
Abstract
Background
Sulphadoxine-pyrimethamine (SP) has been in use for the treatment of uncomplicated falciparum malaria in Malaysia since the 1970s and is still widely employed in spite of widespread clinical resistance. Resistance to SP is known to be mediated by mutations in the pfdhfr and pfdhps genes. The aim of the present study was to investigate the distribution of pfdhfr and pfdhps gene polymorphism in Plasmodium falciparum field isolates from Kalabakan, Sabah, in northern Borneo.
Methods
A total number of 619 individuals were screened from 23 study sites of which 31 were positive for P. falciparum. Analysis of restriction fragment length polymorphisms (RFLP) was used to identify polymorphism in the pfdhfr and pfdhps genes at positions 16, 51, 59, 108, 164 and 437, 540, 581, respectively.
Results
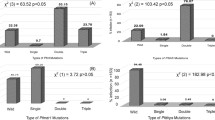
All samples had at least one mutation in each of the genes associated with drug resistance. The prevalence of pfdhfr 59arg, 164leu and 108asn were 100%, 80.65% and 58.06%, respectively. Pfdhps mutants 437gly and 581gly accounted for 100% and 74.19% respectively. In pfdhfr, the most common mutant genotypes were combination 59arg + 164leu (22.58%) and 59arg + 108asn + 164leu (51.61%). In pfdhps the most common genotype was 437gly + 581gly (74.19%). One individual (3.22%) harboured parasites with four pfdhfr (16 val + 59arg + 108asn + 164leu) and two pfdhps (437gly + 581gly) mutations. The highest quintuple pfdhfr/pfdhps (41.94%) was three pfdhfr (59arg + 108asn + 164gly) and two pfdhps (437gly + 581gly).
Conclusion
The data suggest a high prevalence of genetic variations conferring resistance to SP which can predict treatment failure before becoming clinically evident. In areas like this, the use of SP may no longer be indicated.
Similar content being viewed by others


Background
Malaysia is in the pre-elimination phase of the malaria elimination programme [1]. Malaysia is fully committed to controlling malaria, providing good infrastructure for control which dates back to the programme’s implementation in 1961. The impact of the malaria eradication programme has resulted in a major reduction of malaria cases from 243,870 in 1961 to 44,226 in 1980 [1, 2] and has provided the basis for the subsequent malaria control programme which began in 1982. In 2010, the National Malaria Control Programme was re-oriented from control to elimination, with the implementation of the “Malaria Elimination Programme”. This is in line with the global vision of malaria elimination and the aim of achieving malaria elimination status in Peninsular Malaysia by 2012 and Malaysian Borneo by 2020 [3, 4].
The majority of the malaria cases reported in Malaysia in 2012 originated from two states in northern Borneo, Sabah (45%) and Sarawak (29%) (Vector Borne Disease Control 2012, unpublished data). This can largely be attributed to inaccessibility, climate and migration across the nearby border with Indonesia and results in a highly heterogeneous distribution of vector and parasite species as well as drug resistance patterns.
Drug resistance remains a major obstacle to malaria elimination efforts in the region [5, 6]. Sulphadoxine-pyrimethamine (SP) has been in use for the treatment of uncomplicated falciparum malaria in Malaysia since the 1970s. It is used in remote areas for uncomplicated chloroquine-resistant Plasmodium falciparum infections for outpatient as well as inpatient malaria cases. In spite of clinical resistance reported in some places, this combination is still widely employed [7–10].
The genetic background of SP resistance is better documented than any other anti-malarial drug. Mutations in the dihydropteroate synthase (dhps) and dihydrofolate reductase (dhfr) genes, both coding for essential enzymes in the folate biosynthesis pathway, mediate drug resistance to SP [11–13]. Pfdhfr codon ser108asn is likely to play a key role in pyrimethamine resistance with mutations at 51ile, 59arg and 164 leu modulating the level of resistance [14]. The pfdhfr triple mutation 51ile, 59arg and 108asn, has been shown to be associated with SP treatment failure, regardless of pfdhps genotype. Study have shown that findings in vitro may have indication or consistent with reports of failure treatment in the country [15–17]. Sulphadoxine resistance in P. falciparum is associated with mutations at five pfdhps codons; 436ala/phe, 437gly, 540glu, 581gly and 613ser [18–20]. A strong indicator for SP treatment failure is the quintuple mutations in three pfdhfr codons (108asn + 51ile + 59arg) and two pfdhps codons (437gly + 540glu) [21, 22].
