention because of the development of resistance to multiple antimicrobial drugs and its common prevalence in nosocomial infections. Vancomycin-resistant enterococci (VRE) probably represent currently the most serious challenge among many microbes with antibiotic resistance causing human infections [32]. Our results showed that all E. faecalis isolates were susceptible to chloramphenicol, ampicillin, vancomycin, ciprofloxacin, and teicoplanin, but the isolates were much less susceptible to erythromycin. A study by Pinheiro et. al. [12] showed that E. faecalis isolates from oral specimens were completely susceptible in vitro to amoxicillin, amoxicillin-clavulanic acid, vancomycin and to less extent susceptible to erythromycin, moxifloxacin, chloramphenicol, tetracycline, doxycycline, and ciprofloxacin. The susceptibility result of our limited number of E. faecalis isolates indicated higher frequency of resistance rates than those reported in recent studies from western countries [11–13]. Moreover, our susceptibility result correlate well with the high prevalence of resistance among clinical and community Staphylococcus aureus isolates in Jordan [33].
In conclusion, this study shows that all E. faecalis isolates are associated with various dental diseases especially necrotic pulps in patients and they carried both collagen binding protein and endocarditis antigen genes.
References
Sedgley C, Buck G, Appelbe O: Prevalence of Enterococcus faecalis at multiple oral sites in endodontic patients using culture and PCR. J Endod. 2006, 32: 104-109. 10.1016/j.joen.2005.10.022.
Johnson EM, Flannagan SE, Sedgley CM: Coaggregation interactions between oral and endodontic Enterococcus and bacterial species isolated from persistent apical periodentitis. J Endod. 2006, 32: 946-950. 10.1016/j.joen.2006.03.023.
Pinheiro ET, Gomes BP, Ferraz CC, Sousa EL, Teixeira FB, Souza-Filho FJ: Microorganisms from canals of root-filled teeth with periapical lesions. Int Endod J. 2003, 36: 1-11. 10.1046/j.1365-2591.2003.00603.x.
Rams T, Feik D, Young V, Hammond B, Slots J: Enterococci in human periodontitis. Oral Microbiol Immunol. 1992, 7: 249-252. 10.1111/j.1399-302X.1992.tb00034.x.
Kayaoglu G, Ørstavik D: Virulence factors of Enterococcus faecalis: Relationship to endodontic disease. Int Am Asso for Dent Res. 2004, 15: 308-320.
Gomes BPFA, Pinheiro ET, Gade-Neto CR, Sousa EL, Ferraz CC, Zaia AA, Teixeira FB, Souza-Filho FJ: Microbiological examination of infected dental root canal. Oral Microbiol Immunol. 2004, 19: 71-76. 10.1046/j.0902-0055.2003.00116.x.
Reynaud af Geijersstam A, Culak R, Molenaar L, Chattaway M, Røslie E, Peciuliene V, Haapasalo M, Shah HN: Comparative analysis of virulence determinants and mass spectral profiles of Finnish and Lithuanian endodontic Enterococcus faecalis isolates. Oral Microbiol Immunol. 2007, 22: 88-94. 10.1111/j.1399-302X.2007.00327.x.
Tendolkar PM, Baghdavan As, Shankar N: Putative surface proteins encoded within a novel transferable locus confer a high-biofilm phenotype to Enterococcus faecalis. J Bacteriol. 2006, 188: 2063-72. 10.1128/JB.188.6.2063-2072.2006.
Archimbaud C, Shankar N, Forestier C, Baghdayan A, Gilmore MS, Charbonne F, Joly B: In vitro adhesive properties and virulence factors of Enterococcus faecalis strains. Res Microb. 2002, 153: 75-80. 10.1016/S0923-2508(01)01291-8.
Eaton TJ, Gasson MJ: Molecular Screening of enterococcus virulence determinants and potential for genetic exchange between food and medical isolates. Appl Environ Microbiol. 2001, 67: 1628-1635. 10.1128/AEM.67.4.1628-1635.2001.
Reynaud Af, Geijersstam AH, Ellington MJ, Warner M, Woodford N, Haapasalo M: Antimicrobial susceptibility and molecular analysis of Enterococcus faecalis originating from endodontic infections in Finland and Lithuania. Oral Microbiol Immunol. 2006, 21: 164-168. 10.1111/j.1399-302X.2006.00271.x.
Pinheiro ET, Gomes BPFA, Drucker DB, Zaia AA, Ferraz CCR, Souza-Filho FJ: Antimicrobial susceptibility of Enterococcus faecalis isolated from canals of root filled teeth with periapical lesions. Int Endod J. 2004, 37: 756-10.1111/j.1365-2591.2004.00865.x.
Dahle'n G, Samuelsson W, Molander A, Reit C: Identification and antimicrobial susceptibility of enterococci isolated from the root canal. Oral Microbiol Immunol. 2002, 15: 309-312. 10.1034/j.1399-302x.2000.150507.x.
Sedgley CM, Lennan SL, Clewell DB: Prevalence, phenotype and genotype of oral enterococci. Oral Microbiol Immunol. 2004, 19: 95-101. 10.1111/j.0902-0055.2004.00122.x.
Creti R, Imperi M, Bertuccini L, Fabretti F, Orefici G, Di Rosa R, Baldassarri L: Survey for virulence determinants among Enterococcus faecalis isolated from different sources. J Med Microb. 2004, 53: 13-20. 10.1099/jmm.0.05353-0.