In spite of a massive reduction in malaria cases in Malaysia, the drug resistance situation remains poorly documented [9]. Particularly in times of pre-elimination, a better understanding of the epidemiology of drug resistance has become vital for the region. The aim of the present study was therefore to investigate the distribution of pfdhfr and pfdhps gene polymorphism in P. falciparum field isolates from Kalabakan, Sabah, in northern Borneo.
Methods
Study area and sample collection
The study was conducted between 2008 and 2009 in Kalabakan, 100 km from Tawau, in Sabah, bordering East Kalimantan. Samples were collected by active case detection in villages, logging and road construction camps within a radius of 50 to 80 km from Kalabakan. Kalabakan contributes most of the malaria cases in Sabah and was reported to have the highest number of malaria cases in 2008 and 2009 with 21.54% and 22.79%, respectively, of the total number of cases in Sabah. At the time this study was conducted, SP was the official first-line treatment for uncomplicated falciparum malaria and it remains widely used.
The study protocol was reviewed and approved by the institutional review board of the Institute for Medical Research, Kuala Lumpur and the Medical Review and Ethics Committee of the Ministry of Health, Malaysia. Individuals who consented to participate in the study were screened for malaria using rapid diagnostic tests (RDT) (Paramax- 3TM; Zephyr Biomedicals, India). In addition, blood films for malaria parasite (BFMP) were prepared to determine parasite density. All study participants diagnosed positive for malaria infection by RDT had 500 μl of whole blood collected by venepuncture. Blood was then spotted on 3MM Whatman filter paper. The filter paper was allowed to dry completely, transferred into individual plastic bags, labelled, and transported to the Institute for Medical Research in Kuala Lumpur where confirmation of species by PCR and genotype analysis was conducted. Speciation for Plasmodium vivax, P. falciparum, Plasmodium malariae and Plasmodium knowlesi was undertaken using a modified version of published method [23, 24].
DNA extraction
DNA from filter paper was extracted using QIAampTM DNA mini kit (QIAmp; QIAGEN, Hilden, Germany), according to the manufacturer’s instructions (dried blood spots protocol) with the only modification being an adjustment of the elution buffer volume used to elute the DNA. DNA samples were then kept at −20°C until further processing.
Genotyping of pfdhfr and pfdhps by PCR-RFLP
PCR reaction and the restriction fragment polymorphism protocol (PCR-RFLP) were used for the detection of mutation on pfdhfr as described elsewhere [25] with some modification to DNA and primer concentrations. The first round PCR reaction mixture consisted of 50 ng of genomic DNA, 0.20 μM of each primer, 200 μM dNTPs, 1.5 mM MgCl2, and 2.5 U of Taq polymerase in a final reaction volume of 50 μl. Two microlitres of the amplified product from the first PCR were subjected to two sets of secondary round PCR reaction mixtures containing 0.20 μM of each primer, 200 μM dNTPs, 2.0 mM MgCl2, and 2.5 U Taq polymerase. The PCR reaction used primers M4-F amplifying a 326 basepairs (bp) fragment containing cys59arg, ser108asn and ser108thr, and primers M3-F/amplifying a 522 bp fragment containing ala16val, asn51ile, ser108asn and ile164leu (Table 1).
Similarly, nested PCR was conducted for the detection of mutation in the pfdhps gene as described previously [25] with modification on the cycling temperature for the second-round PCR, DNA and primers concentration. The first round PCR was performed using the primer sets R1-R2, followed by two sets of second-round PCR using K-K/and L-L/primers pair (Table 2). The PCR reaction used primers K-K/amplifying a 438 bp fragment containing ala437gly and lys540glu, and primers L-L/amplifying a 161 bp fragment containing ala581gly. The PCR and the nested PCR reactions used the same final concentrations as in the first round PCR carried out for pfdhfr.
The products of the secondary PCR containing the polymorphic region were subjected to enzyme digestion for the detection of mutations at the various sites. The enzyme digestions were conducted according to manufacturer’s instructions (New England Biolabs, Beverly, MA). The details of primer sequences, cycling temperatures, restriction enzyme digestion and fragment sizes for each codon are shown in Tables 1 and 2. DNA of laboratory strain P. falciparum 3D7, K1, W2 and T9.96 were included in each reaction of PCR and RLFP and served as positive and negative controls. Water was used to replace the DNA template for the negative control.
Analysis of PCR-RFLP products using the Agilent 2100 Bioanalyzer
The PCR-RFLP products were analysed using the Agilent 2100 Bioanalyzer and the Agilent DNA 1000 Kit (Agilent Technologies, Molecular Probes Inc, USA). The procedures were conducted according to manufacturer’s instructions (Agilent Technologies, Molecular Probes Inc, USA). The results were then viewed and analysed using the Agilent 2100 software.
Results
Sample collection
A total number of 619 individuals were enrolled and screened at 23 sites. Fifty-eight (9.37%) (95% [CI] = 7.07-11.67%) tested positive for malaria, 5% (95% [CI] = 3.28-6.72%) were positive for P. falciparum. The pfdhfr and pfdhps gene were successfully amplified on all the 31 samples from Kalabakan. These samples were then included in PCR-RFLP analysis for the determination of the prevalence of mutations in the pfdhfr and pfdhps genes.
Pfdhfr mutant genotype
PCR and RFLP products were analysed by Agilent 2100 Bioanalyzer and the Agilent DNA 1000 Kit for the detection of mutations in the pfdhfr gene (details in Figures 1 and 2). Based on PCR-RFLP findings 100%, 80.64% (95% [CI] = 66.74-94.56%), and 58.06% (95% [CI] = 40.69-75.43%) were classified as pfdhfr mutants 59arg, 164leu and 108asn, respectively (Table 3). Mutation at codon 164 and 108 has been identified as strong determinant for pyrimethamine resistant. No mutation was detected at codon 51.

PCR-RFLP of the pfdhfr gene, amplified region of M3-F/primers. BsrI cleaved the 522 bp fragment into 190 and 332 bp indication of 108asn mutation (A). DraI detect 164leu mutations producing 28, 107, 171 and 245 bp fragments for wild type and 107, 143 and 245 bp for mutant (B). Digestion with NlaIII produce 53, 93 and 376 bp for wild type and 146 and 245 bp for mutant at codon 16 (C) and digestion with Tsp5091 yielded 55, 65, 120, and 153 bp fragments for wild type and 55, 65, 120 and 218 bp fragments for mutant for detection on polymorphism at codon 51 (D). Lane L: DNA ladder of Agilent DNA 1000 Kit (Agilent Technologies, Molecular Probes Inc, USA), The controls are in Lane 1 and 2: A: Lane 1: Plasmodium falciparum KI strain (mutant); Lane 2: P. falciparum T9.96 strain (wild type); Lane 3–9: field samples from Kalabakan; well 10: PCR negative control (no DNA was added to the PCR reaction). B and C: Lane 1: Plasmodium falciparum KI strain (wild type); Lane 2: P. falciparum T9.96 strain (wild type); Lane 3–9: field samples from Kalabakan; well 10: PCR negative control (no DNA was added to the PCR reaction). D: Lane 1: Plasmodium falciparum KI strain (wild type); Lane 2: P. falciparum W2 strain (mutant) Lane 3–9: field samples from Kalabakan; well 10: PCR negative control (no DNA was added to the PCR reaction).