NCCLS: Performance Standards for Antimicrobial Susceptibility Testing: 14th Informational Supplements. NCaS document M 100-S14, Wayne, PA: NCaS. 2004
Sedgley CM, Molander A, Flannagan SE, Nagel AC, Appelbe OK, Clewell DB, Dahlen G: Virulence, phenotype and genotype characteristics of endodontic Enterococcus. Oral Microbiol Immunol. 2005, 20: 10-19. 10.1111/j.1399-302X.2004.00180.x.
Shankar N, Lockatell CV, Baghdyan AS, Drachenberg C, Gilmore MS, Johnson DE: Role of Enterococcus faecalis surface protein Esp in the pathogenesis of ascending urinary tract infection. Infect Immun. 2001, 69: 4366-4372. 10.1128/IAI.69.7.4366-4372.2001.
Sedgley CM, Nagel AC, Shelburne CE, Clewell DB, Appelbe O, Molander A: Quantitative real-time PCR detection of oral Enterococcus faecalis in humans. Arch Oral Biol. 2005, 50 (6): 575-83. 10.1016/j.archoralbio.2004.10.017.
Pinheiro ET, Anderson MJ, Gomes BPFA, Drucker DB: Phenotypic and genotypic identification of enterococci isolated from canals of root-filled teeth with periapical lesions. Oral Microbiol Immunol. 2006, 21: 137-144. 10.1111/j.1399-302X.2006.00285.x.
Guven Kayaoglu, Orstakavik D: Virulence enterococcus faecalis: relation to endodontic disease. Crit Rev Oral Biol Med. 2004, 15: 308-320.
Ferrari PHP, Cai S, Bombana AC: Effect of endodontic procedures on enterococci, enteric bacteria and yeasts in primary endodontic infections. Int Endod J. 2005, 38: 372-380. 10.1111/j.1365-2591.2005.00947.x.
Sedgley C, Nagel A, Dahlen G, Reit C, Molander A: Real-time quantative polymerase chain reaction and culture analyses of Enterococcus faecalis in root canals. J Endod. 2003, 32 (3): 173-177. 10.1016/j.joen.2005.10.037.
Molander A, Reit C, Dahlen G, Kvist T: Microbiological status of root-filled teeth with apical periodontitis. Int Endod J. 1998, 31: 1-7. 10.1046/j.1365-2591.1998.t01-1-00111.x.
Nakajo K, Komori R, Ishikawa S, Ueno T, Suzuki Y, Iwami Y, Takahashi N: Resistance to acidic and alkaline environment in the endodontic pathogen Enterococcus faecalis. Oral Microbiol Immunol. 2006, 21: 283-288. 10.1111/j.1399-302X.2006.00289.x.
Hubble TS, Hatton JF, Nallapareddy SR, Murray BE, Gillespie MJ: Influence of Enterococcus faecalis proteases and the collagen-binding protein, Ace, on adhesion to dentin. Oral Microbiol Immunol. 2003, 18: 121-126. 10.1034/j.1399-302X.2003.00059.x.
Waters CM, Antiporta MH, Murray BE, Dunny GM: Role of the Enterococcus faecalis GelE protease in determination of cellular chain length, supernatant pheromone levels, and degradation of fibrin and misfolded surface proteins. J Bacteriol. 2003, 185: 3613-3623. 10.1128/JB.185.12.3613-3623.2003.
Coque TM, Patterson JE, Steckelberg JM, Murray BE: Prevalence of hemolysin, gelatinase, and aggregation substance among enterococci isolated from patients with endocarditis and other infections and from feces of hospitalized and community-based persons. J Infect Dis. 1995, 171: 1223-1229.
Elsner HA, Sobottka I, Mack D, Glaussen M, Laufs R, Wirth R: Virulence factors of Enterococcus faecalis and Enterococcus faecium blood culture isolates. Europ J Clin Microbiol Infect Dis. 2000, 19: 39-42. 10.1007/s100960050007.
Di Rosa R, Creti R, Venditti M, D'Amelio R, Arciola CR, Montanaro L, Baldassarri L: Relationship between biofilm formation, the enterococcal surface protein (Esp) and gelatinase in clinical isolates of Enterococcus faecalis and Enterococcus faecium. FEMS Microbiol Lett. 2006, 256: 145-50. 10.1111/j.1574-6968.2006.00112.x.
Mohamed1 Jamal, Huang David: Biofilm formation by enterococci. J Med Microbiol. 2007, 56: 1581-1588. 10.1099/jmm.0.47331-0.
Willems RJ, Top J, van Santen M, Robinson DA: Global spread of vancomycin-resistant Enterococcus faecium fro distinct nosocomial genetic complex. Emerg Infect Dis. 2006, 11: 821-828.
Al-Zu'bi E, Bdour S, Shehabi AA: Antibiotic resistance patterns of mecA-positive Staphylococcus aureus isolates from clinical specimens and nasal carriage. Microb Drug Resist. 2004, 10: 321-324. 10.1089/mdr.2004.10.321.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1472-6831/8/17/prepub
Acknowledgements
This study was partly supported by grant from the Faculty of Graduate Studies, University of Jordan, Amman, Jordan. The authors thank Dr. Roberta Creti (Laboratory of Bacteriology, Institute of Special Hygiene, University of La Sapienza, Rome, Italy) for sending DNA prepared from certain E. faecalis strains which was used as positive control for esp gene.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
AAS and ND-O contributed to the design of all experiments and writing the manuscript. ND-O and OAH examined all patients and control persons and collected the oral specimens. RS performed all laboratory tests and co-wrote the manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Salah, R., Dar-Odeh, N., Abu Hammad, O. et al. Prevalence of putative virulence factors and antimicrobial susceptibility of Enterococcus faecalis isolates from patients with dental Diseases. BMC Oral Health 8, 17 (2008). https://doi.org/10.1186/1472-6831-8-17
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1472-6831-8-17