PCR-RFLP of the pfdhfr gene, amplified region of M4-F primers. The 326 bp fragment was cut by Alu I into 180 and 118 bp fragments, indications for wild type ser108 and 299 bp for mutant (A). BstNI digested only mutant allele into 145 and 181 bp indicates mutation 108thr. All the tested samples showed wild type (B). Reaction with XmnI produced fragment 163 and 189 bp for wild type; and 26, 137 and 163 bps for 59arg mutation (C). Lane L: DNA ladder of Agilent DNA 1000 Kit (Agilent Technologies, Molecular Probes Inc, USA), The controls are in Lane 1 and 2: A: Lane 1: Plasmodium falciparum KI strain (mutant); Lane 2: P. falciparum T9.96 strain (wild type); Lane 3–9: samples from Kalabakan; Lane 10: PCR negative control (no DNA was added to the PCR reaction). B: Lane 1: Plasmodium falciparum KI strain (wild type); Lane 2: P. falciparum T9.96 strain (wild type); Lane 3–9: samples from Kalabakan; Lane 10: PCR negative control (no DNA was added to the PCR reaction). C: Lane 1: Plasmodium falciparum KI strain (mutant); Lane 2: P. falciparum T9.96 strain (wild type); Lane 3–9: samples from Kalabakan; Lane 10: PCR negative control (no DNA was added to the PCR reaction).
Pfdhps mutant genotype
The most common mutations of the pfdhps gene (details in Figure 3) were observed at 437gly (100%) and 581gly (74.19%) (95% [CI] = 58.79–89.59%) which are commonly associated with sulphadoxine resistance (Table 3). No mutation was observed at codon 540.

PCR-RFLP of pfdhps gene. Amplified region of K-K/primers was targeted to ala437gly with AvaII and lys540glu with FokI, showed 404 bp (mutant) and 438 bps (wild type) respectively (A, B). Reaction of L-L/amplified region with BstUI showed presence of 581gly mutation with a 138 bp fragment and wild type ala581 producing a 105 bp (C). Lane L: DNA ladder of Agilent DNA 1000 Kit (Agilent Technologies, Molecular Probes Inc, USA). The controls are in Lane 1 and 2: A: Lane 1: Plasmodium falciparum 3D7 strain (mutant); Lane 2: P. falciparum K1 strain (mutant); B: Lane 1: Plasmodium falciparum K1 strain (wild type); Lane 2: P. falciparum T9.96 strain (wild type); C: Lane 1: Plasmodium falciparum K1 strain (mutant); Lane 2: P. falciparum W2 strain (wild type). Lane 3–10: samples from Kalabakan; Lane 11: PCR negative control (no DNA was added to the PCR reaction).
Pfdhfr/pfdhps mutant genotype combination
Five different mutant genotypes related to the pfdhfr gene (Table 4) were identified. The three most common combinations were 59arg + 108asn + 164leu (51.61%) (95% [CI] = 34.02%-69.2%) and 59arg + 164leu (22.58%) (95% [CI] = 7.86%-37.3%). The rest of the genes, 25.81% (95% [CI] = 10.41% to 41.21%), existed either on its own or in combination with the other genes (Table 4). Pfdhps mutant genotypes combined 437gly + 581gly (74.19%) (95% [CI] = 58.79%-89.59%) (Table 4). When combining pfdhfr and pfdhps mutations, there was one parasite isolate (3.22%) (95% [CI] = −2.99%-9.43%) harbouring four pfdhfr (16 val + 59arg + 108asn + 164leu) and two pfdhps (437gly + 581gly) mutations (Table 5). The most commonly found mutant genotype combining pfdhfr and pfdhps linked three pfdhfr mutations 59arg + 108asn + 164leu with two pfdhps mutations 437gly + 581gly with 41.94% (95% [CI] = 24.57%- 59.31%) (Table 5).
Discussion
The study report the prevalence of mutations in the pfdhfr and pfdhps genes in P. falciparum field isolates collected from individuals in Kalabakan, Sabah (Northern Borneo). This region remains the focus of P. falciparum infection in a country that has reached pre-elimination and is striving for malaria elimination in the coming years. SP has been used extensively in the region for more than 30 years, as first-line drug until 2010 [26]. This is surprising as SP treatment failures have been reported from Malaysia as early as 1982 [7]. By the late 1990s, SP resistance had reached 47.4% in Peninsular Malaysia [8] and 29.4% in Tawau, Sabah [9] and first evidence of the molecular background of SP resistance in Malaysia came from a study conducted on mainland Malaysia and Borneo reported in 2001 [27].
The findings of the study indicate that all samples collected harbour at least one of the markers known to be involved in SP resistance on both the pfdhfr as well as the pfdhps gene. Without exception all samples (100%) had the pfdhps mutation 437gly, which is a common observation in areas where SP is widely used. Earlier studies suggest that its presence alone or in combination with 540glu is predictive of early SP treatment failure [28, 29]. The 540glu is typically found together with 437gly, particularly in Africa [30, 31]. However, the findings of the study showed that all the samples harboured the pfdhps 437gly mutation together with 581 gly (74.19%) rather than 540glu. In fact, the studies indicate the complete absence of the 540glu mutation in the patient samples. Both combinations have been associated with sulphadoxine resistance [32, 33]. The findings for 581gly also confirm earlier reports from the region [27]. In spite of extensive use of the drug there were surprisingly few changes in the epidemiology of pfdhps and pfdhfr mutations within these seven years.
The other mutation that seems to affect virtually all P. falciparum parasite samples in the region is 59arg (Table 3). This mutation is believed to modulate pyrimethamine resistance [21, 34]. A study conducted in Burkino Faso, showed that pfdhfr 59arg, with 51ile and 108asn is an important marker for SP treatment failure [35]. Another study from Mozambique suggested that the two mutations at pfdhfr 59arg and pfdhps 437gly were enough to predict SP treatment failure [36].
The study suggests that there are two predominant pfdhfr mutation genotypes; 59arg + 164leu (22.58%) and 59arg + 108asn + 164leu (51.61%). There was not a single quadruple mutant (51ile + 59arg + 108asn + 164leu) in the samples, which is considered to be an indication of the highest levels of resistance to pyrimethamine [37]. Similar to the 540glu mutation in pfdhps, this study did not identify any sample with the 51ile mutation. However, Dokomajilar et al. suggested that 59arg, even in the absence of 51ile, may be more important as a marker for pyrimethamine resistance [35].
However, the results observed the presence of a sextuple mutation consisting of four pfdhfr (16val, 59arg, 108asn and 164leu) and two pfdhps (437gly, 581gly) mutations in a single individual from loggers’ camps near the border of Kalabakan to East Kalimantan. There were two sets of three pfdhfr and two pfdhps mutation (a quintuple) observed in the samples; a mutation genotype consisting of 59arg + 108asn + 164le + 437gly + 581gly, making up 41.94% of the samples and 16 val + 59arg + 164leu + 437gly + 581gly, which was found in a single sample only. The association of molecular findings with clinical treatment response was not possible due to the very low malaria prevalence and the active case detection used in this study covering a huge and largely inaccessible catchment area.
Conclusion
Results from this study indicate that all samples harbour at least one mutation on the pfdhfr and pfdhps genes involved in SP resistance, and the predominant mutation genotype consists of a combination of 59arg + 108asn + 164le + 437gly + 581gly (41.94%). There is every indication that these genotypes confer high levels of resistance to SP in the region. This strong evidence of the high prevalence of mutations at the pfdhfr and pfdhps genes in Kalabakan highlights an urgent need for similar studies in other malaria-endemic areas in Sabah to provide urgently needed data on the current situation of SP resistance in the region.
References
Rundi C: Third annual meeting of the Asia Pacific Malaria Elimination Network (APMEN). Malaria Elimination in Malaysia. 2011, Kota Kinabalu, Sabah Malaysia: Ministry of Health Malaysia
WHO: Roll Back Malaria 2005. 2005, Geneva: World Health Organization
Rahman H: First annual meeting of the Asia Pacific Malaria Elimination Network (APMEN). Updates on Malaria Control Activities in Malaysia. 2009, Brisbane, Australia: Ministry of Health Malaysia
Kheong CC: Asian Collaborative Training Network for Malaria (ACT Malaria) Executive Board Meeting; 15–17 March 2010. Country Updates: Malaysia. 2010, Luang Prabang, Lao PDR: Ministry of Health Malaysia
Dondorp AM, Nosten F, Yi P, Das D, Phyo AP, Tarning J, Lwin KM, Ariey F, Hanpithakpong W, Lee SJ, Ringwald P, Silamut K, Imwong M, Chotivanich K, Lim P, Herdman T, An SS, Yeung S, Singhasivanon P, Day NP, Lindegardh N, Socheat D, White NJ: Artemisinin resistance in Plasmodium falciparum malaria. N Engl J Med. 2009, 361: 455-467. 10.1056/NEJMoa0808859.
Olliaro P: Drug resistance hampers our capacity to roll back malaria. Clin Infect Dis. 2005, 41: 247-257. 10.1086/430785.
Ponnampalam JT: Falciparum malaria resistant to Fansidar (sulfadoxine-pyrimethamine) occurring in three children of the same family. Singapore Med J. 1982, 23: 37-38.
Lokman Hakim S, Sharifah Roohi SW, Zurkunai Y, Noor Rain A, Mansor SM, Palmer K, Navaratnam V, Mak JW: Plasmodium falciparum: increased proportion of severe resistance (RII and RIII) to chloroquine and high rate of resistance to sulfadoxine-pyrimethamine in Peninsular Malaysia after two decades. Trans R Soc Trop Med Hyg. 1996, 90: 294-297. 10.1016/S0035-9203(96)90258-8.
Ministry of Health Malaysia: Rancangan Kawalan Penyakit Bawaan Vektor Negeri Sabah: Laporan Tahunan 2010. 2010, Ministry of Health Malaysia: Ministry of Health Malaysia
WHO: World Malaria Report 2010. 2010, Geneva: World Health Organization
Peterson DS, Walliker D, Wellems TE: Evidence that a point mutation in dihydrofolate reductase-thymidylate synthase confers resistance to pyrimethamine in falciparum malaria. Proc Natl Acad Sci USA. 1988, 85: 9114-9118. 10.1073/pnas.85.23.9114.
Peters W: Drug resistance in malaria. Recent Progr Med. 1990, 81: 749-753.
Bwijo B, Kaneko A, Takechi M, Zungu IL, Moriyama Y, Lum JK, Tsukahara T, Mita T, Takahashi N, Bergqvist Y, Björkman A, Kobayakawa T: High prevalence of quintuple mutant dhps/dhfr genes in introduction of sulfadoxine and pyrimethamine as first line treatment in Malawi. Acta Trop. 2003, 85: 363-373. 10.1016/S0001-706X(02)00264-4.
Plowe CV, Cortese JF, Djimde A, Nwanyanwu OC, Watkins WM, Winstanley PA, Estrada-Franco JG, Mollinedo RE, Avila JC, Cespedes JL, Carter D, Doumbo OK: Mutations in Plasmodium falciparum dihydrofolate reductase and dihydropteroate synthase and epidemiologic patterns of pyrimethamine-sulfadoxine use and resistance. J Infect Dis. 1997, 176: 1590-1596. 10.1086/514159.
Hyde JE: The dihydrofolate reductase-thymidylate synthase gene in the drug resistance of malaria parasites. Pharm Ther. 1990, 48: 45-59. 10.1016/0163-7258(90)90017-V.
Peterson DS, Di Santi SM, Povoa M, Calvosa VS, Do Rosario VE, Wellems TE: Prevalence of the dihydrofolate reductase Asn-108 mutation as the basis for pyrimethamine-resistant falciparum malaria in the Brazilian Amazon. Am J Trop Med Hyg. 1991, 45: 492-497.
Basco LK, Eldin de Pecoulas P, Wilson CM, Le Bras J, Mazabraud A: Point mutations in the dihydrofolate reductase-thymidylate synthase gene and pyrimethamine and cycloguanil resistance in Plasmodium falciparum. Mol Biochem Parasitol. 1995, 69: 135-138. 10.1016/0166-6851(94)00207-4.
Brooks DR, Wang P, Read M, Watkins WM, Sims PF, Hyde JE: Sequence variation of the hydroxymethyldihydropterin pyrophosphokinase: dihydropteroate synthase gene in lines of the human malaria parasite, Plasmodium falciparum, with differing resistance to sulfadoxine. Eur J Biochem. 1994, 224: 397-405. 10.1111/j.1432-1033.1994.00397.x.
Triglia T, Menting JG, Wilson C, Cowman AF: Mutations in dihydropteroate synthase are responsible for sulfone and sulfonamide resistance in Plasmodium falciparum. Proc Natl Acad Sci USA. 1997, 94: 13944-13949. 10.1073/pnas.94.25.13944.
Triglia T, Wang P, Sims PF, Hyde JE, Cowman AF: Allelic exchange at the endogenous genomic locus in Plasmodium falciparum proves the role of dihydropteroate synthase in sulfadoxine-resistant malaria. EMBO J. 1998, 17: 3807-3815. 10.1093/emboj/17.14.3807.
Nzila AM, Mberu EK, Sulo J, Dayo H, Winstanley PA, Sibley CH, Watkins WM: Towards an understanding of the mechanism of pyrimethamine-sulfadoxine resistance in Plasmodium falciparum: genotyping of dihydrofolate reductase and dihydropteroate synthase of Kenyan parasites. Antimicrob Agents Chemother. 2000, 44: 991-996. 10.1128/AAC.44.4.991-996.2000.
Wernsdorfer WH, Noedl H: Molecular markers for drug resistance in malaria: use in treatment, diagnosis and epidemiology. Curr Opin Infect Dis. 2003, 16: 553-558. 10.1097/00001432-200312000-00007.
Padley D, Moody AH, Chiodini PL, Saldanha J: Use of a rapid, single-round, multiplex PCR to detect malarial parasites and identify the species present. Ann Trop Med Parasitol. 2003, 97: 131-137. 10.1179/000349803125002977.
Imwong M, Tanomsing N, Pukrittayakamee S, Day NPJ, White NJ, Snounou G: Spurious amplification of a Plasmodium vivax small-subunit RNA gene by use of primers currently used to detect P. knowlesi. J Clin Microbiol. 2009, 47: 4173-4175. 10.1128/JCM.00811-09.
Duraisingh MT, Curtis J, Warhurst DC: Plasmodium falciparum: detection of polymorphisms in the dihydrofolate reductase and dihydropteroate synthetase genes by PCR and restriction digestion. Exp Parasitol. 1998, 89: 1-8. 10.1006/expr.1998.4274.
WHO: World Malaria Report 2011. 2011, Geneva: World Health Organization
Cox-Singh J, Zakaria R, Abdullah MS, Rahman HA, Nagappan S, Singh B: Differences in dihydrofolate reductase but not dihydropteroate synthase alleles in Plasmodium falciparum isolates from geographically distinct areas in Malaysia. Am J Trop Med Hyg. 2001, 64: 28-31.
Omar SA, Adagu IS, Warhurst DC: Can pre-treatment screening for dhps and dhfr point mutations in Plasmodium falciparum infections be used to predict sulfadoxine-pyrimethamine treatment failure?. Trans R Soc Trop Med Hyg. 2001, 95: 315-319. 10.1016/S0035-9203(01)90250-0.
Kublin JG, Dzinjalamala FK, Kamwendo DD, Malkin EM, Cortese JF, Martino LM, Mukadam RA, Rogerson SJ, Lescano AG, Molyneux ME, Winstanley PA, Chimpeni P, Taylor TE, Plowe CV: Molecular markers for failure of sulfadoxine-pyrimethamine and chlorproguanil-dapsone treatment of Plasmodium falciparum malaria. J Infect Dis. 2002, 185: 380-388. 10.1086/338566.
Pearce RJ, Pota H, Evehe MS, Ba El H, Mombo-Ngoma G, Malisa AL, Ord R, Inojosa W, Matondo A, Diallo DA, Mbacham W, Van Den Broek IV, Swarthout TD, Getachew A, Dejene S, Grobusch MP, Njie F, Dunyo S, Kweku M, Owusu-Agyei S, Chandramohan D, Bonnet M, Guthmann JP, Clarke S, Barnes KI, Streat E, Katokele ST, Uusiku P, Agboghoroma CO, Elegba OY, Cissé B, A-Elbasit IE, Giha HA, Kachur SP, Lynch C, Rwakimari JB, Chanda P, Hawela M, Sharp B, Naidoo I, Roper C: Multiple origins and regional dispersal of resistant dhps in African Plasmodium falciparum malaria. PLoS Med. 2009, 6: e1000055-10.1371/journal.pmed.1000055.
Naidoo I, Roper C: Following the path of most resistance: dhps K540E dispersal in African Plasmodium falciparum. Trends Parasitol. 2010, 26: 447-456. 10.1016/j.pt.2010.05.001.
Urdaneta L, Plowe C, Goldman I, Lal AA: Point mutations in dihydrofolate reductase and dihydropteroate synthase genes of plasmodium falciparum isolates from Venezuela. Am J Trop Med Hyg. 1999, 61: 457-462.
Nagesha HS, Din-Syafruddin Casey GJ, Susanti AI, Fryauff DJ, Reeder JC, Cowman AF: Mutations in the pfmdr1, dhfr and dhps genes of Plasmodium falciparum are associated with in-vivo drug resistance in West Papua, Indonesia. Trans R Soc Trop Med Hyg. 2001, 95: 43-49. 10.1016/S0035-9203(01)90329-3.
Basco LK, Ringwald P: Molecular epidemiology of malaria in Yaoundé, Cameroon. II. Baseline frequency of point mutations in the dihydropteroate synthase gene of Plasmodium falciparum. Am J Trop Med Hyg. 1998, 58: 374-377.
Dokomajilar C, Lankoande ZM, Dorsey G, Zongo I, Ouedraogo JB, Rosenthal PJ: Roles of specific Plasmodium falciparum mutations in resistance to amodiaquine and sulfadoxine-pyrimethamine in Burkina Faso. Am J Trop Med Hyg. 2006, 75: 162-165.
Alifrangis M, Lemnge MM, Rønn AM, Segeja MD, Magesa SM, Khalil IF, Bygbjerg IC: Prediction of Plasmodium falciparum resistance to sulfadoxine/pyrimethamine in vivo by mutations in the dihydrofolate reductase and dihydropteroate synthetase genes: a comparative study between sites of differing endemicity. Am J Trop Med Hyg. 2003, 69: 601-606.
Chusacultanachai S, Thiensathit P, Tarnchompoo B, Sirawaraporn W, Yuthavong Y: Novel antifolate resistant mutations of Plasmodium falciparum dihydrofolate reductase selected in Escherichia coli. Mol Biochem Parasitol. 2002, 120: 61-72. 10.1016/S0166-6851(01)00440-6.
Acknowledgements
The authors would like to thank the Director General Of Health Malaysia for the permission to publish this paper. We thank the Director for the Institute for Medical Research (IMR), Kuala Lumpur for her critical review and support in publishing this paper. This study was supported by the National Institute of Health, Ministry of Health Malaysia. We also thank all staff of Tawau Health Department, Sabah for their contributions and all patients for their participation in this important study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interest
The authors declare that they have no competing interest.
Authors’ contributions
NRA prepared study proposal and protocol, study design, lead the study in Kalabakan, data analysis and interpretation and preparation of manuscript. NAA conducted the molecular genetic studies, analysis of data, data statistics and partly drafted the manuscript. HN participated in coordinating the study, reviewing the data, data analysis and English editing. LHS, ZI, HMS oversight the project. JJ participated in the study design in the field. All authors critically reviewed the manuscript and approved the final version before submission to the Journal. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Abdullah, N.R., Norahmad, N.A., Jelip, J. et al. High prevalence of mutation in the Plasmodium falciparum dhfr and dhps genes in field isolates from Sabah, Northern Borneo. Malar J 12, 198 (2013). https://doi.org/10.1186/1475-2875-12-198
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1475-2875-12-198